Abstract
Acute pain intensity related to cesarean section (CS) may be extensive and is often underestimated. This may influence mothers’ quality of life and their children’s development. Regional analgesia techniques that include transversus abdominis plane block (TAPB) and quadratus lumborum block (QLB) have proven their efficacy in the postoperative period after CS. Although several randomized controlled studies and one meta-analysis have investigated the utility of TAPB and QLB in the reduction of acute and chronic pain after CS, only one study directly compared both types of regional blocks and revealed superiority of QLB over TAPB. Our study aimed to reevaluate the effectiveness of transversus TAPB and QLB in controlling acute postoperative pain after CS. We recruited 197 women with singleton pregnancies undergoing CS under spinal anesthesia. The patients were randomized to receive either TAPB or QLB after CS. The acute postoperative pain was evaluated using the visual analog scale (VAS) at 2, 4, 8, 12 and 24 h after the operation. No significant difference in acute postoperative pain intensity between the groups was found. The patients who received TAPB had a higher demand for supplemental morphine injections (p < 0.039). In our study, none of the evaluated regional blocks demonstrated an advantage over the other regarding acute postoperative pain management.
1. Introduction
The number of the cesarean deliveries has almost doubled between 2000 and 2015 [1]. The highest rise of cesarean sections (CSs) in recent years was observed in Eastern Europe and South and Central Asia. In Poland, the percentage of childbirth by cesarean section reached 38.9% of all deliveries in 2018 [2]. Acute pain intensity related to this procedure is often underestimated. Gerbershagen et al. noted that of 179 types of surgical procedures that were performed in Germany, the cesarean delivery was graded as the ninth in terms of postoperative pain intensity [3]. The authors concluded that ineffective pain treatment after CS in comparison with large abdominal/thoracic procedures may be attributed to the use of regional anesthesia techniques, especially epidural in the latter.
Moreover, Marcus et al. revealed that 63% of German parturients did not receive opioids in the postoperative period [4]. Several factors can affect the use of opioids in this specific population, such as respiratory depression or excessive sedation in neonates [5]. Poorly treated postoperative pain may lead to compromised early mother–child interaction due to postpartum depression and consequently to deterioration of the child’s development [6,7,8].
The effectiveness of transversus abdominis plane block (TAPB) has been demonstrated as a part of multimodal analgesia after cesarean delivery; however, its action may be limited to somatic pain and apparently only when intrathecal morphine is not administered [9]. Rafael Blanco developed a novel type of truncal block, called a quadratus lumborum block (QLB), and showed its usefulness in parturients [10]. Recently, several randomized controlled studies and one meta-analysis have provided investigations into the utility of TAPB and QLB in the reduction of acute and chronic postoperative pain after CS [11,12,13,14,15,16]. However, only one study directly compared the two types of regional blocks, which revealed the superiority of QLB over TAPB [11].
Our study aimed to reassess the effectiveness of TAPB and QLB in acute postoperative pain management after cesarean section.
2. Material and Methods
2.1. Study Design
This prospective randomized single-blind trial was conducted in a tertiary obstetric department. The study protocol was approved (permit number KE-0254/85/2016) by the local bioethics committee of Medical University of Lublin, in Lublin, Poland (Prof. Olajossy), and was registered at ClinicalTrials.gov (NCT02804126). Informed, written consent was obtained from every patient, and the study methods were in line with the tenets of the Declaration of Helsinki for medical research involving human subjects.
We included pregnant females (singleton pregnancy) older than 18 years who were scheduled for cesarean section under single-shot spinal anesthesia.
We excluded patients with coagulopathy, allergies to local anesthetics, depression, antidepressant drug therapy, epilepsy, chronic painkiller use before surgery, addiction to alcohol or recreational drugs or gestational age below 36 weeks.
2.2. Anesthesia and Regional Block
All the patients received single-shot spinal anesthesia with a 0.5% solution of hyperbaric bupivacaine. The patients received spinal injections from 2.0 to 3.0 mL of local anesthetic to reach a sufficient level of the blockade (T4–T6). Only individuals with an appropriate level of anesthesia could be randomized. At the end of the procedure, the participants were randomly allocated into one of the study arms (1:1 allocation ratio): TAPB or QLB, for ultrasound-guided regional blockade (Figure 1 and Figure 2). The team member who anesthetized the patient opened an opaque envelope that contained the patient’s study group allocation. The envelope was sealed, and the patient allocation was prepared according to the randomization procedure by a team member not directly involved in the process of anesthesia or further evaluation of the participants.
