
Unsupervised Exercise Training Was Not Found to Improve the Metabolic Health or Phenotype over a 6-Month Dietary Intervention: A Randomised Controlled Trial with an Embedded Economic Analysis

Abstract
:1. Introduction
2. Materials and Methods
3. Results
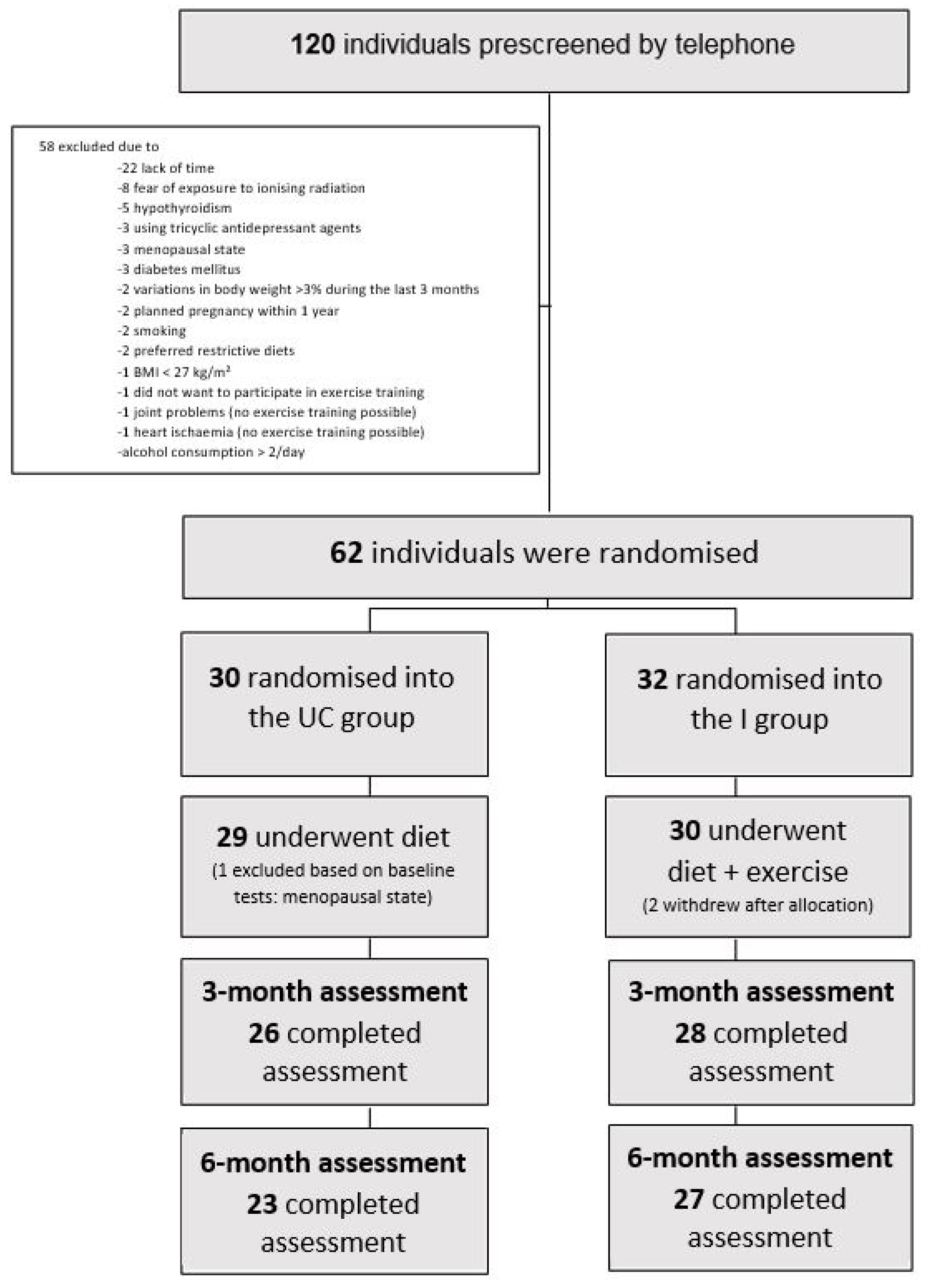
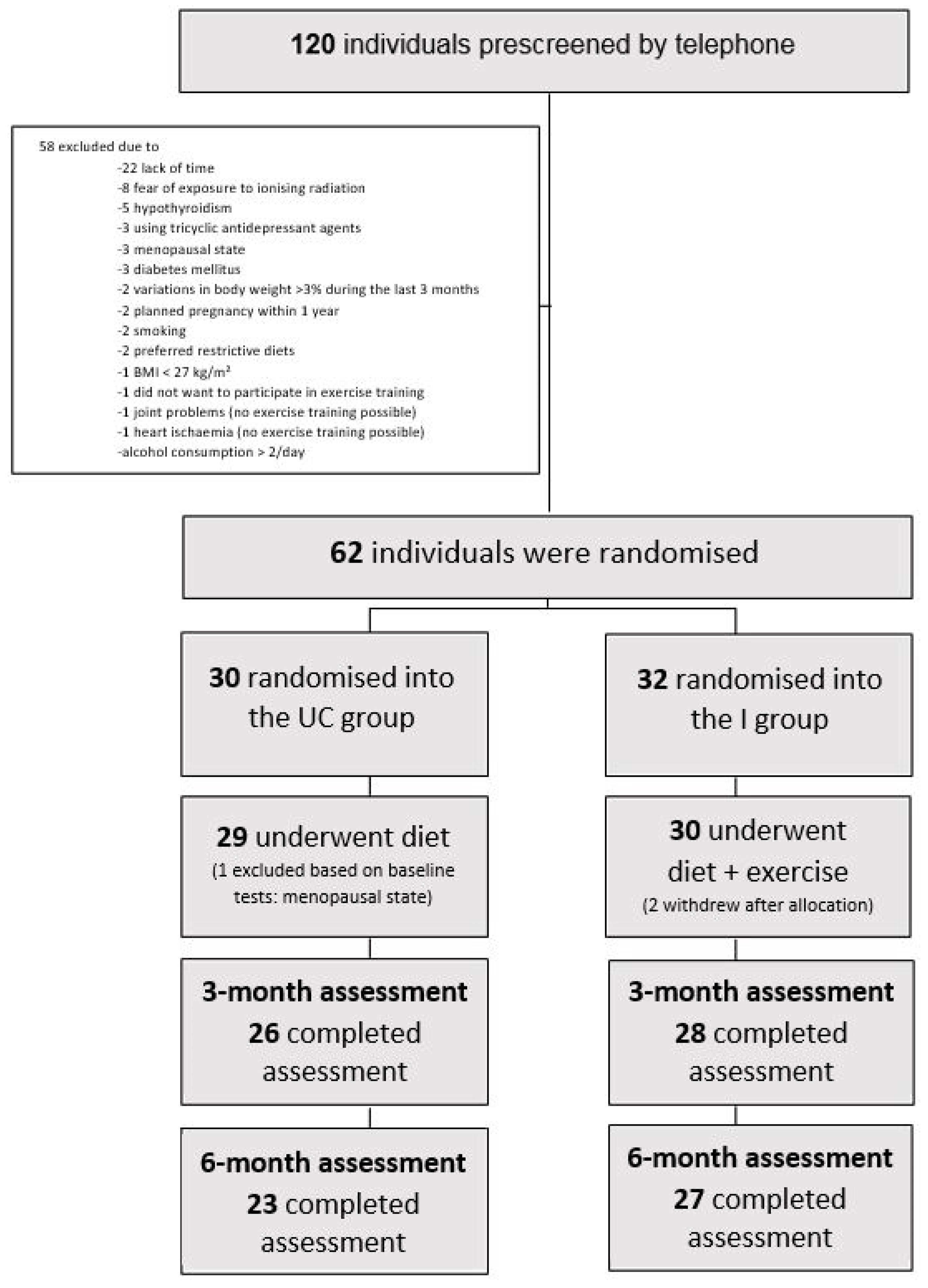
3.1. Flow of Participants
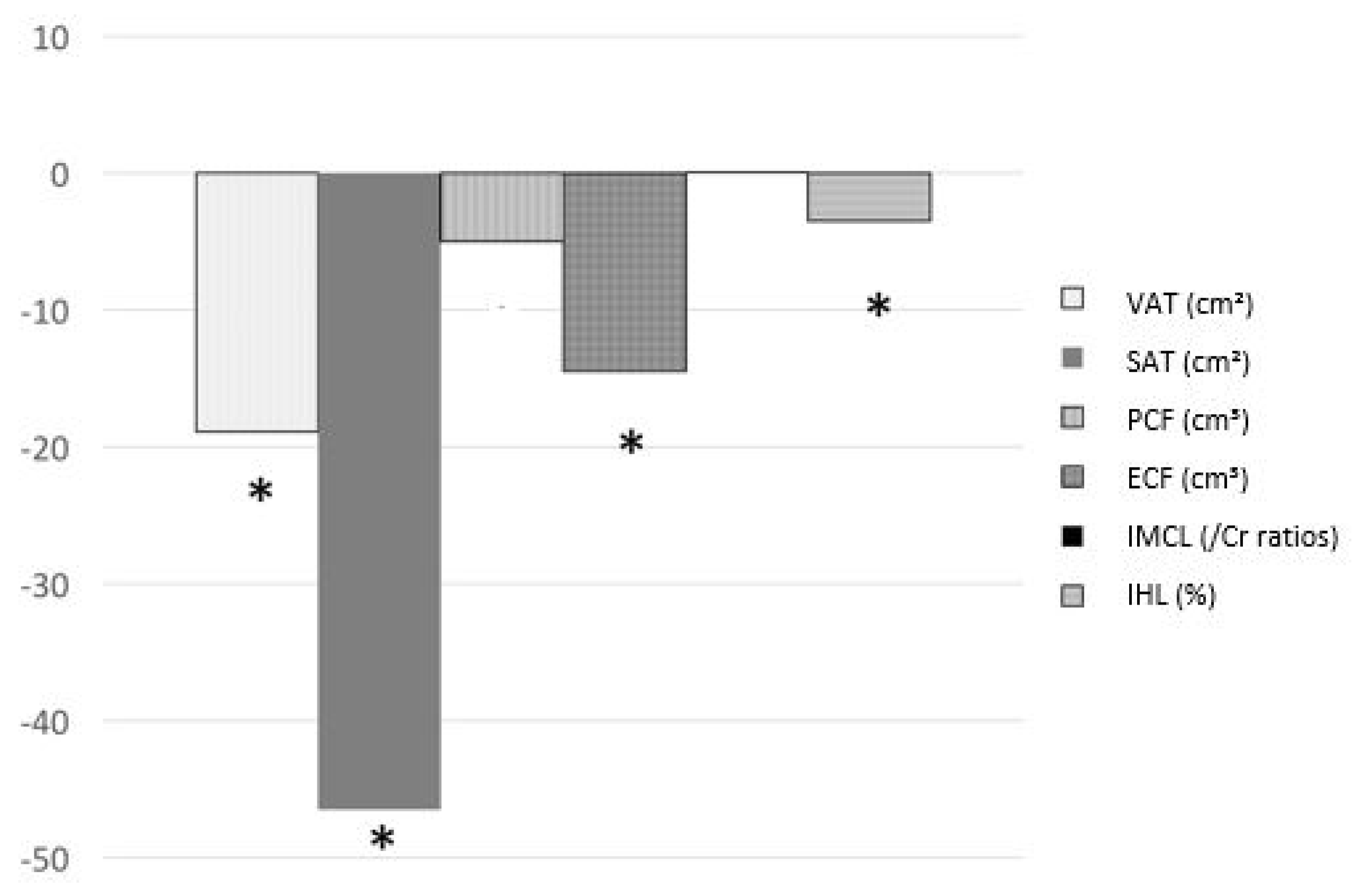
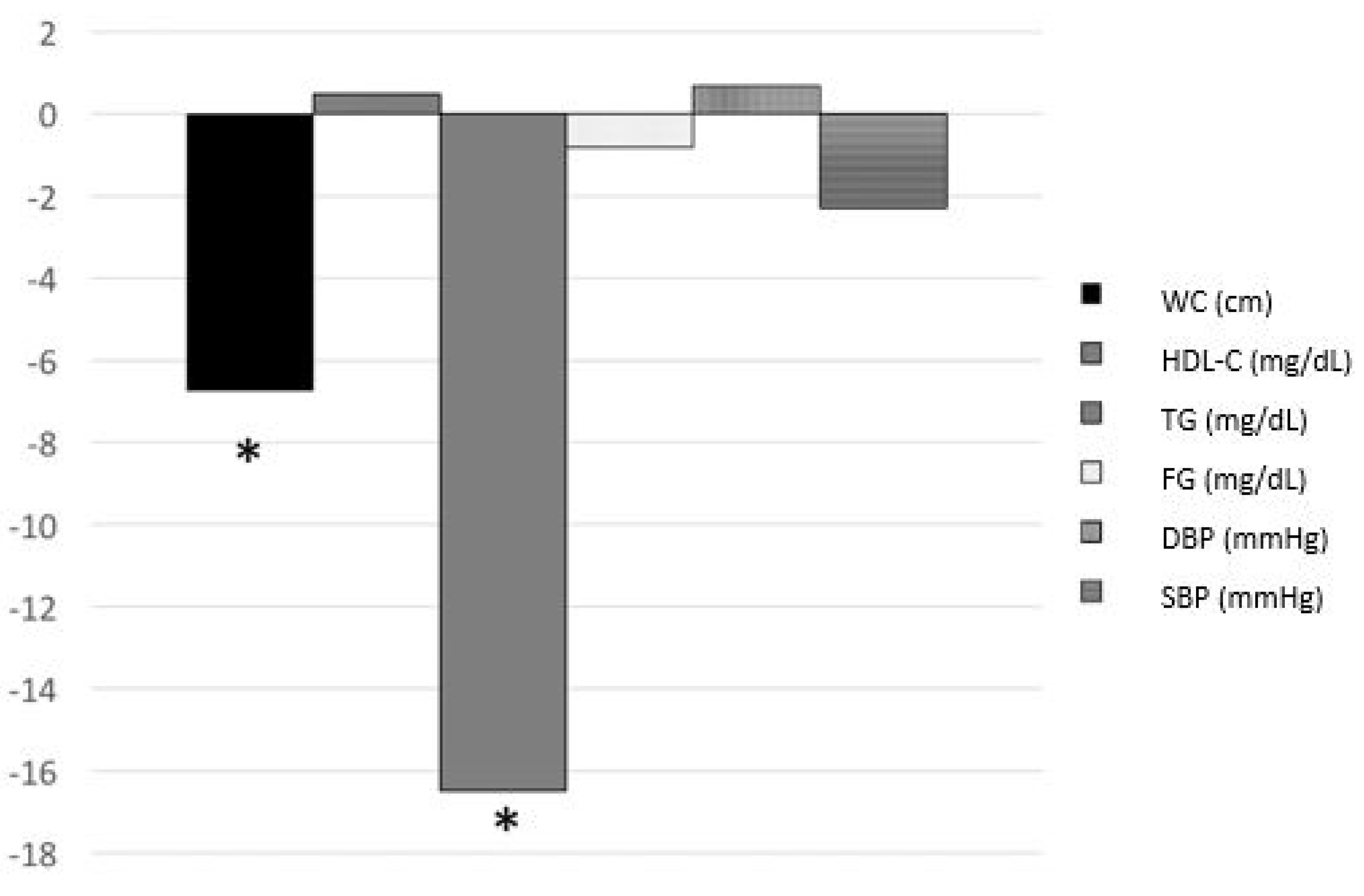
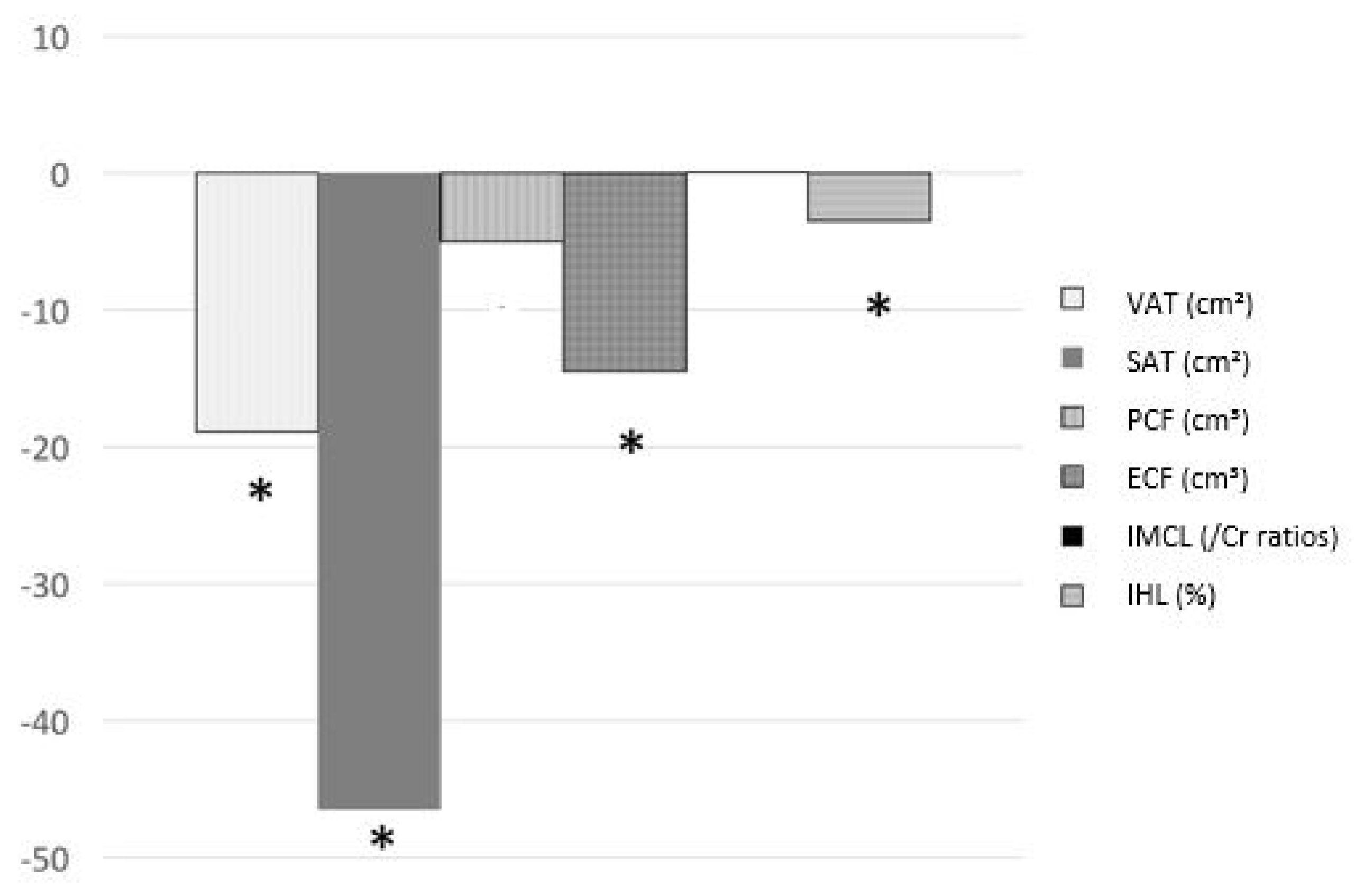
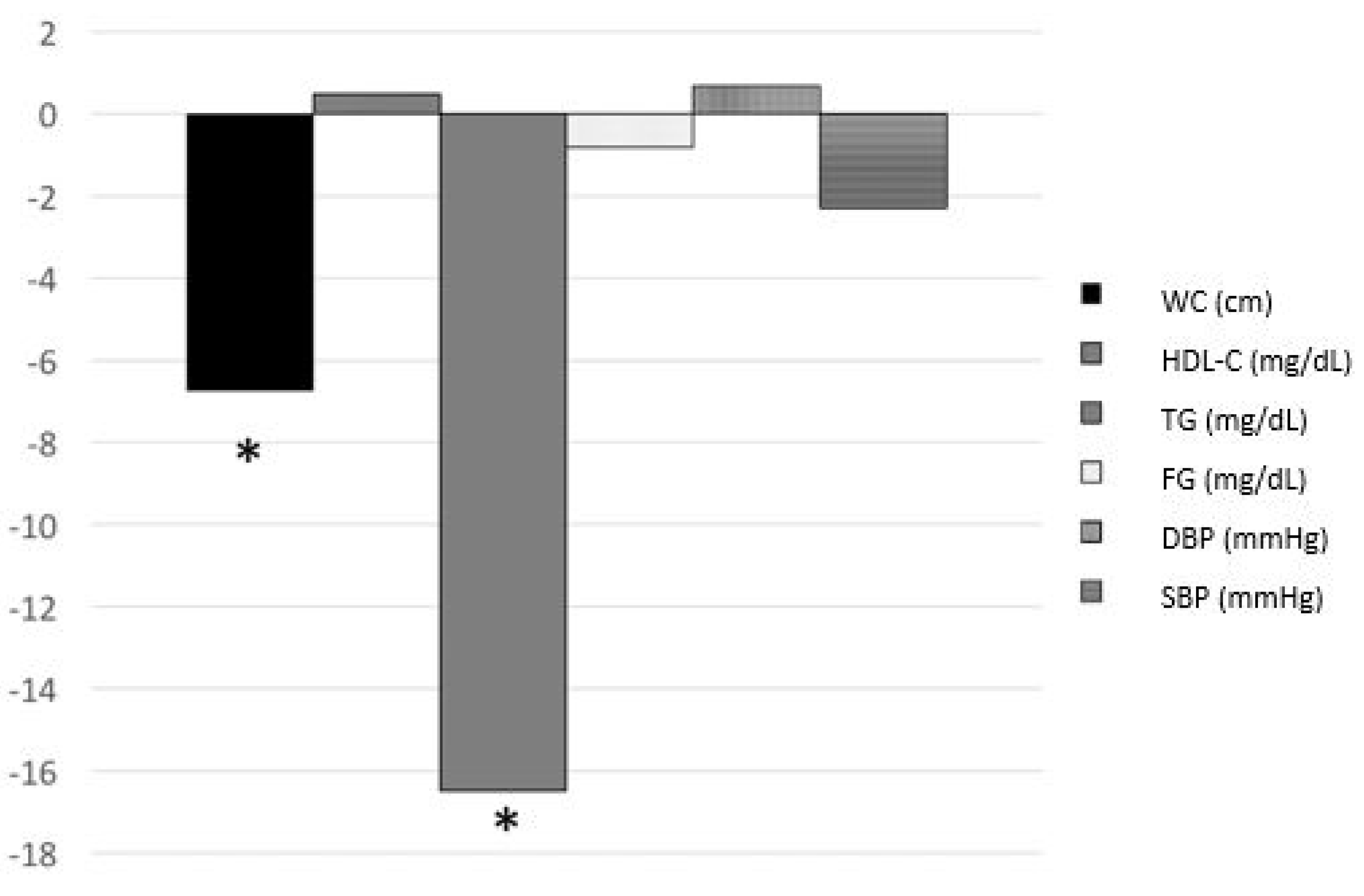
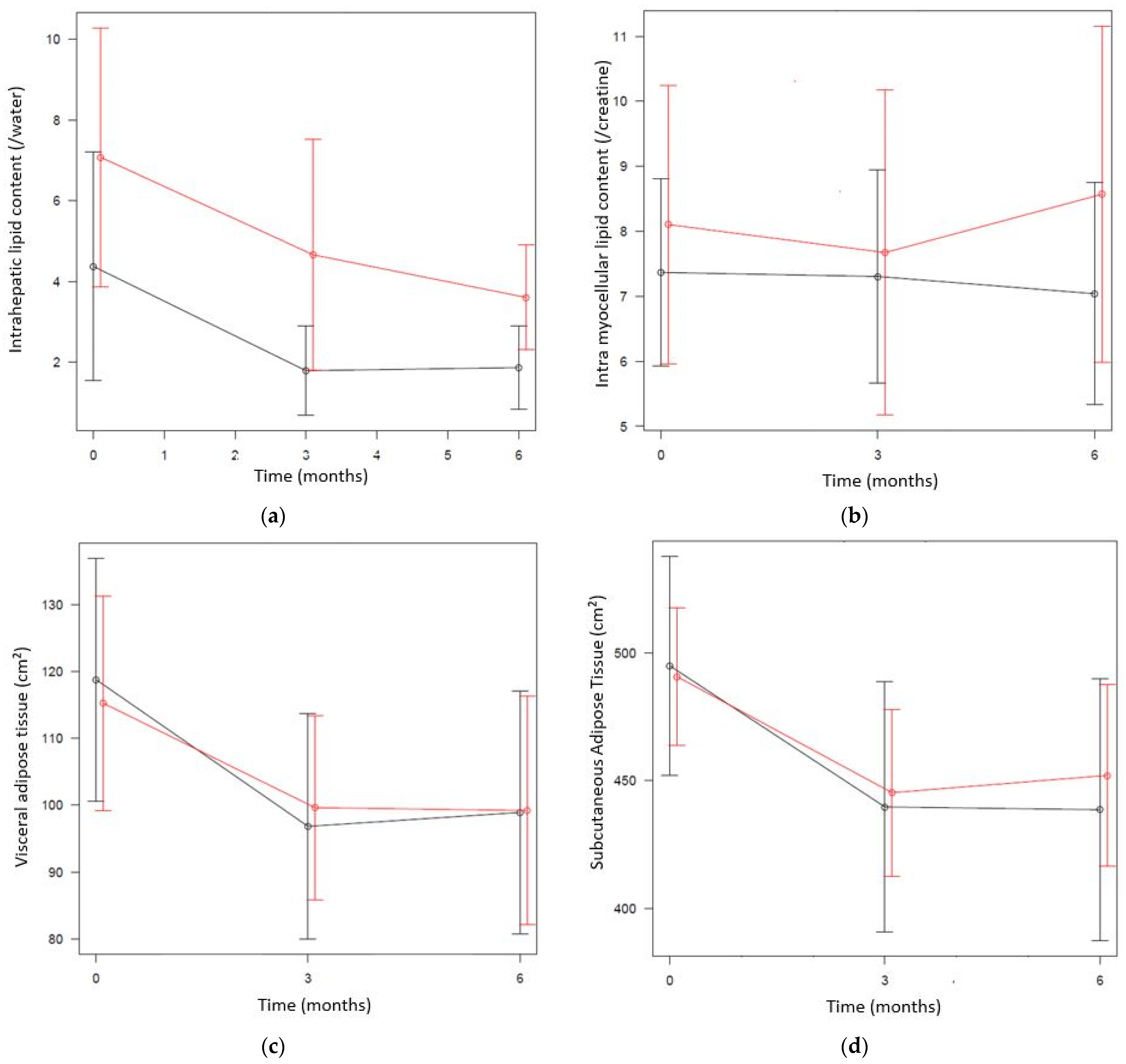
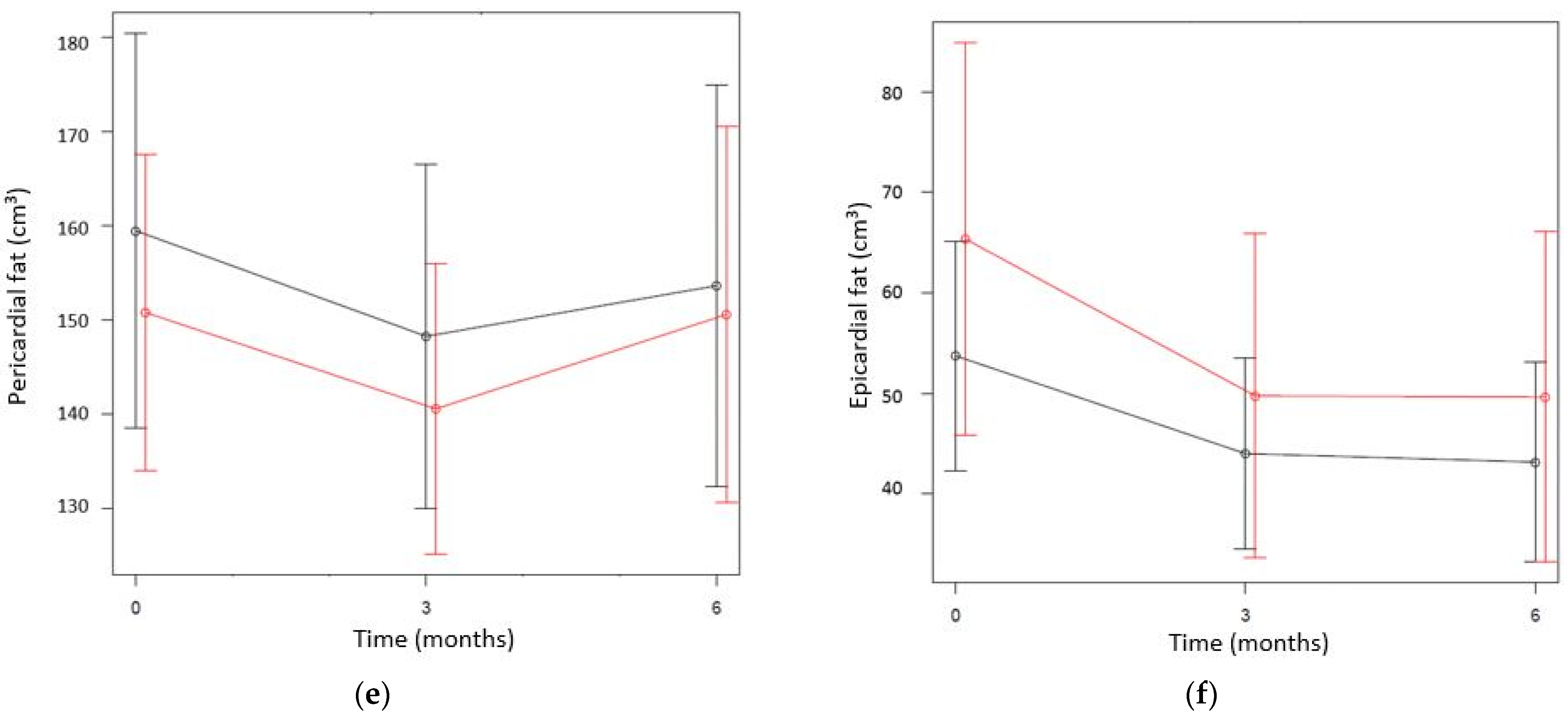
3.2. Changes in Ectopic Fat Deposition and Metabolic Risk Factors in the Total Sample (UC + I Groups)
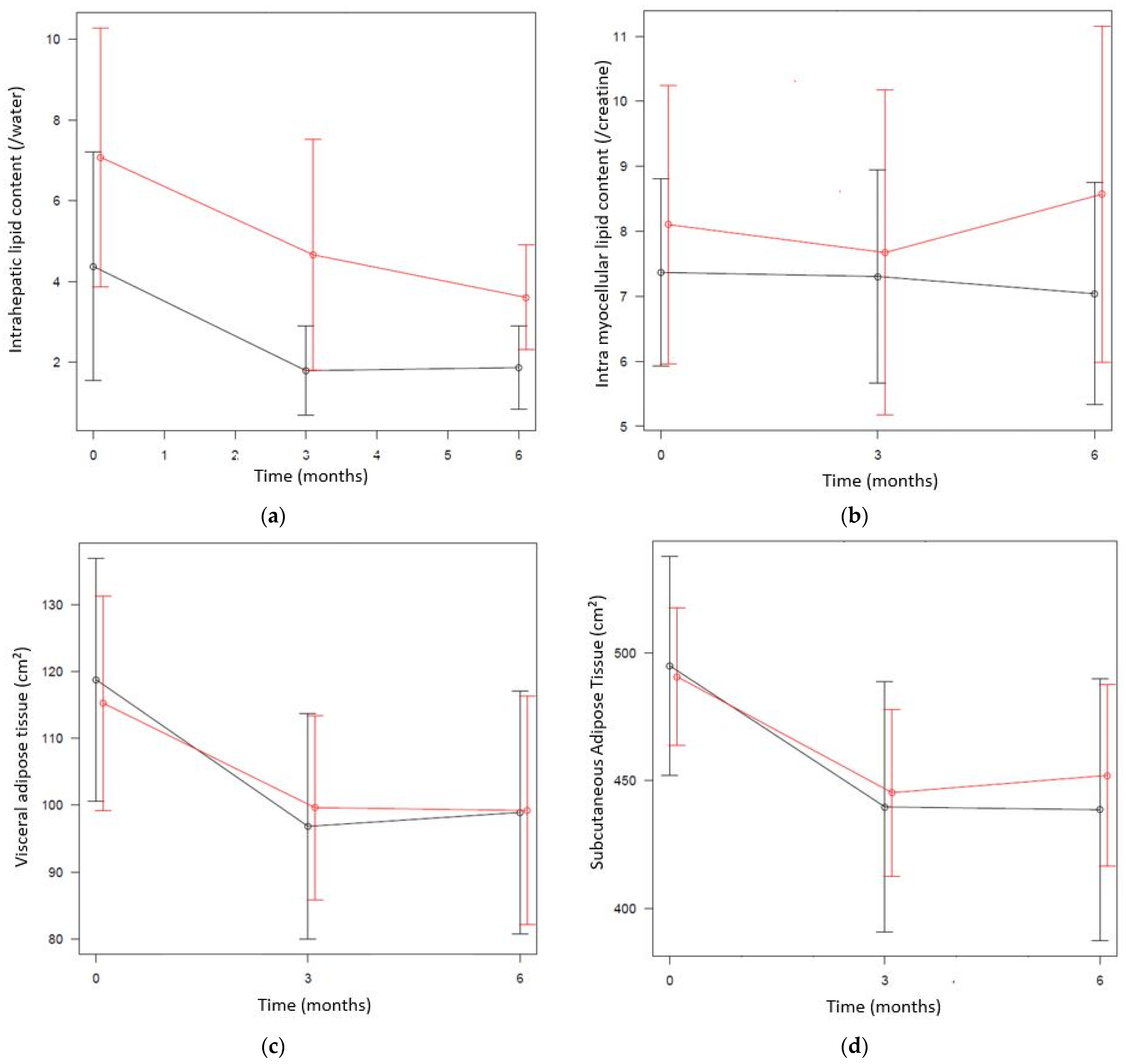
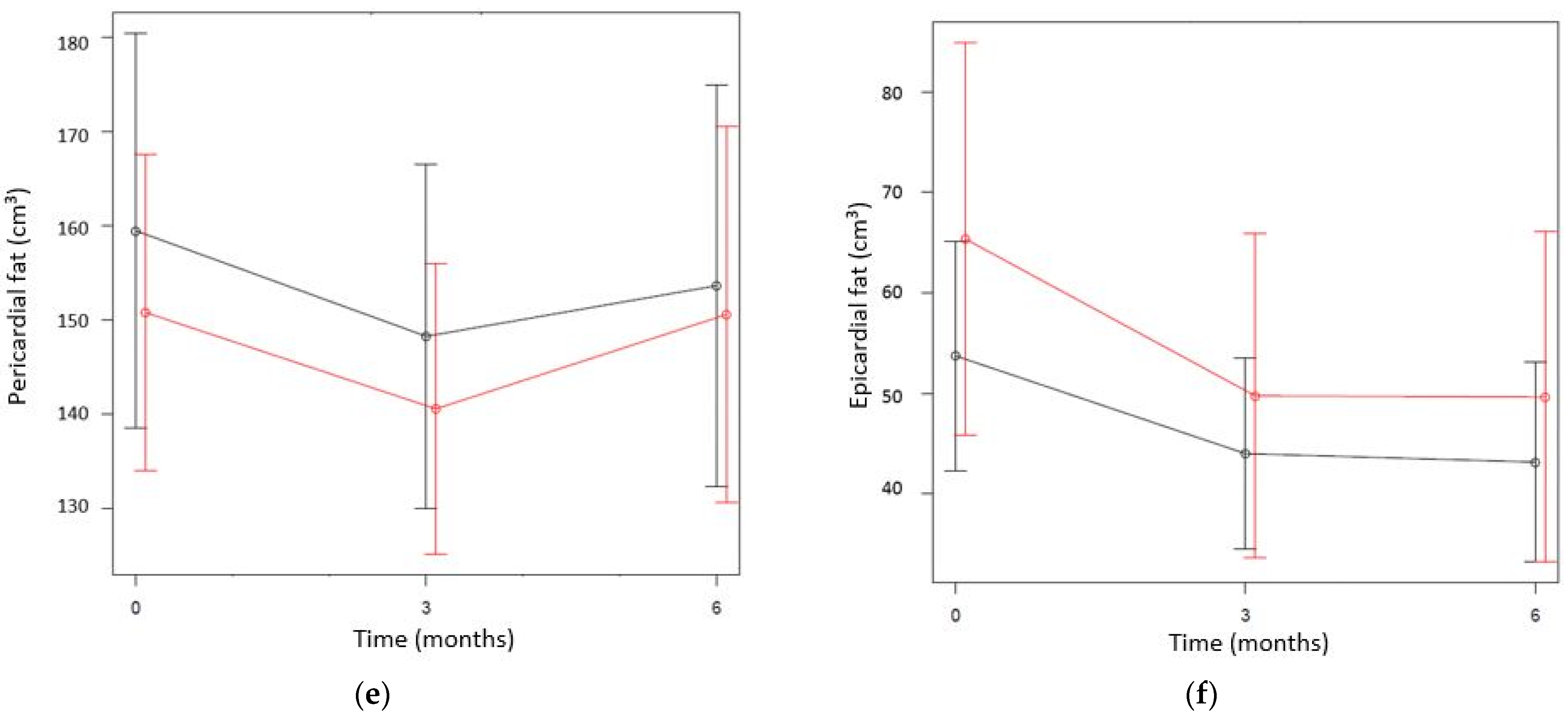
3.3. Differences between the UC and I Groups
3.4. Cost-Effectiveness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hills, A.P.; Byrne, N. State of the science: A focus on physical activity. Asia Pac. J. Clin. Nutr. 2006, 15, 40–48. [Google Scholar] [PubMed]
- Després, J.-P. Obesity and Cardiovascular Disease: Weight Loss Is Not the Only Target. Can. J. Cardiol. 2015, 31, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Hens, W.; Vissers, D.; Annemans, L.; Gielen, J.; Van Gaal, L.; Taeymans, J.; Verhaeghe, N. Health-related costs in a sample of premenopausal non-diabetic overweight or obese females in Antwerp region: A cost-of-illness analysis. Arch. Public Health 2018, 76, 42. [Google Scholar] [CrossRef] [Green Version]
- Stefan, N.; Häring, H.-U.; Schulze, M.B. Metabolically healthy obesity: The low-hanging fruit in obesity treatment? Lancet Diabetes Endocrinol. 2018, 6, 249–258. [Google Scholar] [CrossRef]
