
Lifestyle Habits among Pregnant Women in Denmark during the First COVID-19 Lockdown Compared with a Historical Period—A Hospital-Based Cross-Sectional Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Outcomes
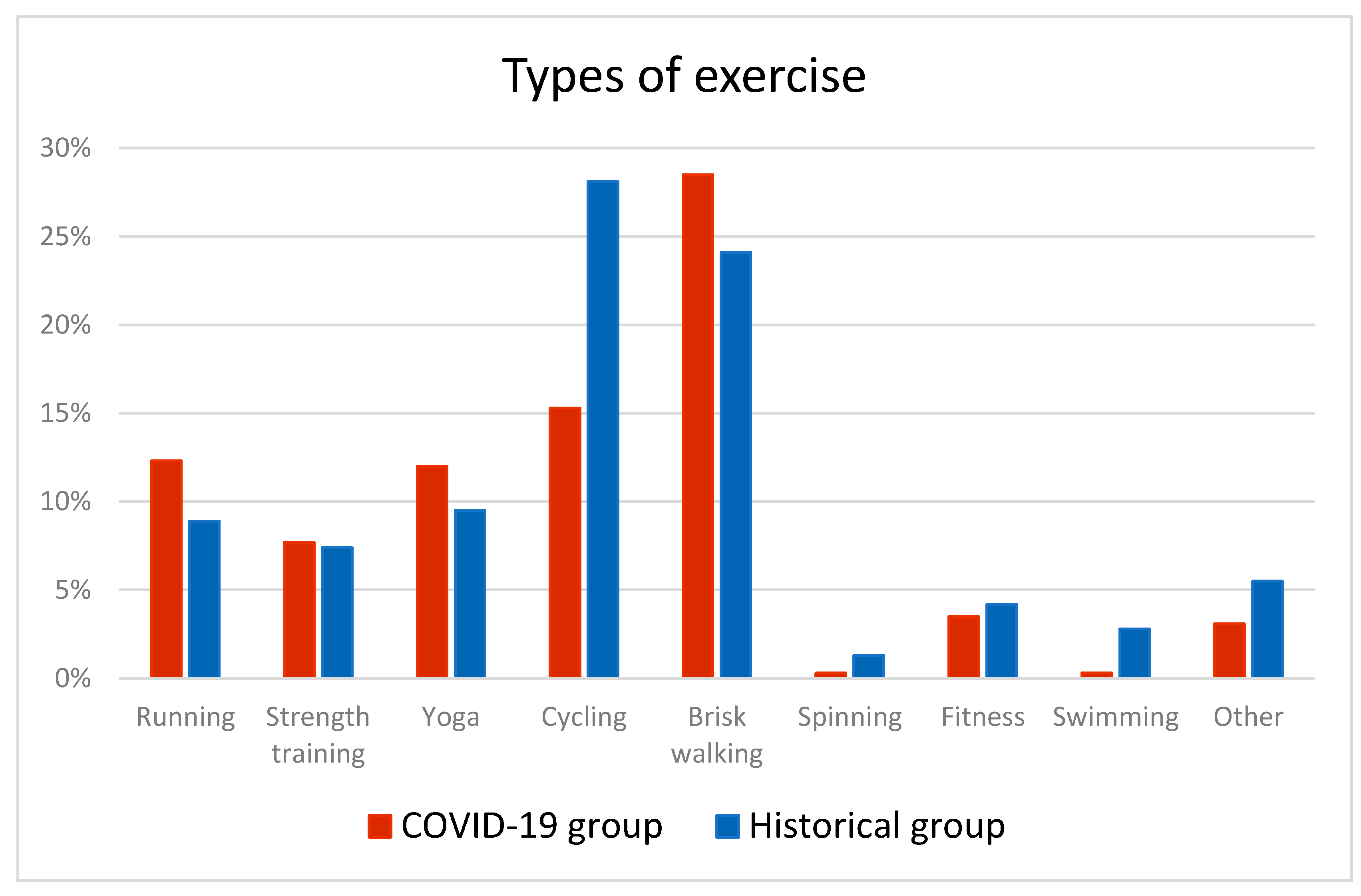
2.1.1. Exercise
2.1.2. Alcohol Consumption
2.1.3. Smoking
2.2. Covariates
2.3. Ethical Approval
2.4. Statistical Analyses
3. Results
3.1. Exercise
3.2. Alcohol Consumption
3.3. Smoking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virtual Press Conference on COVID-19 11 March 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-press-conference-full-and-final-11mar2020.pdf?sfvrsn=cb432bb3_2 (accessed on 21 May 2021).
