
A Service Evaluation of the Military HeadFIT Initiative: An Implementation Study

 , ,
, ,
Abstract
:1. Introduction
1.1. Defence Mental Health
1.2. Military Mental Health Interventions and Preventions
1.3. The HeadFIT Initiative
2. Materials and Methods
2.1. Study Population
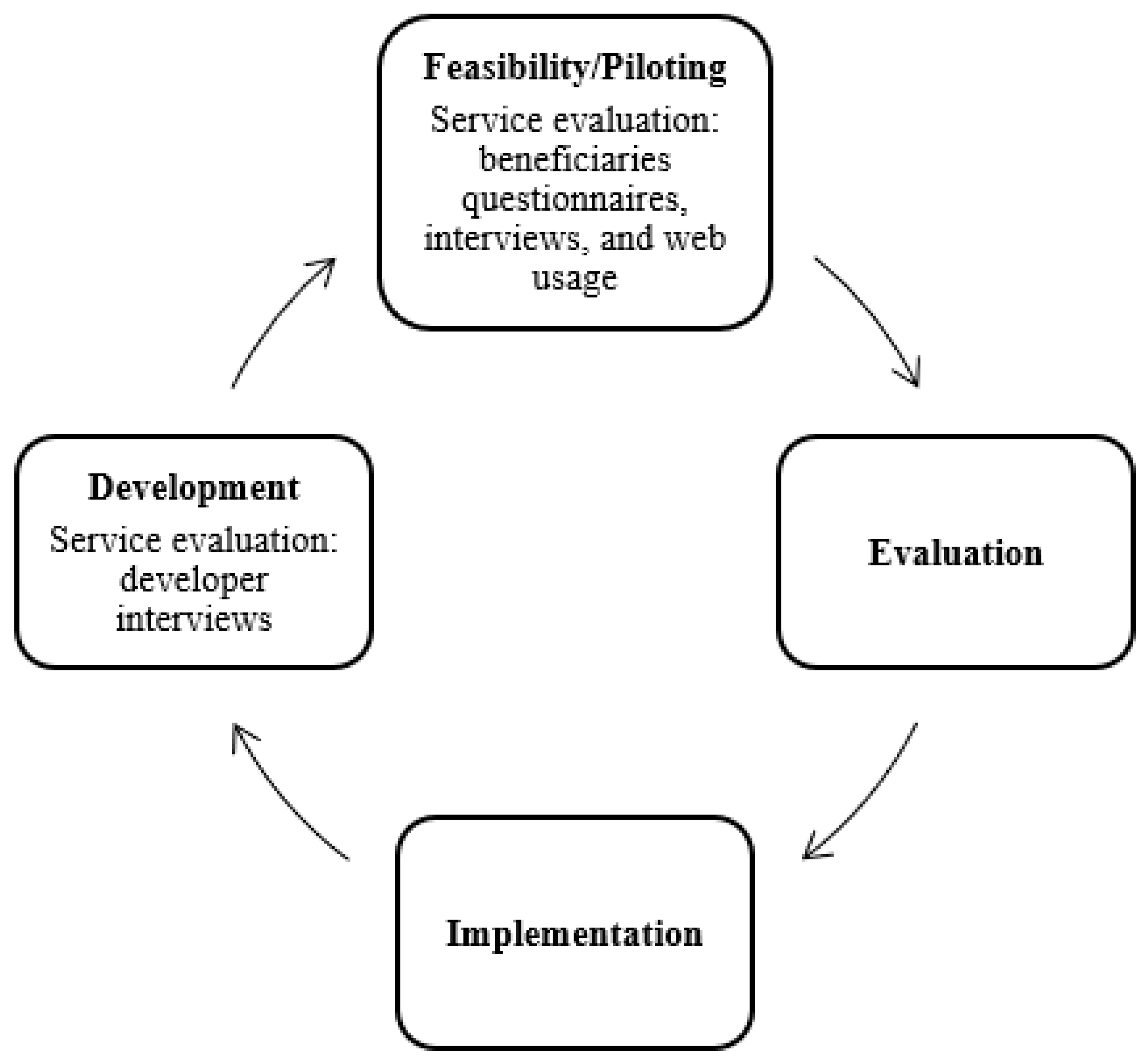