- Van Gaal, L.F.; Mertens, I.L.; De Block, C.E. Mechanisms linking obesity with cardiovascular disease. Nature 2006, 444, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.W.; Lee, S.J. Ectopic Fat in Insulin Resistance, Dyslipidemia, and Cardiometabolic Disease. N. Engl. J. Med. 2014, 371, 2236–2238. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMJ 2013, 346, f1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Obstet. Gynecol 2010, 115, 1063–1070. [Google Scholar] [CrossRef]
- Hens, W.; Vissers, D.; Annemans, L.; Gielen, J.; Van Gaal, L.; Taeymans, J. Cost-Effectiveness Analysis of Exercise in Addition to Diet on the Reduction of Ectopic Fat in Women with Overweight Study Protocol for a Randomised Controlled Trial. Physioscience 2017, 13, 80–87. [Google Scholar] [CrossRef]
- Grave, R.D.; Calugi, S.; Centis, E.; El Ghoch, M.; Marchesini, G. Cognitive-Behavioral Strategies to Increase the Adherence to Exercise in the Management of Obesity. J. Obes. 2011, 2011, 348293. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Johnson, P.E.; Bolonchuk, W.W.; Lykken, G.I. Assessment of fat-free mass using bioelectrical impedance measurements of the human body. Am. J. Clin. Nutr. 1985, 41, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.Y.; Dey, D.; Tamarappoo, B.; Nakazato, R.; Gransar, H.; Miranda-Peats, R.; Ramesh, A.; Wong, N.D.; Shaw, L.J.; Slomka, P.J.; et al. Pericardial Fat Burden on ECG-Gated Noncontrast CT in Asymptomatic Patients Who Subsequently Experience Adverse Cardiovascular Events. JACC Cardiovasc. Imaging 2010, 3, 352–360. [Google Scholar] [CrossRef] [Green Version]