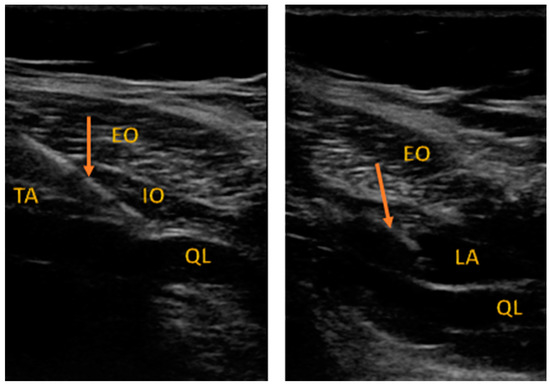
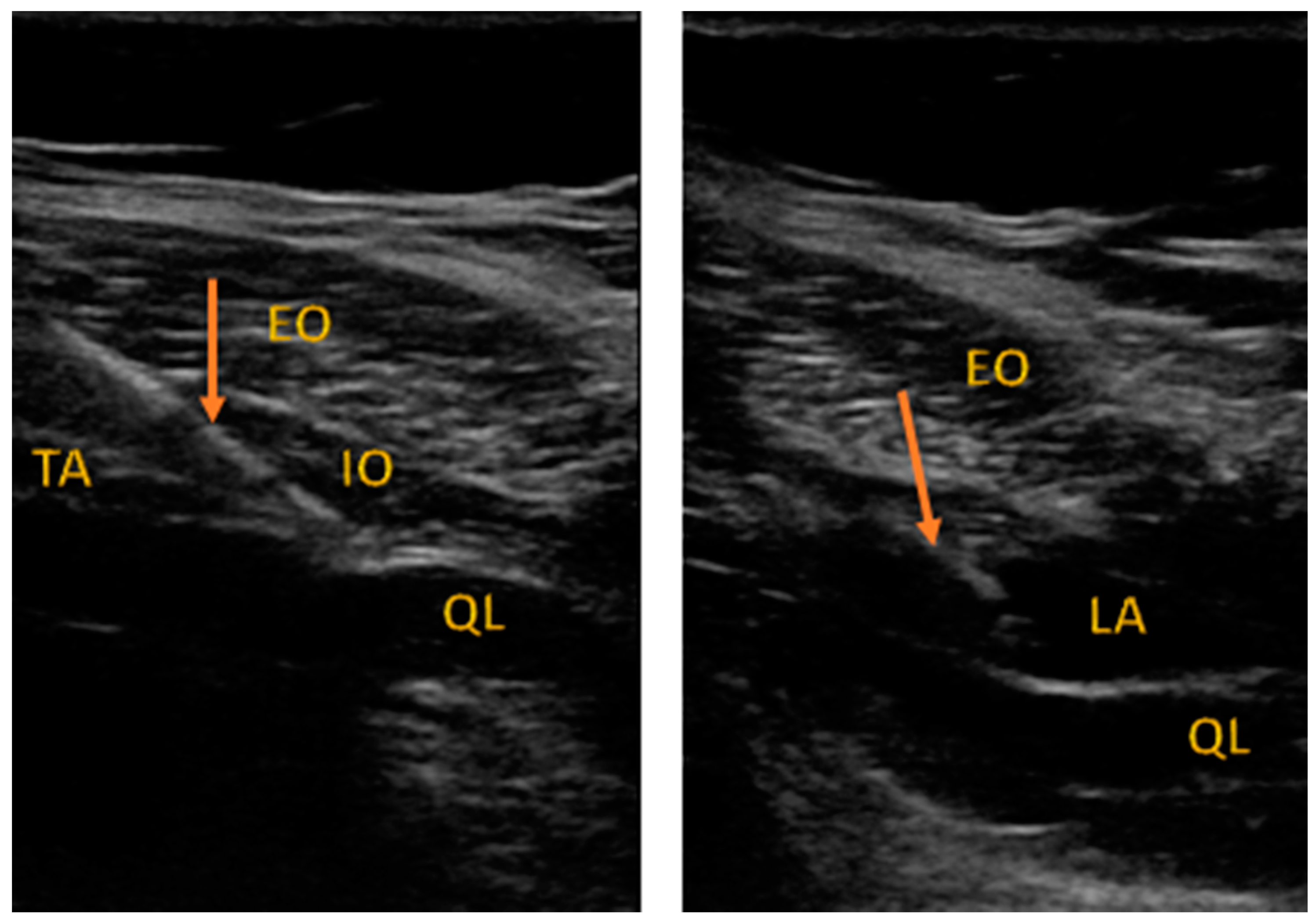
Figure 1.
Sonoanatomy of QLB performed in the study.
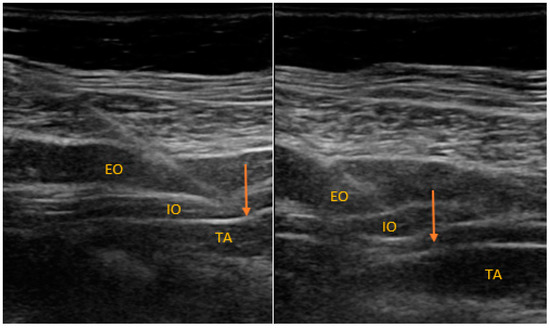
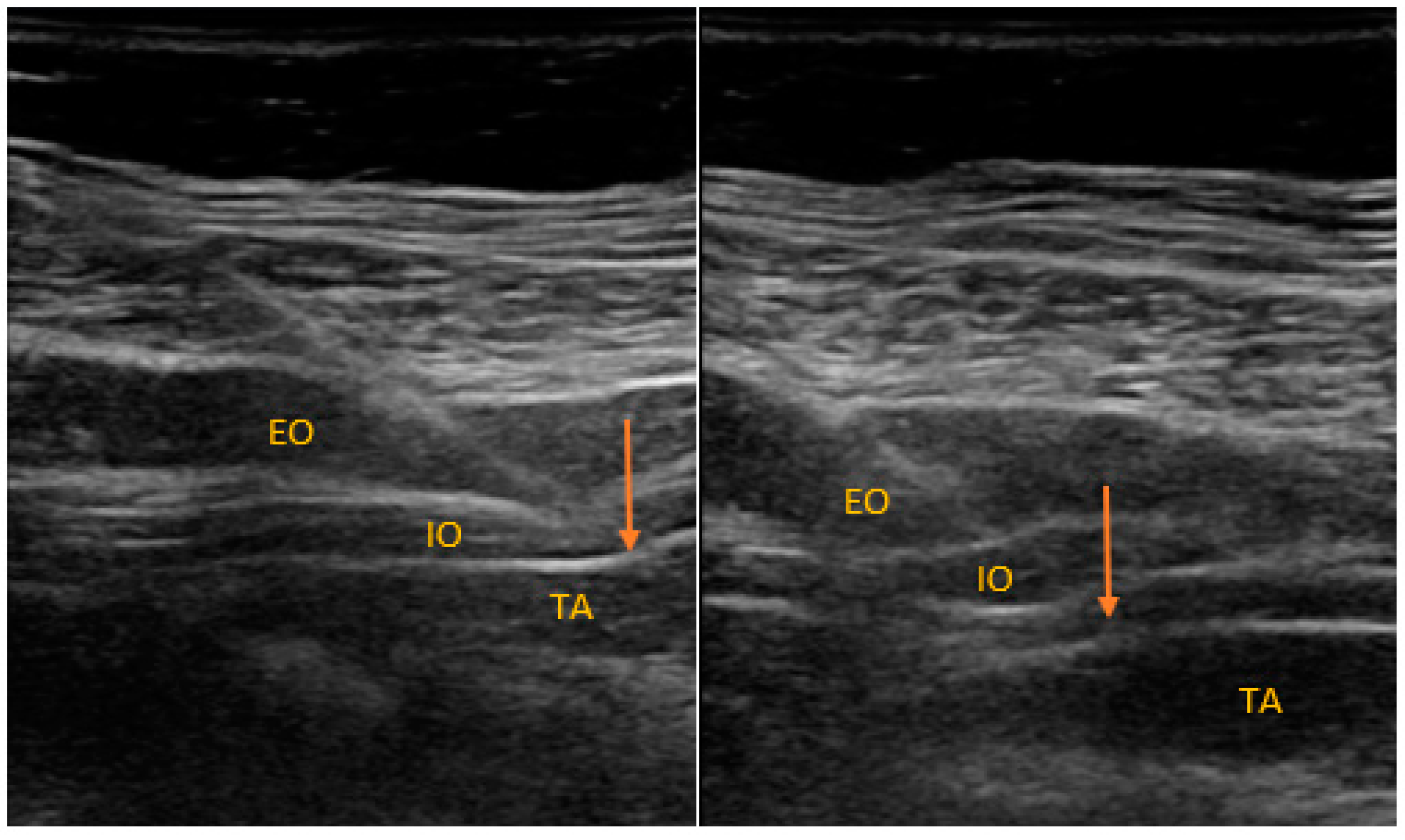
Figure 2.
Sonoanatomy of TAPB performed in the study.
Figure 1 describes the approach to QLB type 2. EO: external oblique, IO: internal