
Exposure to Air Pollution in Rural Malawi: Impact of Cooking Methods on Blood Pressure and Peak Expiratory Flow

 , ,
, ,
Abstract
:1. Introduction
2. Methods
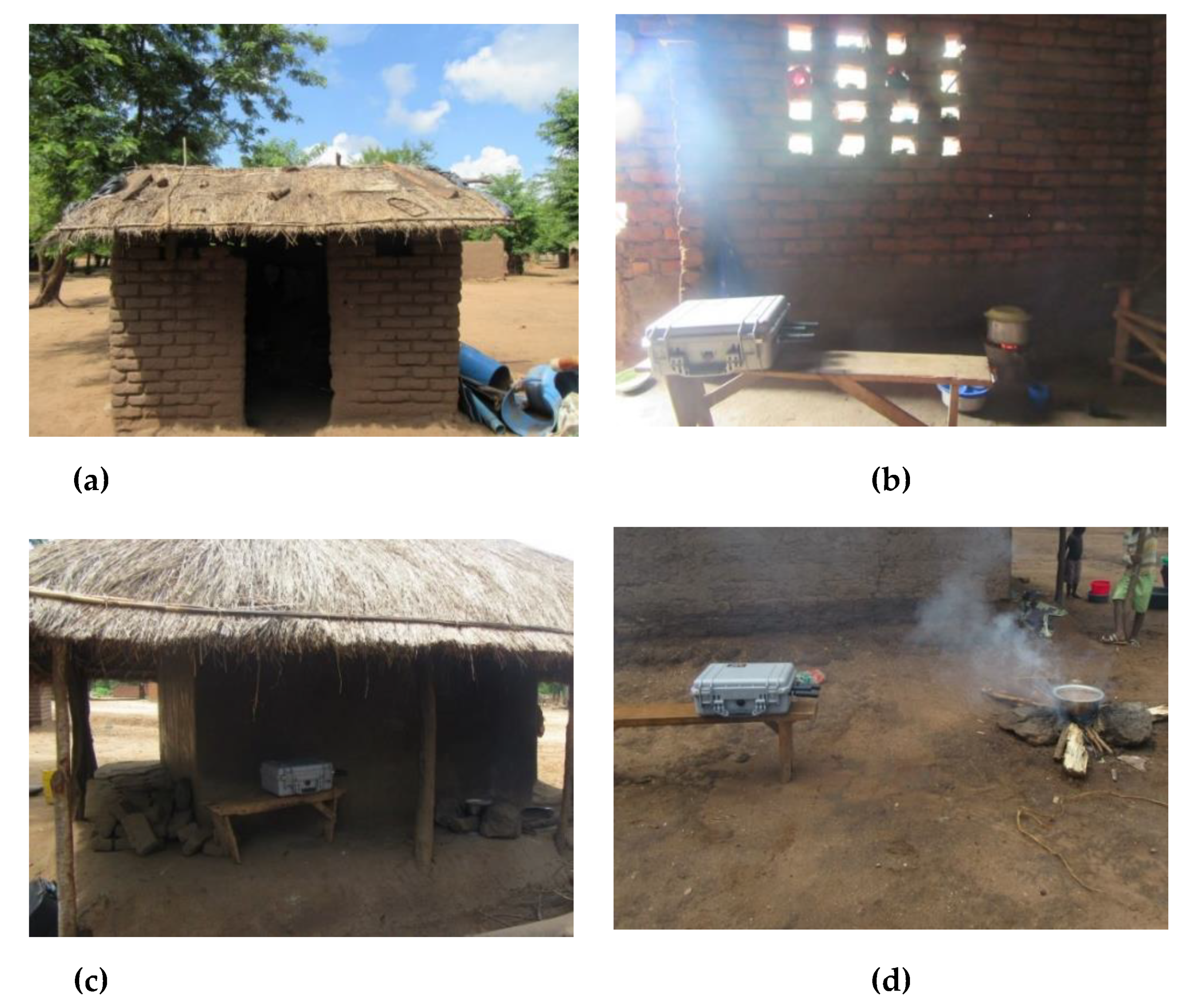
2.1. Sampling Location and Time
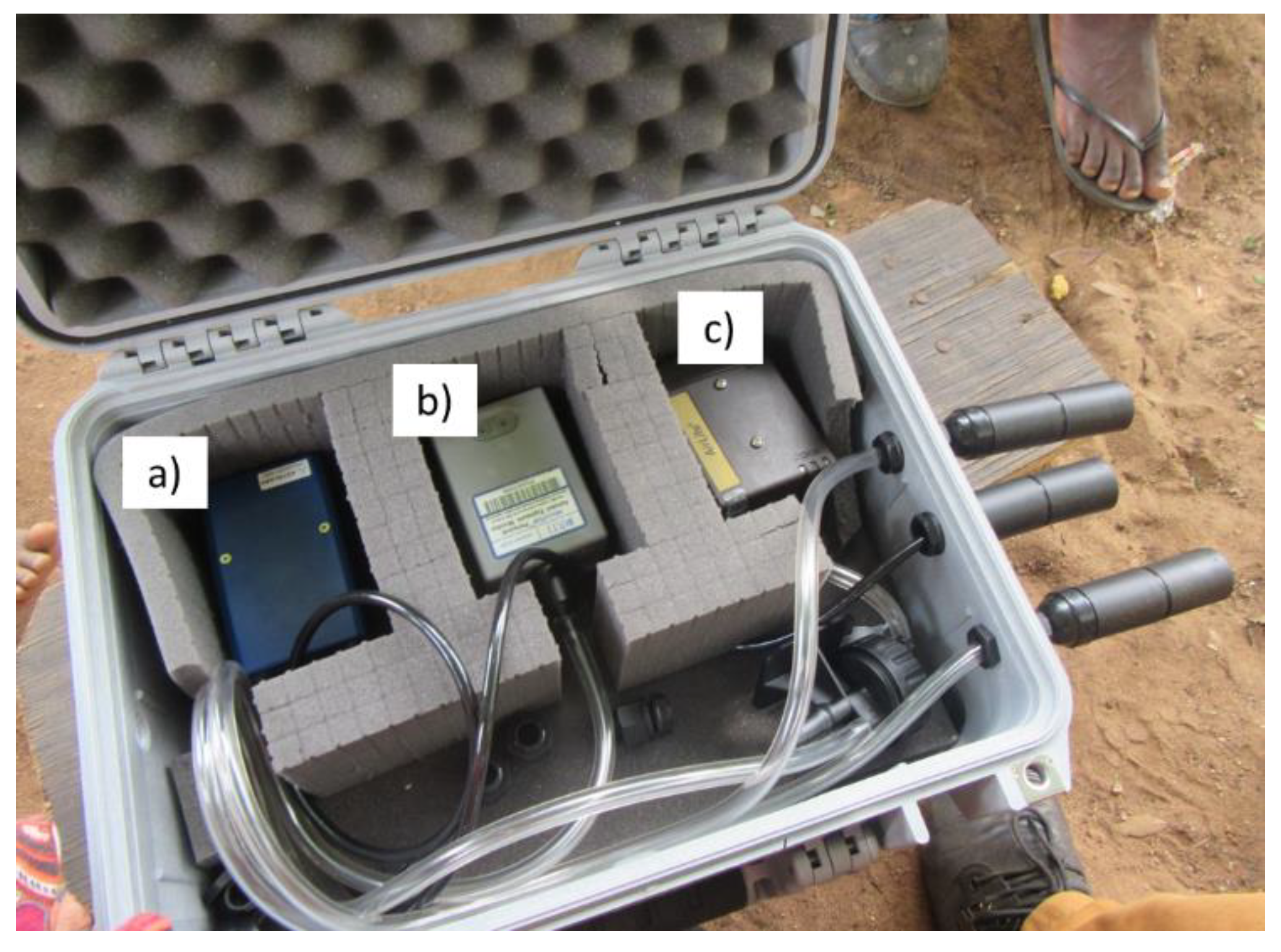