- Sottier, D.; Petit, J.-M.; Guiu, S.; Hamza, S.; Benhamiche, H.; Hillon, P.; Cercueil, J.-P.; Krausé, D.; Guiu, B. Quantification of the visceral and subcutaneous fat by computed tomography: Interobserver correlation of a single slice technique. Diagn. Interv. Imaging 2013, 94, 879–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naressi, A.; Couturier, C.; Devos, J.M.; Janssen, M.; Mangeat, C.; De Beer, R.; Graveron-Demilly, D. Java-based graphical user interface for the MRUI quantitation package. Magma 2001, 12, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Mocioiu, V.; Ortega-Martorell, S.; Olier, I.; Jablonski, M.; Starčuková, J.; Lisboa, P.; Arús, C.; Julià-Sapé, M. From raw data to data-analysis for magnetic resonance spectroscopy—The missing link: JMRUI2XML. BMC Bioinform. 2015, 16, 378. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.S.; Chumlea, W.C.; Heymsfield, S.B.; Lukaski, H.C.; Schoeller, D.; Friedl, K.; Kuczmarski, R.J.; Flegal, K.; Johnson, C.L.; Hubbard, V.S. Development of bioelectrical impedance analysis prediction equations for body composition with the use of a multicomponent model for use in epidemiologic surveys. Am. J. Clin. Nutr. 2003, 77, 331–340. [Google Scholar] [CrossRef] [Green Version]
- EuroQol Group Association. EQ-5D Instruments. Available online: https://euroqol.org/publications/key-euroqol-references/eq-5d-5l/ (accessed on 1 January 2018).
- RIZIV. Revalidatieverstrekkingen, 1 January 2017. Available online: www.riziv.fgov.be/SiteCollectionDocuments/tarief_revalidatie_verstrekkingen_20170101.pdf (accessed on 1 January 2018).
- RIZIV. Omzendbrief aan de Kinesitherapeuten, 2017. Available online: https://www.riziv.fgov.be/nl/professionals/individuelezorgverleners/kinesitherapeuten/Paginas/omzendbrieven-kinesitherapeut.aspx (accessed on 1 January 2018).