oblique, TA: transversus abdominis, QL: quadratus lumborum. The arrow indicates the needle shaft.
Figure 2 describes the approach to TAPB. EO: external oblique, IO: internal oblique, TA: transversus abdominis. The arrow indicates the needle shaft.
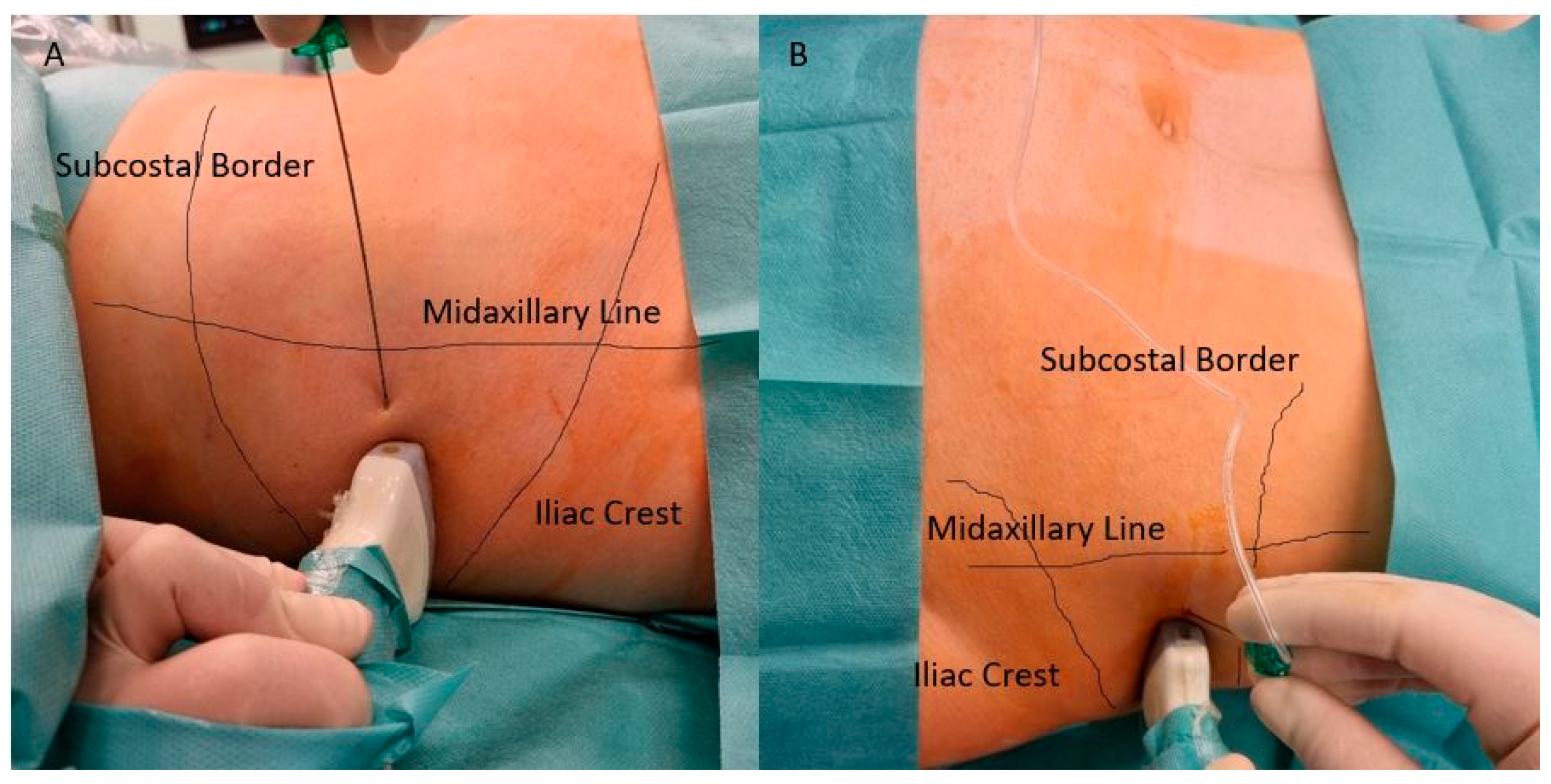
Figure 3 presents site of administration of QLB (A) and TAPB (B).
