
Multidisciplinary Care after Acute Care for Stroke: A Prospective Comparison between a Multidisciplinary Post-Acute Care Group and a Standard Group Matched by Propensity Score

 ,
,  , and
, and 
Abstract
:1. Introduction
- Is a multidisciplinary PAC program delivered early after stroke effective in restoring function?
- Should intensive rehabilitative PAC for stroke routinely include interventions for overall improvement of functional status?
2. Materials and Methods
2.1. The PAC Program
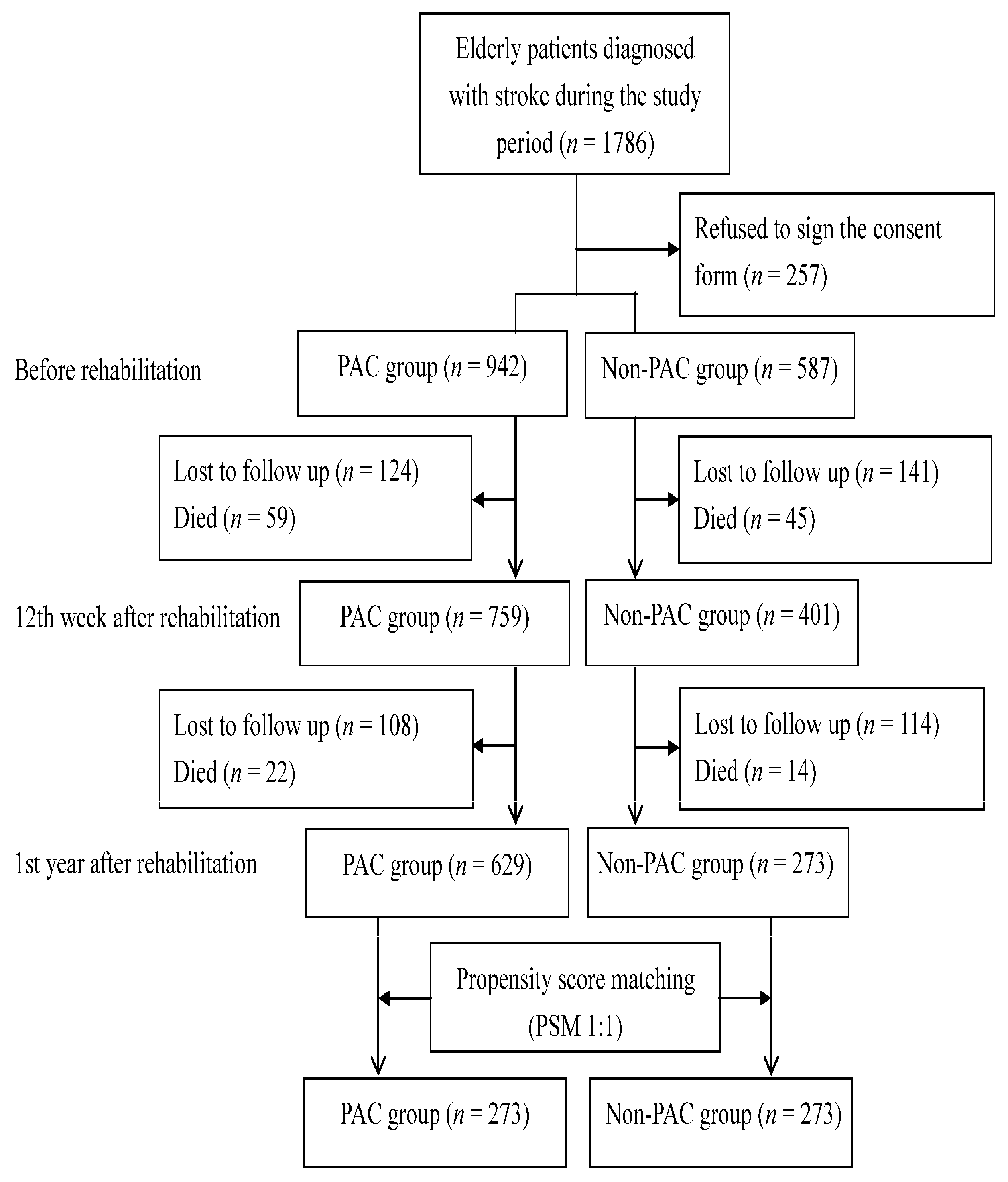
2.2. Sample and Study Design
2.3. Instruments and Measurements
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- An, S.J.; Kim, T.J.; Yoon, B.W. Epidemiology, risk factors, and clinical features of intracerebral hemorrhage: An update. J. Stroke 2017, 19, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Unibaso-Markaida, I.; Iraurgi, I.; Ortiz-Marqués, N.; Martínez-Rodríguez, S. Degree of Functionality and Perception of Health-Related Quality of Life in People with Moderate Stroke: Differences between Ischemic and Hemorrhagic Typology. Behav. Neurol. 2019, 2019, 3405696. [Google Scholar] [CrossRef]
- Chu, C.L.; Chen, Y.P.; Chen, C.C.P.; Chen, C.K.; Chang, H.N.; Chang, C.H.; Pei, Y.C. Functional Recovery Patterns of Hemorrhagic and Ischemic Stroke Patients Under Post-Acute Care Rehabilitation Program. Neuropsychiatr. Dis. Treat. 2020, 16, 1975–1985. [Google Scholar] [CrossRef]
- Mechanic, R. Post-acute care--the next frontier for controlling Medicare spending. N. Engl. J. Med. 2014, 370, 692–694. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.Y.; Hsien, H.H.; Hung, K.W.; Lin, H.F.; Chiou, H.Y.; Yeh, S.C.; Yeh, Y.J.; Shi, H.Y. Multidiscipline Stroke Post-Acute Care Transfer System: Propensity-Score-Based Comparison of Functional Status. J. Clin. Med. 2019, 8, 1233. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.Y.; Seido, M.; Chen, C.H.; Lee, K.C.; Chang, L.C.; Chung, J.H.; Shi, H.Y. Walking ability and functional status after post-acute care for stroke rehabilitation in different age groups: A prospective study based on propensity score matching. Aging (Albany NY) 2020, 12, 10704–10714. [Google Scholar] [CrossRef]
- Ghanbari Ghoshchi, S.; De Angelis, S.; Morone, G.; Panigazzi, M.; Persechino, B.; Tramontano, M.; Capodaglio, E.; Zoccolotti, P.; Paolucci, S.; Iosa, M. Return to Work and Quality of Life after Stroke in Italy: A Study on the Efficacy of Technologically Assisted Neurorehabilitation. Int. J. Environ. Res. Public Health 2020, 17, 5233. [Google Scholar] [CrossRef]
- Fearon, P.; McArthur, K.S.; Garrity, K.; Graham, L.J.; McGroarty, G.; Vincent, S.; Quinn, T.J. Prestroke modified rankin stroke scale has moderate interobserver reliability and validity in an acute stroke setting. Stroke 2012, 43, 3184–3188. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, C.D.; Taub, N.A.; Woodrow, E.J.; Burney, P.G. Assessment of scales of disability and handicap for stroke patients. Stroke 1991, 22, 1242–1244. [Google Scholar] [CrossRef] [Green Version]
- Crary, M.A.; Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Chou, C.Y.; Chien, C.W.; Hsueh, I.P.; Sheu, C.F.; Wang, C.H.; Hsieh, C.L. Developing a short form of the Berg Balance Scale for people with stroke. Phys. Ther. 2006, 86, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Griswold, M.E.; Localio, A.R.; Mulrow, C. Propensity score adjustment with multilevel data: Setting your sites on decreasing selection bias. Ann. Intern. Med. 2010, 152, 393–395. [Google Scholar] [CrossRef]
- Zeger, S.L.; Liang, K.Y. Longitudinal data analysis for discrete and continuous outcomes. Biometrics 1986, 42, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Schluchter, M.D. Flexible Approaches to Computing Mediated Effects in Generalized Linear Models: Generalized Estimating Equations and Bootstrapping. Multivar. Behav. Res. 2008, 43, 268–288. [Google Scholar] [CrossRef]
