
Impact of the Childcare Physical Activity (PLAY) Policy on Young Children’s Physical Activity and Sedentary Time: A Pilot Clustered Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Description of the Childcare PLAY Policy
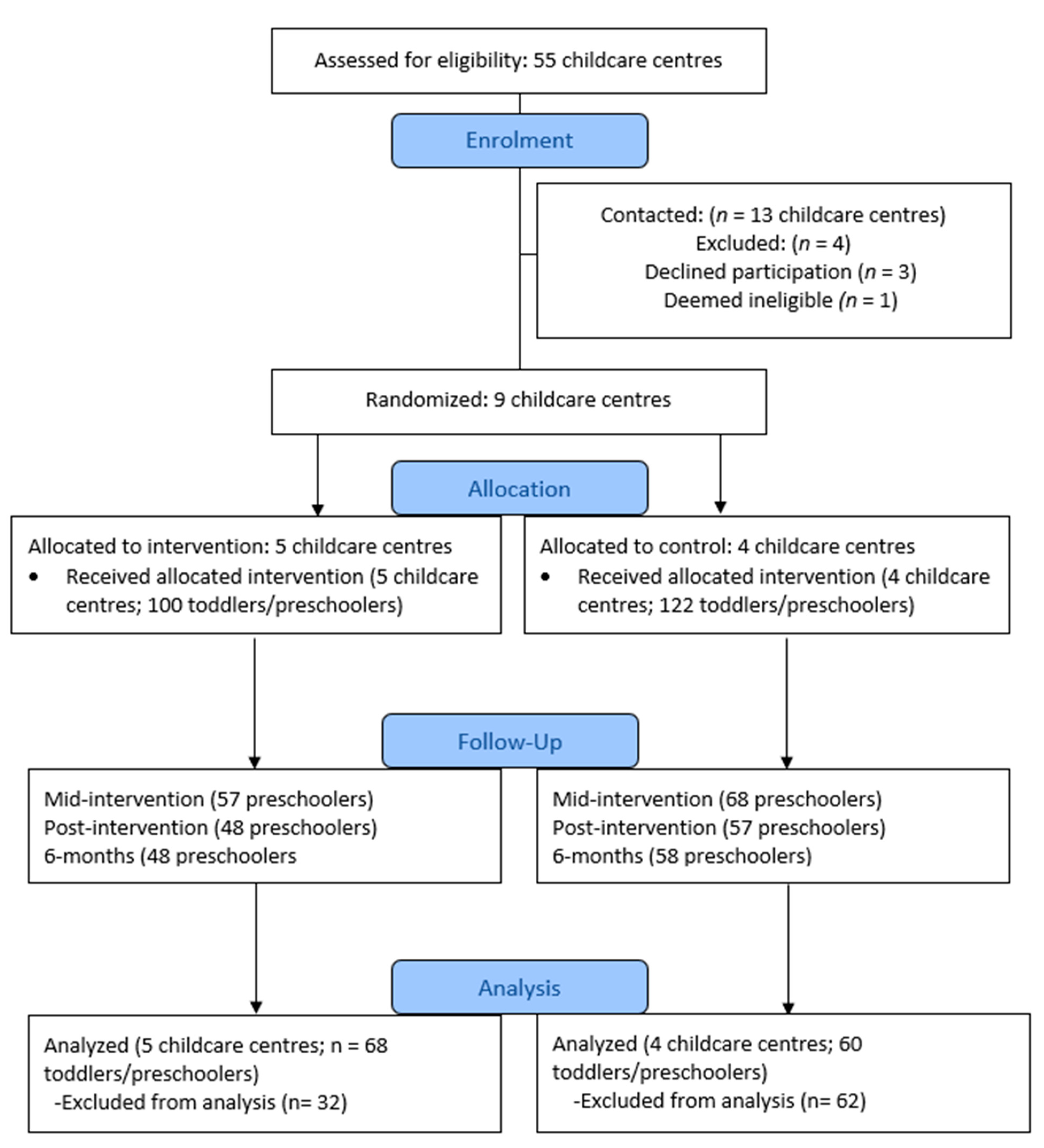
2.2. Study Design and Recruitment
2.3. Participants
2.4. Data Collection
2.5. Instruments and Tools
2.6. Data Analysis
3. Results
3.1. Description of Sample
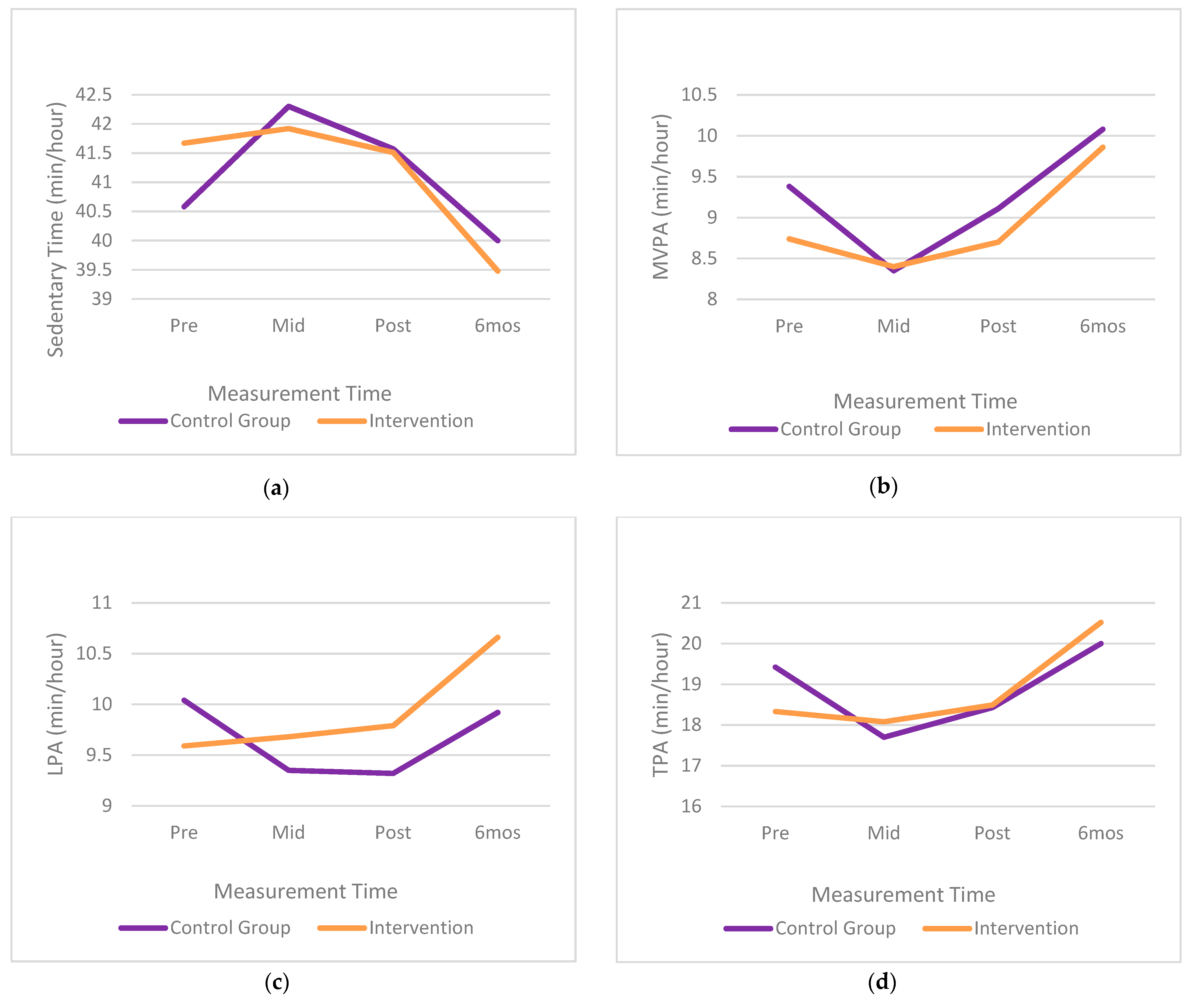
3.2. Effects of Childcare PLAY Policy Intervention on Participants’ Activity Levels
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body mass index |
| ECE | Early childhood educator |
| CSEP | Canadian Society for Exercise Physiology |
| LPA | Light physical activity |
| MVPA | Moderate-to-vigorous physical activity |
| PLAY | Physical Activity |
| RCT | Randomized controlled trial |
| REB | Research ethics board |
| TPA | Total physical activity |
References
- Timmons, B.W.; Leblanc, A.G.; Carson, V.; Gorber, S.C.; Dillman, C.; Janssen, I.; Kho, M.E.; Spence, J.C.; Stearns, J.A.; Tremblay, M.S. Systematic review of physical activity and health in the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 773–792. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Lee, E.-Y.; Hewitt, L.; Jennings, C.; Hunter, S.; Kuzik, N.; Stearns, J.A.; Unrau, S.P.; Poitras, V.J.; Gray, C.; et al. Systematic review of the relationships between physical activity and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 854. [Google Scholar] [CrossRef]
- Colley, R.C.; Garriguet, D.; Adamo, K.B.; Carson, V.; Janssen, I.; Timmons, B.W.; Tremblay, M.S. Physical activity and sedentary behavior during the early years in Canada: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leblanc, A.G.; Spence, J.C.; Carson, V.; Connor Gorber, S.; Dillman, C.; Janssen, I.; Kho, M.E.; Stearns, J.A.; Timmons, B.W.; Tremblay, M.S. Systematic review of sedentary behaviour and health indicators in the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 753–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poitras, V.J.; Gray, C.E.; Janssen, X.; Aubert, S.; Carson, V.; Faulkner, G.; Goldfield, G.S.; Reilly, J.J.; Sampson, M.; Tremblay, M.S. Systematic review of the relationships between sedentary behaviour and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 65–89. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Jackson, D.M.; Montgomery, C.; Kelly, L.A.; Slater, C.; Grant, S.; Paton, J.Y. Total energy expenditure and physical activity in young Scottish children: Mixed longitudinal study. Lancet 2004, 363, 211–212. [Google Scholar] [CrossRef]
- Canadian Society for Exercise Physiology. Canadian 24-Hour Movement Guidelines for the Early Years (0-4 years): An Integration of Physical Activity, Sedentary Behaviour and Sleep. BMC Public Health 2017, 17, 1–32. Available online: https://csepguidelines.ca/early-years-0-4/ (accessed on 17 December 2018).
- Tremblay, M.S.; Chaput, J.-P.; Adamo, K.B.; Aubert, S.; Barnes, J.D.; Choquette, L.; Duggan, M.; Faulkner, G.; Goldfield, G.S.; Gray, C.E.; et al. Canadian 24-Hour Movement Guidelines for the Early Years (0–4 years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep. BMC Public Health 2017, 17, 874. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019; Available online: http://www.who.int/iris/handle/10665/311664 (accessed on 12 July 2021).
