
Impact of Ed-LinQ: A Public Policy Strategy to Facilitate Engagement between Schools and the Mental Health Care System in Queensland, Australia

 , ,
, ,
Abstract
1. Introduction
- -
- Strategic partnerships, including the development of collaborative interdepartmental and interagency relationships, planning and governance mechanisms;
- -
- Enhanced capacities, including workforce development strategies for the mental health, primary care and education sector staff;
- -
- Clinical guidance, including the development of information on young people’s mental health for distribution to the education sector stakeholders [18].
2. Materials and Methods
3. Results
3.1. Quantitative
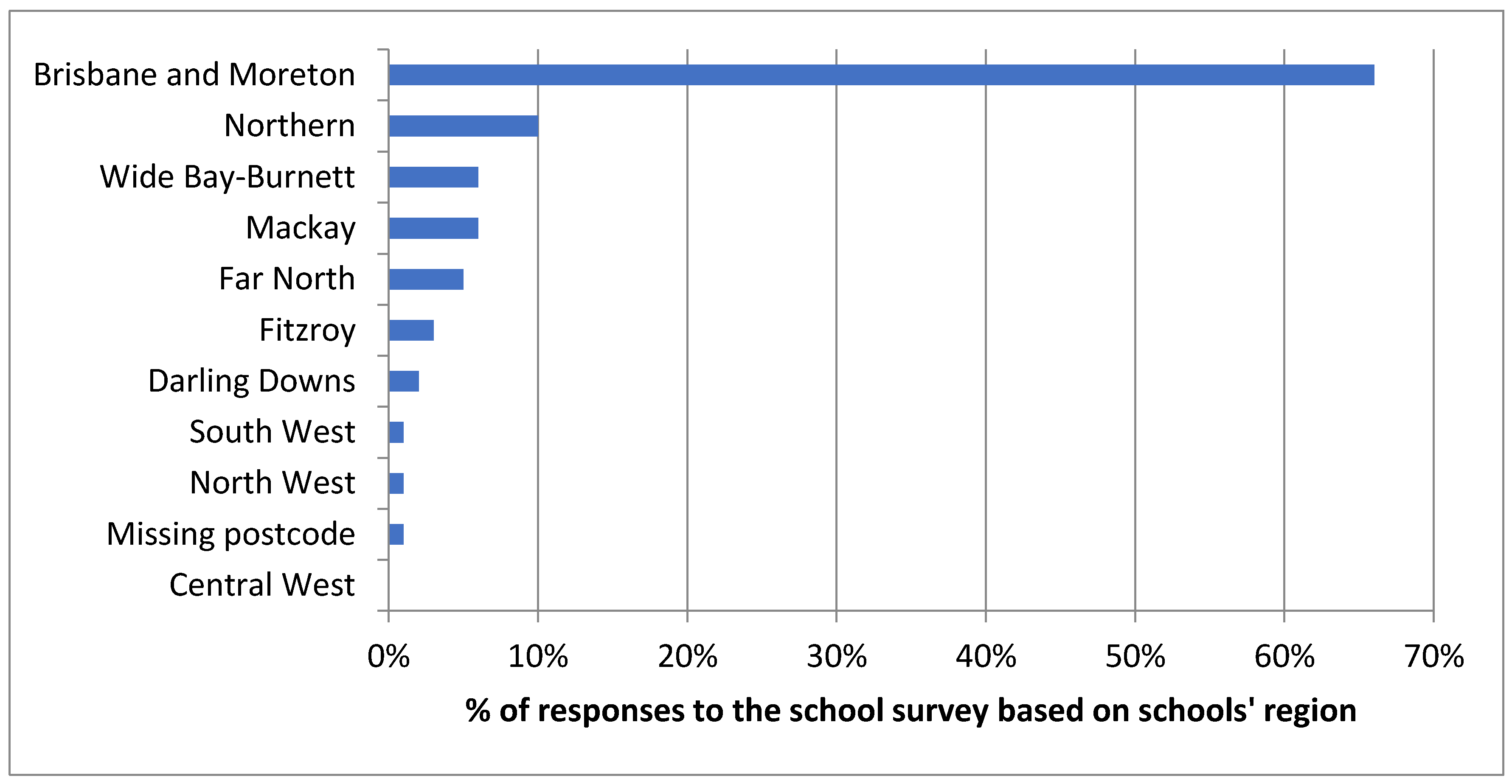
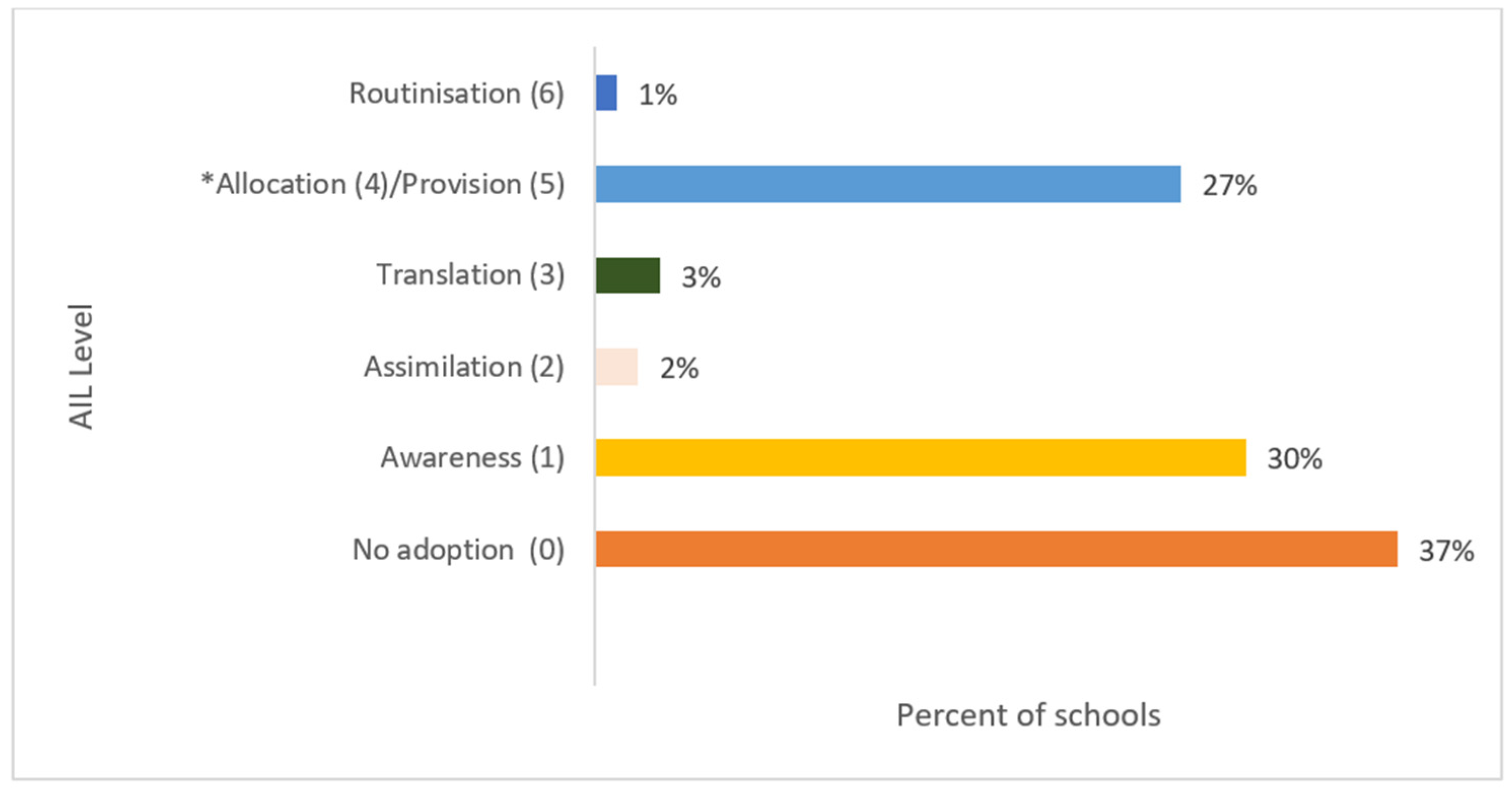
3.1.1. Impact on the School Sector (Survey 1) (Adoption and Penetration)
3.1.2. Impact on the Health Sector (Survey 2) (Adoption)
3.2. Qualitative
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Atlas: Child and Adolescent Mental Health Resources: Global Concerns, Implications for the Future; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Coppens, E.; Vermet, I.; Knaeps, J.; De Clerck, M.; De Schrijver, I.; Matot, J.P.; Van Audenhove, C. Adolescent Mental Health Care in Europe: State of the Art, Recommendations, and Guidelines by the ADOCARE Network; European Union: Brussels, Belgium, 2015. [Google Scholar]
- Hendriks, A.M.; Bartels, M.; Stevens, G.W.J.M.; Walsh, S.D.; Torsheim, T.; Elgar, F.J.; Finkenauer, C. National Child and Adolescent Health Policies as Indicators of Adolescent Mental Health: A Multilevel Analysis of 30 European Countries. J. Early Adolesc. 2019, 40, 537–565. [Google Scholar] [CrossRef]
