
Community-Based Monitoring in the New Normal: A Strategy for Tackling the COVID-19 Pandemic in Malaysia


Abstract
:1. Introduction
1.1. The COVID-19 Pandemic in Malaysia
1.2. Movement Control Order

{kind=link}
{kind=link}
{kind=link}
| 1st MCO | 2nd MCO | 3rd MCO | 4th CMCO | 5th CMCO | 6th RMCO | 7th RMCO | |
|---|---|---|---|---|---|---|---|
| Period | 18 Mar–31 Mar 2020 | 1 Apr–14 Apr 2020 | 15 Apr–28 Apr 2020 | 29 Apr–12 May 2020 | 13 May–9 June 2020 | 10 June–31 Aug 2020 | 1 Sept–31 Dec 2020 |
| Economy Activities | |||||||
| Agricultural | As usual | As usual | As usual | As usual | As usual | As usual | As usual |
| Mining & Quarrying | Ordered to close | Ordered to close | 50% of workforce allowed to operate | 100% workforce allowed to operate | Normal operation with SOP | Normal operation with SOP | Normal operation with SOP |
| Construction | |||||||
| Manufacturing | Food production only | Food production only | |||||
| Services | Allowed to operate:
| Allowed to operate
| Allowed to operate
| All services allowed except cinemas, gymnasium, and salons | All services allowed except cinemas, gymnasium, and salons | All services allowed to operate with SOP | All services allowed to operate with SOP |
| Social Activities | |||||||
| Education | Ordered to close | Ordered to close | Ordered to close | Ordered to close | Ordered to close | Only higher institutions remain closed | Only higher institutions remain closed |
| Religious | Ordered to close | Ordered to close | Ordered to close | Ordered to close | Ordered to close | Allowed to open with SOP | Allowed to open with SOP |