- Copeland, K.A.; Khoury, J.C.; Kalkwarf, H.J. Child care center characteristics associated with preschoolers’ physical activity. Am. J. Prev. Med. 2016, 50, 470–479. [Google Scholar] [CrossRef] [Green Version]
- Vanderloo, L.M.; Tucker, P.; Johnson, A.M.; Van Zandvoort, M.M.; Burke, S.M.; Irwin, J.D. The influence of centre-based childcare on preschoolers’ physical activity levels: A cross-sectional study. Int. J. Env. Res. Public Health 2014, 11, 1794–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, K.T.; Vanderloo, L.M.; Bruijns, B.A.; Truelove, S.; Tucker, P. Physical activity and sedentary time among preschoolers in centre-based childcare: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 117. [Google Scholar] [CrossRef] [PubMed]
- Tucker, P.; Vanderloo, L.M.; Burke, S.M.; Irwin, J.D.; Johnson, A.M. Prevalence and influences of preschoolers’ sedentary behaviors in early learning centers: A cross-sectional study. BMC Pediatr. 2015, 15, 128. [Google Scholar] [CrossRef] [Green Version]
- Vanderloo, L.M. Screen-viewing among preschoolers in childcare: A systematic review. BMC Public Health 2014, 14, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.A.; Christakis, D.A. The association between television viewing and irregular sleep schedules among children less than 3 years of age. Pediatrics 2005, 116, 851–856. [Google Scholar] [CrossRef]
- Simonato, I.; Janosz, M.; Archambault, I.; Pagani, L.S. Prospective associations between toddler televiewing and subsequent lifestyle habits in adolescence. Prev. Med. 2018, 110, 24–30. [Google Scholar] [CrossRef]
- Hesketh, K.R.; Lakshman, R.; Sluijs, E.M.F. Barriers and facilitators to young children’s physical activity and sedentary behaviour: A systematic review and synthesis of qualitative literature. Obes. Rev. 2017, 18, 987–1017. [Google Scholar] [CrossRef]
- Robinson, L.E.; Webster, E.K.; Logan, S.W.; Lucas, W.A.; Barber, L.T. Teaching practices that promote motor skills in early childhood settings. Early Child. Educ. J. 2011, 40, 79–86. [Google Scholar] [CrossRef]
- Vanderloo, L.M.; Tucker, P. Physical Activity and Sedentary Behavior Legislation in Canadian Childcare Facilities: An Update. BMC Public Health 2018, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Vercammen, K.A.; Frelier, J.M.; Poole, M.K.; Kenney, E.L. Obesity prevention in early care and education: A comparison of licensing regulations across Canadian provinces and territories. J. Public Health 2020, 42, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ott, E.; Vanderloo, L.M.; Tucker, P. Physical activity and screen-viewing policies in Canadian childcare centers. BMC Public Health 2019, 19, 145. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.C.; Finch, M.; Wolfenden, L.; Fitzgerald, M.; Morgan, P.J.; Jones, J.; Freund, M.; Wiggers, J. Child physical activity levels and associations with modifiable characteristics in centre-based childcare. Aust. N. Z. J. Public Health 2015, 39, 232–236. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, S.; Morton, S.M.B.; Wall, C.R. Physical activity and screen use policy and practices in childcare: Results from a survey of early childhood education services in New Zealand. Aust. N. Z. J. Public Health 2016, 40, 319–325. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.; Dowda, M.; Neelon, S.E.; Neelon, B.; Pate, R. Effects of a new state policy on physical activity practices in child care centers in South Carolina. Am. J. Public Health 2017, 107, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.K.; Hales, D.P.; Tate, D.F.; Rubin, D.A.; Benjamin, S.E.; Ward, D.S. The Childcare Environment and Children’s Physical Activity. Am. J. Prev. Med. 2008, 34, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Stephens, R.L.; Xu, Y.; Lesesne, C.A.; Dunn, L.; Kakietek, J.; Jernigan, J. Relationship Between Child Care Centers’ Compliance with Physical Activity Regulations and Children’s Physical Activity, New York City, 2010. Prev. Chronic. Dis. 2014, 11, E179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Ren, H.; Yin, Z.; Wang, L.; Zhixiong, Z. A policy-driven multifaceted approach for early childhood physical fitness promotion: Impacts on body composition and physical fitness in young Chinese children. BMC Pediatr. 2014, 14, 118. [Google Scholar] [CrossRef] [Green Version]
- Dowda, M.; Brown, W.H.; McIver, K.L.; Pfeiffer, K.A.; O’Neill, J.R.; Addy, C.L.; Pate, R.R. Policies and Characteristics of the Preschool Environment and Physical Activity of Young Children. Pediatrics 2009, 123, e261–e266. [Google Scholar] [CrossRef] [Green Version]
- Tandon, P.S.; Saelens, B.E.; Zhou, C. A Comparison of Preschoolers’ Physical Activity Indoors versus Outdoors at Child Care. Int. J. Environ. Res. Public Health 2018, 15, 2463. [Google Scholar] [CrossRef] [Green Version]
- Stacey, F.G.; Finch, M.; Wolfenden, L.; Grady, A.; Jessop, K.; Wedesweiler, T.; Bartlem, K.; Jones, J.; Sutherland, R.; Vandevijvere, S.; et al. Evidence of the Potential Effectiveness of Centre-Based Childcare Policies and Practices on Child Diet and Physical Activity: Consolidating Evidence from Systematic Reviews of Intervention Trials and Observational Studies. Curr. Nutr. Rep. 2017, 6, 228–246. [Google Scholar] [CrossRef]
- Staiano, A.E.; Webster, E.K.; Allen, A.T.; Jarrell, A.R.; Martin, C.K. Screen-Time Policies and Practices in Early Care and Education Centers in Relationship to Child Physical Activity. Child. Obes. 2018, 14, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Government of Ontario. Child Care and Early Years Act. 2014. Available online: https://www.ontario.ca/laws/statute/14c11 (accessed on 12 July 2021).