2.2. Measurement of PM2.5
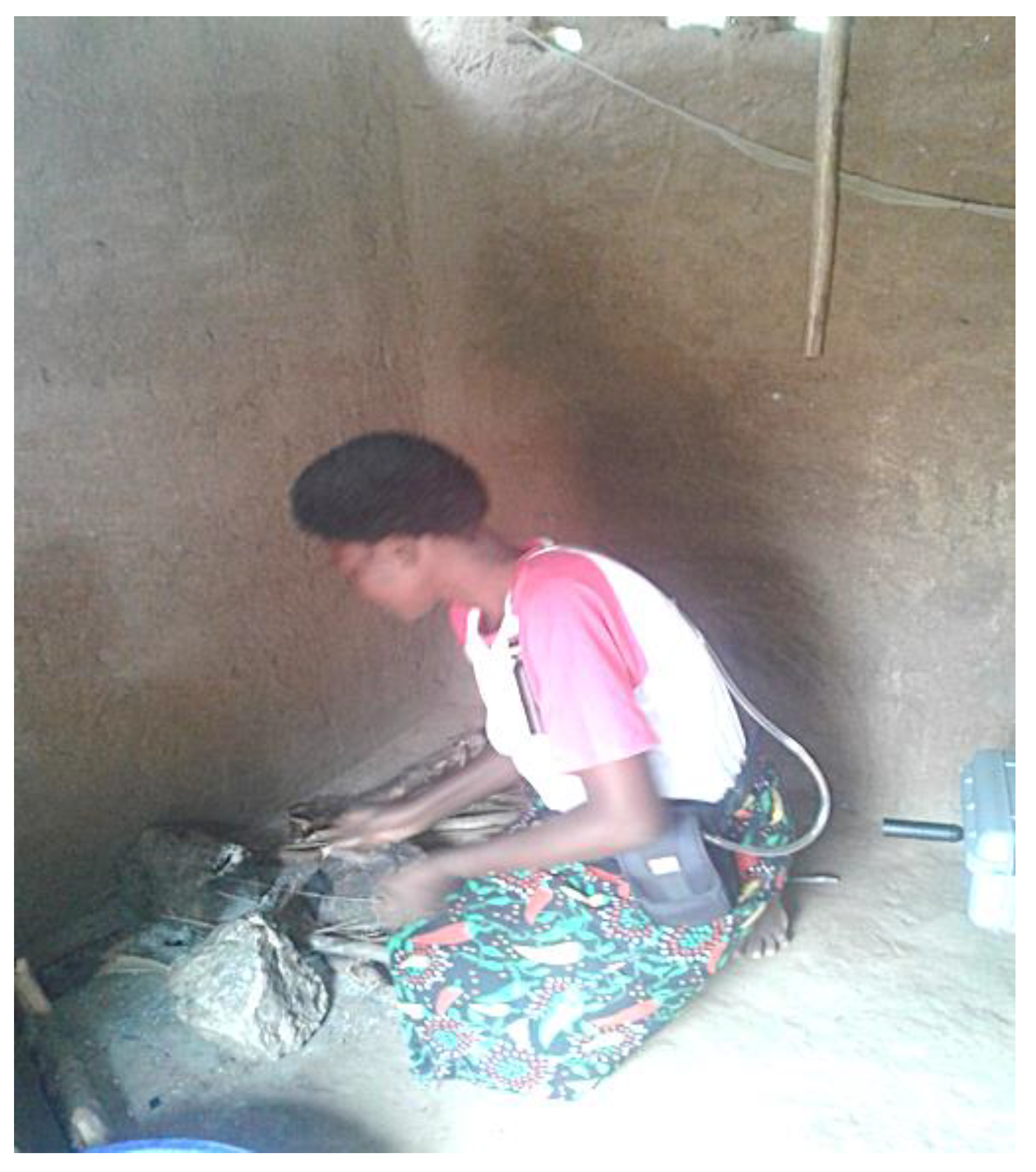
2.3. Measurement of Ambulatory Blood Pressure (BP), Heart Rate (HR) and Peak Expiratory Flow Rate (PEFR)
2.4. Information on Activities and Prior Health Conditions
3. Results