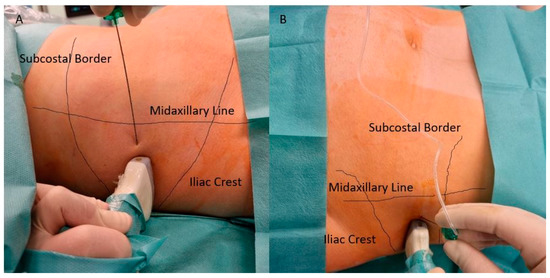
Figure 3.
Site of administration of QLB and TAPB performed in the study. (A) Approach of administration of QLB; (B) Approach of administration of TAPB. Both blocks are performed between Illiac Crest and lower border of rib cage, below Midaxillary Line and guided under linear ultrasonography as presented in Figure 1 and Figure 2.
We chose the second type of QLB as described by Blanco [17]. However, we used a linear probe to identify an optimal point of injection, similarly to the description presented by Ueshima et al. [18]. According to the study protocol, the patients were not informed about the type of regional block performed on them (single-blind or computer-generated randomization). Only three physicians performed the regional blocks (MB, BPS and PP).
The block was administered bilaterally with a 0.25% solution of bupivacaine (from 0.2 mL of local anesthetic per kilogram to a maximum dose of 20 mL per side). Every block was performed in the operating theater before the transfer of patients to the ward.
2.3. Postoperative Pain Assessment
Postoperative pain intensity was measured using the visual analog scale (VAS) at the 2nd, 4th, 8th, 12th and 24th hour after the patients’ referral to the postoperative care unit. VAS forms were collected by midwives who were not aware of the block type. The standard postoperative pain management included two of four intravenously administered drugs: paracetamol, ketoprofen, diclofenac and tramadol. Each painkiller was administered at the scheduled time point. In the case of severe pain (more than 40 mm on VAS), up to two dosages of subcutaneous (s.c.) morphine (5 mg) were administered based on a midwife’s discretion.
2.4. Statistics
Analysis of variance (ANOVA) and Student’s t-test were used to analyze parametric data. Tukey’s honest significant difference test was used for post-hoc analysis. The results obtained using the VAS were presented as means and confidence intervals (CI). The statistics for nonparametric data were calculated using the Mann–Whitney U test or the Kruskal–Wallis test by ranks and were presented as medians and interquartile ranges. Fisher’s exact test was used to analyze the contingency tables. All the measurements were performed using Statistica 12.5 software (Stat Soft. Inc., Tulsa, OK, USA).
2.5. Power Analysis
Our sample size was calculated based on the results obtained by Blanco et al., where the use of two regional blocks in alleviating acute postoperative pain was compared [11]. Because we did not use the patient-controlled analgesia (PCA) technique, we calculated a sample size according to pain intensity measured on the VAS scale. We obtained the raw data from the study by Blanco on the web site of the “Regional Anesthesia and Pain Medicine” journal. We considered five measurements of pain severity, which were obtained during the first 24 h. The mean VAS result (five evaluations) in patients after the TAPB was 19 and 15 mm in the QLB group. The calculated sample size to obtain a significant difference was 200 participants, 100 per group (alfa 0.05, power 0.8).
2.6. Outcomes
The primary outcome of our study was to evaluate pain severity in patients after QLB and TAPB at the 2nd, 4th, 8th, 12th and 24th hour. The secondary outcomes included the consumption of antinociceptive drugs during the first postoperative day and the correlation between pain intensity and indications for the cesarean section.