| Travel | Allowed only within the district | Allowed only within the district | Allowed only within the district | Only interdistrict allowed | Only interdistrict allowed | Restriction only to overseas | Restriction only to overseas |
| Sports | Not allowed | Not allowed | Not allowed | Only nonphysical contact allowed effective 4 May 2020 | Only nonphysical contact allowed | Physical contact sports allowed with SOP | Physical contact sports allowed with SOP |
| Social gathering | Not allowed | Not allowed | Not allowed | Not allowed | Not allowed | Allowed in less than 250 attendees with SOP | Allowed in less than 250 attendees with SOP |
2. Post-COVID-19: The New Normal
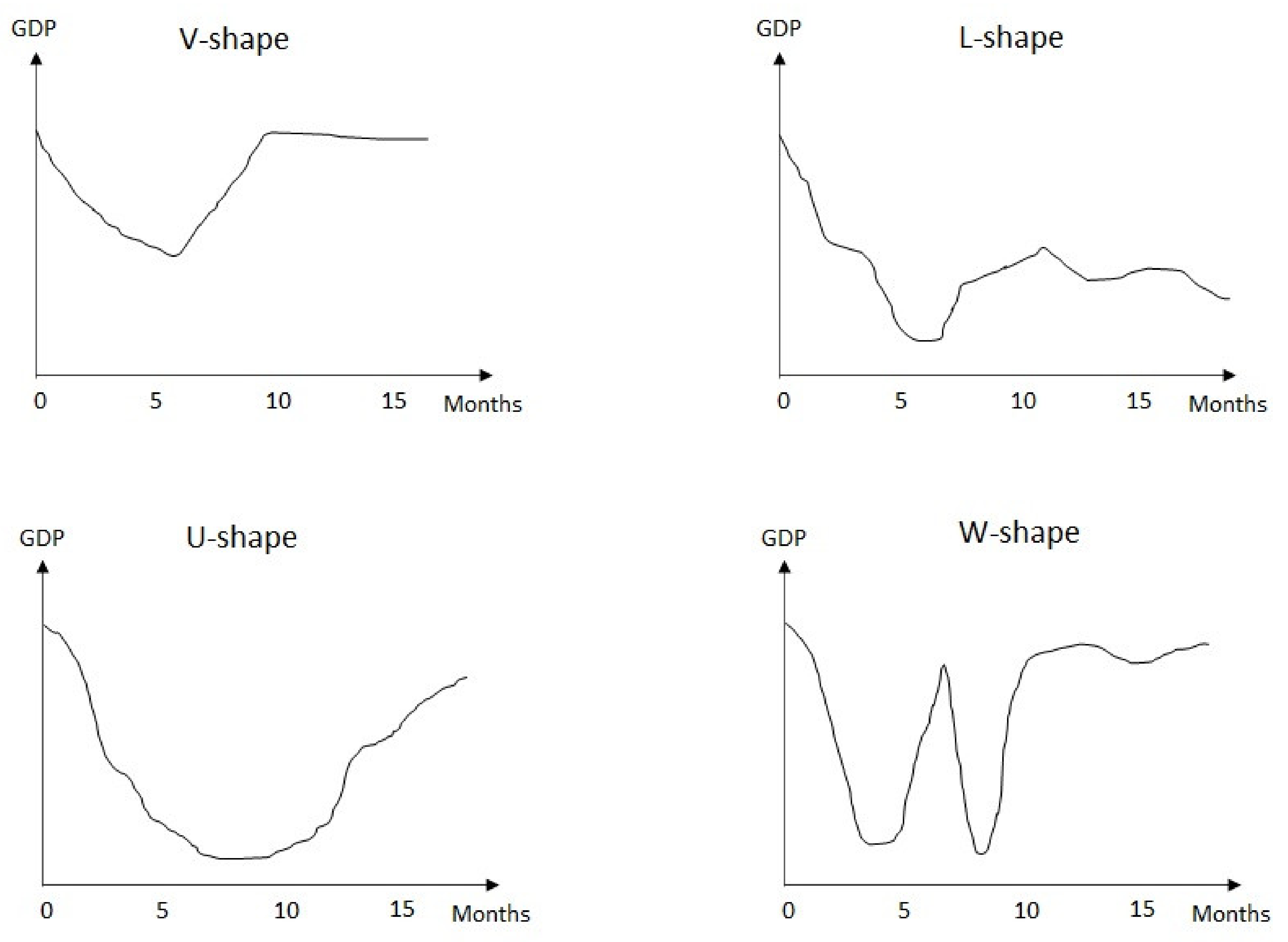
2.1. Economic Reboot
2.2. Social and Behavioral Changes
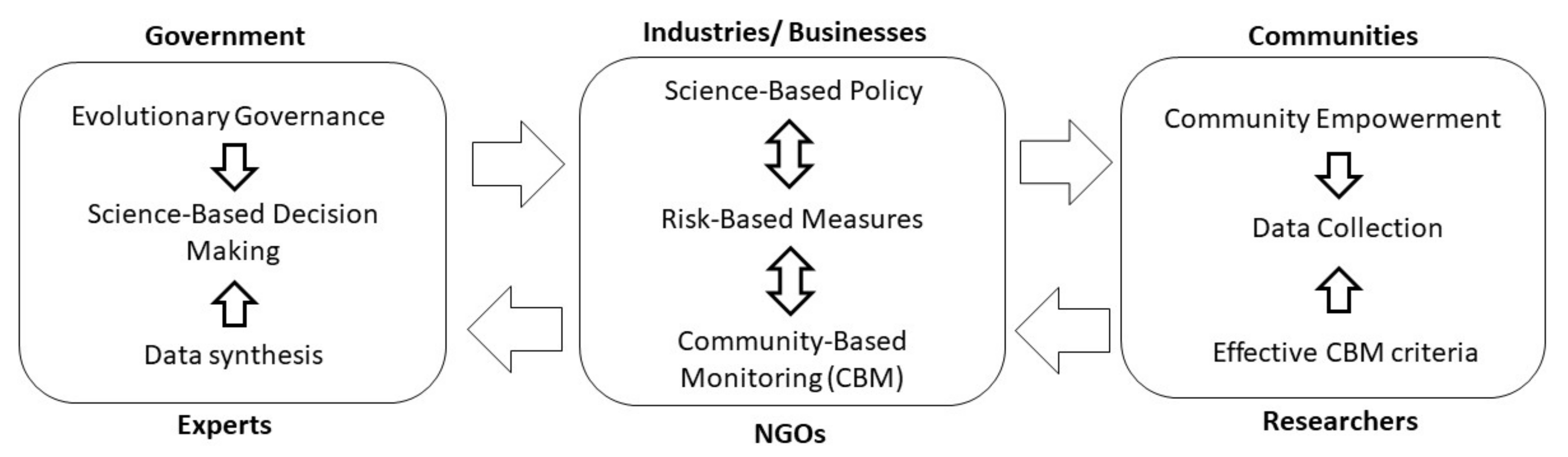
3. Calling for Evolutionary Governance
3.1. Volatility, Uncertainty, Complexity, and Ambiguity
3.2. Science-Driven Policy and Decision Making
| Items | MySejahtera | Selangkah | PGCare | Qmunity |
|---|---|---|---|---|
| Organizer | Federal government | State government (Selangor) | State government (Penang) | State government (Sarawak) |
| Date of launched | 20 Apr–now | 5 May–now | 15 May–31 Aug 2020 | 9 Apr–now |
| Status | Active | Active | Deactivated | Active |
| Coverage | Whole Malaysia | Restricted to Selangor | Restricted to Penang | Restricted to Sarawak |
| Registration document |
| Phone number | Phone number |
|
| Function |
|
|
|
|
| Type of data collected |
|
|
|
|