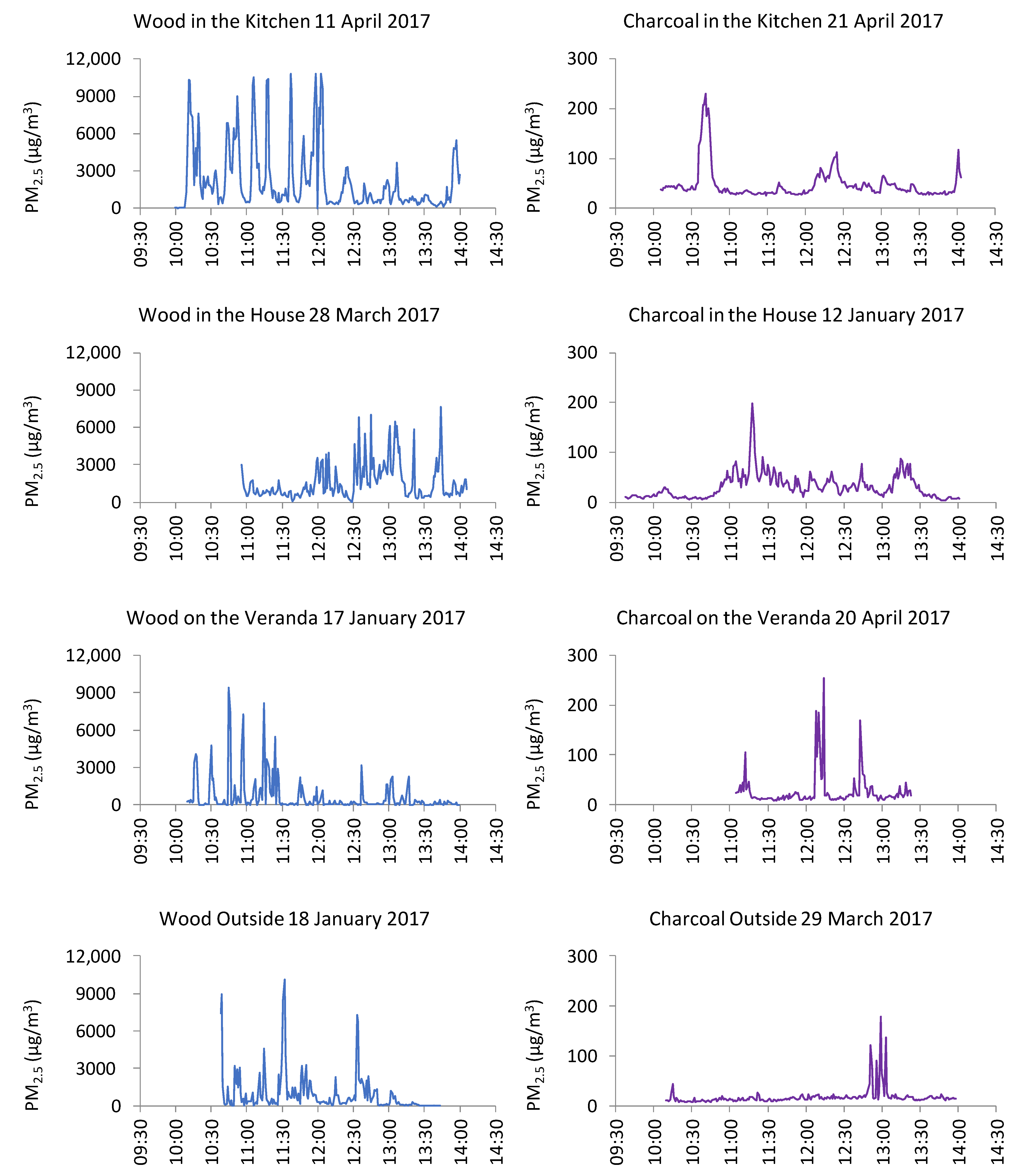
3.1. PM2.5 Concentrations Observed during Static Sampling
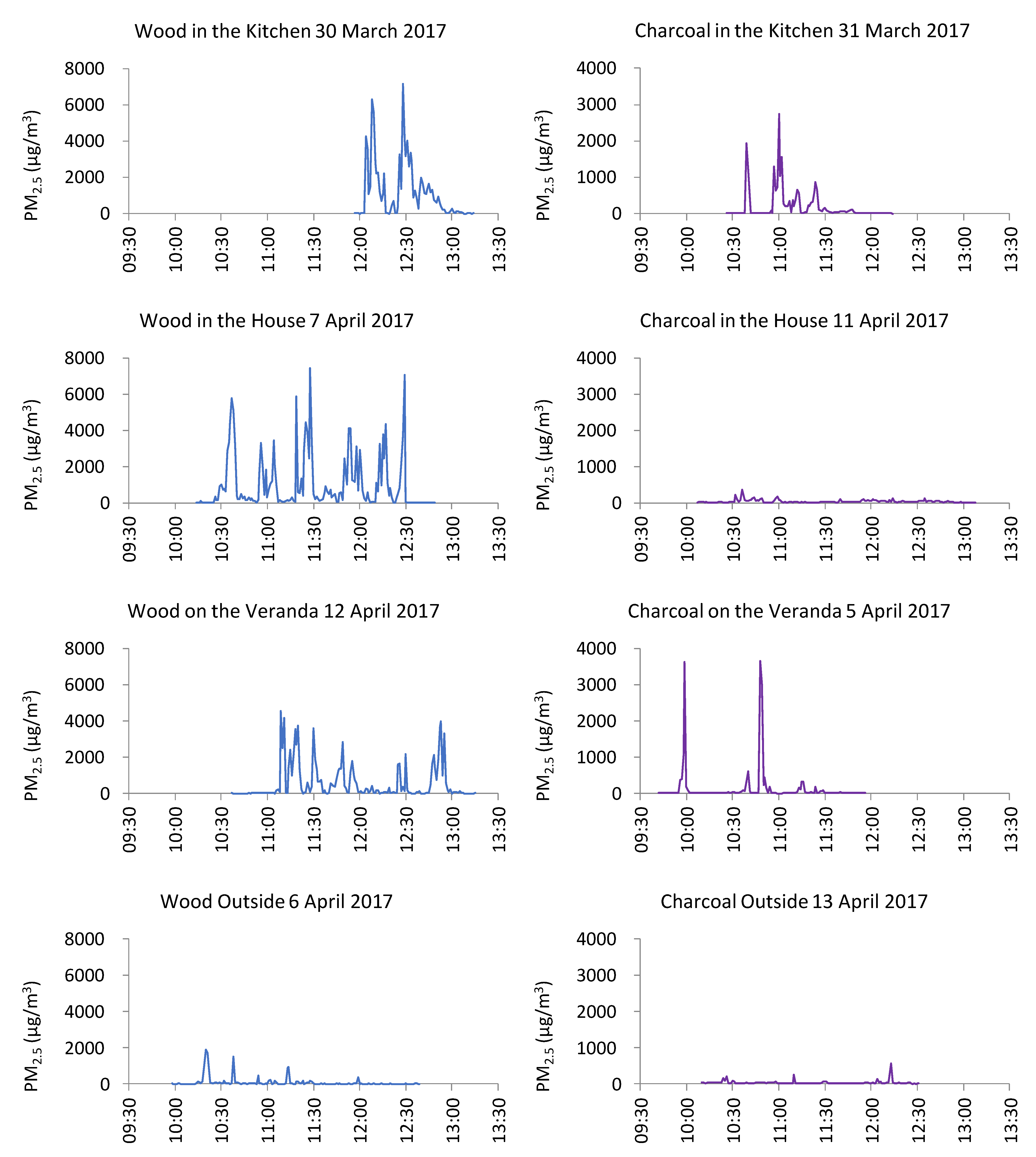
3.2. PM2.5 Exposures Observed during Personal Sampling
3.3. Health Data
3.3.1. Blood Pressure and Heart Rate
3.3.2. Peak Expiratory Flow Rate (PEFR) Tests
3.3.3. Information from Questionnaires and Health Passports
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Fact Sheet Household Air Pollution. Available online: https://www.who.int/en/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 17 April 2020).