3. Results
3.1. Patient Demographics
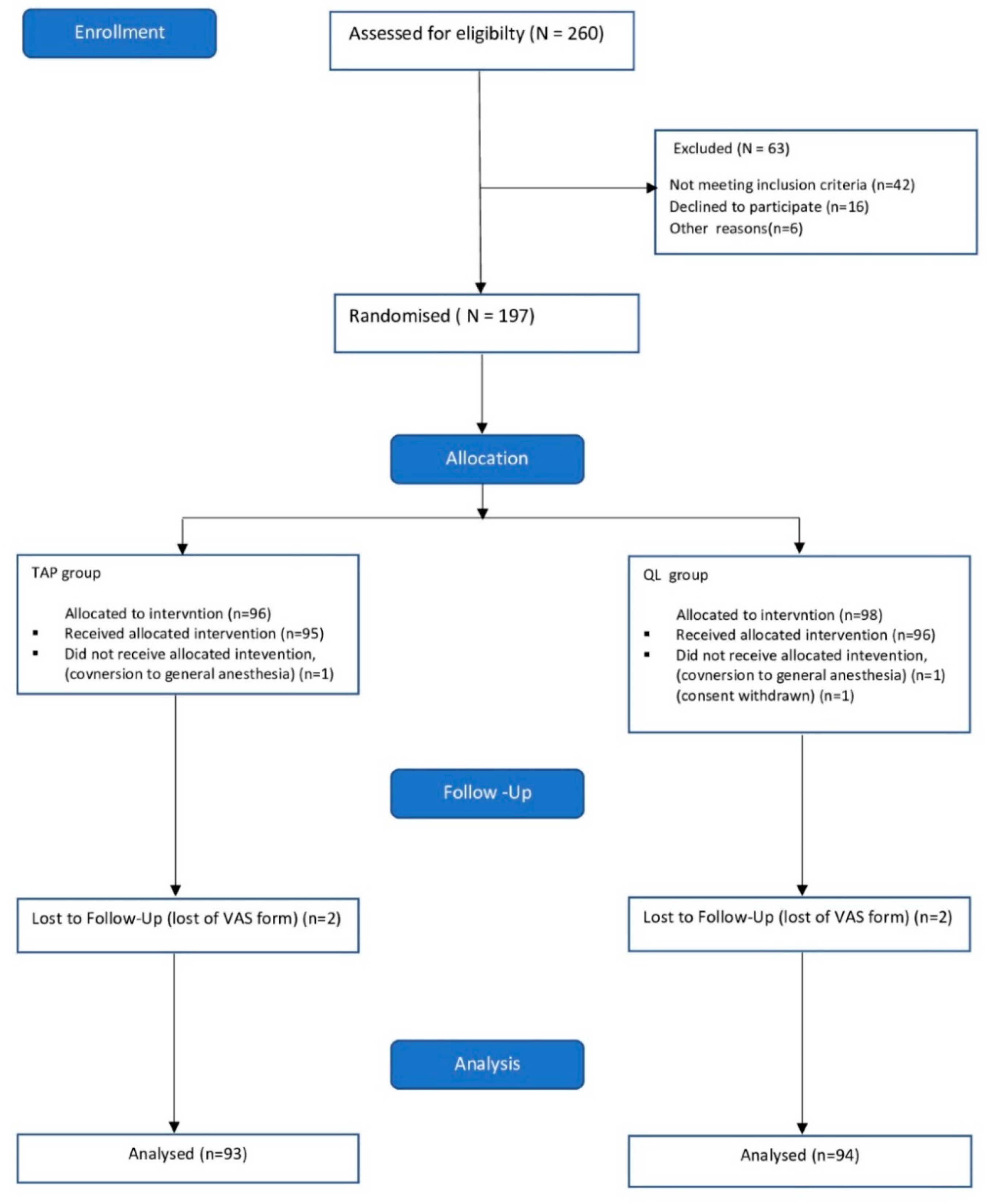
The study was conducted from June 2017 to February 2018. The CONSORT flowchart is presented in Figure 4. The patient demographics are shown in Table 1. No differences were found in age, weight, height and BMI between the study groups. The indications for cesarean deliveries are listed in Table 2.
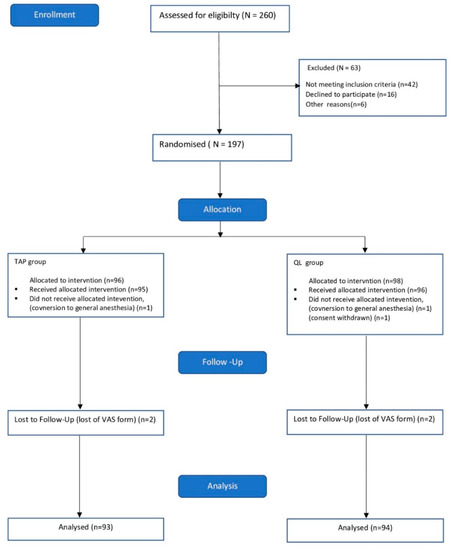
Figure 4.
Study flowchart.

Table 1.
Patient demographic.
Table 2.
Indications for cesarean delivery.
3.2. Acute Postoperative Pain
No difference in pain severity was found on the first postoperative day between the study groups. The VAS results are presented in Table 3.
Table 3.
Postoperative pain severity during the first 24 after the surgery.
3.3. Antinociceptive Drugs
No statistical significance was found in the total postoperative analgesic consumption between the study groups (Table 4). However, more patients in the TAPB group required supplemental subcutaneous morphine injections when compared with the QLB group (60 versus 46 patients, p = 0.039).
Table 4.
Mean analgesic drug consumption during the first 24 h after the surgery.