- Du Rietz, E.; Jangmo, A.; Kuja-Halkola, R.; Chang, Z.; D’Onofrio, B.M.; Ahnemark, E.; Werner-Kiechle, T.; Larsson, H. Trajectories of healthcare utilization and costs of psychiatric and somatic multimorbidity in adults with childhood ADHD: A prospective register-based study. J. Child Psychol. Psychiatry 2020, 61, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.O.N.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.Y.E.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168. [Google Scholar]
- Whiteford, H.A.; Buckingham, W.J.; Harris, M.G.; Burgess, P.M.; Pirkis, J.E.; Barendregt, J.J.; Hall, W.D. Estimating treatment rates for mental disorders in Australia. Aust. Health Rev. 2014, 38, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Diminic, S.; Harris, M.; Sinclair, D.; Carstensen, G.; Degenhardt, L. Estimating the Community Prevalence and Treatment Rates for Mental and Substance Use Disorders in Queensland; The University of Queensland: Brisbane, Australia, 2013. [Google Scholar]
- Gore, F.M.; Bloem, P.J.; Patton, G.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global burden of disease in young people aged 10–24 years: A systematic analysis. Lancet 2011, 377, 2093–2102. [Google Scholar] [CrossRef]
- Campos, L.; Dias, P.; Duarte, A.; Veiga, E.; Dias, C.C.; Palha, F. Is It Possible to “Find Space for Mental Health” in Young People? Effectiveness of a School-Based Mental Health Literacy Promotion Program. Int. J. Environ. Res. Public Health 2018, 15, 1426. [Google Scholar] [CrossRef] [PubMed]