| Language |
|
|
|
|
| Security | Phone number verification | Not Available | Phone number verification |
|
| Additional features |
|
| Not Available |
|
| Check-in history | Yes | No | No | Yes |
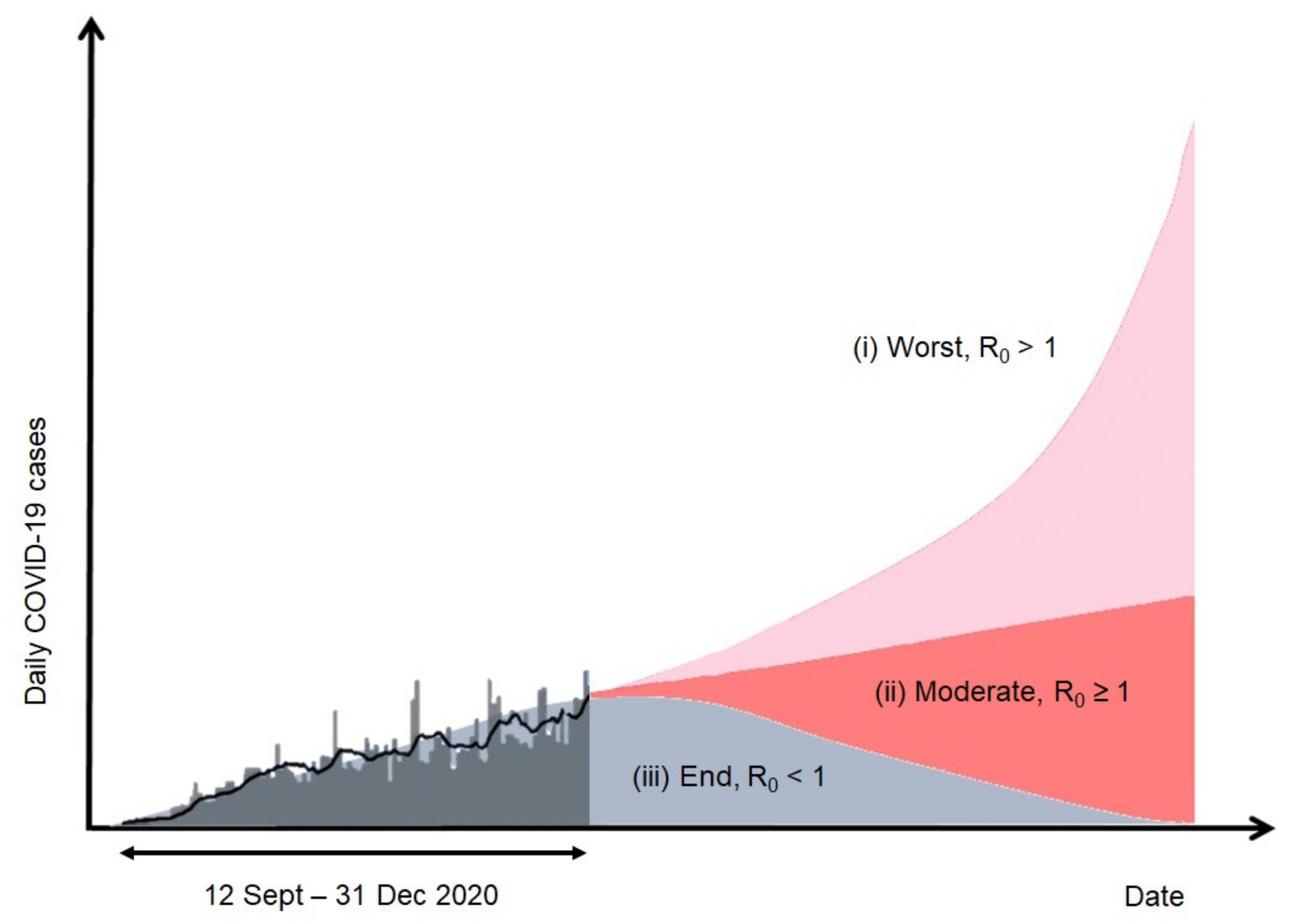
3.3. Risk-Based Measures
4. Community-Based Monitoring as a Means of Moving Forward in Terms of the Response of the Government to the Pandemic and the New Normal
4.1. Approach
4.2. Criteria
4.2.1. Efficacy
4.2.2. Technicality
4.2.3. Feedback
4.2.4. Sustainability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ebrahim, S.H.; Ahmed, Q.A.; Gozzer, E.; Schlagenhauf, P.; Memish, Z.A. Covid-19 and community mitigation strategies in a pandemic. BMJ 2020, 368, m1066. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, M.U.G.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D.M.; Du Plessis, L.; Faria, N.R.; Li, R.; Hanage, W.P.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [Green Version]
- Arolas, H.P.I.; Acosta, E.; López-Casasnovas, G.; Lo, A.; Nicodemo, C.; Riffe, T.; Myrskylä, M. Years of life lost to COVID-19 in 81 countries. Sci. Rep. 2021, 11, 1–6. [Google Scholar] [CrossRef]
- Nurchis, M.C.; Pascucci, D.; Sapienza, M.; Villani, L.; D’Ambrosio, F.; Castrini, F.; Specchia, M.L.; Laurenti, P.; Damiani, G. Impact of the Burden of COVID-19 in Italy: Results of Disability-Adjusted Life Years (DALYs) and Productivity Loss. Int. J. Environ. Res. Public Health 2020, 17, 4233. [Google Scholar] [CrossRef]