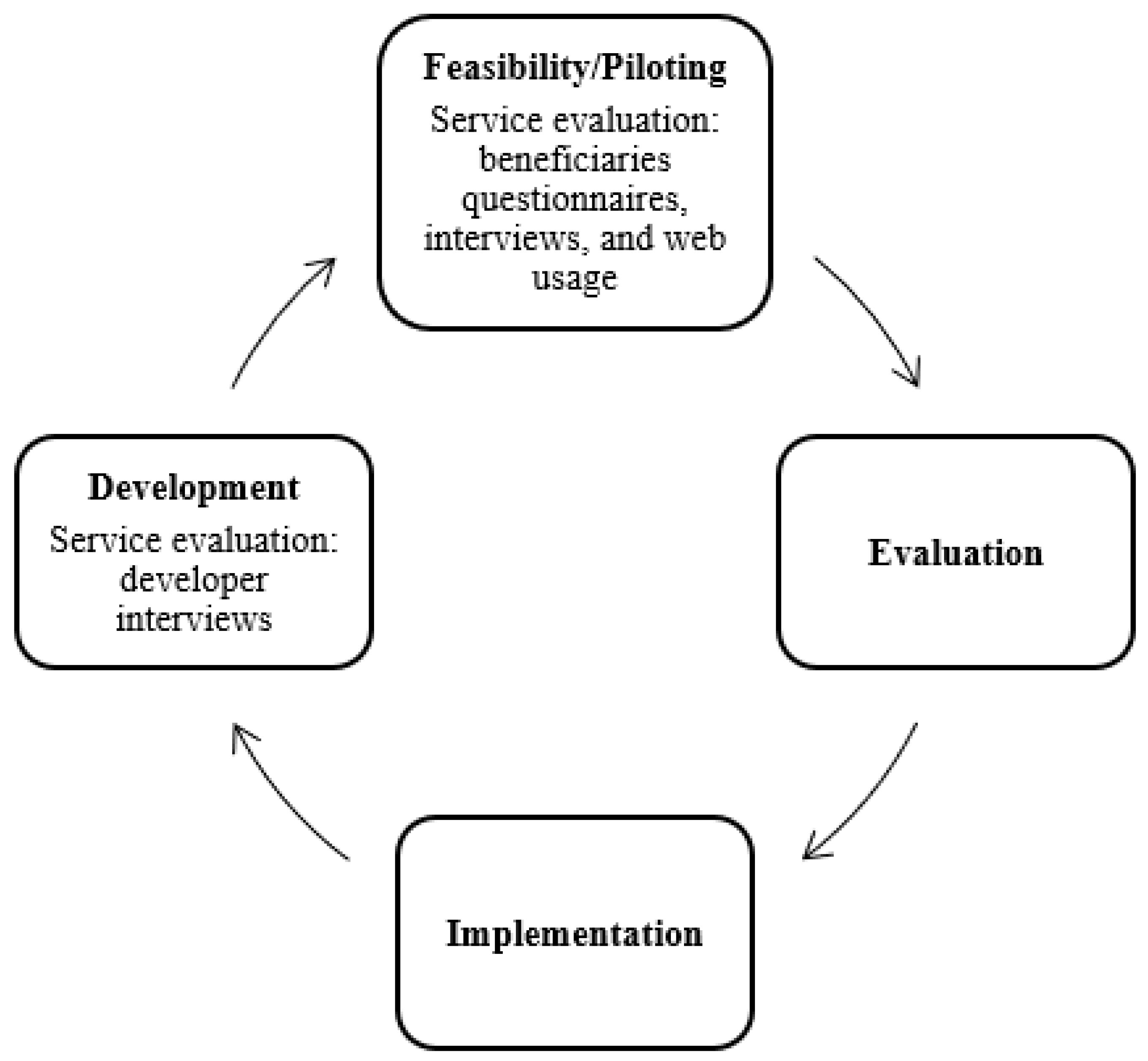
2.2. Design
- (1)
- Development of the theory and the intervention;
- (2)
- Feasibility/piloting the intervention with target users;
- (3)
- Evaluation of the effectiveness and changes to the intervention; and
- (4)
- Implementation and dissemination of the intervention.