3.4. Correlation between Pain Intensity and Indications for Cesarean Section
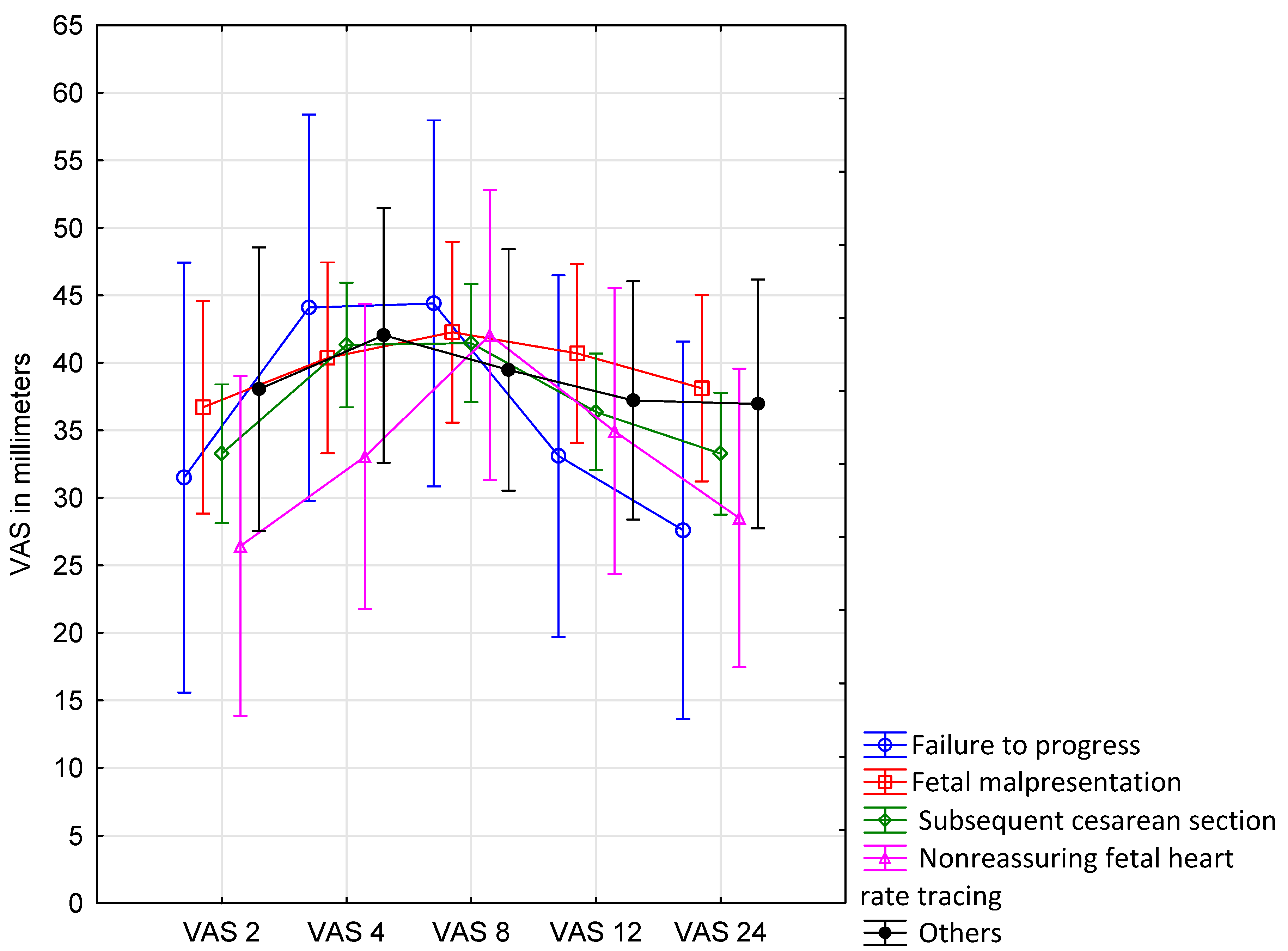
The postoperative pain severity was not affected by the indication for cesarean section (Figure 5, Table 5).
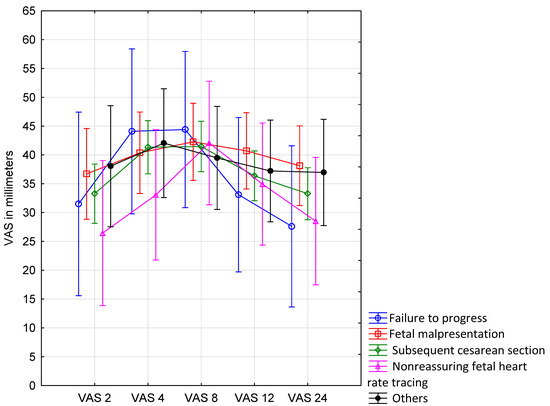
Figure 5.
Postoperative pain severity during the first 24 h after the surgery according to indications for cesarean section. The plots represent VAS results according to the type of indication for cesarean section (without the division to the study groups). The results from each measurement are shown as a mean. Vertical bars denote 0.95 confidence intervals (CI).
Table 5.
Postoperative pain severity during the first 24 h after the surgery according to indications for cesarean section and type of regional analgesia.
4. Discussion
The primary goal of our study was to compare two techniques of regional anesthesia, TAPB and QLB, in their effectiveness in postoperative pain management in obstetric patients. However, we did not find a difference between the methods according to the primary outcome of our study. Moreover, no difference was found in the total postoperative analgesic consumption between the TAPB and QLB groups. The only significant difference demonstrated in our study was associated with a higher number of TAPB patients who received s.c. morphine in the postoperative period in comparison to QLB.