- Securex. Absenteïsme in 2013 Versnelde Stijging Lange Afwezigheden Maakt Re-Integratiebeleid Noodzakelijk. Available online: http://www.securex.be/export/sites/default/.content/download-gallery/nl/whitepapers/white-paper-absenteisme-in-2013.pdf (accessed on 1 January 2018).
- Gerard, M.; Valsamis, D.; Van der Beken, W. Why Invest in Employment? A Study on the Cost of Unemployment; IDEA Consult: Brussels, Belgium, 2012. [Google Scholar]
- Hallsworth, K.; Fattakhova, G.; Hollingsworth, K.G.; Thoma, C.; Moore, S.; Taylor, R.; Day, C.P.; Trenell, M.I. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut 2011, 60, 1278–1283. [Google Scholar] [CrossRef]
- Inelmen, E.M.; Toffanello, E.D.; Enzi, G.; Gasparini, G.; Miotto, F.; Sergi, G.; Busetto, L. Predictors of drop-out in overweight and obese outpatients. Int. J. Obes. 2004, 29, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Sawamoto, R.; Nozaki, T.; Furukawa, T.A.; Tanahashi, T.; Morita, C.; Hata, T.; Komaki, G.; Sudo, N. Predictors of Dropout by Female Obese Patients Treated with a Group Cognitive Behavioral Therapy to Promote Weight Loss. Obes. Facts 2016, 9, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Britton, K.A.; Fox, C.S. Ectopic Fat Depots and Cardiovascular Disease. Circulation 2011, 124, e837–e841. [Google Scholar] [CrossRef]
- Franz, M.J.; VanWormer, J.J.; Crain, A.L.; Boucher, J.L.; Histon, T.; Caplan, W.; Bowman, J.D.; Pronk, N.P. Weight-Loss Outcomes: A Systematic Review and Meta-Analysis of Weight-Loss Clinical Trials with a Minimum 1-Year Follow-Up. J. Am. Diet. Assoc. 2007, 107, 1755–1767. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.A.; Gennat, H.C.