- Prime Minister Mette Frederiksen’s Introduction at a Press Conference in the Prime Minister’s Office on the Coronavirus on 11 March 2020 (Statsminister Mette Frederiksens Indledning På Pressemøde i Statsministeriet Om Corona-Virus Den 11. Marts 2020). Available online: https://www.regeringen.dk/nyheder/2020/statsminister-mette-frederiksens-indledning-paa-pressemoede-i-statsministeriet-om-corona-virus-den-11-marts-2020/ (accessed on 21 May 2021).
- Wood, W.; Tam, L.; Witt, M.G. Changing Circumstances, Disrupting Habits. J. Personal. Soc. Psychol. 2005, 88, 918–933. [Google Scholar] [CrossRef] [PubMed]
- Turna, J.; Zhang, J.; Lamberti, N.; Patterson, B.; Simpson, W.; Francisco, A.P.; Bergmann, C.G.; Ameringen, M.V. Anxiety, Depression and Stress during the COVID-19 Pandemic: Results from a Cross-Sectional Survey. J. Psychiatr. Res. 2021, 137, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Jose, B.S. Stressors and alcohol consumption. Alcohol Alcohol. 2000, 35, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Fidler, J.A.; West, R. Self-Perceived Smoking Motives and Their Correlates in a General Population Sample. Nicotine Tob. Res. 2009, 11, 1182–1188. [Google Scholar] [CrossRef]
- Lawson, P.J.; Flocke, S.A. Teachable Moments for Health Behavior Change: A Concept Analysis. Patient Educ. Couns. 2009, 76, 25–30. [Google Scholar] [CrossRef]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef]
- New Exercise Habits Forming during Coronavirus Crisis. Available online: https://www.sportengland.org/news/new-exercise-habits-forming-during-coronavirus-crisis (accessed on 25 February 2021).
- Bommele, J.; Hopman, P.; Walters, B.H.; Geboers, C.; Croes, E.; Fong, G.T.; Quah, A.C.K.; Willemsen, M. The Double-Edged Relationship between COVID-19 Stress and Smoking: Implications for Smoking Cessation. Tob. Induc. Dis. 2020, 18, 63. [Google Scholar] [CrossRef] [PubMed]
- Bourdas, D.I.; Zacharakis, E.D. Impact of COVID-19 Lockdown on Physical Activity in a Sample of Greek Adults. Sports 2020, 8, 139. [Google Scholar] [CrossRef]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between Changes in Self-Reported Physical Activity, Sedentary Behaviour and Health during the Coronavirus (COVID-19) Pandemic in France and Switzerland. J. Sports Sci. 2020, 39, 699–704. [Google Scholar] [CrossRef]
- Alpers, S.E.; Skogen, J.C.; Mæland, S.; Pallesen, S.; Rabben, Å.K.; Lunde, L.-H.; Fadnes, L.T. Alcohol Consumption during a Pandemic Lockdown Period and Change in Alcohol Consumption Related to Worries and Pandemic Measures. Int. J. Environ. Res. Public Health 2021, 18, 1220. [Google Scholar] [CrossRef]
- Koopmann, A.; Georgiadou, E.; Kiefer, F.; Hillemacher, T. Did the General Population in Germany Drink More Alcohol during the COVID-19 Pandemic Lockdown? Alcohol Alcohol. 2020, 55, 698–699. [Google Scholar] [CrossRef] [PubMed]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-Reported Alcohol, Tobacco, and Cannabis Use during COVID-19 Lockdown Measures: Results from a Web-Based Survey. Eur. Addict. Res. 2020, 26, 309–315. [Google Scholar] [CrossRef]
- Jacob, L.; Smith, L.; Armstrong, N.C.; Yakkundi, A.; Barnett, Y.; Butler, L.; McDermott, D.T.; Koyanagi, A.; Shin, J.I.; Meyer, J.; et al. Alcohol Use and Mental Health during COVID-19 Lockdown: A Cross-Sectional Study in a Sample of UK Adults. Drug Alcohol Depend. 2021, 219, 108488. [Google Scholar] [CrossRef]
