Measurement Equivalence between the Original and Estimated Mini-Mental State Examination in People with Dementia



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.T.; Prina, M. World Alzheimer Report 2015: The Global Impact of Dementia; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Kishita, N.; Backhouse, T.; Mioshi, E. Nonpharmacological interventions to improve depression, anxiety, and quality of life (QoL) in people with dementia: An overview of systematic reviews. J. Geriatr. Psychiatry Neurol. 2020, 33, 28–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltes, B.B.; Rudolph, C.W.; Zacher, H. Work across the Lifespan; Elsevier: New York, NY, USA, 2019. [Google Scholar]
- Mazzi, M.C.; Iavarone, A.; Russo, G.; Musella, C.; Milan, G.; D’Anna, F.; Garofalo, E.; Chieffi, S.; Sannino, M.; Illario, M.; et al. Mini-mental state examination: New normative values on subjects in Southern Italy. Aging Clin. Exp. Res. 2020, 32, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Tom, S.E.; Phadke, M.; Hubbard, R.A.; Crane, P.K.; Stern, Y.; Larson, E.B. Association of demographic and early-life socioeconomic factors by birth cohort with dementia incidence among US adults born between 1893 and 1949. JAMA Netw. Open 2020, 3, e2011094. [Google Scholar] [CrossRef] [PubMed]
- Ideno, Y.; Takayama, M.; Hayashi, K.; Takagi, H.; Sugai, Y. Evaluation of a Japanese version of the mini-mental state examination in elderly persons. Geriatr. Gerontol. Int. 2012, 12, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.N.; Wang, P.N.; Liu, C.Y.; Chen, W.T.; Lee, Y.C.; Liu, H.C. Cutoff scores of the cognitive abilities screening instrument, Chinese version in screening of dementia. Dement. Geriatr. Cogn. Disord. 2002, 14, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Larson, E.B.; Shofer, J.B.; Crane, P.K.; Gibbon, L.E.; McCormick, W.; Bowen, J.D.; Thompson, M.L. Cognitive trajectory changes over 20 years before dementia diagnosis: A large cohort study. J. Am. Geriatr. Soc. 2017, 65, 2627–2633. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Teng, E.L.; Hasegawa, K.; Homma, A.; Imai, Y.; Larson, E.; Graves, A.; Sugimoto, K.; Yamaguchi, T.; Sasaki, H.; Chiu, D.; et al. The cognitive abilities screening instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int. Psychogeriatr. 1994, 6, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Delice, A. The sampling issues in quantitiative research. Educ. Sci. Theory Pract. 2010, 10, 2001–2018. [Google Scholar]
- Faber, J.; Fonseca, L.M. How sample size influences research outcome. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Honda, T.; Narazaki, K.; Chen, T.; Nofuji, Y.; Kumagai, S. Global cognitive performance and frailty in non-demented community-dwelling older adults: Findings from the S asaguri G enkimon Study. Geriatr. Gerontol. Int. 2016, 16, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Chiu, E.C.; Yip, P.K.; Woo, P.; Lin, Y.T. Test.-retest reliability and minimal detectable change of the Cognitive Abilities Screening Instrument in patients with dementia. PLoS ONE 2019, 14, e0216450. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.C. The clinical dementia rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C. Clinical dementia rating: A reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int. Psychogeriatr. 1997, 9 (Suppl. S1), 173–176. [Google Scholar] [CrossRef] [PubMed]
- Chaves, M.L.F.; Camozzato, A.L.; Godinho, C.; Kochhann, R.; Schuh, A.; De Almeida, V.L.; Kaye, J. Validity of the clinical dementia rating scale for the detection and staging of dementia in Brazilian patients. Alzheimer Dis. Assoc. Disord. 2007, 21, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, B.R.; Oliveira, C.B.; Araujo, G.M.D.; Silva, F.G.; Damato, T.M.; Pinto, R.Z.; Christofaro, D.G. Is there equivalence between the electronic and paper version of the questionnaires for assessment of patients with chronic low back pain? Spine 2018, 45, 1. [Google Scholar] [CrossRef] [PubMed]