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst. Rev. 2006, 4, CD003817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodpaster, B.H.; DeLany, J.; Otto, A.D.; Kuller, L.; Vockley, J.; South-Paul, J.E.; Thomas, S.B.; Brown, J.; McTigue, K.; Hames, K.C.; et al. Effects of Diet and Physical Activity Interventions on Weight Loss and Cardiometabolic Risk Factors in Severely Obese Adults: A randomized trial. JAMA 2010, 304, 1795–1802. [Google Scholar] [CrossRef] [Green Version]
- Okura, T.; Nakata, Y.; Lee, D.J.; Ohkawara, K.; Tanaka, K. Effects of aerobic exercise and obesity phenotype on abdominal fat reduction in response to weight loss. Int. J. Obes. 2005, 29, 1259–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vissers, D.; Hens, W.; Taeymans, J.; Baeyens, J.-P.; Poortmans, J.; Van Gaal, L. The Effect of Exercise on Visceral Adipose Tissue in Overweight Adults: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e56415. [Google Scholar] [CrossRef] [Green Version]
- Jakicic, J.M.; Marcus, B.H.; Gallagher, K.I.; Napolitano, M.; Lang, W. Effect of Exercise Duration and Intensity on Weight Loss in Overweight, Sedentary Women: A randomized trial. JAMA 2003, 290, 1323–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepaniak, L.S.; Nurenberg, P.; Leonard, D.; Browning, J.D.; Reingold, J.S.; Grundy, S.; Hobbs, H.H.; Dobbins, R.L. Magnetic resonance spectroscopy to measure hepatic triglyceride content: Prevalence of hepatic steatosis in the general population. Am. J. Physiol. Endocrinol. Metab. 2005, 288, E462–E468. [Google Scholar] [CrossRef] [Green Version]