- Elling, J.; Crutzen, R.; Talhout, R.; De Vries, H. Tobacco Smoking and Smoking Cessation in Times of COVID-19. Tob. Prev. Cessat. 2020, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Guignard, R.; Andler, R.; Quatremère, G.; Pasquereau, A.; du Roscoät, E.; Arwidson, P.; Berlin, I.; Nguyen-Thanh, V. Changes in Smoking and Alcohol Consumption during COVID-19-Related Lockdown: A Cross-Sectional Study in France. Eur. J. Public Health 2021. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Jackson, S.E.; Garnett, C.; Shahab, L.; Oldham, M.; Brown, J. Association of the COVID-19 Lockdown with Smoking, Drinking and Attempts to Quit in England: An Analysis of 2019–20 Data. Addiction 2020, 116, 1233–1244. [Google Scholar] [CrossRef]
- Mottola, M.F.; Davenport, M.H.; Ruchat, S.-M.; Davies, G.A.; Poitras, V.J.; Gray, C.E.; Garcia, A.J.; Barrowman, N.; Adamo, K.B.; Duggan, M.; et al. 2019 Canadian Guideline for Physical Activity throughout Pregnancy. Br. J. Sports Med. 2018, 52, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Syed, H.; Slayman, T.; DuChene Thoma, K. ACOG Committee Opinion No. 804: Physical Activity and Exercise during Pregnancy and the Postpartum Period. Obs. Gynecol. 2021, 137, 375–376. [Google Scholar] [CrossRef]
- Mund, M.; Louwen, F.; Klingelhoefer, D.; Gerber, A. Smoking and Pregnancy—A Review on the First Major Environmental Risk Factor of the Unborn. Int. J. Environ. Res. Public Health 2013, 10, 6485–6499. [Google Scholar] [CrossRef]
- Ion, R.; Bernal, A.L. Smoking and Preterm Birth. Reprod. Sci. 2015, 22, 918–926. [Google Scholar] [CrossRef]
- Broccia, M.; Vikre-Jørgensen, J.; Rausgaard, N.L.K. A Danish fetal alcohol spectrum disorders definition. Ugeskr Laeger 2017, 179, 32. [Google Scholar]
- Bjørnholt, S.M.; Leite, M.; Albieri, V.; Kjaer, S.K.; Jensen, A. Maternal Smoking during Pregnancy and Risk of Stillbirth: Results from a Nationwide Danish Register-Based Cohort Study. Acta Obs. Gynecol. Scand. 2016, 95, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.; Gray, R.; Brocklehurst, P. Systematic Review of Effects of Low-Moderate Prenatal Alcohol Exposure on Pregnancy Outcome. BJOG Int. J. Obstet. Gynaecol. 2007, 114, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Henderson, J.; Kesmodel, U.; Gray, R. Systematic Review of the Fetal Effects of Prenatal Binge-Drinking. J. Epidemiol. Community Health 2007, 61, 1069–1073. [Google Scholar] [CrossRef]
- Recommendations for Pregnancy Care (Anbefalinger for Svangreomsorgen 2013). 2013. Available online: https://www.sst.dk/da/udgivelser/2015/anbefalinger-for-svangreomsorgen (accessed on 21 May 2021).
- WHO Recommendations for the Prevention and Management of Tobacco Use and Second-Hand Smoke Exposure in Pregnancy. Available online: https://www.who.int/tobacco/publications/pregnancy/guidelinestobaccosmokeexposure/en/ (accessed on 26 February 2021).
- Physical Activity-Handbook on Prevention and Treatment 2018 (Fysisk Aktivitet-Håndbog Om Forebyggelse Og Behandling 2018). Available online: https://www.sst.dk/da/udgivelser/2018/fysisk-aktivitet---haandbog-om-forebyggelse-og-behandling (accessed on 21 May 2021).