Feasibility/Piloting: Beneficiaries
2.3. Recruitment
2.4. Evaluation Procedure and Materials
2.4.1. Questionnaires
2.4.2. Interviews
2.5. Analysis
2.5.1. Questionnaires
2.5.2. Interviews
3. Results
3.1. Questionnaires
3.1.1. Demographic Information
3.1.2. Opinions on Mental Fitness (S1)
3.1.3. Definition of Mental Fitness
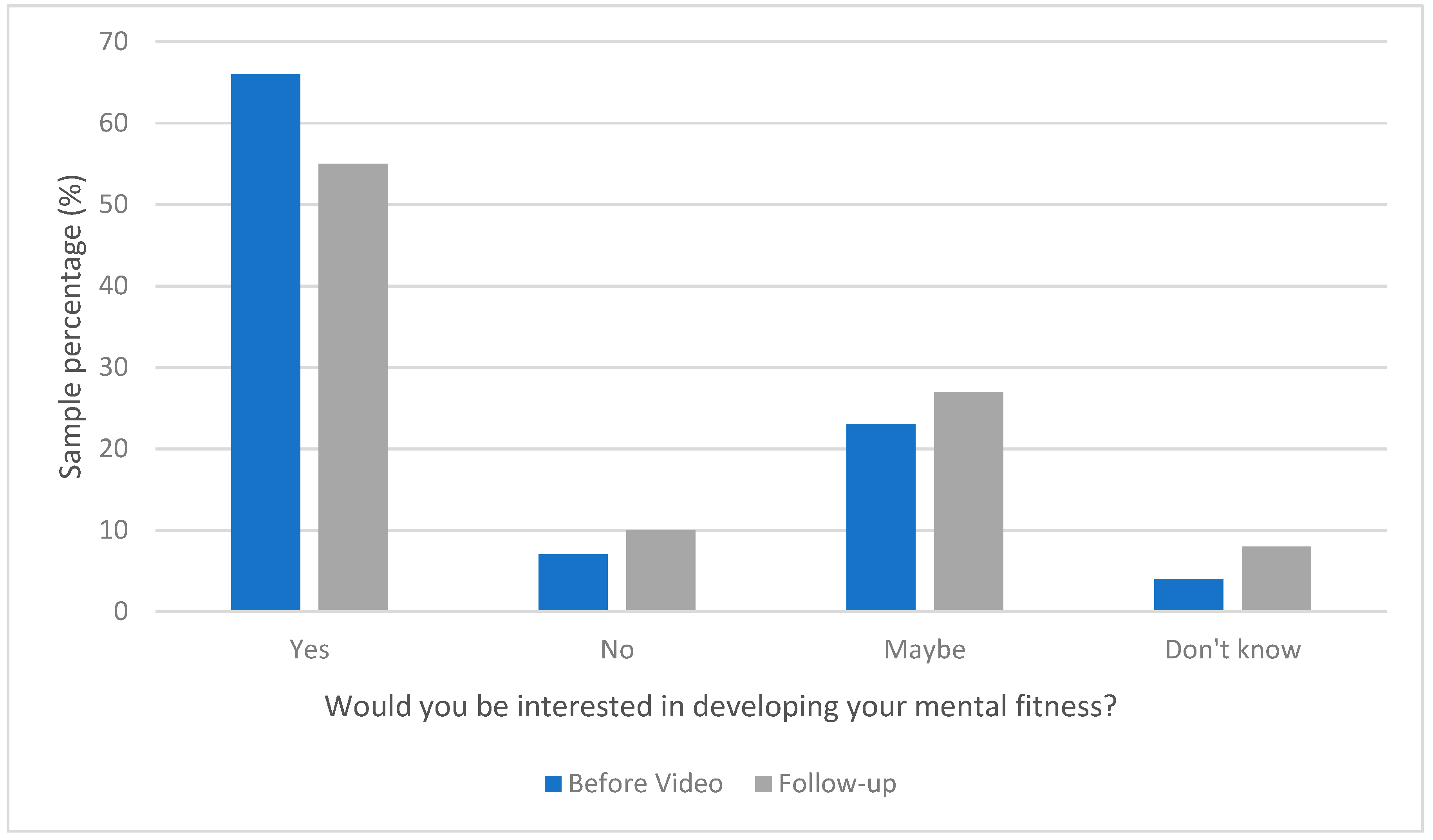
3.1.4. Developing Mental Fitness
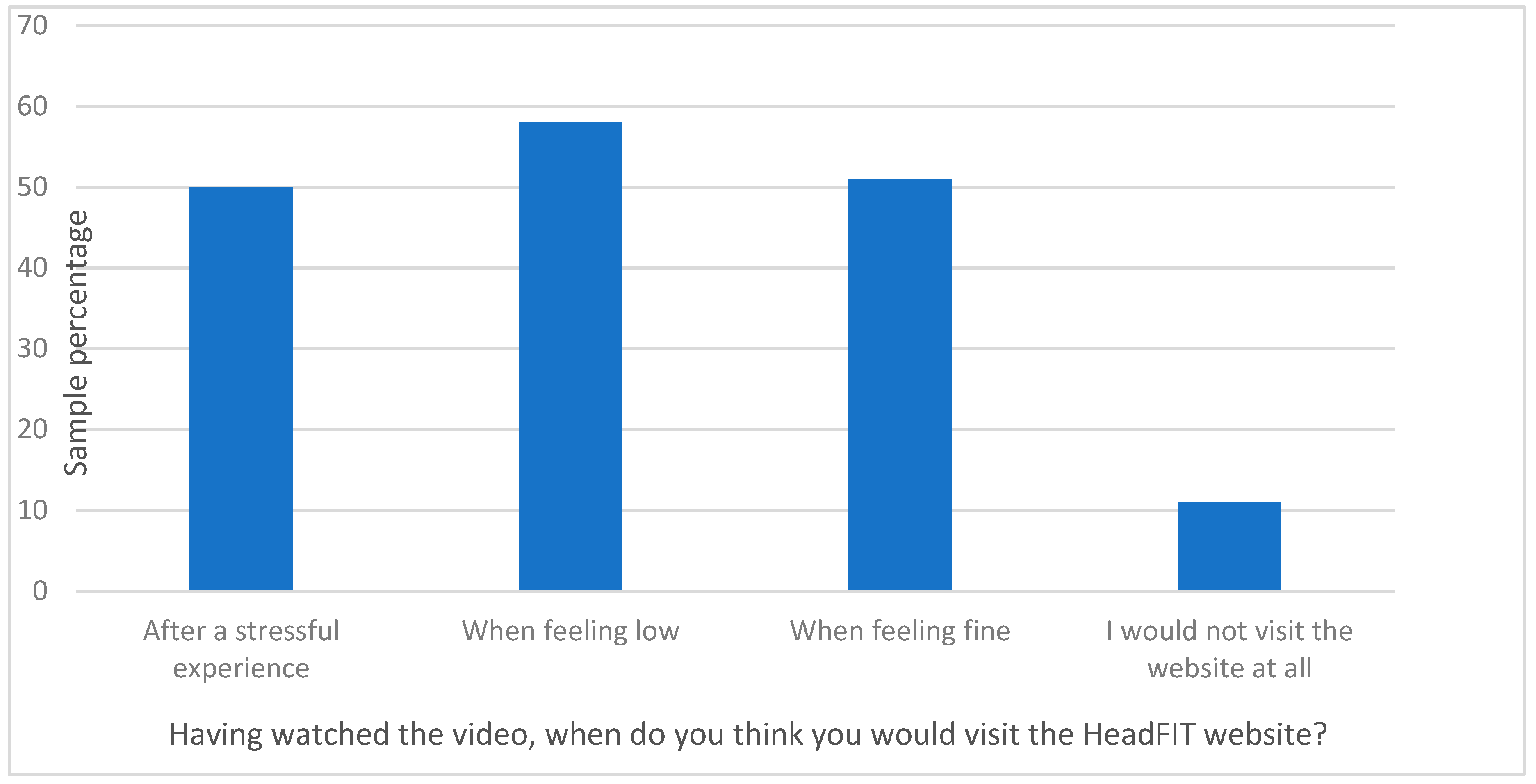
3.1.5. HeadFIT Video Feedback and Intent to Use (S2)