- Dobson, F.; Hinman, R.S.; Hall, M.; Marshall, C.J.; Sayer, T.; Anderson, C.; Newcomb, N.; Stratford, P.W.; Bennell, K.L. Reliability and measurement error of the Osteoarthritis Research Society International (OARSI) recommended performance-based tests of physical function in people with hip and knee osteoarthritis. Osteoarthr. Cartil. 2017, 25, 1792–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, E.C.; Lee, S.C. Test.-retest reliability of the Wisconsin Card Sorting Test. in people with schizophrenia. Disabil. Rehabil. 2021, 43, 996–1000. [Google Scholar] [CrossRef] [PubMed]
- Hong, I.; Kim, Y.J.; Sonnenfeld, M.L.; Grattan, E.; Reistetter, T.A. Disability measurement for Korean community-dwelling adults with stroke: Item-level psychometric analysis of the Korean longitudinal study of ageing. Ann. Rehabil. Med. 2018, 42, 336–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, C.F.; Hwang, A.W.; Liou, T.H.; Chiu, T.Y.; Hsu, H.Y.; Chi, W.C.; Wu, T.F.; Chang, B.S.; Lu, S.J.; Liao, H.F.; et al. Validity and reliability of the Functioning Disability Evaluation Scale-Adult Version based on the WHODAS 2.0—36 items. J. Formos. Med. Assoc. 2014, 113, 839–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Characteristic | |
|---|---|
| Age (years), mean (SD) | 83.1 (7.9) |
| Gender, n (%) | |
| Male | 28 (49.1) |
| Female | 29 (50.9) |
| CDR, mean (SD) | 1.24 (0.70) |
| Total Score and Domain Score | Original MMSE Mean ± SD | Estimated MMSE Mean ± SD | ICC (95% CI) | r (p-Value) | SEM (SEM%) | t-Test (p-Value) | Cohen’s d |
|---|---|---|---|---|---|---|---|
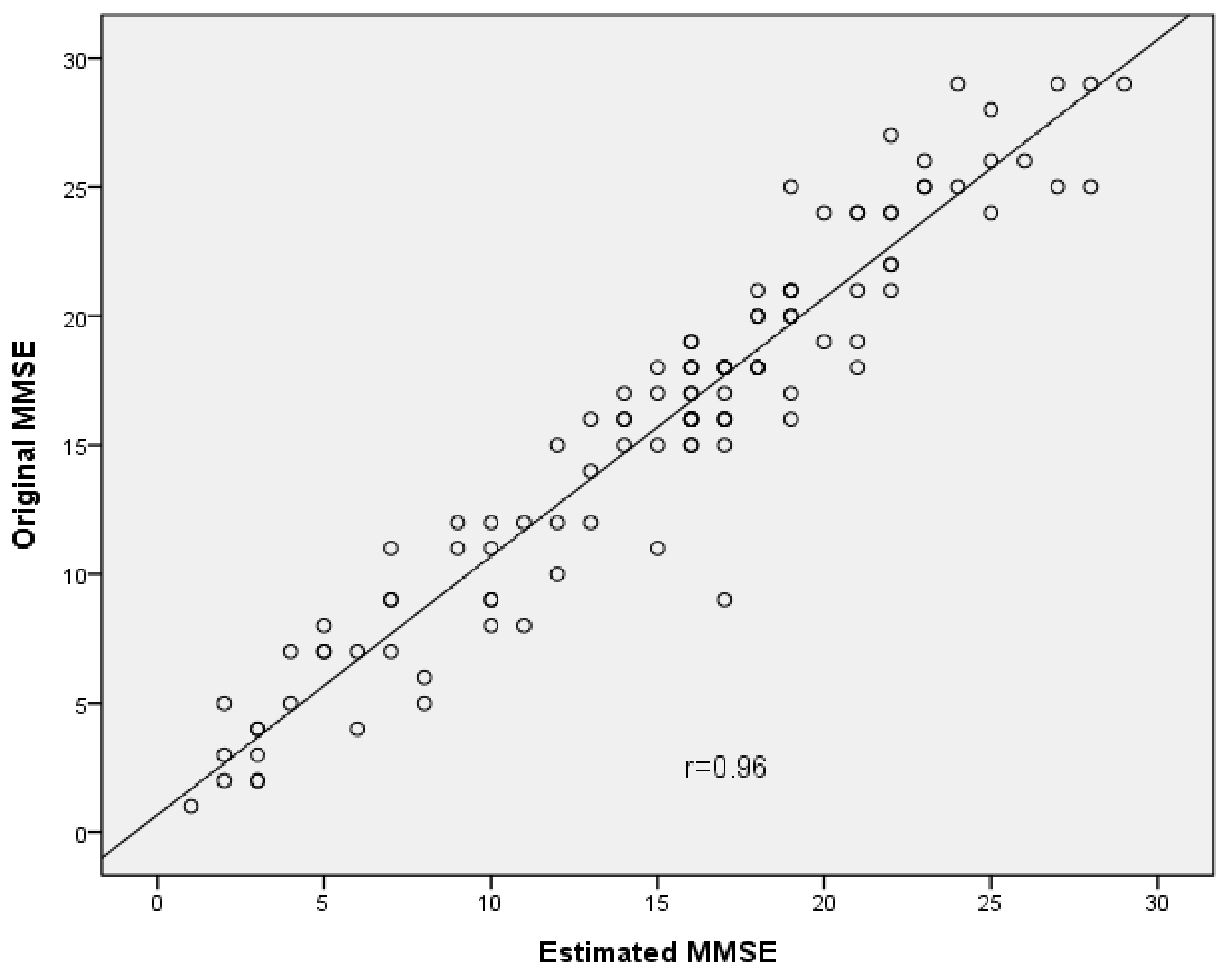
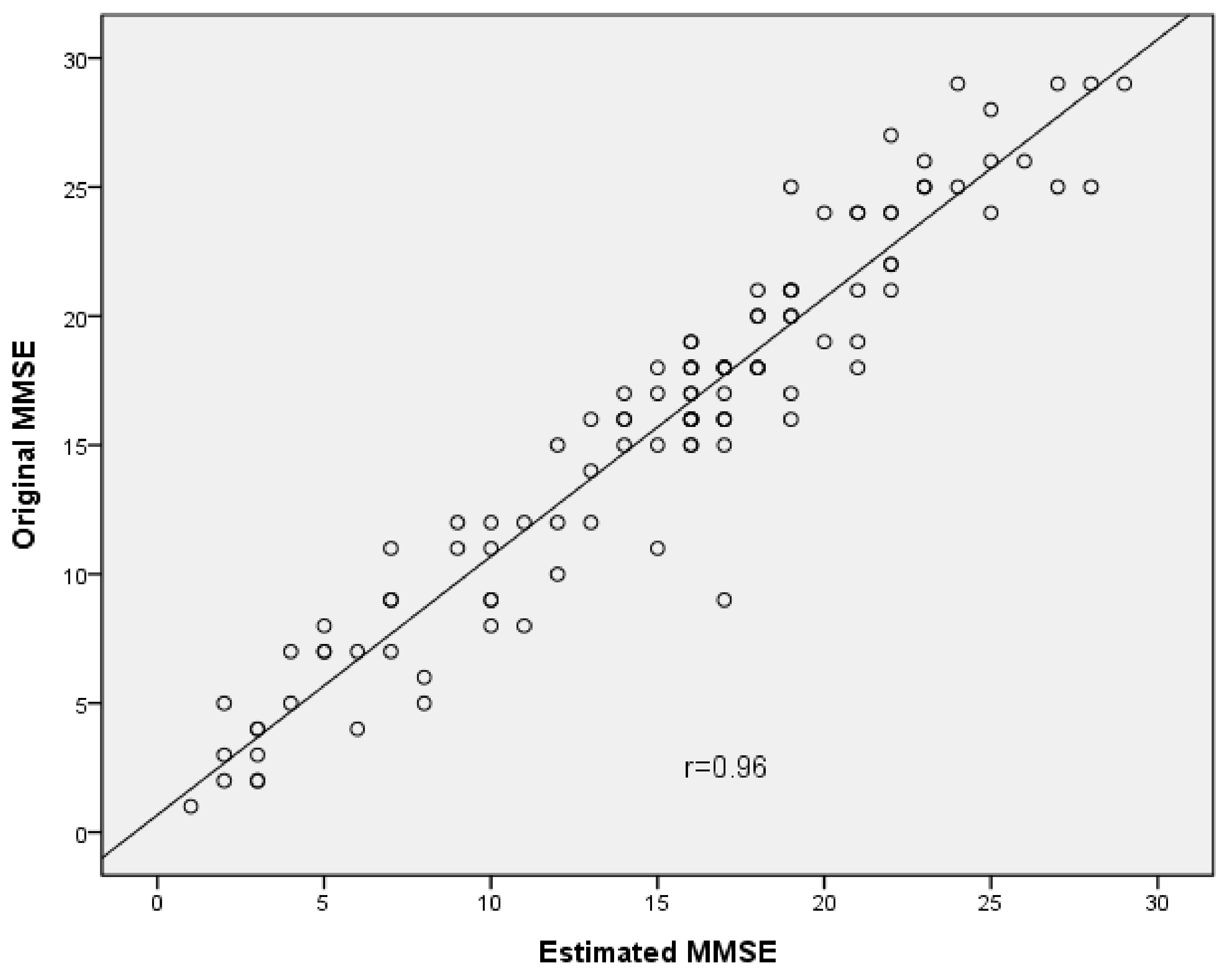
| Total score | 15.88 ± 7.17 | 15.18 ± 6.85 | 0.95 (0.92, 0.97) | 0.96 (<0.001) | 0.18 (0.6%) | 3.51 (0.001) * | 0.10 |