- Davenport, M.H.; Meyer, S.; Meah, V.L.; Strynadka, M.C.; Khurana, R. Moms Are Not OK: COVID-19 and Maternal Mental Health. Front. Glob. Womens Health 2020, 1, 1. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Psychological Responses and Lifestyle Changes among Pregnant Women with Respect to the Early Stages of COVID-19 Pandemic. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Biviá-Roig, G.; La Rosa, V.L.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J.F. Analysis of the Impact of the Confinement Resulting from COVID-19 on the Lifestyle and Psychological Wellbeing of Spanish Pregnant Women: An Internet-Based Cross-Sectional Survey. Int. J. Env. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef]
- Dansk Føtalmedicinsk Database—Sundhed.Dk. Available online: https://www.sundhed.dk/sundhedsfaglig/kvalitet/kliniske-kvalitetsdatabaser/screening/foetalmedicin/ (accessed on 2 July 2021).
- Høgh, S.; Wolf, H.T.; von Euler-Chelpin, M.; Huusom, L.; Pinborg, A.; Tabor, A.; Hegaard, H.K. Multivitamin Use and Risk of Preeclampsia in a High-Income Population: A Cohort Study. Sex. Reprod. Healthc. 2020, 24, 100500. [Google Scholar] [CrossRef]
- McNutt, L.-A.; Wu, C.; Xue, X.; Hafner, J.P. Estimating the Relative Risk in Cohort Studies and Clinical Trials of Common Outcomes. Am. J. Epidemiol. 2003, 157, 940–943. [Google Scholar] [CrossRef] [PubMed]
- Broberg, L.; Ersbøll, A.S.; Backhausen, M.G.; Damm, P.; Tabor, A.; Hegaard, H.K. Compliance with National Recommendations for Exercise during Early Pregnancy in a Danish Cohort. BMC Pregnancy Childbirth 2015, 15, 317. [Google Scholar] [CrossRef] [PubMed]
- Juhl, M.; Madsen, M.; Andersen, A.-M.N.; Andersen, P.K.; Olsen, J. Distribution and Predictors of Exercise Habits among Pregnant Women in the Danish National Birth Cohort: Exercise during Pregnancy. Scand. J. Med. Sci. Sports 2012, 22, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Strandberg-larsen, K.; Rod, N.N.; Nybo, A.A.; Olsen, J.; Grønbæk, M. Characteristics of Women Who Binge Drink before and after They Become Aware of Their Pregnancy. Eur. J. Epidemiol. 2008, 23, 565–572. [Google Scholar] [CrossRef]
- Iversen, M.L.; Sørensen, N.O.; Broberg, L.; Damm, P.; Hedegaard, M.; Tabor, A.; Hegaard, H.K. Alcohol Consumption and Binge Drinking in Early Pregnancy. A Cross-Sectional Study with Data from the Copenhagen Pregnancy Cohort. BMC Pregnancy Childbirth 2015, 15, 327. [Google Scholar] [CrossRef]
- de Wolff, M.G.; Backhausen, M.G.; Iversen, M.L.; Bendix, J.M.; Rom, A.L.; Hegaard, H.K. Prevalence and Predictors of Maternal Smoking Prior to and during Pregnancy in a Regional Danish Population: A Cross-Sectional Study. Reprod. Health 2019, 16, 82. [Google Scholar] [CrossRef] [PubMed]
- Ekblad, M.; Gissler, M.; Korkeila, J.; Lehtonen, L. Trends and Risk Groups for Smoking during Pregnancy in Finland and Other Nordic Countries. Eur. J. Public Health 2014, 24, 544–551. [Google Scholar] [CrossRef]
- McCormick, M.C.; Brooks-Gunn, J.; Shorter, T.; Holmes, J.H.; Wallace, C.Y.; Heagarty, M.C. Factors Associated with Smoking in Low-Income Pregnant Women: Relationship to Birth Weight, Stressful Life Events, Social Support, Health Behaviors and Mental Distress. J. Clin. Epidemiol. 1990, 43, 441–448. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Gaston, A.; Cramp, A. Exercise during Pregnancy: A Review of Patterns and Determinants. J. Sci. Med. Sport 2011, 14, 299–305. [Google Scholar] [CrossRef]
- Constant, A.; Conserve, D.F.; Gallopel-Morvan, K.; Raude, J. Socio-Cognitive Factors Associated With Lifestyle Changes in Response to the COVID-19 Epidemic in the General Population: Results from a Cross-Sectional Study in France. Front. Psychol. 2020, 11, 579460. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Baescu, O.; Christiansen, H. The Danish National Travel Survey Annual Statistical Report TU0619v2. Available online: https://orbit.dtu.dk/en/publications/the-danish-national-travel-survey-annual-statistical-report-tu061 (accessed on 2 July 2021).