- Vasishtha, G.; Mohanty, S.K.; Mishra, U.S.; Dubey, M.; Sahoo, U. Impact of COVID-19 infection on life expectancy, premature mortality, and DALY in Maharashtra, India. BMC Infect. Dis. 2021, 21, 343. [Google Scholar] [CrossRef]
- Zhao, J.; Jin, H.; Li, X.; Jia, J.; Zhang, C.; Zhao, H.; Ma, W.; Wang, Z.; He, Y.; Lee, J.; et al. Disease Burden Attributable to the First Wave of COVID-19 in China and the Effect of Timing on the Cost-Effectiveness of Movement Restriction Policies. Value Health 2021, 24, 615–624. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Abdullah, N.H. Tindakan KKM Bagi Pengesanan Kontak (Contact Tracing) Kepada Kes Pertama Positif Novel Coronavirus Di Negara Singapura Pada 24 Januari 2020. Available online: https://kpkesihatan.com/2020/01/24/kenyataan-akhbar-kpk-24-januari-2020-tindakan-kkm-bagi-pengesanan-kontak-contact-tracing-kepada-kes-pertama-positif-novel-coronavirus-di-negara-singapura-pada-24-januari-2020/ (accessed on 20 June 2020).
- Abdullah, N.H. Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia, MOH Malaysia. 2020. Available online: https://kpkesihatan.com/2020/03/04/kenyataan-akhbar-kpk-4-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 12 October 2020).
- New Straits Times. How Sri Petaling Tabligh Became Southeast Asia’s COVID-19 Hotspot. 2020. Available online: https://www.nst.com.my/news/nation/2020/03/575560/how-sri-petaling-tabligh-became-southeast-asias-COVID-19-hotspot/ (accessed on 14 June 2020).
- Roslan, S. Tabligh Event Attendees 12k, not 16k. 2020. Available online: https://www.nst.com.my/news/nation/2020/03/577014/tabligh-event-attendees-12k-not-16k/ (accessed on 9 July 2020).
