
Feasibility and Efficacy of the “FUNPALs Playgroup” Intervention to Improve Toddler Dietary and Activity Behaviors: A Pilot Randomized Controlled Trial

 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Recruitment and Participants
2.3. Sample Size and Randomization
2.4. Procedure
2.5. Theoretical Framework
2.6. Experimental Group
2.7. Control Group
2.8. Process Evaluation Outcome Measurements
2.8.1. Facilitators and Barriers of Recruitment
2.8.2. Demographics
2.8.3. Participants Engagement
2.8.4. Facilitators and Barriers of Retention and Perceived Impact
- “What motivated you to come to playgroup/class every week?”;
- “What barriers did you face coming to playgroup/class every week?”;
- “To what extent did the playgroup/class help your family make changes in nutrition/physical activity/parenting?”
2.8.5. Fidelity
2.9. Preliminary Effect Outcome Measurements
2.9.1. Dietary Intake of Children
2.9.2. Children’s Activity and Sleep
2.9.3. Feeding Practices
2.9.4. Home Environment
2.9.5. Anthropometrics
2.10. Statistical Analysis
3. Results
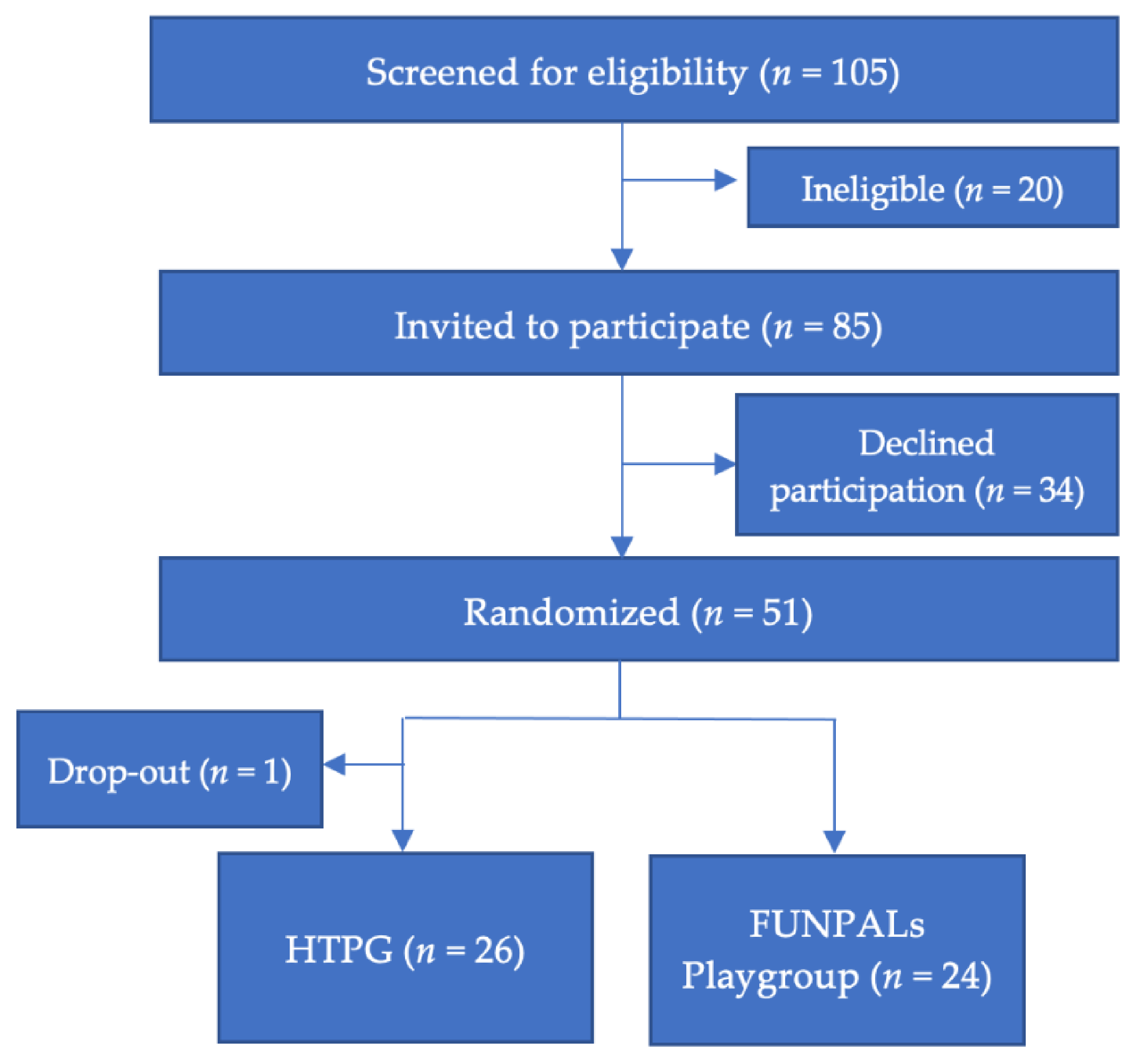
3.1. Sample Characteristics
3.2. Recruitment and Retention: Facilitators and Barriers
3.3. Perceived Impact
3.4. Fidelity
3.5. Preliminary Effects
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kelsey, M.M.; Zaepfel, A.; Bjornstad, P.; Nadeau, K.J. Age-related consequences of childhood obesity. Gerontology 2014, 60, 222–228. [Google Scholar] [CrossRef]
- Ogden, C.L.; Fryar, C.D.; Hales, C.M.; Carroll, M.D.; Aoki, Y.; Freedman, D.S. Differences in obesity prevalence by demographics and urbanization in US children and adolescents, 2013-2016. JAMA 2018, 319, 2410–2418. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, E.S.; Clifford, L.M.; Stark, L.J. Obesity in preschoolers: Behavioral correlates and directions for treatment. Obesity 2012, 20, 3–29. [Google Scholar] [CrossRef]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef]
- McGuire, S. Institute of Medicine (IOM) Early Childhood Obesity Prevention Policies. Washington, DC: The National Academies Press; 2011. Adv. Nutr. 2012, 3, 56–57. [Google Scholar] [CrossRef] [PubMed]
- CDC. Toddlers (1-2 Years of Age): Developmental Milestones. 2021. Available online: https://www.cdc.gov/ncbddd/childdevelopment/positiveparenting/toddlers.html (accessed on 22 February 2021).
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120, S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Lee, E.Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic review of the relationships between physical activity and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 854. [Google Scholar] [CrossRef]