- Ezzati, M.; Kammen, D.M. Review The Health Impacts of Exposure to Indoor Air Pollution from Solid Fuels in Developing Countries: Knowledge, Gaps, and Data Needs. Environ. Health Perspect. 2002, 110, 1057–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, M.A.; Mehta, S.; Smith, K.R. Indoor Smoke from Solid Fuels: Assessing the Environmental Burden of Disease at National and Local Levels; (WHO Environmental Burden of Disease Series, No.4); WHO: Geneva, Switzerland, 2004; pp. 7–14. [Google Scholar]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef] [Green Version]
- Norris, C.; Goldberg, M.S.; Marshall, J.D.; Valois, M.F.; Pradeep, T.; Narayanswamy, M.; Jain, G.; Sethuraman, K.; Baumgartner, J. A panel study of the acute effects of personal exposure to household air pollution on ambulatory blood pressure in rural Indian women. Environ. Res. 2016, 147, 331–342. [Google Scholar] [CrossRef]
- Sana, A.; Somda, S.M.A.; Meda, N.; Bouland, C. Chronic obstructive pulmonary disease associated with biomass fuel use in women: A systematic review and meta-analysis. BMJ Open Respir. Res. 2018, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.R.; Mehta, S.; Maeusezahl-Feuz, M. Indoor air pollution from household use of solid fuels. In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; Ezzati, M., Lopez, A.D., Rodgers, A., Murray, C.J.L., Eds.; World Health Organization: Geneva, Switzerland, 2004; pp. 1453–1493. ISBN 92 4 158031 3. [Google Scholar]
- WHO. WHO Air Quality Guidelines: Global Update 2005; Report on a Working Group Meeting, Bonn, Germany, 18–20 October 2005; WHO: Geneva, Switzerland, 2006; p. 7. [Google Scholar] [CrossRef]
- Elledge, M.F.; Phillips, M.J.; Thornburg, V.E.; Everett, K.H.; Nandasena, S. A profile of biomass stove use in Sri Lanka. Int. J. Environ. Res. Public Health 2012, 9, 1097–1110. [Google Scholar] [CrossRef] [Green Version]
- Fullerton, D.G.; Semple, S.; Kalambo, F.; Suseno, A.; Malamba, R.; Henderson, G.; Ayres, J.G.; Gordon, S.B. Biomass fuel use and indoor air pollution in homes in Malawi. Occup. Environ. Med. 2009, 66, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, V.; Retherford, R.D.; Smith, K.R. Effects of Cooking Smoke on Prevalence of Tuberculosis in India. Int. J. Infect. Dis. 1999, 3, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Mukhopadhyay, R.; Sambandam, S.; Pillarisetti, A.; Jack, D.; Mukhopadhyay, K.; Balakrishnan, K.; Vaswani, M.; Bates, M.N.; Kinney, P.L.; Arora, N.; et al. Cooking practices, air quality, and the acceptability of advanced cookstoves in Haryana, India: An exploratory study to inform large-scale interventions. Glob. Health Action 2012, 5, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Rumchev, K.; Spickett, J.T.; Brown, H.L.; Mkhweli, B. Indoor air pollution from biomass combustion and respiratory symptoms of women and children in a Zimbabwean village. Indoor Air 2007, 17, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.H.; Chartier, R.T.; Mortimer, K.; Dherani, M.; Tafatatha, T. A personal particulate matter exposure monitor to support household air pollution exposure and health studies. In Proceedings of the 2016 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 13–16 October 2016; pp. 817–818. [Google Scholar] [CrossRef]
- Rylance, S.; Jewell, C.; Naunje, A.; Mbalume, F.; Chetwood, J.D.; Nightingale, R.; Zurba, L.; Flitz, G.; Gordon, S.B.; Lesosky, M.; et al. Non-communicable respiratory disease and air pollution exposure in Malawi: A prospective cohort study. Thorax 2020, 75, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Chartier, R.; Phillips, M.; Mosquin, P.; Elledge, M.; Bronstein, K.; Nandasena, S.; Thornburg, V.; Thornburg, J.; Rodes, C. A comparative study of human exposures to household air pollution from commonly used cookstoves in Sri Lanka. Indoor Air 2017, 27, 147–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fullerton, D.G.; Suseno, A.; Semple, S.; Kalambo, F.; Malamba, R.; White, S.; Jack, S.; Calverley, P.M.; Gordon, S.B. Wood smoke exposure, poverty and impaired lung function in Malawian adults. Int. J. Tuberc. Lung Dis. 2011, 15, 391–398. [Google Scholar] [PubMed]
- UN. United Nations—Malawi. Available online: https://mw.one.un.org/country-profile/ (accessed on 14 February 2020).