- Abdullah, N.H. Nilai Rt Terkini Bagi Wabak COVID-19 di Malaysia. 2020. Available online: https://kpkesihatan.com/2020/10/18/kenyataan-akhbar-kpk-18-oktober-2020-nilai-rt-terkini-bagi-wabak-COVID-19-di-malaysia/ (accessed on 20 October 2020).
- Abdullah, N.H. Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia. 2020. Available online: https://kpkesihatan.com/2020/12/31/kenyataan-akhbar-kpk-31-disember-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 31 December 2020).
- Tan, T. Covid-19: 1870 New Cases, Johor Tops List. 2020. Available online: https://www.thestar.com.my/news/nation/2020/12/30/covid-19-1870-new-cases-johor-tops-list/ (accessed on 30 December 2020).
- Yassin, M. The Prime Minister’s Special Message on COVID-19 16 March 2020. 2020. Available online: https://www.pmo.gov.my/2020/03/perutusan-khas-yab-perdana-menteri-mengenai-COVID-19-16-mac-2020/ (accessed on 26 June 2020).
- López, L.; Rodó, X. The end of social confinement and COVID-19 re-emergence risk. Nat. Hum. Behav. 2020, 4, 746–755. [Google Scholar] [CrossRef]
- MOH Malaysia. SOP Perintah Kawalan Pergerakan Diperketatkan (PKPD). 2020. Available online: http://COVID-19.moh.gov.my/faqsop/sop-perintah-kawalan-pergerakan-pkp/ (accessed on 25 November 2020).
- MOH Malaysia. SOP PKP Pemulihan (Bermula 10 June 2020). 2020. Available online: http://COVID-19.moh.gov.my/faqsop/sop-pkp-pemulihan/ (accessed on 22 September 2020).
- TheStar. NZ in Deepest Recession as Q2 GDP Shrinks. 2020. Available online: https://www.thestar.com.my/business/business-news/2020/09/17/new-zealand-economy-in-deepest-recession-as-q2-gdp-shrinks/ (accessed on 5 October 2020).
- The Straits Times. Oil Sinks below US$30 a Barrel on Global Recession Threat. 2020. Available online: https://www.straitstimes.com/business/companies-markets/brent-crude-sinks-below-us30-a-barrel-as-recession-fears-weigh (accessed on 5 May 2020).
- Kelly, S. Oil Prices Surge as Coronavirus Lockdowns Ease. 2020. Available online: https://www.reuters.com/article/us-global-oil/oil-prices-rise-on-demand-prospects-as-lockdowns-start-to-ease-idUSKBN22H033/ (accessed on 6 November 2020).
- Gualdi, S.; Tarzia, M.; Zamponi, F.; Bouchaud, J.-P. Monetary policy and dark corners in a stylized agent-based model. J. Econ. Interact. Co-Ord. 2016, 12, 507–537. [Google Scholar] [CrossRef] [Green Version]
- Góes, M.C.B.; Gallo, E. A Predator-Prey Model of Unemployment and W-shaped Recession in the COVID-19 Pandemic. Grad. Fac. Philos. J. 2020. Available online: http://www.economicpolicyresearch.org/econ/2020/NSSR_WP_062020.pdf (accessed on 17 September 2020).
- New Straits Times. Government Announces Second Round of BPN Aid for B40, M40. 2020. Available online: https://www.nst.com.my/news/nation/2020/09/626633/government-announces-second-round-bpn-aid-b40-m40/ (accessed on 16 September 2020).
- Yassin, M. Prihatin Rakyat Economic Stimulus Package (PRIHATIN). 2020. Available online: https://www.pmo.gov.my/2020/03/speech-text-prihatin-esp/ (accessed on 26 June 2020).
- Sharma, D.; Bouchaud, J.P.; Gualdi, S.; Tarzia, M.; Zamponi, F. Economic recovery after COVID-19? Insights from an agent-based model1. COVID Econ. 2020, 40, 149–161. [Google Scholar] [CrossRef]
- Ellis, R. WHO Changes Stance Says Public Should Wear Masks. 2020. Available online: https://www.webmd.com/lung/news/20200608/who-changes-stance-says-public-should-wear-masks/ (accessed on 13 November 2020).