- Rosenthal, M.B.; Alidina, S.; Friedberg, M.W.; Singer, S.J.; Eastman, D.; Li, Z.; Schneider, E.C. A Difference-in-Difference Analysis of Changes in Quality, Utilization and Cost Following the Colorado Multi-Payer Patient-Centered Medical Home Pilot. J. Gen. Intern. Med. 2016, 31, 289–296. [Google Scholar] [CrossRef]
- Miyai, I.; Sonoda, S.; Nagai, S.; Takayama, Y.; Inoue, Y.; Kakehi, A.; Kurihara, M.; Ishikawa, M. Results of new policies for inpatient rehabilitation coverage in Japan. Neurorehabil. Neural Repair 2011, 25, 540–547. [Google Scholar] [CrossRef]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for adult stroke rehabilitation and recovery: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [PubMed]
- Turner, M.; Barber, M.; Dodds, H.; Dennis, M.; Langhorne, P.; Macleod, M.J.; Scottish Stroke Care Audit. The impact of stroke unit care on outcome in a Scottish stroke population, taking into account case mix and selection bias. J. Neurol. Neurosurg. Psychiatry 2015, 86, 314–318. [Google Scholar] [CrossRef] [Green Version]
- Chiu, A.; Shen, Q.; Cheuk, G.; Cordato, D.; Chan, D.K.Y. Establishment of a stroke unit in a district hospital: Review of experience. Intern. Med. J. 2007, 37, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.R.F.; Badhiwala, J.H.; Jiang, F.; Wilson, J.R.; Kopjar, B.; Vaccaro, A.R.; Fehlings, M.G. The Impact of Older Age on Functional Recovery and Quality of Life Outcomes after Surgical Decompression for Degenerative Cervical Myelopathy: Results from an Ambispective, Propensity-Matched Analysis from the CSM-NA and CSM-I International, Multi-Center Studies. J. Clin. Med. 2019, 8, 1708. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Li, F.; Li, X.; Du, G. Effect of Intermittent Pneumatic Compression on Preventing Deep Vein Thrombosis Among Stroke Patients: A Systematic Review and Meta-Analysis. Worldviews Evid. Based Nurs. 2018, 15, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Xian, Y.; Holloway, R.G.; Chan, P.S.; Noyes, K.; Shah, M.N.; Ting, H.H.; Chappel, A.R.; Peterson, E.D.; Friedman, B. Association between Stroke Center Hospitalization for Acute Ischemic Stroke and Mortality. JAMA 2011, 305, 373–380. [Google Scholar] [CrossRef]
- Renoux, C.; Coulombe, J.; Li, L.; Ganesh, A.; Silver, L.; Rothwell, P.M.; Oxford Vascular Study. Confounding by Pre-Morbid Functional Status in Studies of Apparent Sex Differences in Severity and Outcome of Stroke. Stroke 2017, 48, 2731–2738. [Google Scholar] [CrossRef]
- Nadeau, S.E.; Dobkin, B.; Wu, S.S.; Pei, Q.; Duncan, P.W.; The LEAPS Investigative Team. The Effects of Stroke Type, Locus, and Extent on Long-Term Outcome of Gait Rehabilitation: The LEAPS Experience. Neurorehabil. Neural Repair 2016, 30, 615–625. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Before Propensity Score Matching | After Propensity Score Matching | ||||||
|---|---|---|---|---|---|---|---|
| Variables | PAC Group (n = 942) | Non-PAC Group (n = 587) | p Value | PAC Group (n = 273) | Non-PAC Group (n = 273) | p Value | |
| Age, years | 69.3 ± 8.5 | 68.8 ± 7.6 | 0.736 | 69.1 ± 8.3 | 68.9 ± 8.0 | 0.834 | |
| Gender | Female | 403 (42.8%) | 238 (40.6%) | 0.704 | 116 (42.4%) | 114 (41.9%) | 0.684 |
| Male | 539 (57.2%) | 349 (59.4%) | 157 (57.6%) | 159 (58.1%) | |||
| Education, years | 7.8 ± 4.3 | 9.4 ± 4.5 | <0.001 | 8.9 ± 4.1 | 9.2 ± 4.4 | 0.888 | |
| BMI, kg/m2 | 24.4 ± 3.2 | 24.4 ± 3.9 | 0.976 | 24.0 ± 3.0 | 23.9 ± 3.3 | 0.849 | |
| Stroke type | Ischemic | 806 (85.6%) | 512 (87.2%) | 0.669 | 232(85.0%) | 236 (86.4%) | 0.891 |
| Hemorrhagic | 136 (14.4%) | 75 (12.8%) | 41 (15.0%) | 37 (13.6%) | |||
| Hypertension | Yes | 677 (71.9%) | 421 (71.8%) | 0.995 | 196 (72.0%) | 196 (72.0%) | 0.997 |