- Chaput, J.P.; Gray, C.E.; Poitras, V.J.; Carson, V.; Gruber, R.; Birken, C.S.; MacLean, J.E.; Aubert, S.; Sampson, M.; Tremblay, M.S. Systematic review of the relationships between sleep duration and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 855. [Google Scholar] [CrossRef]
- Bandura, A. Human agency in social cognitive theory. Am. Psychol. 1989, 44, 1175–1184. [Google Scholar] [CrossRef]
- Yavuz, H.M.; van Ijzendoorn, M.H.; Mesman, J.; van der Veek, S. Interventions aimed at reducing obesity in early childhood: A meta-analysis of programs that involve parents. J. Child Psychol. Psychiatry 2015, 56, 677–692. [Google Scholar] [CrossRef] [PubMed]
- Volger, S.; Rigassio Radler, D.; Rothpletz-Puglia, P. Early childhood obesity prevention efforts through a life course health development perspective: A scoping review. PLoS ONE 2018, 13, e0209787. [Google Scholar] [CrossRef]
- Skelton, J.A.; Buehler, C.; Irby, M.B.; Grzywacz, J.G. Where are family theories in family-based obesity treatment?: Conceptualizing the study of families in pediatric weight management. Int. J. Obes. 2012, 36, 891–900. [Google Scholar] [CrossRef]
- Pratt, K.J.; Skelton, J.A.; Eneli, I.; Coliler, D.N.; Lazorick, S. Providers’ involvement of parents, families, and family dynamics in youth weight management programs. Glob. Pediatr. Health 2018, 5, 2333794x18817134. [Google Scholar] [CrossRef] [PubMed]
- Kitzman-Ulrich, H.; Wilson, D.K.; St George, S.M.; Lawman, H.; Segal, M.; Fairchild, A. The integration of a family systems approach for understanding youth obesity, physical activity, and dietary programs. Clin. Child Fam. Psychol. Rev. 2010, 13, 231–253. [Google Scholar] [CrossRef]
- Morgan, P.J.; Jones, R.A.; Collins, C.E.; Hesketh, K.D.; Young, M.D.; Burrows, T.L.; Magarey, A.M.; Brown, H.L.; Hinkley, T.; Perry, R.A.; et al. Practicalities and research considerations for conducting childhood obesity prevention interventions with families. Children 2016, 3. [Google Scholar] [CrossRef]
- Miller, A.L.; Miller, S.E.; Clark, K.M. Child, caregiver, family, and social-contextual factors to consider when implementing parent-focused child feeding interventions. Curr. Nutr. Rep. 2018, 7, 303–309. [Google Scholar] [CrossRef]
- Henchy, G. Making WIC Work Better: Strategies to Reach More Women and Children and Strengthen Benefits Use. Food Research Action Center. 2019. Available online: https://frac.org/wp-content/uploads/Making-WIC-Work-Better-Exec-Summary-FNL.pdf. (accessed on 30 November 2020).