- Abas, A. RM1000 Fine Flouting Mask Wearing Rule. 2020. Available online: https://www.nst.com.my/news/nation/2020/08/613889/rm1000-fine-flouting-mask-wearing-rule-excessive/ (accessed on 10 October 2020).
- MOH Malaysia. Annex 8a: Guidance on the Use of Masks with Regards to COVID-19 Pandemic. 2020. Available online: http://COVID-19.moh.gov.my/garis-panduan/garis-panduan-kkm/Annex_8a_RECOMENDATIONS_ON_FACE_MASK.pdf/ (accessed on 17 November 2020).
- Irhas, E.M.; Dyah, S.; Yuni, I. Social Media Adoption in SMEs Impacted by COVID-19: The TOE Model. J. Asian Financ. Econ. Bus. 2020, 7, 915–925. [Google Scholar] [CrossRef]
- Hasanat, M.W.; Hoque, A.; Shikha, F.A.; Anwar, M.; Hamid, A.B.A.; Tat, H.H. The Impact of Coronavirus (COVID-19) on E-Business in Malaysia. Asian J. Multidiscip. Stud. 2020, 3, 85–90. [Google Scholar]
- New Straits Times. Panic Buying at Supermarkets Nationwide. 2020. Available online: https://www.nst.com.my/news/nation/2020/03/575302/COVID-19-panic-buying-supermarkets-nationwide-nsttv/ (accessed on 9 June 2020).
- Kouchaki, M.; Desai, S.D. Anxious, threatened, and also unethical: How anxiety makes individuals feel threatened and commit unethical acts. J. Appl. Psychol. 2015, 100, 360–375. [Google Scholar] [CrossRef] [Green Version]
- Yau, E.K.B.; Ping, N.P.T.; Shoesmith, W.D.; James, S.; Hadi, N.M.N.; Loo, L.J. The Behaviour Changes in Response to COVID-19 Pandemic within Malaysia. Malays. J. Med Sci. 2020, 27, 45–50. [Google Scholar] [CrossRef]
- The Straits Times. Coronavirus: Malaysia to Allow Weddings Social Events from July 1 with Maximum of 250 People. 2020. Available online: https://www.straitstimes.com/asia/se-asia/coronavirus-malaysia-to-allow-weddings-social-events-from-july-1-with-maximum-of-250/ (accessed on 9 August 2020).
- MOH Malaysia. SOP am Pelaksanaan Majlis Sosial. MOH Malaysia. 2020. Available online: http://COVID-19.moh.gov.my/faqsop/sop-pkp-pemulihan/SOP-Majlis-Sosial_-25-JUN-2020.pdf/ (accessed on 10 October 2020).
- Janssen, M.; van der Voort, H. Agile and adaptive governance in crisis response: Lessons from the COVID-19 pandemic. Int. J. Inf. Manag. 2020, 55, 102180. [Google Scholar] [CrossRef]
- Van Assche, K.; Beunen, R.; Duineveld, M. Evolutionary Governance Theory: An Introduction; Springer Science & Business Media: Heidelberg, Germany; New York, NY, USA; London, UK, 2013. [Google Scholar]
- Beunen, R.; van Assche, K.; Duineveld, M. Evolutionary Governance Theory; Springer International Publishing: Cham, Switzerland, 2015. [Google Scholar]
- Hassan, M.M.; Lee, K.E.; Mokhtar, M. Mainstreaming, Institutionalizing and Translating Sustainable Development Goals into Non-governmental Organization’s Programs. In Plant-Microbes-Engineered Nano-particles (PM-ENPs) Nexus in Agro-Ecosystems; Springer: Cham, Switzerland, 2020; pp. 93–118. [Google Scholar]
- Hassan, M.M.; Lee, K.E.; Mokhtar, M. Streamlining non-governmental organizations’ programs towards achieving the sustainable development goals: A conceptual framework. Sustain. Dev. 2019, 27, 401–408. [Google Scholar] [CrossRef]
- Johansen, B. Get There Early: Sensing the Future to Compete in the Present; Berrett-Koehler: San Francisco, CA, USA, 2007. [Google Scholar]
- Chermack, T.J. Scenario Planning in Organizations: How to Create, Use and Assess Scenarios; Berrett-Koehler: Oakland, CA, USA, 2011. [Google Scholar]
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio Med. Atenei Parm. 2020, 91, 157–160. [Google Scholar]
- Klinke, A.; Renn, O. A new approach to risk evaluation and management: Risk-based, precaution-based, and discourse-based strategies 1. Risk Anal. Int. J. 2002, 22, 1071–1094. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef]
- Béland, L.P.; Brodeur, A.; Wright, T. The Short-Term Economic Consequences of COVID-19: Exposure to Disease, Remote Work and Government Response; IZA Institute of Labor Economics: Bonn, Germany, 2020; Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3584922 (accessed on 9 June 2020).