| Hyperlipidemia | Yes | 265 (28.1%) | 273 (46.5%) | <0.001 | 114 (41.8%) | 117 (42.8%) | 0.507 |
| Diabetes mellitus | Yes | 343 (36.4%) | 338 (57.6%) | 0.270 | 103 (37.7%) | 102 (37.4%) | 0.990 |
| Atrial fibrillation | Yes | 78 (8.3%) | 49 (8.3%) | 0.989 | 22(8.0%) | 17 (6.3%) | 0.534 |
| Previous stroke | Yes | 131 (13.9%) | 146 (24.9%) | <0.001 | 49 (18.0%) | 50 (18.4%) | 0.879 |
| Acute care LOS, days | 13.01 ± 27.83 | 24.45 ± 34.61 | <0.001 | 23.75 ± 11.84 | 24.50 ± 11.56 | 0.356 | |
| LOS during rehabilitation, days | 31.52 ± 17.75 | 37.1 ± 12.59 | <0.001 | 35.52 ± 12.04 | 36.63 ± 11.91 | 0.916 | |
| BI score before rehabilitation | 41.91 ± 23.10 | 34.67 ± 23.48 | <0.001 | 34.90 ± 20.00 | 34.43 ± 17.80 | 0.879 | |
| FOIS score before rehabilitation | 5.95 ± 3.04 | 5.38 ± 2.25 | <0.001 | 5.57 ± 2.80 | 5.13 ± 2.75 | 0.974 | |
| EQ5D score before rehabilitation | 10.67 ± 1.86 | 10.40 ±1.78 | 0.015 | 10.81 ± 1.90 | 10.87 ± 2.15 | 0.891 | |
| IADL score before rehabilitation | 1.41 ± 1.20 | 1.15 ± 1.12 | <0.001 | 1.32 ± 1.14 | 1.13 ± 1.01 | 0.934 | |
| BBS score before rehabilitation | 15.30 ± 14.99 | 16.91 ± 17.27 | 0.097 | 16.13 ± 14.08 | 16.67 ± 15.57 | 0.882 | |
| MMSE score before rehabilitation | 20.15 ± 7.90 | 18.50 ± 9.66 | 0.001 | 20.67 ± 11.50 | 19.57 ± 10.20 | 0.859 | |
| Functional Status Measures | Before Rehabilitation | After Rehabilitation | 12th Week after Rehabilitation before Rehabilitation | 1st Year after Rehabilitation before Rehabilitation | ||||
|---|---|---|---|---|---|---|---|---|
| 12th Week | 1st Year | |||||||
| Mean | Mean | Mean | Mean | Standard Error | Mean | Standard Error | ||
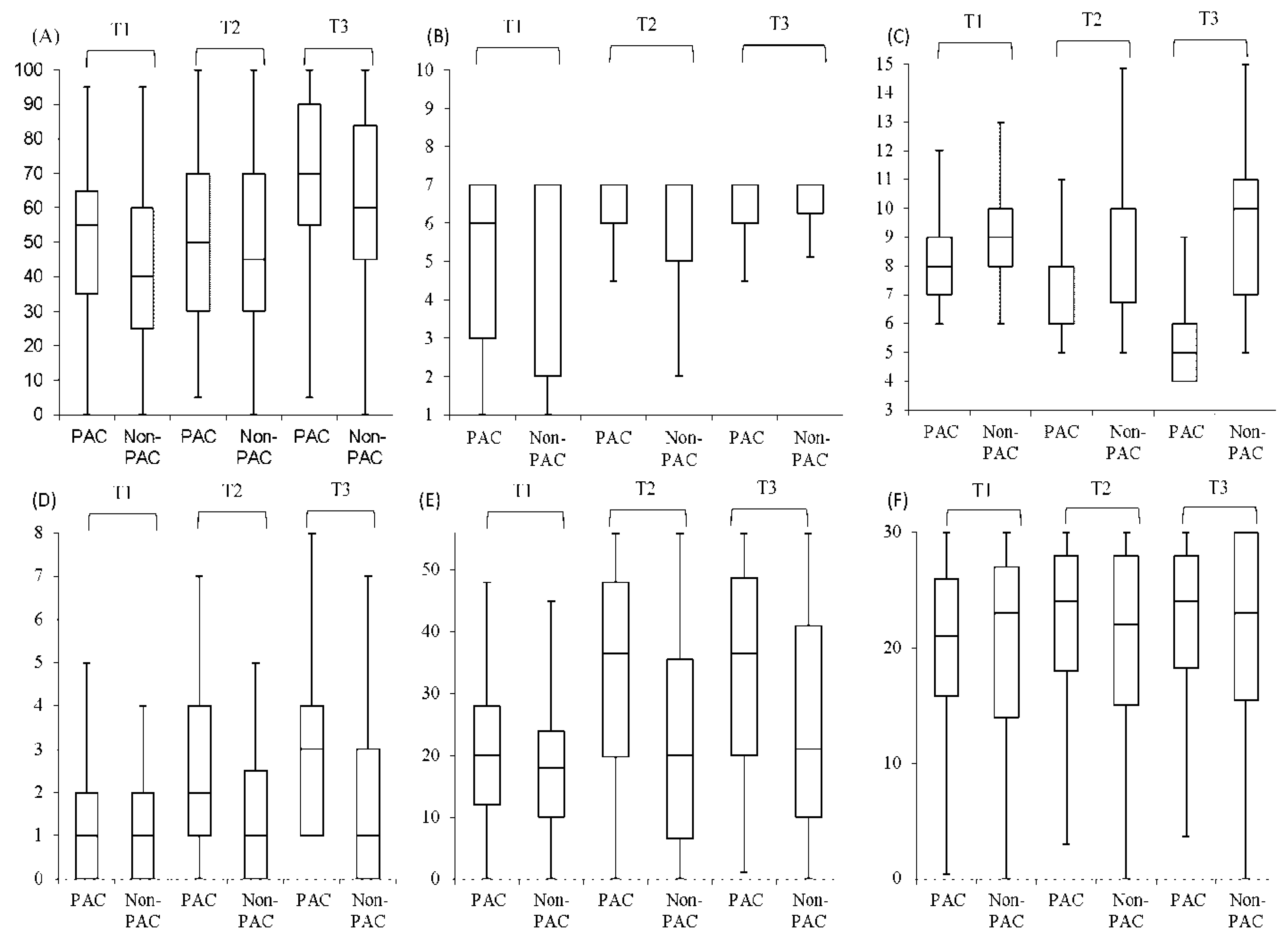
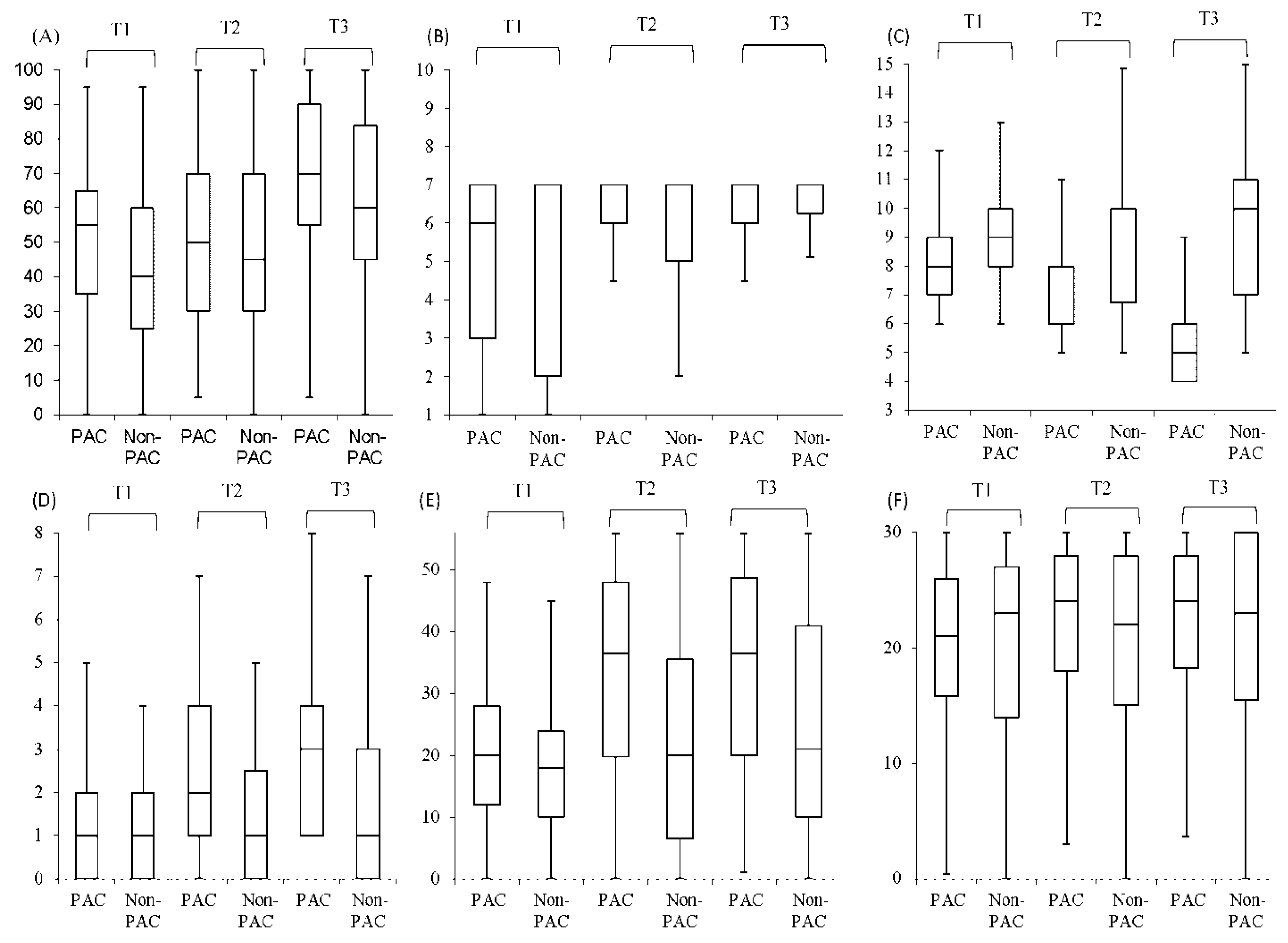
| BI | PAC | 51.90 | 59.32 | 65.76 | 7.42 | 1.95 | 13.86 | 4.84 |
| Non-PAC | 50.79 | 54.20 | 60.29 | 3.41 | 1.18 | 9.50 | 3.66 | |