- Gaston, A.; Vamos, C.A. Leisure-Time Physical Activity Patterns and Correlates among Pregnant Women in Ontario, Canada. Matern. Child. Health J. 2013, 17, 477–484. [Google Scholar] [CrossRef]
- Gjestland, K.; Bø, K.; Owe, K.M.; Eberhard-Gran, M. Do Pregnant Women Follow Exercise Guidelines? Prevalence Data among 3482 Women, and Prediction of Low-Back Pain, Pelvic Girdle Pain and Depression. Br. J. Sports Med. 2013, 47, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Jukic, A.M.Z.; Evenson, K.R.; Herring, A.H.; Wilcox, A.J.; Hartmann, K.E.; Daniels, J.L. Correlates of Physical Activity at Two Time Points during Pregnancy. J. Phys. Act. Health 2012, 9, 325–335. [Google Scholar] [CrossRef]
- Davenport, M.H.; Meah, V.L.; Ruchat, S.-M.; Davies, G.A.; Skow, R.J.; Barrowman, N.; Adamo, K.B.; Poitras, V.J.; Gray, C.E.; Jaramillo Garcia, A.; et al. Impact of Prenatal Exercise on Neonatal and Childhood Outcomes: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2018, 52, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Hessami, K.; Romanelli, C.; Chiurazzi, M.; Cozzolino, M. COVID-19 Pandemic and Maternal Mental Health: A Systematic Review and Meta-Analysis. J. Matern. Fetal Neonatal Med. 2020. [Google Scholar] [CrossRef]
- Ahlers-Schmidt, C.R.; Hervey, A.M.; Neil, T.; Kuhlmann, S.; Kuhlmann, Z. Concerns of Women Regarding Pregnancy and Childbirth during the COVID-19 Pandemic. Patient Educ. Couns. 2020, 103, 2578–2582. [Google Scholar] [CrossRef]
- Backhausen, M.G.; Ekstrand, M.; Tydén, T.; Magnussen, B.K.; Shawe, J.; Stern, J.; Hegaard, H.K. Pregnancy Planning and Lifestyle Prior to Conception and during Early Pregnancy among Danish Women. Eur. J. Contracept. Reprod. Health Care 2014, 19, 57–65. [Google Scholar] [CrossRef]
- Oei, J.L. Alcohol Use in Pregnancy and Its Impact on the Mother and Child. Addiction 2020, 115, 2148–2163. [Google Scholar] [CrossRef] [PubMed]
- Torres, O.V.; O’Dell, L.E. Stress Is a Principal Factor That Promotes Tobacco Use in Females. Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 65, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Bliddal, M.; Liew, Z.; Pottegård, A.; Kirkegaard, H.; Olsen, J.; Nohr, E.A. Examining Nonparticipation in the Maternal Follow-up Within the Danish National Birth Cohort. Am. J. Epidemiol. 2018, 187, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Lagerros, Y.T.; Lagiou, P. Assessment of Physical Activity and Energy Expenditure in Epidemiological Research of Chronic Diseases. Eur. J. Epidemiol. 2007, 22, 353–362. [Google Scholar] [CrossRef]
- Sanda, B.; Vistad, I.; Haakstad, L.A.H.; Berntsen, S.; Sagedal, L.R.; Lohne-Seiler, H.; Torstveit, M.K. Reliability and Concurrent Validity of the International Physical Activity Questionnaire Short Form among Pregnant Women. BMC Sports Sci. Med. Rehabil. 2017, 9. [Google Scholar] [CrossRef]
- Taylor, H.L.; Jacobs, D.R.; Schucker, B.; Knudsen, J.; Leon, A.S.; Debacker, G. A Questionnaire for the Assessment of Leisure Time Physical Activities. J. Chronic Dis. 1978, 31, 741–755. [Google Scholar] [CrossRef]
- Kesmodel, U.; Olsen, S.F. Self Reported Alcohol Intake in Pregnancy: Comparison between Four Methods. J. Epidemiol. Community Health 2001, 55, 738–745. [Google Scholar] [CrossRef]