- Calear, A.L.; Werner-Seidler, A.; Torok, M.; Christensen, H. School-Based Prevention and Early Intervention Programs for Depression. In Handbook of School-Based Mental Health Promotion; Springer: Berlin/Heidelberg, Germany, 2018; pp. 279–297. [Google Scholar]
- McGorry, P.D.; Sartorius, N.; De Girolamo, G. Conclusions: From the Study of the Age of Onset to the Development of Age-Specific Interventions in Mental Health. In Age of Onset of Mental Disorders; Springer: Berlin/Heidelberg, Germany, 2018; pp. 255–261. [Google Scholar]
- National Research Council and Institute of Medicine. Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities; The National Academies Press: Washington, DC, USA, 2009.
- Fazel, M.; Hoagwood, K.; Stephan, S.; Ford, T. Mental health interventions in schools in high-income countries. Lancet Psychiatry 2014, 1, 377–387. [Google Scholar] [CrossRef]
- Bowman, S.; McKinstry, C.; McGorry, P. Youth mental ill health and secondary school completion in Australia: Time to act. Early Interv. Psychiatry 2016, 11, 277–289. [Google Scholar] [CrossRef]
- Queensland Mental Health Commission. Ed-Linq Program. 2015. Available online: https://www.qmhc.qld.gov.au/awareness-promotion/early-intervention-initiatives/ed-linq-program (accessed on 23 March 2020).
- Alliance, N.R.H. Demographic Composition of the Australian Population. 2021. Proportion of Each Jurisdictions Population in Each Remoteness Area. Available online: https://www.ruralhealth.org.au/book/demography (accessed on 17 July 2021).