- Tucker, P.; Driediger, M.; Vanderloo, L.M.; Burke, S.M.; Irwin, J.D.; Johnson, A.M.; Shelley, J.; Timmons, B.W. Exploring the Feasibility and Effectiveness of a Childcare PhysicaL ActivitY (PLAY) Policy: Rationale and Protocol for a Pilot, Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4400. [Google Scholar] [CrossRef] [Green Version]
- McClain, J.J.; Tudor-Locke, C. Objective monitoring of physical activity in children: Considerations for instrument selection. J. Sci. Med. Sport. 2009, 12, 526–533. [Google Scholar] [CrossRef]
- Engelen, L.; Bundy, A.C.; Naughton, G.; Simpson, J.M.; Bauman, A.; Ragen, J.; Baur, L.; Wyver, S.; Tranter, P.; Niehues, A.; et al. Increasing physical activity in young primary school children—It’s child’s play: A cluster randomised controlled trial. Prev. Med. 2013, 56, 319–325. [Google Scholar] [CrossRef]
- Alhassan, S.; Laurent CSt Burkart, S.; Greever, C.J.; Ahmadi, M. Effects of integrating physical activity into early education learning standards on preschoolers’ physical activity levels. Med. Sci. Sport Exerc. 2018, 50, 762. [Google Scholar] [CrossRef]
- Pate, R.R.; Almeida, M.J.; McIver, K.L.; Pfeiffer, K.A.; Dowda, M. Validation and calibration of an accelerometer in preschool children. Obesity 2006, 14, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat 2002, 246, 1–190. [Google Scholar]
- Witjzes, A.L.; Kooijman, M.N.; Kiefte-de Jong, J.C.; de Vries, S.I.; Henrichs, J.; Jansen, W.; Jaddoe, V.W.; Hofman, A.; A Moll, H.; Raat, H. Correlates of physical activity in 2-year-old toddlers: The Generation R Study. J. Pediatr. 2013, 163, 791–799. [Google Scholar]
- Bunn, A.; Korpela, M. R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.r-project.org/ (accessed on 25 February 2019).
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D. Nlme: Linear and Nonlinear Mixed Effects Models. R Package Version 3.1-152. R Core Team, 2021. Available online: https://CRAN.R-project.org/package=nlme (accessed on 12 July 2021).
- Fox, J.; Weisberg, S. An {R} Companion to Applied Regression, 3th ed.; Sage: Thousand Oaks, CA, USA, 2019; Available online: https://socialsciences.mcmaster.ca/jfox/Books/Companion/ (accessed on 28 October 2020).
- Lenth, R. Emmeans: Estimaed Marginal Means, Aka Least-Squares, Version 1.4. 4. 2020. Available online: https://cran.r-project.org/web/packages/emmeans/emmeans.pdf (accessed on 12 July 2021).