| Difference | 1.12 | 3.12 | 3.47 | 4.01 | 0.88 | 4.36 | 0.91 | |
| FOIS | PAC | 5.38 | 6.39 | 6.52 | 1.01 | 0.12 | 1.14 | 0.19 |
| Non-PAC | 5.19 | 5.74 | 5.95 | 0.55 | 0.11 | 0.76 | 0.15 | |
| Difference | 0.19 | 0.65 | 0.58 | 0.46 | 0.10 | 0.38 | 0.07 | |
| EQ-5D | PAC | 8.41 | 6.28 | 4.99 | −2.13 | 0.43 | −3.42 | 0.58 |
| Non-PAC | 8.92 | 8.12 | 7.53 | −0.80 | 0.42 | −1.39 | 0.41 | |
| Difference | −0.50 | −1.84 | −2.54 | −1.33 | 0.16 | −2.03 | −0.26 | |
| IADL | PAC | 1.58 | 2.85 | 3.42 | 1.27 | 0.11 | 1.84 | 0.12 |
| Non-PAC | 1.17 | 2.36 | 2.90 | 1.19 | 0.18 | 1.73 | 0.20 | |
| Difference | 0.40 | 0.50 | 0.52 | 0.08 | 0.03 | 0.11 | 0.03 | |
| BBS | PAC | 20.59 | 29.53 | 34.40 | 8.94 | 1.32 | 13.81 | 4.25 |
| Non-PAC | 18.89 | 24.85 | 29.60 | 5.96 | 1.64 | 10.71 | 2.38 | |
| Difference | 1.70 | 4.68 | 4.80 | 2.98 | 0.68 | 3.10 | 0.83 | |
| MMSE | PAC | 20.72 | 22.46 | 23.13 | 1.74 | 0.20 | 2.41 | 0.22 |
| Non-PAC | 19.41 | 20.77 | 21.15 | 1.36 | 0.18 | 1.74 | 0.13 | |
| Difference | 1.31 | 1.69 | 1.98 | 0.38 | 0.10 | 0.67 | 0.10 | |
| Variables | BI | FOIS | EQ-5D | IADL | BBS | MMSE |
|---|---|---|---|---|---|---|
| Group PAC vs. non-PAC | 2.24 * | 0.46 * | −0.47 ** | 0.15 ** | 1.94 * | 0.27 * |
| Gender Male vs. female | 0.01 | 0.02 | −0.02 | 0.15 | 0.76 | 0.07 |
| Age, years | −0.20 ** | −0.02 | 0.02 *** | −0.01 ** | −0.17 *** | −0.07 ** |
| Education, years | 0.12 | 0.01 | 0.04 | 0.01 | −0.13 | 0.02 |
| BMI, kg/m2 | 0.23 | 0.01 | 0.01 | 0.02 | 0.07 | 0.07 |
| Stroke type Ischemic vs. hemorrhagic | 0.14 | 0.15 | −0.43 * | 0.23 * | −0.08 | −0.18 |
| CCI, score | 1.78 | −0.01 | −0.03 | −0.19 | 1.42 | −0.33 |
| Length of stay, days | 0.04 | −0.01 | 0.01 | −0.01 | 0.02 | 0.01 |
| UTI Yes vs. no | −1.56 | −0.04 | 0.30 | 0.02 | −0.86 | 1.11 |
| Renal disease Yes vs. no | 0.41 | 0.06 | 0.18 | 0.01 | −1.27 | 0.24 |
| Hypertension Yes vs. no | −2.26 | 0.03 | −0.05 | 0.04 | −1.67 | 0.07 |