- Raine, R.; Fitzpatrick, R.; Barratt, H.; Bevan, G.; Black, N.; Boaden, R.; Bower, P.; Campbell, M.; Denis, J.L.; Devers, K.; et al. Challenges, solutions and future directions in the evaluation of service innovations in health care and public health. Health Serv. Deliv. Res. 2016, 4. [Google Scholar] [CrossRef]
- Mendoza, J.; Wands, M.; Salvador-Carulla, L.; Hackett, M.; Najlepszy, L.F.; Fernandez, A. Evaluation of the Queensland Ed-LinQ Initiative: A School-Community Mental Health Initiative; Coolum Beach: Queensland, Australia, 2014. [Google Scholar]
- Cohen, G.; Schroeder, J.; Newson, R.; King, L.; Rychetnik, L.; Milat, A.J.; Bauman, A.E.; Redman, S.; Chapman, S. Does health intervention research have real world policy and practice impacts: Testing a new impact assessment tool. Health Res. Policy Syst. 2015, 13, 3. [Google Scholar] [CrossRef]
- Gill, K.J.; Campbell, E.; Gauthier, G.; Xenocostas, S.; Charney, D.; Macaulay, A.C. From policy to practice: Implementing frontline community health services for substance dependence-study protocol. Implement. Sci. 2014, 9, 108. [Google Scholar] [CrossRef][Green Version]
- Alonso-Trujillo, F.; Salinas-Pérez, J.A.; Gutiérrez-Colosía, M.R.; González-Caballero, J.L.; Salvador-Carulla, L. Impact assessment of a multisectoral plan for the promotion of health and social wellbeing in Andalusia (Spain). Gac. Sanit. 2019, 34, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Ratnapalan, S.; Uleryk, E. Organizational learning in health care organizations. Systems 2014, 2, 24–33. [Google Scholar] [CrossRef]
- Mathieson, A.; Grande, G.; Luker, K. Strategies, facilitators and barriers to implementation of evidence-based practice in community nursing: A systematic mixed-studies review and qualitative synthesis. Prim. Health Care Res. Dev. 2019, 20, E6. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef]
- Romero-Lopez-Alberca, C.; Alonso-Trujillo, F.; Almenara-Abellan, J.; JA, S.-P.; Ruiz Gutierrez-Colosia, M.; Conzales-Caballero, J.L.; Pinzon Pulido, S.; Salvador-Carulla, L. Maturity of a semi-automated classificaiton system to produce service directories in Social and Health Care (DESDE-AND): Maurity Assessment Study. J. Med. Internet. Res. 2021, 23, e24930. [Google Scholar] [CrossRef]
- Lukersmith, S. A Taxonomy of Case Management: Development, Dissemination and Impact. Ph.D. Thesis, University of Sydney, Sydney, Australia, 28 March 2017. [Google Scholar]
- Salinas-Perez, J.A.; Gutierrez-Colosia, M.R.; Romero Lopez-Alberca, C.; Poole, M.; Rodero-Cosano, M.L.; Garcia-Alonso, C.R.; Salvador-Carulla, L. Everything is on the map: Integrated Mental Health Atlases as support tools for service planning. SESPAS Report 2020. Gac. Sanit. 2020, 34, 11–19. [Google Scholar]
- Pinnock, H.; Barwick, M.; Carpenter, C.; Eldridge, S.; Grandes, G.; Griffiths, C.J.; Rycroft-Malone, J.; Meissner, P.; Murray, E.; Patel, A.; et al. Standards for Reporting Implementation Studies (StaRI) Statement. BMJ 2017, 356, i6795. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.; Salvador-Carulla, L. PERSPECTIVES: Accountability for Mental Health: The Australian Experience. J. Ment. Health Policy Econ. 2017, 20, 37–54. [Google Scholar] [PubMed]
- O’Reilly, M.; Svirydzenka, N.; Adams, S.; Dogra, N. Review of mental health promotion interventions in schools. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 647–662. [Google Scholar] [CrossRef]
- Raghavan, R.; Inkelas, M.; Franke, T.; Halfon, N. Administrative Barriers to the Adoption of High-Quality Mental Health Services for Children in Foster Care: A National Study. Adm. Policy Ment. Health Ment. Health Serv. Res. 2007, 34, 191–201. [Google Scholar] [CrossRef]
- Weare, K.; Nind, M. Mental health promotion and problem prevention in schools: What does the evidence say? Health Promot. Int. 2011, 26, i29–i69. [Google Scholar] [CrossRef] [PubMed]
- Slee, P.T.; Dix, K.L.; Askell-Williams, H. Whole-school mental health promotion in Australia. Int. J. Emot. Educ. 2011, 3, 37–49. [Google Scholar]