The number of techniques available to enhance postoperative pain control in puerperal patients is limited [19]. The preemptive administration of antiepileptic drugs, such as gabapentinoids, lidocaine and ketamine, is controversial due to the transfer to the baby through the placenta and breastfeeding. Therefore, the broader implementation of regional anesthesia techniques seems to be the preferred approach in obstetric patients.
To our knowledge, only one randomized controlled trial involved the difference between the TAPB and QLB blocks in the management of acute postoperative pain [11]. In the study by Blanco et al., QLB was superior to TAPB in alleviating pain severity, as measured using the VAS. Moreover, patients in the QLB group consumed less morphine with patient-controlled analgesia (PCA). Contrarily, a recent meta-analysis of randomized controlled trials performed by El-Boghdadly et al. did not prove the superiority of one block over the other due to data inconsistency and methodological limitations. The authors suggested that both interventions provided comparable postoperative analgesia and opioid-sparing effects. Interestingly, both techniques were superior to inactive control only in the absence of intrathecal morphine [12]. Previously published randomized controlled studies presented the advantages of trunk blocks, such as QLB or TAPB, in comparison to standard care groups or sham blocks [15,20,21]. QLB topographically covers a broader field (T7-T12) in comparison to the ultrasound-guided TAPB (T10–T12) [22]. Ultrasound-guided or lateral TAPB has a high success rate and is safer compared with a landmark-based technique (a posterior approach through the triangle of Petit); however, it seems less effective in pain relief than the posterior approach [23]. Moreover, the lateral TAPB failed to relieve pain better than spinal morphine [24]. More studies are needed to present the advantages of different types of QLB regarding pain relief. However, the second type of QLB seems to be safer in comparison to QLB I due to a further distance from the perineum and visceral organs [25].
Although a statistical difference was found in the number of patients who received morphine, the total dose of opioids used did not differ between the groups. We suggest that this result was caused by the manner morphine was administered in the study and could be incidental. A subcutaneous route of morphine administration is controversial if other less invasive approaches, such as an oral route, are available. However, this manner was preferred by personnel of the maternity ward. The other explanation for higher morphine expenditures in the TAPB group could be a slightly lower consumption of tramadol among these patients in comparison to individuals after QLB (Table 5).
The total expenditure of intravenous opioids administered by a PCA pump is one of the best options to compare different analgesic technique. PCA possesses advantages, for example, in measuring the precise expenditure of opioids over time, drawing the drug–response curve and having excellent control of pain. However, as patients need to be immobilized by their connection to the pump, which is not coherent with the ERAS (enhanced recovery after surgery) protocol implemented in our Obstetric Department for elective cesarean sections, PCA was not used in our study [26]. Without long-lasting regional anesthesia techniques such as TAPB or QLB, the implementation of the ERAS protocol would be extremely difficult.
The main limitation of our study was the lack of a control group without any postoperative analgesic block. We did not add any opioid through the spine, which could have affected pain severity after the procedure. We did not test the spinal block area with the pinprick technique. The other drawback of our trial was associated with the route of administration of morphine and the lack of patient-controlled analgesia techniques, which could enable a better comparison with other randomized controlled trials.
5. Conclusions
In our study, none of the evaluated regional blocks demonstrated an advantage over the other in regard to acute postoperative pain management.
Author Contributions
M.B., B.P.-S. and P.P. made substantial contributions to the study design. These authors conducted the study, collected and analyzed data, and prepared the manuscript. J.S.-S. and M.C. helped to analyze and prepare the manuscript. M.B., B.P.-S., P.P., J.S.-S., P.K., E.R., T.G., A.K. helped in collection and data interpretation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved bioethics committee of Medical University of Lublin, in Lublin, Poland (permit number KE-0254/85/2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Due to the applicable privacy regulation (GDPR) and Good Clinical Practices (GCP) legislation, the full underlying dataset supporting the study cannot be provided. Anonymized data is available on motivated request and can be send to corresponding author—Michał Borys (michalborys1@gmail.com).
Acknowledgments
Assistance with the study: midwives from the Department of Obstetrics and Pathology of Pregnancy.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
ANOVA: analysis of variance; CI: confidence interval, CPSP: chronic postsurgical pain; ERAS: enhanced recovery after surgery; NPSI: Neuropathic Pain Symptom Inventory; PCA: patient-controlled analgesia; TAPB: transversus abdominis plane block; VAS: visual analogue scale; QLB: quadratus lumborum block.
References
- Boerma, T.; Ronsmans, C.; Melesse, D.Y.; Barros, A.J.D.; Barros, F.C.; Juan, L.; Moller, A.B.; Say, L.; Hosseinpoor, A.R.; Yi, M.; et al. Global epidemiology of use of and disparities in caesarean sections. Lancet 2018, 392, 1341–1348. [Google Scholar] [CrossRef]
- Caesarean sections—Organisation for Economic Co-operation and Development. Available online: https://data.oecd.org/healthcare/caesarean-sections.htm (accessed on 17 May 2021).