3.1.6. Feedback on the HeadFIT Website and Reported Use of HeadFIT (S3)
Reported Use of the Website
Perceived Ability of HeadFIT to Affect Mental Fitness
3.1.7. Feedback on the HeadFIT Website
3.2. Interviews
Demographics
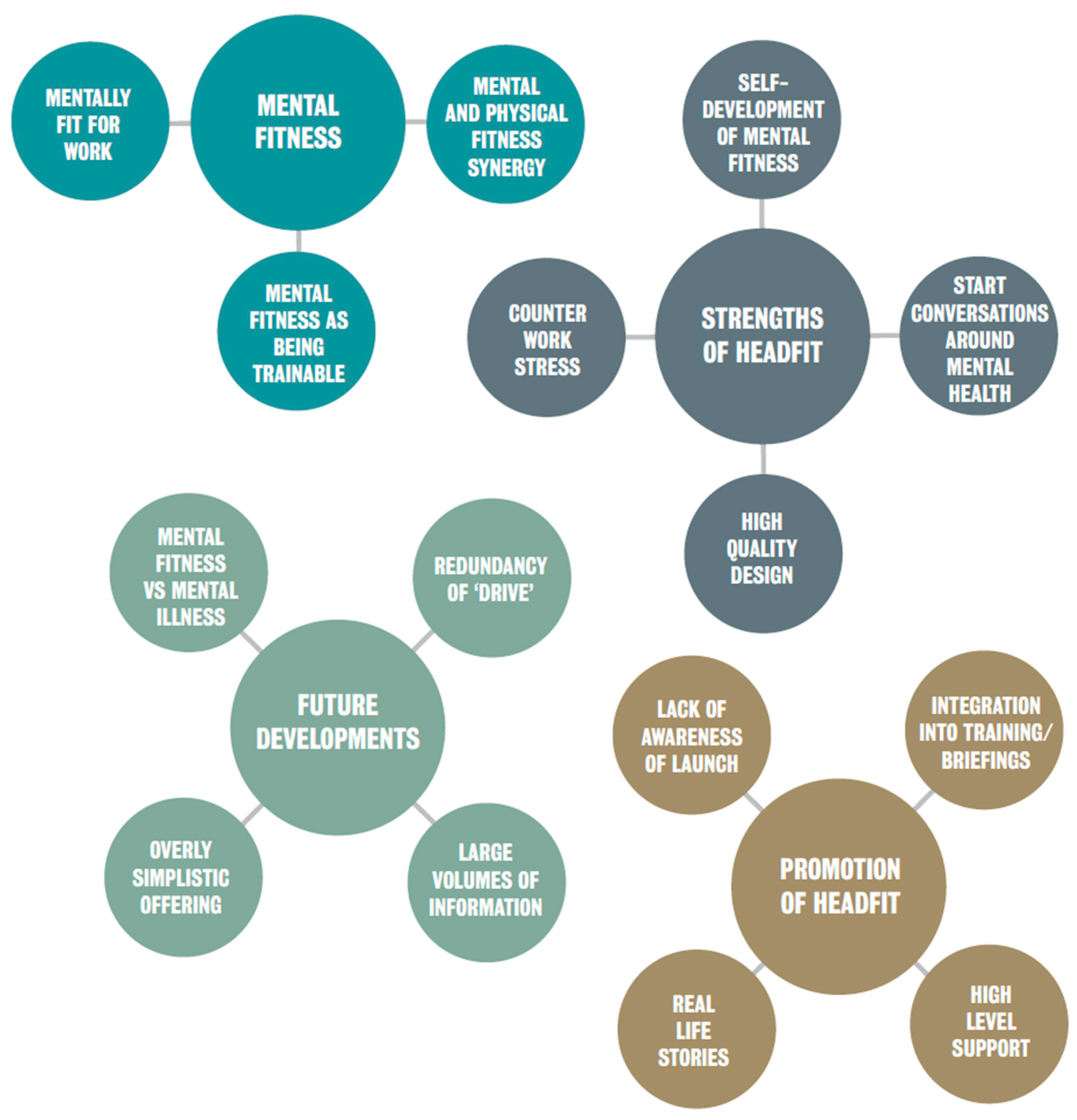
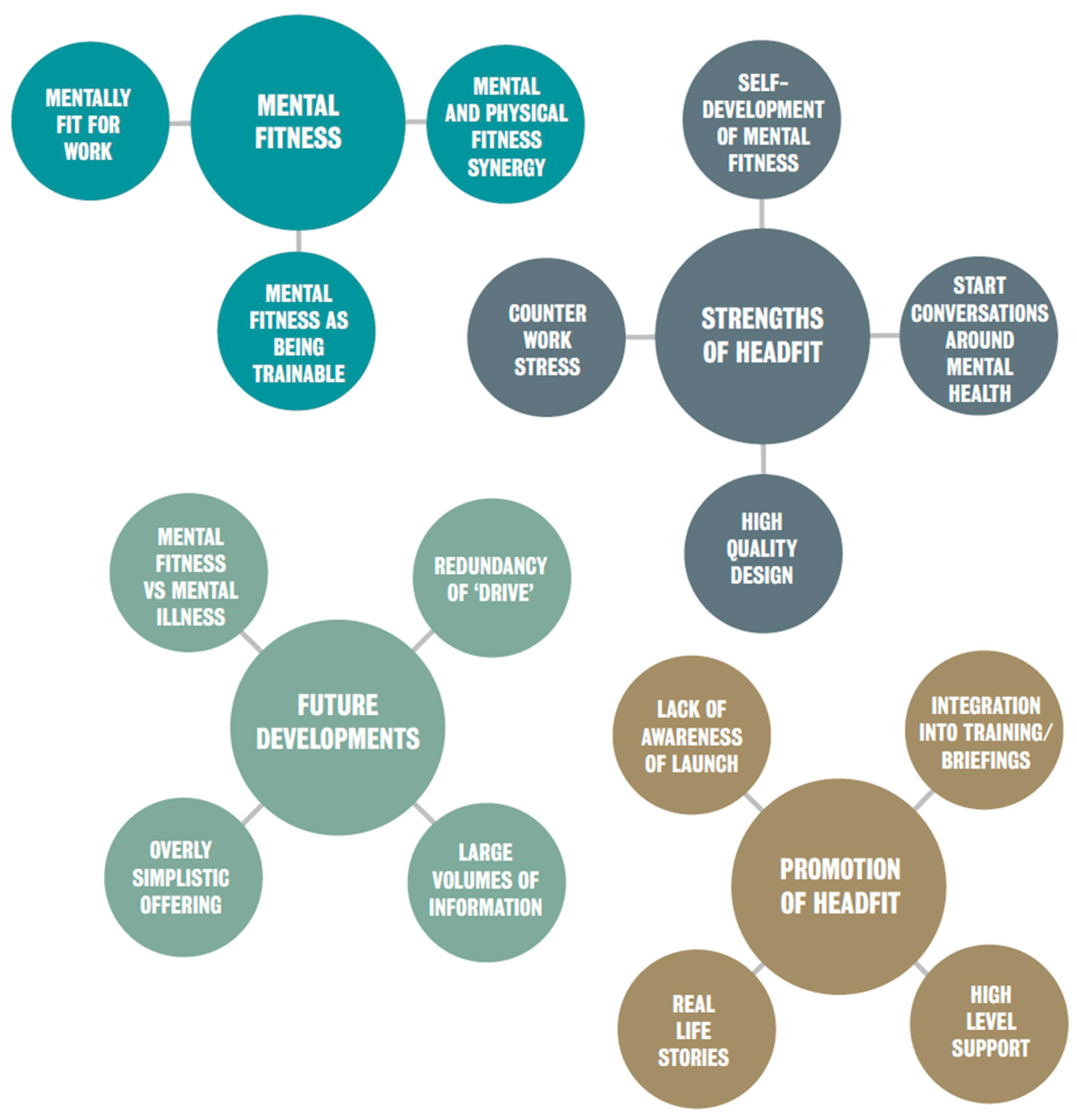
- (a)
- Mental fitness
- (b)
- Strengths of HeadFIT
- (c)
- Future developments
- (d)
- Promotion of HeadFIT
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reid, G. Adjustment Disorder: An Occupational Perspective (with Particular Focus on the Military). In Adjustment Disorders: From Controversy to Clinical Practice; Casey, P., Ed.; Oxford University Press: Oxford, UK, 2018; pp. 173–188. [Google Scholar]
- Campbell, D.; Noble, O.B.Y. Occupational stressors in military service: A review and framework. Mil. Psychol. 2009, 21, S47–S67. [Google Scholar] [CrossRef]
- Stevelink, S.A.M.; Jones, M.; Hull, L.; Pernet, D.; MacCrimmon, S.; Goodwin, L.; Macmanus, D.; Murphy, D.; Jones, N.; Greenberg, N.; et al. Mental health outcomes at the end of the British involvement in the Iraq and Afghanistan conflicts: A cohort study. Br. J. Psychiatry 2018, 213, 690–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, N.; Langston, V.; Jones, N. Trauma risk management (TRiM) in the UK Armed Forces. BMJ Mil. Health 2008, 154, 124–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Army. Mental Resilience. Available online: https://www.army.mod.uk/people/join-well/mental-resilience/ (accessed on 25 May 2021).