- Sarma, H.; Uddin, M.F.; Islam, M.A.; Rahman, M.; Aaron, G.J.; Harbour, C.; Banwell, C.; Ahmed, T. Use of concurrent evaluation to improve implementation of a home fortification programme in Bangladesh: A methodological innovation. Public Health Nutr. 2020, 24, S37–S47. [Google Scholar] [CrossRef] [PubMed]
- Domitrovich, C.E.; Bradshaw, C.P.; Poduska, J.M.; Hoagwood, K.; Buckley, J.A.; Olin, S.; Romanelli, L.H.; Leaf, P.J.; Greenberg, M.T.; Ialongo, N.S. Maximizing the Implementation Quality of Evidence-Based Preventive Interventions in Schools: A Conceptual Framework. Adv. Sch. Ment. Health Promot. 2008, 1, 6–28. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.; Hickie, I. Depression in Young People: A National School-Based Initiative for Prevention, Early Intervention and Pathways for Care. Australas. Psychiatry 2002, 10, 134–138. [Google Scholar] [CrossRef]
- Jones, J.E.; Scanlon, K.; Raphael, B.; Hillin, A.; McAlpine, R.; Critchley, A.; Stonehouse, R.; McKie, D.; Kerr-Roubicek, H.; Meerman, G. Health and Education Working Together: The New South Wales School-Link Initiative. Int. J. Ment. Health Promot. 2002, 4, 36–43. [Google Scholar] [CrossRef]
- State Government Victoria. CAMHS and Schools-Early Action Program (CASEA). 2006. Available online: http://www.austin.org.au/CASEA/ (accessed on 21 July 2021).
- Maloney, D.; Walter, G. Contribution of ’school-link’ to an area mental health service. Australas Psychiatry 2005, 13, 399–402. [Google Scholar] [CrossRef]
- New South Wales Government. Getting on Track in Time. Available online: http://www.keepthemsafe.nsw.gov.au/initiatives/prevention_and_early_intervention/getting_on_track_in_time (accessed on 29 June 2016).
- Maloney, D.; Jones, J.; Walter, G.; Davenport, R. Addressing Mental Health Concerns in Schools: Does School-Link Achieve Its Aims? Australas. Psychiatry 2008, 16, 48–53. [Google Scholar] [CrossRef]
- The Common Benefits of School Based Mental Health Programs: A Systematic Review. Available online: https://sophia.stkate.edu/msw_papers/757 (accessed on 21 July 2021).
- Hornik, R.C. Epilogue: Evaluation design for public health communication programs. In Public Health Communication: Evidence for Behavior Change; Lawrence Erllbaum Associates: Mahwah, NJ, USA, 2002; pp. 385–405. [Google Scholar]
- Noar, S.M. A 10-Year Retrospective of Research in Health Mass Media Campaigns: Where Do We Go From Here? J. Health Commun. 2006, 11, 21–42. [Google Scholar] [CrossRef]
- Furst, M.A.; Bagheri, N.; Salvador-Carulla, L. An ecosystems approach to mental health services research. BJPsych. Int. 2021, 18, 23–25. [Google Scholar] [CrossRef]
- Hornik, R.; Yanovitzky, I. Using Theory to Design Evaluations of Communication Campaigns: The Case of the National Youth Anti-Drug Media Campaign. Commun. Theory 2003, 13, 204–224. [Google Scholar] [CrossRef]
- Mealing, N.M.; Banks, E.; Jorm, L.R.; Steel, D.G.; Clements, M.S.; Rogers, K.D. Investigation of relative risk estimates from studies of the same population with contrasting response rates and designs. BMC Med Res. Methodol. 2010, 10, 1–12. [Google Scholar] [CrossRef]
- Morton, S.M.; Bandara, D.K.; Robinson, E.M.; Carr, P.E.A. In the 21stCentury, what is an acceptable response rate? Aust. N. Z. J. Public Health 2012, 36, 106–108. [Google Scholar] [CrossRef]
- Milat, A.J.; Laws, R.; King, L.; Newson, R.; Rychetnik, L.; Rissel, C.; Bauman, A.E.; Redman, S.; Bennie, J. Policy and practice impacts of applied research: A case study analysis of the New South Wales Health Promotion Demonstration Research Grants Scheme 2000–2006. Health Res. Policy Syst. 2013, 11, 5. [Google Scholar] [CrossRef][Green Version]
- Kroelinger, C.; Ehrenthal, D. Translating Policy to Practice and Back Again: Implementing a Preconception Program in Delaware. Women’s Health Issues 2008, 18, S74–S80. [Google Scholar] [CrossRef]
- Slater, H.; Briggs, A.M.; Smith, A.J.; Bunzli, S.; Davies, S.J.; Quintner, J.L. Implementing Evidence-Informed Policy into Practice for Health Care Professionals Managing People with Low Back Pain in Australian Rural Settings: A Preliminary Prospective Single-Cohort Study. Pain Med. 2014, 15, 1657–1668. [Google Scholar] [CrossRef] [PubMed]