- Kesmodel, U. Binge Drinking during Pregnancy--Is It Possible to Obtain Valid Information on a Weekly Basis? Am. J. Epidemiol. 2004, 159, 803–808. [Google Scholar] [CrossRef]
- Strandberg-Larsen, K.; Andersen, A.-M.; Olsen, J.; Nielsen, N.R.; Grønbæk, M. Do Women Give the Same Information on Binge Drinking during Pregnancy When Asked Repeatedly? Eur. J. Clin. Nutr. 2006, 60, 1294–1298. [Google Scholar] [CrossRef][Green Version]
- Mattsson, K.; Källén, K.; Rignell-Hydbom, A.; Lindh, C.H.; Jönsson, B.A.G.; Gustafsson, P.; Olofsson, P.; Ivarsson, S.A.; Rylander, L. Cotinine Validation of Self-Reported Smoking During Pregnancy in the Swedish Medical Birth Register. Nicotine Tob. Res. 2016, 18, 5. [Google Scholar] [CrossRef]
- Grundy, E.J.; Suddek, T.; Filippidis, F.T.; Majeed, A.; Coronini-Cronberg, S. Smoking, SARS-CoV-2 and COVID-19: A Review of Reviews Considering Implications for Public Health Policy and Practice. Tob. Induc. Dis. 2020, 18, 58. [Google Scholar] [CrossRef]
- Terada, M.; Ohtsu, H.; Saito, S.; Hayakawa, K.; Tsuzuki, S.; Asai, Y.; Matsunaga, N.; Kutsuna, S.; Sugiura, W.; Ohmagari, N. Risk Factors for Severity on Admission and the Disease Progression during Hospitalisation in a Large Cohort of Patients with COVID-19 in Japan. BMJ Open 2021, 11, e047007. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, L.; De Vivo, M.; Hayes, L.; Hesketh, K.R.; Mills, H.; Newham, J.J.; Olander, E.K.; Smith, D.M. Encouraging Physical Activity during and after Pregnancy in the COVID-19 Era, and Beyond. Int. J. Environ. Res. Public Health 2020, 17, 7304. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| COVID-19 Group | Historical Group | p-Value | |
|---|---|---|---|
| n (%) | n (%) | ||
| Total (N = 1472) | 685 (47) | 787 (53) | |
| Characteristics | |||
| Age (years) | 0.0633 | ||
| 18–24 | 27 (4) | 20 (3) | |
| 25–29 | 189 (28) | 257 (33) | |
| 30–34 | 307 (45) | 317 (40) | |
| ≥35 | 161 (24) | 193 (25) | |
| Missing | 1 (0) | 0 | |
| Mean (±SD) | 31.5 (±4.2) | 31.6 (±4.4) | 0.7092 |
| Parity | 0.5460 | ||
| Nullipara | 452 (66) | 531 (67) | |
| Multipara | 233 (34) | 256 (33) | |
| Highest obtained educational level | 0.6330 | ||
| Higher degree | 413 (60) | 472 (60) | |
| Intermediate degree (3–4 years) | 39 (6) | 43 (5) | |
| Short degree (1–2 years) | 14 (2) | 22 (3) | |
| Technical degree | 186 (27) | 195 (25) | |
| Compulsory education | 29 (4) | 42 (5) | |
| Missing | 4 (1) | 13 (2) | |
| Body Mass Index (BMI)(kg/m2) | 0.5782 | ||
| Underweight (<18.5) | 24 (4) | 38 (5) | |
| Normal (18.5–24.9) | 511 (75) | 578 (73) | |
| Overweight (25–29.9) | 95 (14) | 105 (13) | |
| Obese (≥30) | 36 (5) | 36 (5) | |
| Missing | 19 (3) | 30 (4) | |
| Mean (±SD) | 22.8 (±3.9) | 22.8 (±3.8) | 0.7300 |
| Danish language skills | 0.8691 | ||
| Yes | 638 (93) | 737 (94) | |
| Missing | 11 (2) | 10 (1) | |
| Previous miscarriage | 0.3213 | ||
| Yes | 196 (29) | 207 (26) | |
| Assisted reproductive technology (ART) | 0.1634 | ||
| Yes | 90 (13) | 123 (16) | |
| Missing | 1 (0) | 5 (1) | |
| Chronic disorder | 0.3377 | ||
| Yes | 191 (28) | 202 (26) | |
| Previous contact with a psychiatrist and/or self-reported psychiatric condition | |||
| Yes | 72 (11) | 55 (7) | 0.0164 |