- Gabor, V.; Cates, S.; Gleason, S.; Long, V.; Aponte Clarke, G.; Blitstein, J.; Williams, P.; Bell, L.; Hersey, J.; Ball, M. SNAP Education and Evaluation (Wave I). Final Report; United States Department of Agriculture: Alexandria, VA, USA, 2021; Available online: www.fns.usda.gov/ora (accessed on 30 November 2020).
- IBISWorld. Children’s Fitness Center Franchises in the US Industry Trends (2015–2020). Available online: https://www.ibisworld.com/united-states/market-research-reports/childrens-fitness-center-franchises-industry (accessed on 30 November 2020).
- The Top 10 Children’s Fitness Franchises. Entrepreneur. 2011. Available online: https://www.entrepreneur.com/slideshow/217871 (accessed on 30 November 2020).
- McLean, K.; Edwards, S.; Evangelou, M.; Skouteris, H.; Harrison, L.J.; Hemphill, S.A.; Sullivan, P.; Lambert, P. Playgroups as sites for parental education. J. Early Child. Res. 2017, 15, 227–237. [Google Scholar] [CrossRef]
- Hancock, K.; Lawrence, D.; Mitrou, F.; Zarb, D.; Berthelsen, D.; Nicholson, J.; Zubrick, S. The association between playgroup participation, learning competence and social-emotional wellbeing for children aged four–five years in Australia. Australas. J. Early Child. 2012, 37, 72–81. [Google Scholar] [CrossRef]
- Hancock, K.J.; Cunningham, N.K.; Lawrence, D.; Zarb, D.; Zubrick, S.R. Playgroup Participation and Social Support Outcomes for Mothers of Young Children: A Longitudinal Cohort Study. PLoS ONE 2015, 10, e0133007. [Google Scholar] [CrossRef]
- Mose, T.R. The Playdate: Parents, Children, and the New Expectations of Play; NYU Press: New York, NY, USA, 2016. [Google Scholar]
- Shanley, J.R.; Niec, L.N. Coaching parents to change: The impact of in vivo feedback on parents’ acquisition of skills. J. Clin. Child. Adolesc. Psychol. 2010, 39, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Niec, L.N.; Peer, S.O.; Jent, J.F.; Weinstein, A.; Gisbert, P.; Simpson, G. Successful therapist-parent coaching: How in vivo feedback relates to parent engagement in parent-child interaction therapy. J. Clin. Child. Adolesc. Psychol. 2017, 46, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Raising Children: The Australian Parenting Website. Available online: https://raisingchildren.net.au/toddlers/play-learning/playing-with-others/about-playgroups#finding-a-local-playgroup-nav-title (accessed on 9 April 2020).