- Wolfenden, L.; Jones, J.; Williams, C.M.; Finch, M.; Wyse, R.L.; Kingsland, M.; Tzelepsis, F.; Wiggers, J.; Williams, A.J.; Seward, K.; et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane Database Syst. Rev. 2015, 10. [Google Scholar] [CrossRef]
- Sterdt, E.; Pape, N.; Kramer, S.; Urban, M.; Werning, R.; Walter, R. Do preschools differ in promoting children’s physical activity? An instrument for the assessment of preschool physical activity programmes. BMC Public Health 2013, 13, 795. [Google Scholar] [CrossRef] [Green Version]
- Wolfenden, L.; Neve, M.; Farrell, L.; Lecathelinais, C.; Bell, C.; Milat, A.; Wiggers, J.; Sutherland, R. Physical activity policies and practices of childcare centres in Australia. J. Paediatr. Child Health 2011, 47, 73–76. [Google Scholar] [CrossRef]
- Breck, A.; Goodman, K.; Dunn, L.; Stephens, R.L.; Dawkins, N.; Dixon, B.; Jernigan, J.; Kakietek, J.; Lesesne, C.; Lessard, L.; et al. Evaluation design of New York City’s regulations on nutrition, physical activity, and screen time in early child care centers. Prev. Chronic. Dis. 2014, 11, E184. [Google Scholar] [CrossRef]
- LaRowe, T.L.; Tomayko, E.J.; Meinen, A.M.; Hoiting, J.; Saxler, C.; Cullen, B. Active Early: One-year policy intervention to increase physical activity among early care and education programs in Wisconsin. BMC Public Health 2016, 16, 607. [Google Scholar] [CrossRef] [Green Version]
- Henderson, K.E.; Grode, G.M.; O’Connell, M.L.; Schwartz, M.B. Environmental factors associated with physical activity in childcare centers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Vanderloo, L.M.; Tucker, P.; Johnson, A.M.; Holmes, J.D. Physical activity among preschoolers during indoor and outdoor childcare play periods. Appl. Physiol. Nutr. Metab. 2013, 38, 1173–1175. [Google Scholar] [CrossRef]
- Alhassan, S.; Nwaokelemeh, O.; Mendoza, A.; Shitole, S.; Puleo, E.; Pfeiffer, K.A.; Whitt-Glover, M.C. Feasibility and Effects of Short Activity Breaks for Increasing Preschool-Age Children’s Physical Activity Levels. J. Sch. Health 2016, 86, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Driediger, M.; Truelove, S.; Johnson, A.M.; Vanderloo, L.M.; Timmons, B.W.; Burke, S.M.; Irwin, J.D.; Tucker, P. The impact of shorter, more frequent outdoor play periods on preschoolers’ physical activity during childcare: A cluster randomized controlled trial. Int. J. Env. Res. Public Health 2019, 16, 4126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfenden, L.; Wiggers, J.; Morgan, P.; Razak, L.A.; Jones, J.; Finch, M.; Sutherland, R.; Lecathenlinais, C.; Gillham, K.; Yoong, S.L. A randomised controlled trial of multiple periods of outdoor free-play to increase moderate-to-vigorous physical activity among 3 to 6 year old children attending childcare: Study protocol. BMC Public Health 2016, 16, 926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, P.; Vanderloo, L.M.; Johnson, A.M.; Burke, S.M.; Irwin, J.D.; Gaston, A.; Driediger, M.; Timmons, B.W. Impact of the Supporting Physical Activity in the Childcare Environment (SPACE) intervention on preschoolers’ physical activity levels and sedentary time: A single-blind cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szpunar, M.; Johnson, A.M.; Driediger, M.V.; Burke, S.M.; Irwin, J.D.; Shelley, J.; Timmons, B.W.; Vanderloo, L.M.; Tucker, P. Implementation adherence and perspectives of the childcare PhysicaL ActivitY (PLAY) policy: A process evaluation. Health Educ Behav. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.; van Kann, D.H.; Stafleu, A.; Candel, M.J.; Dagnelie, P.C. Interaction between physical environment, social environment, and child characteristics in determining physical activity at childcare. Health Psychol. 2011, 30, 84. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Control | Experimental | p-Value |