- Cox, J.; Cho, S.H.; Ryan, P.; Isiugo, K.; Ross, J.; Chillrud, S.; Zhu, Z.; Jandarov, R.; Grinshpun, S.A.; Reponen, T. Combining sensor-based measurement and modeling of PM2.5 and black carbon in assessing exposure to indoor aerosols. Aerosol Sci. Technol. 2019, 53, 817–829. [Google Scholar] [CrossRef]
- Guak, S.; Lee, K. Different relationships between personal exposure and ambient concentration by particle size. Environ. Sci. Pollut. Res. 2018, 25, 16945–16950. [Google Scholar] [CrossRef]
- Du, Y.; Wang, Q.; Sun, Q.; Zhang, T.; Li, T.; Yan, B. Assessment of PM2.5 monitoring using MicroPEM: A validation study in a city with elevated PM2.5 levels. Ecotoxicol. Environ. Saf. 2019, 171, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Masey, N.; Wu, H.; Jackson, M.; Carruthers, D.J.; Reis, S.; Doherty, R.M.; Beverland, I.J.; Heal, M.R. Practical Field Calibration of Portable Monitors for Mobile Measurements of Multiple Air Pollutants. Atmosphere 2017, 8, 231. [Google Scholar] [CrossRef] [Green Version]
- Zhang, T.; Chillrud, S.N.; Ji, J.; Chen, Y.; Pitiranggon, M.; Li, W.; Liu, Z.; Yan, B. Comparison of PM2.5 exposure in hazy and non-hazy days in Nanjing, China. Aerosol Air Qual. Res. 2017, 17, 2235–2246. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Chen, F.; Cai, Y.; Fan, S.; Cai, J.; Chen, R.; Kan, H.; Lu, Y.; Zhao, Z. Validation of a light-scattering PM2.5 sensor monitor based on the long-term gravimetric measurements in field tests. PLoS One 2017, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- NHS NHS Blood Pressure Test. Available online: https://www.nhs.uk/conditions/blood-pressure-test/ (accessed on 4 February 2020).
- Clement Clark International Peak Flow Test. Available online: http://www.peakflow.com/top_nav/normal_values/PEFNorms.html (accessed on 14 November 2019).
- American Lung Association Measure Your Peak Flow Rate. Available online: https://www.lung.org/lung-health-and-diseases/lung-disease-lookup/asthma/living-with-asthma/managing-asthma/measuring-your-peak-flow-rate.html (accessed on 14 November 2019).
- Delapena, S.; Piedrahita, R.; Pillarisetti, A.; Garland, C.; Rossanese, M.E.; Johnson, M.; Pennise, D. Using personal exposure measurements of particulate matter to estimate health impacts associated with cooking in peri-urban Accra, Ghana. Energy Sustain. Dev. 2018, 45, 190–197. [Google Scholar] [CrossRef]
- Van Vliet, E.D.S.; Asante, K.; Jack, D.W.; Kinney, P.L.; Whyatt, R.M.; Chillrud, S.N.; Abokyi, L.; Zandoh, C.; Owusu-Agyei, S. Personal exposures to fine particulate matter and black carbon in households cooking with biomass fuels in rural Ghana. Environ. Res. 2013, 127, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Phillips, M.J.; Smith, E.A.; Mosquin, P.L.; Chartier, R.; Nandasena, S.; Bronstein, K.; Elledge, M.F.; Thornburg, V.; Thornburg, J.; Brown, L.M. Sri lanka pilot study to examine respiratory health effects and personal PM2.5 exposures from cooking indoors. Int. J. Environ. Res. Public Health 2016, 13, 791. [Google Scholar] [CrossRef] [Green Version]
- Kurmi, O.P.; Semple, S.; Steiner, M.; Henderson, G.D.; Ayres, J.G. Particulate matter exposure during domestic work in Nepal. Ann. Occup. Hyg. 2008, 52, 509–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bede-Ojimadu, O.; Orisakwe, O.E. Exposure to Wood Smoke and Associated Health Effects in Sub-Saharan Africa: A Systematic Review. Ann. Glob. Health 2020, 86, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, I.; Jagger, P.; Yeatts, K. Biomass Cooking Fuels and Health Outcomes for Women in Malawi. Ecohealth 2017, 14, 