- Kawohl, W.; Nordt, C. COVID-19, unemployment, and suicide. Lancet Psychiatry 2020, 7, 389–390. [Google Scholar] [CrossRef]
- Depoux, A.; Martin, S.; Karafillakis, E.; Preet, R.; Wilder-Smith, A.; Larson, H. The pandemic of social media panic travels faster than the COVID-19 outbreak. J. Travel Med. 2020, 27, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.D.; Ng, F.; Li, W.H.C. COVID-19: Emerging compassion, courage and resilience in the face of misinformation and adversity. J. Clin. Nurs. 2020, 29, 1425–1428. [Google Scholar] [CrossRef] [Green Version]
- Erev, I.; Plonsky, O.; Roth, Y. Complacency, panic, and the value of gentle rule enforcement in addressing pandemics. Nat. Hum. Behav. 2020, 4, 1095–1097. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Wang, R.; Wang, M.; Wei, G.W. Mutations strengthened SARS-CoV-2 infectivity. arXiv 2020, arXiv:2005.14669. [Google Scholar] [CrossRef]
- Tee, K. Decision on MCO Extension will be Based on Science and Facts, Says Health D-G. 2020. Available online: https://www.malaymail.com/news/malaysia/2020/04/18/decision-on-mco-extension-will-be-based-on-science-and-fact-says-health-d-g/1858026/ (accessed on 20 July 2020).
- Shah, A.U.M.; Safri, S.N.A.; Thevadas, R.; Noordin, N.K.; Rahman, A.A.; Sekawi, Z.; Ideris, A.; Sultan, M.T.H. COVID-19 outbreak in Malaysia: Actions taken by the Malaysian government. Int. J. Infect. Dis. 2020, 97, 108–116. [Google Scholar] [CrossRef]
- New Straits Times. Collaboration for Food Distribution. 2020. Available online: https://www.nst.com.my/news/nation/2020/03/579541/collaborate-food-distribution-say-ngos/ (accessed on 16 September 2020).
- Abdullah, N.H. Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia. 2020. Available online: https://kpkesihatan.com/2020/04/06/kenyataan-akhbar-kpk-6-april-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 16 June 2020).
- The Straits Times. Coronavirus: Malaysia to Allow Some Sectors to Ramp up Work from Half to Full Capacity. 2020. Available online: https://www.straitstimes.com/asia/se-asia/coronavirus-malaysia-to-allow-some-sectors-to-ramp-up-work-from-half-to-full-capacity/ (accessed on 20 July 2020).
- Giest, S. Big data for policymaking: Fad or fasttrack? Policy Sci. 2017, 50, 367–382. [Google Scholar] [CrossRef] [Green Version]
- Loo, C. Thermal Scanners Now in Place at KLIA Departure and Arrival Gates. 2020. Available online: https://www.thesundaily.my/local/thermal-scanners-now-in-place-at-klia-departure-and-arrival-gates-YJ2193203/ (accessed on 12 May 2020).
- Quilty, B.J.; Clifford, S.; Flasche, S.; Eggo, R.M.; CMMID nCoV Working Group. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV). Eurosurveillance 2020, 25, 2000080. [Google Scholar] [CrossRef]
- MySejahtera. 2020. Available online: https://mysejahtera.malaysia.gov.my/intro/ (accessed on 6 September 2020).
- MOH Malaysia. Akta Pencegahan dan Pengawalan Penyakit Berjangkit 1988. 2020. Available online: http://COVID-19.moh.gov.my/faqsop/akta-342/ (accessed on 17 November 2020).
- TheStar. MySejahtera App a Must for All Businesses. 2020. Available online: https://www.thestar.com.my/news/nation/2020/08/04/mysejahtera-app-a-must-for-all-businesses/ (accessed on 9 August 2020).