- Weber, D.; Rissel, C.; Hector, D.; Wen, L.M. Supported playgroups as a setting for promoting physical activity of young children: Findings from a feasibility study in south-west Sydney, Australia. J. Paediatr. Child. Health 2014, 50, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Yogman, M.; Garner, A.; Hutchinson, J.; Hirsh-Pasek, K.; Golinkoff, R.M. The power of play: A pediatric role in enhancing development in young children. Pediatrics 2018, 142. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot. Feasibility Stud. 2016, 2, 64. [Google Scholar] [CrossRef] [PubMed]
- US Census Bureau. 2013-2017 American Community Survey 5-Year Estimates; American Community Survey: Suitland, MA, USA, 2018. [Google Scholar]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef]
- Ortiz, C.; Del Vecchio, T. Cultural diversity: Do we need a new wake-up call for parent training? Behav. Ther. 2013, 44, 443–458. [Google Scholar] [CrossRef]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G. Intervention mapping: A process for developing theory and evidence-based health education programs. Health Educ. Behav. 1998, 25, 545–563. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inquiry 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Swindle, T.M.; Ward, W.L.; Whiteside-Mansell, L. Facebook: The use of social media to engage parents in a preschool obesity prevention curriculum. J. Nutr. Educ. Behav. 2018, 50. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Duncan, T.; Tammen, V.V. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: A confirmatory factor analysis. Res. Q Exerc. Sport 1989, 60, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Tsigilis, N.; Theodosiou, A. Temporal stability of the intrinsic motivation inventory. Percept Mot. Skills 2003, 97, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry & Research Design: Choosing among Five Approaches, 4th ed.; SAGE: Los Angeles, CA, USA, 2018; 459p. [Google Scholar]
- Aguilar, S.S.; Wengreen, H.J.; Lefevre, M.; Madden, G.J.; Gast, J. Skin carotenoids: A biomarker of fruit and vegetable intake in children. J. Acad. Nutr. Diet. 2014, 114, 1174–1180. [Google Scholar] [CrossRef]
- Kaiser, L.L.; Aguilera, A.L.; Horowitz, M.; Lamp, C.; Johns, M.; Gomez-Camacho, R.; Ontai, L.; de la Torre, A. Correlates of food patterns in young Latino children at high risk of obesity. Public Health Nutr. 2015, 18, 3042–3050. [Google Scholar] [CrossRef][Green Version]
- Radtke, M.D.; Pitts, S.J.; Jahns, L.; Firnhaber, G.C.; Loofbourrow, B.M.; Zeng, A.; Scherr, R.E. Criterion-related validity of spectroscopy-based skin carotenoid measurements as a proxy for fruit and vegetable intake: A systematic review. Adv. Nutr. 2020, 11, 1282–1299. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Gubbels, J.; De Bourdeaudhuij, I.; Cardon, G. Feasibility and validity of accelerometer measurements to assess physical activity in toddlers. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 67. [Google Scholar] [CrossRef]
- Bisson, M.; Tremblay, F.; Pronovost, E.; Julien, A.S.; Marc, I. Accelerometry to measure physical activity in toddlers: Determination of wear time requirements for a reliable estimate of physical activity. J. Sports Sci. 2019, 37, 298–305. [Google Scholar] [CrossRef]
- Hnatiuk, J.A.; Lamb, K.E.; Ridgers, N.D.; Salmon, J.; Hesketh, K.D. Changes in volume and bouts of physical activity and sedentary time across early childhood: A longitudinal study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 42. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.S.; Rollins, B.Y.; Kugler, K.C.; Birch, L.L.; Marini, M.E. Development of a theory-based questionnaire to assess structure and control in parent feeding (SCPF). Int. J. Behav. Nutr. Phys. Act. 2017, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Bryant, M.J.; Ward, D.S.; Hales, D.; Vaughn, A.; Tabak, R.G.; Stevens, J. Reliability and validity of the Healthy Home Survey: A tool to measure factors within homes hypothesized to relate to overweight in children. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 23. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Nelson, M.C.; Lytle, L.; Moe, S.; Heitzler, C.; Pasch, K.E. The validation of a home food inventory. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 55. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.E.; Miller, A.L.; Lumeng, J.C.; Chervin, R.D. Sleep environments and sleep durations in a sample of low-income preschool children. J. Clin. Sleep Med. 2014, 10, 299–305. [Google Scholar] [CrossRef]
- Cepni, A.B.; Taylor, A.; Thompson, D.; Moran, N.E.; Olvera, N.; O’Connor, D.P.; Johnston, C.A.; Ledoux, T.A. Exploring qualities of ethnically diverse parents associated with healthy home environment of toddlers. Appetite 2021, in press. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988; Volume 177. [Google Scholar]
- WHO. Child Growth Standards based on length/height, weight and age. Acta. Paediatr. 2006, 95, 76–85. [Google Scholar]
- Furlong, K.R.; Anderson, L.N.; Kang, H.; Lebovic, G.; Parkin, P.C.; Maguire, J.L.; O’Connor, D.L.; Birken, C.S. BMI-for-age and weight-for-length in children 0 to 2 years. Pediatrics 2016, 138. [Google Scholar] [CrossRef]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- McGee, M.; Bergasa, N.V. Imputing Missing Data in Clinical Pilot Studies. Southern Methodist University: Dallas, TX, USA, 2005. [Google Scholar]
- Beretta, L.; Santaniello, A. Nearest neighbor imputation algorithms: A critical evaluation. BMC Med. Inform. Decis. Mak. 2016, 16 (Suppl. S3), 74. [Google Scholar] [CrossRef]
- Lee, C.Y.; Ledoux, T.A.; Johnston, C.A.; Ayala, G.X.; O’Connor, D.P. Association of parental body mass index (BMI) with child’s health behaviors and child’s BMI depend on child’s age. BMC Obesity 2019, 6, 11. [Google Scholar] [CrossRef]
- Taghizadeh, S.; Farhangi, M.A. The effectiveness of pediatric obesity prevention policies: A comprehensive systematic review and dose-response meta-analysis of controlled clinical trials. J. Transl. Med. 2020, 18, 480. [Google Scholar] [CrossRef] [PubMed]
- Heerman, W.J.; Sommer, E.C.; Qi, A.; Burgess, L.E.; Mitchell, S.J.; Samuels, L.R.; Martin, N.C.; Barkin, S.L. Evaluating dose delivered of a behavioral intervention for childhood obesity prevention: A secondary analysis. BMC Public Health 2020, 20, 885. [Google Scholar] [CrossRef] [PubMed]
- Neal, J.W.; Neal, Z.P.; VanDyke, E.; Kornbluh, M. Expediting the analysis of qualitative data in evaluation: A procedure for the rapid identification of themes from audio recordings (RITA). Am. J. Eval. 2015, 36, 118–132. [Google Scholar] [CrossRef]
- Kerr, C.; Nixon, A.; Wild, D. Assessing and demonstrating data saturation in qualitative inquiry supporting patient-reported outcomes research. Expert Rev. Pharm. Outcomes Res. 2010, 10, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code saturation versus meaning saturation: How many interviews are enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef]
- Pathirana, T.; Stoneman, R.; Lamont, A.; Harris, N.; Lee, P. Impact evaluation of “Have Fun-Be Healthy” program: A community based health promotion intervention to prevent childhood obesity. Health Promot. J. Aust. 2018, 29, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Arigo, D.; Pagoto, S.; Carter-Harris, L.; Lillie, S.E.; Nebeker, C. Using social media for health research: Methodological and ethical considerations for recruitment and intervention delivery. Digit. Health 2018, 4, 2055207618771757. [Google Scholar] [CrossRef]
- Whitaker, C.; Stevelink, S.; Fear, N. The use of Facebook in recruiting participants for health research purposes: A systematic review. J. Med. Int. Res. 2017, 19, e290. [Google Scholar] [CrossRef]
- Fuller, A.B.; Byrne, R.A.; Golley, R.K.; Trost, S.G. Supporting healthy lifestyle behaviours in families attending community playgroups: Parents’ perceptions of facilitators and barriers. BMC Public Health 2019, 19, 1740. [Google Scholar] [CrossRef]