| Orientation | 4.43 ± 2.98 | 4.15 ± 3.03 | 0.93 (0.90, 0.96) | 0.93 (<0.001) | 0.11 (1.1%) | 2.70 (0.008) * | 0.09 |
| Registration | 2.71 ± 0.67 | 2.61 ± 0.79 | 0.62 (0.49, 0.72) | 0.63 (<0.001) | 0.14 (4.6%) | 1.65 (0.101) | 0.14 |
| Attention and calculation | 2.17 ± 1.78 | 2.04 ± 1.67 | 0.62 (0.49, 0.72) | 0.62 (<0.001) | 0.33 (6.6%) | 0.95 (0.344) | 0.08 |
| Recall | 0.38 ± 0.89 | 0.33 ± 0.81 | 0.88 (0.82, 0.91) | 0.88 (<0.001) | 0.05 (1.7%) | 1.35 (0.181) | 0.06 |
| Language | 5.68 ± 2.28 | 5.43 ± 2.26 | 0.91 (0.87, 0.94) | 0.92 (<0.001) | 0.10 (1.1%) | 2.92 (0.004) * | 0.11 |
| Visual-constructional ability | 0.51 ± 0.50 | 0.64 ± 0.48 | 0.64 (0.50, 0.74) | 0.66 (<0.001) | 0.09 (8.9%) | −3.27 (0.001) * | 0.27 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, E.-C.; Chien, T.-H.; Lee, Y.-C. Measurement Equivalence between the Original and Estimated Mini-Mental State Examination in People with Dementia. Int. J. Environ. Res. Public Health 2021, 18, 7616. https://doi.org/10.3390/ijerph18147616
Chiu E-C, Chien T-H, Lee Y-C. Measurement Equivalence between the Original and Estimated Mini-Mental State Examination in People with Dementia. International Journal of Environmental Research and Public Health. 2021; 18(14):7616. https://doi.org/10.3390/ijerph18147616
Chicago/Turabian StyleChiu, En-Chi, Tzu-Hua Chien, and Ya-Chen Lee. 2021. "Measurement Equivalence between the Original and Estimated Mini-Mental State Examination in People with Dementia" International Journal of Environmental Research and Public Health 18, no. 14: 7616. https://doi.org/10.3390/ijerph18147616
APA StyleChiu, E.-C., Chien, T.-H., & Lee, Y.-C. (2021). Measurement Equivalence between the Original and Estimated Mini-Mental State Examination in People with Dementia. International Journal of Environmental Research and Public Health, 18(14), 7616. https://doi.org/10.3390/ijerph18147616