- Jones, N.; Whelan, C.; Harden, I.; Macfarlane, A.; Burdett, H.; Greenberg, N. Resilience-based intervention for UK military recruits: A randomised controlled trial. Occup. Environ. Med. 2019, 76, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Royal Navy. Project Regain | Royal Navy. Available online: https://www.royalnavy.mod.uk/news-and-latest-activity/features/project-regain (accessed on 24 May 2021).
- Williamson, V.; Greenberg, N.; Stevelink, S.A.M. Perceived stigma and barriers to care in UK Armed Forces personnel and veterans with and without probable mental disorders. BMC Psychol. 2019, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Greenberger, D.; Padesky, C.A. Mind over Mood: A Cognitive Therapy Treatment Manual for Clients; Guilford Press: New York, NY, USA, 1995. [Google Scholar]
- Gilbert, P. The Compassionate Mind—A New Approach to Life’s Challenges; Constable & Robinson, Ltd.: London, UK, 2009. [Google Scholar]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and Evaluating Complex. Interventions: Following Considerable Development in the Field Since 2006, MRC and NIHR Have Jointly Commissioned an Update of This Guidance to be Published in 2019, 2006; Medical Research Council: London, UK, 2008. [Google Scholar]
- Ritchie, J.; Lewis, J. Qualitative Research Practice: A Guide for Social Science Students and Researchers; Sage: London, UK, 2003. [Google Scholar]
- Ministry of Defence. UK Armed Forces Biannual Diversity Statistics Report. Available online: https://www.gov.uk/government/publications/uk-armed-forces-biannual-diversity-statistics-2020/uk-armed-forces-biannual-diversity-statistics-1-april-2020 (accessed on 13 May 2021).
- Dempsey, N. UK Defence Personnel Statistics, 2020. Houses of Common Library, UK Parliament. Available online: https://commonslibrary.parliament.uk/research-briefings/cbp-7930/ (accessed on 13 May 2021).
- Harden, L.; Jones, N.; Whelan, C.; Phillips, A.; Simms, A.; Greenberg, N. A systematic review of psychological training or interventions given to UK military personnel prior to deployment. BMJ Mil. Health 2021, 167, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.A.; Adler, A.B. Military mental health training: Building resilience. In Resilience and Mental Health: Challenges across the Lifespan; Southwick, S.M., Litz, L.B., Charney, D., Friedman, M.J., Eds.; Cambridge University Press: Cambridge, UK, 2011; pp. 323–339. [Google Scholar]
- Robinson, P.; Oades, L.; Caputi, P. Conceptualising and measuring mental fitness: A Delphi study. Int. J. Wellbeing 2015, 5, 53–73. [Google Scholar] [CrossRef]
- McGinty, E.; Pescosolido, B.; Kennedy-Hendricks, A.; Barry, C.L. Communication Strategies to Counter Stigma and Improve Mental Illness and Substance Use Disorder Policy. Psychiatr. Serv. 2018, 69, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Quirk, H.; Crank, H.; Carter, A.; Leahy, H.; Copeland, R.J. Barriers and facilitators to implementing workplace health and wellbeing services in the NHS from the perspective of senior leaders and wellbeing practitioners: A qualitative study. BMC Public Health 2018, 18, 1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodall, J.; White, J.; South, J. Improving health and well-being through community health champions: A thematic evaluation of a programme in Yorkshire and Humber. Perspect. Public Health 2013, 132, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, F.; Orji, R. Insights from user reviews to improve mental health apps. Health Inform. J. 2020, 26, 2042–2066. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | S1 | S3 |
|---|---|---|
| n (%) | n (%) | |
| Total Number of Beneficiaries | 145 | 209 |
| Age | ||
| <24 | 21 (15%) | 47 (23%) |
| 25–34 | 48 (33%) | 69 (34%) |
| 35–44 | 40 (28%) | 49 (24%) |