- Williams, N.A.; Coday, M.; Somes, G.; Tylavsky, F.A.; Richey, P.A.; Hare, M. Risk factors for poor attendance in a family-based pediatric obesity intervention program for young children. J. Dev. Behav. Pediatr. 2010, 31, 705–712. [Google Scholar] [CrossRef]
- Skelton, J.A.; Beech, B.M. Attrition in paediatric weight management: A review of the literature and new directions. Obes. Rev. 2011, 12, e273–e281. [Google Scholar] [CrossRef]
- Jago, R.; Steeds, J.K.; Bentley, G.F.; Sebire, S.J.; Lucas, P.J.; Fox, K.R.; Stewart-Brown, S.; Turner, K.M. Designing a physical activity parenting course: Parental views on recruitment, content and delivery. BMC Public Health 2012, 12, 356. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Lovell, A.; Bulloch, R.; Wall, C.R.; Grant, C.C. Quality of food-frequency questionnaire validation studies in the dietary assessment of children aged 12 to 36 months: A systematic literature review. J. Nutr. Sci. 2017, 6, e16. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.M.; Scherr, R.E.; Linnell, J.D.; Ermakov, I.V.; Gellermann, W.; Jahns, L.; Keen, C.L.; Miyamoto, S.; Steinberg, F.M.; Young, H.M.; et al. Evaluating the relationship between plasma and skin carotenoids and reported dietary intake in elementary school children to assess fruit and vegetable intake. Arch. Biochem. Biophys. 2015, 572, 73–80. [Google Scholar] [CrossRef]
- Scarmo, S.; Henebery, K.; Peracchio, H.; Cartmel, B.; Lin, H.; Ermakov, I.V.; Gellermann, W.; Bernstein, P.S.; Duffy, V.B.; Mayne, S.T. Skin carotenoid status measured by resonance Raman spectroscopy as a biomarker of fruit and vegetable intake in preschool children. Eur. J. Clin. Nutr. 2012, 66, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Jurkowski, J.M.; Lawson, H.A.; Green Mills, L.L.; Wilner, P.G., 3rd; Davison, K.K. The empowerment of low-income parents engaged in a childhood obesity intervention. Fam. Commun. Health 2014, 37, 104–118. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Lesson | Parenting Topic | Activity Topic | Nutrition Topic |
|---|---|---|---|
| 1 | Active listening | MVPA recommendations | Role of parents at mealtimes |
| 2 | Imitation play | Types of activities for health | Importance of fruit |
| 3 | Descriptive communication | Guided activity | Eat more veggies! |
| 4 | Positive reinforcement | Unguided activity | Importance of whole grains |
| 5 | Giving your child good directions | Activity in the home | Reducing fat intake |
| 6 | Using the choices technique | Sleep | Reducing sugar |
| 7 | Delivering consequences | Reducing sedentary activity | Picky eating |
| 8 | Using timeouts effectively | Limiting screen time | Meal planning and grocery shopping |
| 9 | Dealing with tantrums | Overcoming barriers to activity | Healthy home environment |
| 10 | Review | Review | Review |
| Total (n = 50, 100%) | FP (n = 24, 48%) | HTPG (n = 26, 52%) | p | |
|---|---|---|---|---|
| Parental Characteristics | ||||
| Age (years), mean (SD) | 31.7 (5.7) | 31.5 (6.1) | 31.8 (5.4) | 0.842 |
| Female, n (%) | 42 (84) | 19 (79.2) | 23 (88.5) | 0.199 |
| Race/ethnicity, n (%) | 0.706 | |||
| Hispanic/Latino | 19 (38) | 10 (41.7) | 9 (34.6) | |
| Non-Hispanic White | 6 (12) | 3 (12.5) | 3 (11.5) | |
| Non-Hispanic African American | 16 (32) | 8 (33.3) | 8 (30.8) | |
| Asian | 7 (14) | 2 (8.3) | 5 (19.2) | |
| Other | 1 (2) | 0 (0) | 1 (3.8) | |
| Marital Status, n (%) | 0.221 | |||
| Married or cohabiting | 30 (60) | 12 (50) | 18 (69.2) | |
| Single | 19 (38) | 11 (45.8) | 8 (30.8) | |
| Education status, n (%) | 0.545 | |||
| High school graduate | 5 (10) | 3 (12.5) | 2 (7.7) | |
| Some college or technical school | 14 (28) | 8 (33.3) | 6 (23.1) | |
| College graduate | 31 (62) | 13 (54.2) | 18 (69.2) | |
| Household annual income, n (%) | 0.062 | |||
| <24,999 USD | 14 (28) | 10 (41.7) | 4 (15.4) | |