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain intensity on the first day after surgery: A prospective cohort study comparing 179 surgical procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcus, H.; Gerbershagen, H.J.; Peelen, L.M.; Aduckathil, S.; Kappen, T.H.; Kalkman, C.J.; Meissner, W.; Stamer, U.M. Quality of pain treatment after caesarean section: Results of a multicentre cohort study. Eur. J. Pain 2015, 19, 929–939. [Google Scholar] [CrossRef]
- Hendrickson, R.G.; McKeown, N.J. Is maternal opioid use hazardous to breast-fed infants? Clin. Toxicol. 2012, 50, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Eisenach, J.C.; Pan, P.H.; Smiley, R.; Lavand’homme, P.; Landau, R.; Houle, T.T. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain 2008, 140, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Grace, S.L.; Evindar, A.; Stewart, D.E. The effect of postpartum depression on child cognitive development and behavior: A review and critical analysis of the literature. Arch. Womens Ment. Health 2003, 6, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Keenan, T.R.; Shipton, E.A. Psychosocial adjustment and physical health of children living with maternal chronic pain. J. Paediatr. Child. Health 2007, 43, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Champaneria, R.; Shah, L.; Wilson, M.; Daniels, J. Clinical effectiveness of transversus abdominis plane (TAP) blocks for pain relief after caesarean section: A meta-analysis. Int. J. Obstet. Anesth. 2016, 28, 45–60. [Google Scholar] [CrossRef]
- Blanco, R.; Ansari, T.; Girgis, E. Quadratus lumborum block for postoperative pain after caesarean section: A randomised controlled trial. Eur. J. Anaesthesiol. 2015, 32, 812–818. [Google Scholar] [CrossRef]
- Blanco, R.; Ansari, T.; Riad, W.; Shetty, N. Quadratus Lumborum Block Versus Transversus Abdominis Plane Block for Postoperative Pain After Cesarean Delivery: A Randomized Controlled Trial. Reg. Anesth. Pain Med. 2016, 41, 757–762. [Google Scholar] [CrossRef]
- El-Boghdadly, K.; Desai, N.; Halpern, S.; Blake, L.; Odor, P.M.; Bampoe, S.; Carvalho, B.; Sultan, P. Quadratus lumborum block vs. transversus abdominis plane block for caesarean delivery: A systematic review and network meta-analysis *. Anaesthesia 2021, 76, 393–403. [Google Scholar] [CrossRef]
- Kwikiriza, A.; Kiwanuka, J.K.; Firth, P.G.; Hoeft, M.A.; Modest, V.E.; Ttendo, S.S. The analgesic effects of intrathecal morphine in comparison with ultrasound-guided transversus abdominis plane block after caesarean section: A randomised controlled trial at a Ugandan regional referral hospital. Anaesthesia 2019, 74, 167–173. [Google Scholar] [CrossRef]
- Hansen, C.K.; Dam, M.; Steingrimsdottir, G.E.; Laier, G.H.; Lebech, M.; Poulsen, T.D.; Chan, V.W.S.; Wolmarans, M.; Bendtsen, T.F.; Børglum, J. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: A double-blind randomized trial. Reg. Anesth. Pain Med. 2019. Ahead of print. [Google Scholar] [CrossRef]
- Irwin, R.; Stanescu, S.; Buzaianu, C.; Rademan, M.; Roddy, J.; Gormley, C.; Tan, T. Quadratus lumborum block for analgesia after caesarean section: A randomised controlled trial. Anaesthesia 2020, 75, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borys, M.; Potręć-Studzińska, B.; Wiech, M.; Piwowarczyk, P.; Sysiak-Sławecka, J.; Rypulak, E.; Gęca, T.; Kwaśniewska, A.; Czuczwar, M. Transversus abdominis plane block and quadratus lumborum block did not reduce the incidence or severity of chronic postsurgical pain following cesarean section: A prospective, observational study. Anaesthesiol. Intensive Ther. 2019, 51, 257–261. [Google Scholar] [CrossRef]
- Blanco, R.; McDonnell, J.G. Optimal Point of Injection: The Quadratus Lumborum Type I and II Blocks. 2013. Available online: http://www.respond2articles.com/ANA/forums/post/1550.aspx (accessed on 1 June 2016).
- Ueshima, H.; Otake, H.; Lin, J.A. Ultrasound-Guided Quadratus Lumborum Block: An Updated Review of Anatomy and Techniques. Biomed. Res. Int. 2017, 2017, 2752876. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P. Postoperative cesarean pain: Real but is it preventable? Curr. Opin. Anaesthesiol. 2018, 31, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Belavy, D.; Cowlishaw, P.J.; Howes, M.; Phillips, F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br. J. Anaesth. 2009, 103, 726–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonnell, J.G.; O’Donnell, B.; Curley, G.; Heffernan, A.; Power, C.; Laffey, J.G. The analgesic efficacy of transversus abdominis plane block after abdominal surgery: A prospective randomized controlled trial. Anesth. Analg. 2007, 104, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Akerman, M.; Pejčić, N.; Veličković, I. A Review of the Quadratus Lumborum Block and ERAS. Front. Med. 2018, 5, 44. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Laffey, J.G.; Halpern, S.H.; Brull, R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: A meta-analysis. Br. J. Anaesth. 2013, 111, 721–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMorrow, R.C.; Ni Mhuircheartaigh, R.J.; Ahmed, K.A.; Aslani, A.; Ng, S.C.; Conrick-Martin, I.; Dowling, J.J.; Gaffney, A.; Loughrey, J.P.; McCaul, C.L. Comparison of transversus abdominis plane block vs spinal morphine for pain relief after Caesarean section. Br. J. Anaesth. 2011, 106, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Børglum, J.; Gögenür, I.; Bendtsen, T.F. Abdominal wall blocks in adults. Curr. Opin. Anaesthesiol. 2016, 29, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Corso, E.; Hind, D.; Beever, D.; Fuller, G.; Wilson, M.J.; Wrench, I.J.; Chambers, D. Enhanced recovery after elective caesarean: A rapid review of clinical protocols, and an umbrella review of systematic reviews. BMC Pregnancy Childbirth 2017, 17, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).