| Diabetes Yes vs. no | −0.18 | 0.05 | 0.14 | 0.23 | −0.33 | 0.64 |
| Hyperlipidemia Yes vs. no | 1.80 | 0.13 | −0.11 | 0.09 | 0.29 | −0.06 |
| Functional status before rehabilitation | 0.82 *** | 0.69 *** | −0.74 *** | 0.86 *** | 0.83 *** | 0.73 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, C.-C.; Lin, H.-F.; Lin, C.-H.; Chang, H.-T.; Hsien, H.-H.; Hung, K.-W.; Tung, S.-L.; Shi, H.-Y. Multidisciplinary Care after Acute Care for Stroke: A Prospective Comparison between a Multidisciplinary Post-Acute Care Group and a Standard Group Matched by Propensity Score. Int. J. Environ. Res. Public Health 2021, 18, 7696. https://doi.org/10.3390/ijerph18147696
Chiu C-C, Lin H-F, Lin C-H, Chang H-T, Hsien H-H, Hung K-W, Tung S-L, Shi H-Y. Multidisciplinary Care after Acute Care for Stroke: A Prospective Comparison between a Multidisciplinary Post-Acute Care Group and a Standard Group Matched by Propensity Score. International Journal of Environmental Research and Public Health. 2021; 18(14):7696. https://doi.org/10.3390/ijerph18147696
Chicago/Turabian StyleChiu, Chong-Chi, Hsiu-Fen Lin, Ching-Huang Lin, Hong-Tai Chang, Hong-Hsi Hsien, Kuo-Wei Hung, Sheng-Li Tung, and Hon-Yi Shi. 2021. "Multidisciplinary Care after Acute Care for Stroke: A Prospective Comparison between a Multidisciplinary Post-Acute Care Group and a Standard Group Matched by Propensity Score" International Journal of Environmental Research and Public Health 18, no. 14: 7696. https://doi.org/10.3390/ijerph18147696
APA StyleChiu, C.-C., Lin, H.-F., Lin, C.-H., Chang, H.-T., Hsien, H.-H., Hung, K.-W., Tung, S.-L., & Shi, H.-Y. (2021). Multidisciplinary Care after Acute Care for Stroke: A Prospective Comparison between a Multidisciplinary Post-Acute Care Group and a Standard Group Matched by Propensity Score. International Journal of Environmental Research and Public Health, 18(14), 7696. https://doi.org/10.3390/ijerph18147696