7–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Po, J.Y.T.; FitzGerald, J.M.; Carlsten, C. Respiratory disease associated with solid biomass fuel exposure in rural women and children: Systematic review and meta-analysis. Thorax 2011, 66, 232–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.S.; Hang, J.Q.; Zhang, F.Y.; Dai, H.L.; Su, L.; Christiani, D.C. In-home solid fuel use and cardiovascular disease: A cross-sectional analysis of the Shanghai Putuo study. Environ. Heal. A Glob. Access Sci. Source 2012, 11, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, K.J.; Chan, C.C.; Shiao, G.M.; Su, T.C. Associations between submicrometer particles exposures and blood pressure and heart rate in patients with lung function impairments. J. Occup. Environ. Med. 2005, 47, 1093–1098. [Google Scholar] [CrossRef]
- Kubesch, N.; De Nazelle, A.; Guerra, S.; Westerdahl, D.; Martinez, D.; Bouso, L.; Carrasco-Turigas, G.; Hoffmann, B.; Nieuwenhuijsen, M.J. Arterial blood pressure responses to short-term exposure to low and high traffic-related air pollution with and without moderate physical activity. Eur. J. Prev. Cardiol. 2015, 22, 548–557. [Google Scholar] [CrossRef]
- Brook, R.D.; Weder, A.B.; Rajagopalan, S. “Environmental Hypertensionology” the effects of environmental factors on blood pressure in clinical practice and research. J. Clin. Hypertens. 2011, 13, 836–842. [Google Scholar] [CrossRef] [PubMed]
- Liang, R.; Zhang, B.; Zhao, X.; Ruan, Y.; Lian, H.; Fan, Z. Effect of exposure to PM2.5 on blood pressure: A systematic review and meta-analysis. J. Hypertens. 2014, 32, 2130–2141. [Google Scholar] [CrossRef]
- Ministry of Natural Resources Energy & Mining National Charcoal Strategy. Available online: https://cepa.rmportal.net/Library/government-publications/national-charcoal-strategy-2017-2027/view (accessed on 7 July 2020).
- Wathore, R.; Mortimer, K.; Grieshop, A.P. In-Use Emissions and Estimated Impacts of Traditional, Natural- and Forced-Draft Cookstoves in Rural Malawi. Environ. Sci. Technol. 2017, 51, 1929–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location | Static | Personal | ||
|---|---|---|---|---|
| Wood | Charcoal | Wood | Charcoal | |
| Kitchen | 11/01/17 | 21/04/17 | 30/03/17 | 31/03/17 |
| (210 min) | (231 min) | (77 min) | (108 min) | |
| House | 28/03/17 | 12/01/17 | 07/04/17 | 11/04/17 |
| (190 min) | (262 min) | (155 min) | (181 min) | |
| Veranda | 17/01/17 | 20/04/17 | 12/04/17 | 05/04/17 |
| (228 min) | (138 min) | (158 min) | (134 min) | |
| Outside | 18/01/17 | 29/03/17 | 06/04/17 | 13/04/17 |
| (185 min) | (227 min) | (161 min) | (141 min) | |
| Systolic Blood Pressure (mmHg) | Diastolic Blood Pressure (mmHg) | Category |
|---|---|---|
| 90–120 | 60–80 | Normal |
| 120–139 | 80–89 | Elevated |
| >140 | >90 | High |
| Statistic: | Location: | Static | Static | Personal | Personal | Static | Personal |
|---|---|---|---|---|---|---|---|
| Wood | Charcoal | Wood | Charcoal | W:C Ratio | W:C Ratio | ||
| Mean: | Kitchen | 2184 | 46 | 1163 | 193 | 47 | 6 |
| House | 1602 | 33 | 1008 | 44 | 49 | 23 | |
| Veranda | 638 | 27 | 554 | 100 | 24 | 6 | |
| Outside | 929 | 17 | 97 | 39 | 55 | 2 | |
| Mean: | Indoor | 1893 | 40 | 1086 | 119 | 48 | 9 |
| Outdoor | 784 | 22 | 326 | 70 | 36 | 4 | |
| All | 1338 | 31 | 706 | 94 | 44 | 7 | |
| In:Out ratio | 2.4 | 1.8 | 3.3 | 1.7 | |||
| Max: | Kitchen | 11,032 | 251 | 10,476 | 9164 | 44 | 1 |
| House | 11,268 | 245 | 11,296 | 777 | 46 | 15 | |
| Veranda | 11,733 | 1378 | 11,370 | 10,660 | 9 | 1 | |
| Outside | 11,242 | 1707 | 9666 | 2328 | 7 | 4 | |
| Max: | Indoor | 11,150 | 248 | 10,886 | 4971 | 45 | 2 |