| Cohabitation | 0.0659 | ||
| Yes | 640 (93) | 713 (91) | |
| Occupation | 0.1775 | ||
| Employed | 508 (74) | 615 (78) | |
| Unemployed | 47 (7) | 39 (5) | |
| Student | 85 (12) | 86 (11) | |
| Other | 47 (7) | 39 (5) | |
| Missing | 3 (0) | 8 (1) | |
| Pregnancy planning | 0.9217 | ||
| Very planned | 335 (49) | 371 (47) | |
| Fairly planned | 177 (26) | 208 (26) | |
| Neither planned nor unplanned | 117 (17) | 140 (18) | |
| Fairly unplanned | 25 (4) | 34 (4) | |
| Very unplanned | 24 (4) | 25 (3) | |
| Missing | 7 (1) | 9 (1) | |
| Smoking status during pregnancy | 0.8680 | ||
| Smokers | 5 (1) | 6 (1) | |
| Non-smokers | 613 (89) | 698 (89) | |
| Quitters | 64 (9) | 80 (10) | |
| Missing | 3 (0) | 3 (0) | |
| Group | N | Prevalence of Outcome (%) n | Crude | Adjusted | |||||
|---|---|---|---|---|---|---|---|---|---|
| PR | (95% CI) | Model 1 | Model 2 | ||||||
| PR | (95% CI) | PR | (95% CI) | ||||||
| Any Exercise * | COVID-19 | 681 | 59 (406) | 0.95 | (0.87 to 1.03) | 0.93 | (0.86 to 1.01) | 0.91 | (0.84 to 0.99) |
| Historical | 783 | 63 (492) | 1.00 | - | 1.00 | - | 1.00 | - | |
| Adherence to recommended level of exercise (≥3.5 h/week) | COVID-19 | 685 | 43 (294) | 0.90 | (0.80 to 1.01) | 0.89 | (0.80 to 0.99) | 0.89 | (0.80 to 0.99) |
| Historical | 787 | 48 (376) | 1.00 | - | 1.00 | - | 1.00 | - | |
| Binge drinking ** | COVID-19 | 641 | 23 (161) | 0.76 | (0.64 to 0.89) | 0.79 | (0.67 to 0.93) | 0.80 | (0.68 to 0.93) |
| Historical | 719 | 30 (239) | 1.00 | - | 1.00 | - | - | ||
| Smoking cessation | COVID-19 | 69 | 9 (64) | 1.00 | (0.91 to 1.09) | - | - | - | - |
| Historical | 86 | 10 (80) | 1.00 | - | - | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hegaard, H.K.; Rom, A.L.; Christensen, K.B.; Broberg, L.; Høgh, S.; Christiansen, C.H.; Nathan, N.O.; de Wolff, M.G.; Damm, P. Lifestyle Habits among Pregnant Women in Denmark during the First COVID-19 Lockdown Compared with a Historical Period—A Hospital-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7128. https://doi.org/10.3390/ijerph18137128
Hegaard HK, Rom AL, Christensen KB, Broberg L, Høgh S, Christiansen CH, Nathan NO, de Wolff MG, Damm P. Lifestyle Habits among Pregnant Women in Denmark during the First COVID-19 Lockdown Compared with a Historical Period—A Hospital-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(13):7128. https://doi.org/10.3390/ijerph18137128
Chicago/Turabian StyleHegaard, Hanne Kristine, Ane Lilleøre Rom, Karl Bang Christensen, Lotte Broberg, Stinne Høgh, Cecilie Holm Christiansen, Nina Olsen Nathan, Mie Gaarskjaer de Wolff, and Peter Damm. 2021. "Lifestyle Habits among Pregnant Women in Denmark during the First COVID-19 Lockdown Compared with a Historical Period—A Hospital-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 13: 7128. https://doi.org/10.3390/ijerph18137128
APA StyleHegaard, H. K., Rom, A. L., Christensen, K. B., Broberg, L., Høgh, S., Christiansen, C. H., Nathan, N. O., de Wolff, M. G., & Damm, P. (2021). Lifestyle Habits among Pregnant Women in Denmark during the First COVID-19 Lockdown Compared with a Historical Period—A Hospital-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(13), 7128. https://doi.org/10.3390/ijerph18137128