|---|---|---|---|
| Age (years), M (SD) | 2.66 (0.58) | 2.65 (0.63) | 0.36 |
| Sex (male, female), n | 40, 45 | 40, 43 | 0.88 |
| Body mass index percentiles, M (SD) | 51.6 (30.4) | 53.3 (31.1) | 0.79 |
| Hours spent in childcare/week (hours) | 0.004 | ||
| <10 | 2 | 2 | |
| 10–19 | 2 | 2 | |
| 20–29 | 23 | 5 | |
| 30+ | 58 | 73 | |
| Ethnicity | 0.30 | ||
| Caucasian | 55 | 52 | |
| African Canadian | 7 | 2 | |
| Native/Aboriginal | 1 | 3 | |
| Arab | 7 | 3 | |
| Latin American | 4 | 4 | |
| Asian | 6 | 8 | |
| Other | 5 | 8 | |
| Family situation | 0.71 | ||
| Single-parent | 11 | 13 | |
| Double-parent | 74 | 68 | |
| Prefer not to answer | 1 | 2 | |
| Yearly household income | 0.48 | ||
| <20,000 | 10 | 9 | |
| 20–39,000 | 9 | 9 | |
| 40,000–59,000 | 7 | 7 | |
| 60,000–79,000 | 2 | 8 | |
| 80,000–99,000 | 6 | 8 | |
| 100,000–119,000 | 7 | 6 | |
| 120,000–149,000 | 6 | 5 | |
| More than 150,000 | 7 | 12 | |
| Highest level of education | 0.71 | ||
| Elementary school | 3 | 1 | |
| Secondary school | 10 | 13 | |
| College | 21 | 26 | |
| University | 35 | 27 | |
| Graduate school | 13 | 13 |
| Time | LPA | MVPA | TPA | Sedentary Time | ||||
|---|---|---|---|---|---|---|---|---|
| Control | Exp | Control | Exp | Control | Exp | Control | Exp | |
| Baseline | 10.04 (1.73) | 9.59 (2.04) | 9.38 (3.13) | 8.74 (3.71) | 19.42 (4.63) | 18.33 (5.43) | 40.58 (4.63) | 41.67 (5.43) |
| Mid | 9.35 (1.86) | 9.68 (2.02) | 8.35 (3.03) | 8.40 (3.47) | 17.70 (4.57) | 18.08 (5.20) | 42.30 (4.57) | 41.92 (5.20) |
| Post | 9.32 (1.84) | 9.79 (2.03) | 9.11 (3.21) | 8.70 (3.72) | 18.43 (4.64) | 18.49 (5.25) | 41.57 (4.64) | 41.51 (5.25) |
| 6-Month | 9.92 (1.53) | 10.66 (1.88) | 10.08 (2.83) | 9.86 (4.10) | 20.00 (3.88) | 20.52 (5.40) | 40.00 (3.88) | 39.48 (5.40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szpunar, M.; Driediger, M.; Johnson, A.M.; Vanderloo, L.M.; Burke, S.M.; Irwin, J.D.; Shelley, J.; Timmons, B.W.; Tucker, P. Impact of the Childcare Physical Activity (PLAY) Policy on Young Children’s Physical Activity and Sedentary Time: A Pilot Clustered Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 7468. https://doi.org/10.3390/ijerph18147468
Szpunar M, Driediger M, Johnson AM, Vanderloo LM, Burke SM, Irwin JD, Shelley J, Timmons BW, Tucker P. Impact of the Childcare Physical Activity (PLAY) Policy on Young Children’s Physical Activity and Sedentary Time: A Pilot Clustered Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(14):7468. https://doi.org/10.3390/ijerph18147468
Chicago/Turabian StyleSzpunar, Monika, Molly Driediger, Andrew M. Johnson, Leigh M. Vanderloo, Shauna M. Burke, Jennifer D. Irwin, Jacob Shelley, Brian W. Timmons, and Patricia Tucker. 2021. "Impact of the Childcare Physical Activity (PLAY) Policy on Young Children’s Physical Activity and Sedentary Time: A Pilot Clustered Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 14: 7468. https://doi.org/10.3390/ijerph18147468
APA StyleSzpunar, M., Driediger, M., Johnson, A. M., Vanderloo, L. M., Burke, S. M., Irwin, J. D., Shelley, J., Timmons, B. W., & Tucker, P. (2021). Impact of the Childcare Physical Activity (PLAY) Policy on Young Children’s Physical Activity and Sedentary Time: A Pilot Clustered Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(14), 7468. https://doi.org/10.3390/ijerph18147468