- Hens, W.; Taeymans, J.; Cornelis, J.; Gielen, J.; Van Gaal, L.; Vissers, D. The Effect of Lifestyle Interventions on Excess Ectopic Fat Deposition Measured by Noninvasive Techniques in Overweight and Obese Adults: A Systematic Review and Meta-Analysis. J. Phys. Act. Health 2016, 13, 671–694. [Google Scholar] [CrossRef]
- Hens, W.; Vissers, D.; Hansen, D.; Peeters, S.; Gielen, J.; Van Gaal, L.; Taeymans, J. The effect of diet or exercise on ectopic adiposity in children and adolescents with obesity: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 1310–1322. [Google Scholar] [CrossRef]
- Dubé, J.J.; Amati, F.; Stefanovic-Racic, M.; Toledo, F.; Sauers, S.E.; Goodpaster, B.H. Exercise-induced alterations in intramyocellular lipids and insulin resistance: The athlete’s paradox revisited. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E882–E888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gepner, Y.; Shelef, I.; Schwarzfuchs, D.; Cohen, N.; Bril, N.; Rein, M.; Tsaban, G.; Zelicha, H.; Meir, A.; Tene, L.; et al. Intramyocellular triacylglycerol accumulation across weight loss strategies; Sub-study of the CENTRAL trial. PLoS ONE 2017, 12, e0188431. [Google Scholar] [CrossRef] [Green Version]
- Yki-Järvinen, H. Ectopic fat accumulation: An important cause of insulin resistance in humans. J. R. Soc. Med. 2002, 95 (Suppl. 42), 39–45. [Google Scholar] [PubMed]
- Loher, H.; Kreis, R.; Boesch, C.H.; Christ, E. The Flexibility of Ectopic Lipids. Int. J. Mol. Sci. 2016, 17, 1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihaylova, B.; Briggs, A.; O’Hagan, A.; Thompson, S.G. Review of statistical methods for analysing healthcare resources and costs. Health Econ. 2011, 20, 897–916. [Google Scholar] [CrossRef]