| 45–54 | 23 (16%) | 27 (13%) |
| 55+ | 12 (8%) | 13 (6%) |
| Mean (SD) a | 36 (10.9) | 34 (10.8) |
| Gender | ||
| Male | 111 (77%) | 160 (78%) |
| Female | 34 (23%) | 45 (22%) |
| Service Branch | ||
| Royal Navy | 15 (10%) | 17 (8%) |
| Army | 62 (43%) | 116 (57%) |
| Royal Air Force | 36 (25%) | 38 (18%) |
| Civil Service | 31 (22%) | 34 (17%) |
| Military Service Rank | ||
| Senior Commissioned Officer | 9 (8%) | 9 (5%) |
| Junior Commissioned Officer | 22 (19%) | 28 (17%) |
| Senior Non-Commissioned Officer | 31 (27%) | 39 (23%) |
| Junior Non-Commissioned Officer | 26 (23%) | 40 (23%) |
| Other Ranks | 24 (23%) | 55 (32%) |
| Military Role | ||
| Combat and Combat Support Role | 22 (21%) | 26 (15%) |
| Combat Support Role | 84 (79%) | 140 (85%) |
| Definitions of Mental Fitness | BV (%) | Follow Up (%) |
|---|---|---|
| Wellbeing and mental health | ☒(34%) | ☒(35%) |
| Resilience | ☒(15%) | ☒(17%) |
| Positive mental state | ☒(15%) | ☒(7%) |
| Stress management | ☒(9%) | ☒(5%) |
| Coping | ☒(6%) | ☒(1%) |
| Strength | ☒(6%) | ☒(9%) |
| Robust mental state | ☐(-) | ☒(5%) |
| Thought processes impacting behaviour | ☐(-) | ☒(4%) |
| Other | ☒(10%) | ☒(17%) |
| Feedback Statements | Agree | Disagree |
|---|---|---|
| n (%) | n (%) | |
| I think the HeadFIT tools could be useful to me | 391 (87%) | 60 (13%) |
| I know where to find the HeadFIT tools | 376 (84%) | 51(16%) |
| I know which HeadFIT tools are available to me | 306 (69%) | 136 (31%) |
| The video has increased my understanding of what mental fitness means | 350 (79%) | 96 (21%) |
| I now know more about how to manage my mental fitness | 332 (74%) | 112 (26%) |
| The video was the right length | 434 (96%) | 18 (4%) |
| The video was relevant to me | 372 (83%) | 79 (17%) |
| The video used good examples | 368 (83%) | 75 (17%) |
| The video provided me with important information | 378 (84%) | 71 (16%) |
| Feedback Statements | Agree | Disagree |
|---|---|---|
| n (%) | n (%) | |
| I found the HeadFIT website too complicated | 8 (10%) | 68 (90%) |
| I thought the HeadFIT website was easy to understand | 71 (94%) | 5 (6%) |
| I found the tools in the HeadFIT website were put together well | 59 (93%) | 5 (7%) |
| I found the HeadFIT website difficult/awkward to use | 8 (11%) | 67 (89%) |
| I had to take some time to learn how to use the HeadFIT website before I could use it properly | 23 (32%) | 50 (68%) |
| The HeadFIT website content was relevant to my work | 64 (86%) | 10 (14%) |
| The HeadFIT website content was relevant to my personal life | 66 (91%) | 7 (9%) |
| I found the HeadFIT website kept my attention | 59 (79%) | 16 (21%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McKenzie, A.; Croak, B.; Rafferty, L.; Greenberg, N.; Stevelink, S.A.M. A Service Evaluation of the Military HeadFIT Initiative: An Implementation Study. Int. J. Environ. Res. Public Health 2021, 18, 7375. https://doi.org/10.3390/ijerph18147375
McKenzie A, Croak B, Rafferty L, Greenberg N, Stevelink SAM. A Service Evaluation of the Military HeadFIT Initiative: An Implementation Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7375. https://doi.org/10.3390/ijerph18147375
Chicago/Turabian StyleMcKenzie, Amber, Bethany Croak, Laura Rafferty, Neil Greenberg, and Sharon A. M. Stevelink. 2021. "A Service Evaluation of the Military HeadFIT Initiative: An Implementation Study" International Journal of Environmental Research and Public Health 18, no. 14: 7375. https://doi.org/10.3390/ijerph18147375
APA StyleMcKenzie, A., Croak, B., Rafferty, L., Greenberg, N., & Stevelink, S. A. M. (2021). A Service Evaluation of the Military HeadFIT Initiative: An Implementation Study. International Journal of Environmental Research and Public Health, 18(14), 7375. https://doi.org/10.3390/ijerph18147375