- Wiljer, D.; Le, L.; Logan, H.; Neligan, D.; Brierley, J. From policy to practice: Assessing the impact of staging policies for recording cancer stage across Canada. Health Q. 2008, 11, 98–103. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thoroddsen, A.; Ehnfors, M. Putting policy into practice: Pre-and posttests of implementing standardized languages for nursing documentation. J. Clin. Nurs. 2007, 16, 1826–1838. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level of Adoption | Definition | Questions to Respondents |
|---|---|---|
| 0. No Adoption (no impact) | The Ed-LinQ initiative was not adopted (had no impact) in the target school. |
|
| 1. Awareness | The target schools and specific decision makers within the school/health service providers are cognizant of the Ed-LinQ initiative, have taken action to improve its knowledge on the topic or have received or provided feedback on the information delivered. |
|
| 2. Assimilation | There is evidence that the target school and specific decision makers within the school have incorporated the Ed-LinQ initiative into their own existing knowledge-base and organisational strategy. |
|
| 3. Conversion | The target schools have transferred the Ed-LinQ initiative into policy action in legislation, plans, policy programs, regulatory norms, and/or official indicators. |
|
| (4. Allocation and) 5. Provision | The translation of the new knowledge has had an impact on financing, budgeting, funding, and/or resource allocation in the target audience. |
|
| Care delivery, including services, interventions and/or technologies directly related to the Ed-LinQ initiative has been made available and it is used by the target population in the school environment. | ||
| 6. Routinisation (monitoring) | The target school has incorporated the Ed-LinQ initiative into its own assessment, surveillance and monitoring systems. |
|
| Perceived Outcome | Percentage of Schools’ Respondents Reporting This Perceived Outcome |
|---|---|
| Improvement in students’ access to mental health resources | 64% |
| Improvement in students’ attendance | 27% |
| Improvement in students’ performance | 26% |
| Better management of students with mental health issues | 56% |
| Increased capacity of staff to support students | 73% |
| Improved staff knowledge | 67% |
| Enhancement of staff access to mental health resources | 68% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvador-Carulla, L.; Fernandez, A.; Sarma, H.; Mendoza, J.; Wands, M.; Gandre, C.; Chevreul, K.; Lukersmith, S. Impact of Ed-LinQ: A Public Policy Strategy to Facilitate Engagement between Schools and the Mental Health Care System in Queensland, Australia. Int. J. Environ. Res. Public Health 2021, 18, 7924. https://doi.org/10.3390/ijerph18157924
Salvador-Carulla L, Fernandez A, Sarma H, Mendoza J, Wands M, Gandre C, Chevreul K, Lukersmith S. Impact of Ed-LinQ: A Public Policy Strategy to Facilitate Engagement between Schools and the Mental Health Care System in Queensland, Australia. International Journal of Environmental Research and Public Health. 2021; 18(15):7924. https://doi.org/10.3390/ijerph18157924
Chicago/Turabian StyleSalvador-Carulla, Luis, Ana Fernandez, Haribondhu Sarma, John Mendoza, Marion Wands, Coralie Gandre, Karine Chevreul, and Sue Lukersmith. 2021. "Impact of Ed-LinQ: A Public Policy Strategy to Facilitate Engagement between Schools and the Mental Health Care System in Queensland, Australia" International Journal of Environmental Research and Public Health 18, no. 15: 7924. https://doi.org/10.3390/ijerph18157924
APA StyleSalvador-Carulla, L., Fernandez, A., Sarma, H., Mendoza, J., Wands, M., Gandre, C., Chevreul, K., & Lukersmith, S. (2021). Impact of Ed-LinQ: A Public Policy Strategy to Facilitate Engagement between Schools and the Mental Health Care System in Queensland, Australia. International Journal of Environmental Research and Public Health, 18(15), 7924. https://doi.org/10.3390/ijerph18157924