| 25,000 to 49,999 USD | 14 (28) | 6 (25) | 8 (30.8) | |
| ≥50,000 USD | 17 (34) | 5 (20.8) | 12 (46.2) | |
| BMI (kg/m2), mean (SD) | 28.4 (6.4) | 27.3 (6.3) | 29.4 (6.4) | 0.259 |
| Toddler characteristics | ||||
| Age (months), mean (SD) | 22.6 (6.6) | 22.3 (6.8) | 22.9 (6.5) | 0.722 |
| Female, n (%) | 21 (42) | 10 (41.7) | 11 (42.3) | 0.963 |
| BMI-for-age percentile, mean (SD) | 76.2 (25.8) | 70.8 (32.2) | 80.9 (17.8) | 0.191 |
| Toddler outcomes, mean (SD) | ||||
| Snack intake | 17.9 (4.9) | 19.5 (4.8) | 16.5 (4.6) | 0.028 |
| FV intake (FFQ) | 32.1 (8.4) | 30.9 (7.5) | 33.3 (9.2) | 0.321 |
| SSB intake | 4.5 (2) | 5 (2.2) | 4 (1.8) | 0.083 |
| FV intake (SCS) | 253.4 (121.8) | 276.9 (126.9) | 231.7 (115.2) | 0.193 |
| MVPA (min) | 26.2 (14.7) | 27.1 (16.1) | 25.4 (13.5) | 0.677 |
| Sleep (min) | 612.2 (51.5) | 607.7 (52.8) | 616.4 (50.9) | 0.555 |
| Adjusted Difference within Groups | Adjusted Difference between Groups | ||
|---|---|---|---|
| FUNPALs (T) (n = 24) | HTPG (C) (n = 26) | T vs. C | |
| Outcome Variable | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) |
| Snack intake | −1.4 (−3.60 to −1.04) p = 0.207 | 0.6 (−1.00 to 2.16) p = 0.458 | −0.4 (−1.71 to 0.90); p = 0.536 G × T; p = 0.137 |
| FV intake (FFQ) | 1.2 (−2.06 to 4.37) p = 0.466 | −1.8 (−5.06 to 1.46) p = 0.266 | −0.3 (−2.56 to 1.91); p = 0.772 G × T; p = 0.190 |
| SSB intake ** | −0.7 (−1.35 to −0.14) p = 0.018 | 1.1 (0.47 to 1.72) p = 0.001 | 0.2 (−0.25 to 0.60); p = 0.407 G × T; p < 0.001 |
| FV intake (SCS) * | 70.7 (−1.29 to 142.75) p = 0.054 | 51.6 (−16.8 to 119.98) p = 0.133 | 61.2 (12.79 to 109.51); p = 0.014 G × T; p = 0.692 |
| MVPA (min) | −2.9 (−9.07 to 3.30) p = 0.344 | 7.1 (−3.18 to 17.47) p = 0.166 | 2.1 (−3.86 to 8.12); p = 0.479 G × T; p = 0.099 |
| Sleep (min) | 6.9 (−13.24 to 27.00) p = 0.486 | −18.2 (−39.02 to 2.71) p = 0.085 | −5.6 (−19.80 to 8.53); p = 0.428 G × T; p = 0.082 |
| Parenting Mediators | |||
| SF: Limit-setting | 0.2 (−1.53 to 1.90) p = 0.827 | 0.4 (−1.65 to 2.54) p = 0.667 | 0.3 (−1.02 to 1.65); p = 0.639 G × T; p = 0.846 |
| SF: Consistency | 1.6 (−1.20 to 4.34) p = 0.253 | 0.7 (−1.93 to 3.43) p = 0.570 | 1.2 (−0.72 to 3.04); p = 0.220 G × T; p = 0.663 |
| Home Environment Mediators | |||
| Home Environment Composite Score | −3.7 (−8.01 to 0.66) p = 0.093 | 0.6 (−3.82 to 5.08) p = 0.773 | −1.5 (−4.56 to 1.51); p = 0.319 G × T; p = 0.161 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cepni, A.B.; Taylor, A.; Crumbley, C.; Thompson, D.; Moran, N.E.; Olvera, N.; O’Connor, D.P.; Arlinghaus, K.R.; Johnston, C.A.; Ledoux, T.A. Feasibility and Efficacy of the “FUNPALs Playgroup” Intervention to Improve Toddler Dietary and Activity Behaviors: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 7828. https://doi.org/10.3390/ijerph18157828
Cepni AB, Taylor A, Crumbley C, Thompson D, Moran NE, Olvera N, O’Connor DP, Arlinghaus KR, Johnston CA, Ledoux TA. Feasibility and Efficacy of the “FUNPALs Playgroup” Intervention to Improve Toddler Dietary and Activity Behaviors: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(15):7828. https://doi.org/10.3390/ijerph18157828
Chicago/Turabian StyleCepni, Aliye B., Ashley Taylor, Christine Crumbley, Debbe Thompson, Nancy E. Moran, Norma Olvera, Daniel P. O’Connor, Katherine R. Arlinghaus, Craig A. Johnston, and Tracey A. Ledoux. 2021. "Feasibility and Efficacy of the “FUNPALs Playgroup” Intervention to Improve Toddler Dietary and Activity Behaviors: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 15: 7828. https://doi.org/10.3390/ijerph18157828
APA StyleCepni, A. B., Taylor, A., Crumbley, C., Thompson, D., Moran, N. E., Olvera, N., O’Connor, D. P., Arlinghaus, K. R., Johnston, C. A., & Ledoux, T. A. (2021). Feasibility and Efficacy of the “FUNPALs Playgroup” Intervention to Improve Toddler Dietary and Activity Behaviors: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(15), 7828. https://doi.org/10.3390/ijerph18157828