- Bang, H.; Zhao, H. Average Cost-Effectiveness Ratio with Censored Data. J. Biopharm. Stat. 2012, 22, 401–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| UC Group: Diet (n = 30) | I Group: Diet + Exercise (n = 32) | p-Value | |
|---|---|---|---|
| General characteristics | |||
| Age (years) | 36.11 ± 8.94 | 37.64 ± 8.53 | 0.49 |
| BMI (kg/m2) | 32.27 ± 3.50 | 32.98 ± 3.60 | 0.51 |
| Participants with NAFLD | n = 5 (17%) | n = 12 (37.5%) | |
| Participants with metabolic syndrome | n = 1 (3%) | n = 2 (6.25%) | |
| Ectopic fat deposition | |||
| Intrahepatic lipid content (%) | 4.37 ± 7.49 | 7.08 ± 8.95 | 0.20 |
| Intramyocellular lipid content (/creatine) | 7.37 ± 3.82 | 8.10 ± 5.99 | 0.57 |
| VAT (cm2) | 118.78 ± 48.18 | 115.27 ± 44.89 | 0.77 |
| SAT (cm2) | 493.46 ±112.07 | 493.87 ± 76.20 | 0.99 |
| Pericardial fat (cm3) | 159.47 ± 55.58 | 150.81 ± 46.94 | 0.51 |
| Epicardial fat (cm3) | 53.73 ± 30.32 | 65.36 ±54.65 | 0.31 |
| Body fat (%) | 39.20 ± 4.21 | 39.18 ± 3.83 | 0.98 |
| Fat-free mass (kg) | 54.70 ± 5.23 | 54.11 ± 6.26 | 0.69 |
| Metabolic parameters | |||
| Waist (cm) | 100.09 ± 10.13 | 101.28 ± 8.38 | 0.61 |
| Triglycerides (mg/dL) | 105.22 ± 69.19 | 99.13 ± 43.19 | 0.68 |
| Systolic blood pressure (mm Hg) | 121.81 ± 14.78 | 120.00 ± 10.34 | 0.58 |
| Diastolic blood pressure (mm Hg) | 72.48 ±9.94 | 73.93 ± 9.18 | 0.55 |
| HDL cholesterol (mg/dL) | 57.19 ± 10.72 | 58.63 ± 11.35 | 0.55 |
| Fasting glucose (mg/dL) | 84.56 ± 7.23 | 86.30 ± 8.57 | 0.29 |
| Economic Outcome Parameters | Baseline | p-Value (Group) | Month 6 | p-Value (Group) |
|---|---|---|---|---|
| Societal direct medical and non-medical costs | ||||
| UC group | 405.48 ± 845.97 | 0.40 | 301.94 ± 535.74 | 0.48 |
| I group | 731.65 ± 1669.53 | 518.53 ± 1359.65 | ||
| Quality-adjusted life year (QALY) | ||||