| Outdoor | 11,488 | 1543 | 10,518 | 6494 | 7 | 2 | |
| All | 11,319 | 895 | 10,702 | 5732 | 13 | 2 | |
| In:Out ratio | 1.0 | 0.2 | 1.0 | 0.8 |
| Systolic BP (mm Hg) | Diastolic BP (mm Hg) | Heart Rate (bpm) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fuel | Location | Participant | Age | Height (cm) | Before | During | After | Difference | Before | During | After | Difference | Before | During | After | Difference |
| Wood | Kitchen | 1 | 30 | 163 | 116 | 118 | 109 | −7 | 73 | 75 | 71 | −2 | 106 | 108 | 101 | −5 |
| Wood | House | 2 | 81 | 154 | 150 | 123 | 123 | −27 | 92 | 75 | 75 | −17 | 91 | 81 | 81 | −10 |
| Wood | Veranda | 3 | 48 | 162 | 158 | 159 | 152 | −6 | 82 | 86 | 76 | −6 | 81 | 75 | 79 | −2 |
| Wood | Outside | 4 | 15 | 148 | 120 | 111 | 114 | −6 | 73 | 69 | 68 | −5 | 137 | 123 | 113 | −24 |
| Charcoal | Kitchen | 5 | 12 | 160 | 104 | 103 | 95 | −9 | 72 | 72 | 71 | −1 | 84 | 82 | 87 | 3 |
| Charcoal | House | 6 | 24 | 166 | 113 | 97 | 108 | −5 | 76 | 65 | 72 | −4 | 64 | 79 | 77 | 13 |
| Charcoal | Veranda | 7 | 33 | 155 | 103 | 106 | 106 | 3 | 73 | 71 | 75 | 2 | 78 | 80 | 77 | −1 |
| Charcoal | Outside | 8 | 21 | 160 | 110 | 105 | 104 | −6 | 79 | 75 | 74 | −5 | 83 | 84 | 86 | 3 |
| Fuel/ | Age | Height | Normal PEFR | Obs 1 PEFR | Obs 2 PEFR | Obs 3 PEFR | Obs 4 PEFR | Obs 5 PEFR | Change in PEFR |
|---|---|---|---|---|---|---|---|---|---|
| Location | (years) | (cm) | (L/min) | (L/min) | (Lmin) | (L/min) | (L/min) | (L/min) | (L/min) |
| Wood: | |||||||||
| Kitchen | 30 | 163 | 441 | 450 (102%) | 500 (113%) | 450 (102%) | 450 (102%) | 390 (88%) | −60 (−14%) |
| House | 81 | 154 | 319 | 180 (56%) | 160 (50%) | 200 (63%) | 190 (60%) | 140 (44%) | −40 (−13%) |
| Veranda | 48 | 162 | 418 | 350 (84%) | 340 (81%) | 330 (79%) | 280 (67%) | 300 (72%) | −50 (−12%) |
| Outside | 15 | 148 | 380 | 220 (58%) | 240 (63%) | 250 (66%) | 240 (63%) | 230 (61%) | 10 (3%) |
| Charcoal: | |||||||||
| Kitchen | 12 | 160 | 394 | 240 (61%) | 240 (61%) | 290 (74%) | 260 (66%) | 240 (61%) | 0 (0%) |
| House | 24 | 166 | 438 | 248 (57%) | 270 (62%) | 269 (61%) | 225 (51%) | 255 (58%) | 7 (2%) |
| Veranda | 33 | 155 | 431 | 310 (72%) | 300 (70%) | 230 (53%) | 270 (63%) | 240 (56%) | −70 (−16%) |
| Outside | 21 | 160 | 423 | 250 (59%) | 290 (69%) | 240 (57%) | 250 (59%) | 260 (61%) | 10 (2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mabonga, F.; Beattie, T.K.; Luwe, K.; Morse, T.; Hope, C.; Beverland, I.J. Exposure to Air Pollution in Rural Malawi: Impact of Cooking Methods on Blood Pressure and Peak Expiratory Flow. Int. J. Environ. Res. Public Health 2021, 18, 7680. https://doi.org/10.3390/ijerph18147680
Mabonga F, Beattie TK, Luwe K, Morse T, Hope C, Beverland IJ. Exposure to Air Pollution in Rural Malawi: Impact of Cooking Methods on Blood Pressure and Peak Expiratory Flow. International Journal of Environmental Research and Public Health. 2021; 18(14):7680. https://doi.org/10.3390/ijerph18147680
Chicago/Turabian StyleMabonga, Fiona, Tara K. Beattie, Kondwani Luwe, Tracy Morse, Caitlin Hope, and Iain J. Beverland. 2021. "Exposure to Air Pollution in Rural Malawi: Impact of Cooking Methods on Blood Pressure and Peak Expiratory Flow" International Journal of Environmental Research and Public Health 18, no. 14: 7680. https://doi.org/10.3390/ijerph18147680
APA StyleMabonga, F., Beattie, T. K., Luwe, K., Morse, T., Hope, C., & Beverland, I. J. (2021). Exposure to Air Pollution in Rural Malawi: Impact of Cooking Methods on Blood Pressure and Peak Expiratory Flow. International Journal of Environmental Research and Public Health, 18(14), 7680. https://doi.org/10.3390/ijerph18147680