| UC group | 0.83 ± 0.16 | 0.81 | 0.86 ± 0.14 | 0.79 |
| I group | 0.84 ± 0.14 | 0.87 ± 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hens, W.; Vissers, D.; Verhaeghe, N.; Gielen, J.; Van Gaal, L.; Taeymans, J. Unsupervised Exercise Training Was Not Found to Improve the Metabolic Health or Phenotype over a 6-Month Dietary Intervention: A Randomised Controlled Trial with an Embedded Economic Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8004. https://doi.org/10.3390/ijerph18158004
Hens W, Vissers D, Verhaeghe N, Gielen J, Van Gaal L, Taeymans J. Unsupervised Exercise Training Was Not Found to Improve the Metabolic Health or Phenotype over a 6-Month Dietary Intervention: A Randomised Controlled Trial with an Embedded Economic Analysis. International Journal of Environmental Research and Public Health. 2021; 18(15):8004. https://doi.org/10.3390/ijerph18158004
Chicago/Turabian StyleHens, Wendy, Dirk Vissers, Nick Verhaeghe, Jan Gielen, Luc Van Gaal, and Jan Taeymans. 2021. "Unsupervised Exercise Training Was Not Found to Improve the Metabolic Health or Phenotype over a 6-Month Dietary Intervention: A Randomised Controlled Trial with an Embedded Economic Analysis" International Journal of Environmental Research and Public Health 18, no. 15: 8004. https://doi.org/10.3390/ijerph18158004
APA StyleHens, W., Vissers, D., Verhaeghe, N., Gielen, J., Van Gaal, L., & Taeymans, J. (2021). Unsupervised Exercise Training Was Not Found to Improve the Metabolic Health or Phenotype over a 6-Month Dietary Intervention: A Randomised Controlled Trial with an Embedded Economic Analysis. International Journal of Environmental Research and Public Health, 18(15), 8004. https://doi.org/10.3390/ijerph18158004