- Abdullah, N.H. Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia. 2020. Available online: https://kpkesihatan.com/2020/11/19/kenyataan-akhbar-kpk-19-november-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 25 November 2020).
- Mohsen, A.S. MySejahtera Contact Tracing App Required to Enjoy RM50 e-Wallet Credit. 2020. Available online: https://www.thesundaily.my/COVID-19/mysejahtera-contact-tracing-app-required-to-enjoy-rm50-e-wallet-credit-DX2541603/ (accessed on 8 June 2020).
- Allam, Z.; Jones, D.S. On the Coronavirus (COVID-19) Outbreak and the Smart City Network: Universal Data Sharing Standards Coupled with Artificial Intelligence (AI) to Benefit Urban Health Monitoring and Management. Healthcare 2020, 8, 46. [Google Scholar] [CrossRef] [Green Version]
- PGcare. 2020. Available online: https://pgcare.my/home/ (accessed on 20 September 2020).
- SELangkah. 2020. Available online: https://www.selangkah.my/web/ (accessed on 8 November 2020).
- Qmunity. 2020. Available online: https://web.qmunity.app/ (accessed on 8 November 2020).
- Carcione, J.M.; Santos, J.E.; Bagaini, C.; Ba, J. A Simulation of a COVID-19 Epidemic Based on a Deterministic SEIR Model. Front. Public Health 2020, 8, 230. [Google Scholar] [CrossRef]
- Heffernan, J.M.; Smith, R.J.; Wahl, L. Perspectives on the basic reproductive ratio. J. R. Soc. Interface 2005, 2, 281–293. [Google Scholar] [CrossRef]
- Diekmann, O.; Heesterbeek, J.A.P.; Metz, J.A.J. On the definition and the computation of the basic reproduction ratio R 0 in models for infectious diseases in heterogeneous populations. J. Math. Biol. 1990, 28, 365–382. [Google Scholar] [CrossRef] [Green Version]
- Delamater, P.L.; Street, E.J.; Leslie, T.F.; Yang, Y.T.; Jacobsen, K. Complexity of the Basic Reproduction Number (R0). Emerg. Infect. Dis. 2019, 25, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Povera, A. Community Empowerment is Final Criteria in Covid-19 Exit Plan. 2020. Available online: https://www.nst.com.my/news/nation/2020/05/596047/community-empowerment-final-criteria-COVID-19-exit-plan/ (accessed on 13 June 2020).
- Abdullah, A. Going Glocal: Cultural Dimensions in Malaysian Management; Malaysian Institute of Management: Selangor, Malaysia, 1996. [Google Scholar]
- Chirimbu, S.; Vargolici, N. Community Leader between Influence, Responsibility and Progress; SSRN 2013. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2377069 (accessed on 17 May 2020).
- Rahman, F. The Malaysian Response to COVID-19: Building Preparedness for ‘Surge Capacity’, Testing Efficiency, and Containment. 2020. Available online: https://kpkesihatan.com/2020/06/16/the-malaysian-response-to-covid-19-building-preparedness-for-surge-capacity-testing-efficiency-and-containment/ (accessed on 2 November 2020).
- Khair, N.M.; Lee, K.; Mokhtar, M. Sustainable City and Community Empowerment through the Implementation of Community-Based Monitoring: A Conceptual Approach. Sustainability 2020, 12, 9583. [Google Scholar] [CrossRef]
- Conrad, C.C.; Hilchey, K.G. A review of citizen science and community-based environmental monitoring: Issues and opportunities. Environ. Monit. Assess. 2010, 176, 273–291. [Google Scholar] [CrossRef]
- Danielsen, F.; Burgess, N.D.; Balmford, A.; Donald, P.F.; Funder, M.; Jones, J.P.G.; Alviola, P.; Balete, D.S.; Blomley, T.; Brashares, J.; et al. Local Participation in Natural Resource Monitoring: A Characterization of Approaches. Conserv. Biol. 2009, 23, 31–42. [Google Scholar] [CrossRef]
- Whitelaw, G.; Vaughan, H.; Craig, B.; Atkinson, D. Establishing the Canadian Community Monitoring Network. Environ. Monit. Assess. 2003, 88, 409–418. [Google Scholar] [CrossRef]
- Overdevest, C.; Orr, C.H.; Stepenuck, K. Volunteer stream monitoring and local participation in natural resource issues. Res. Hum. Ecol. 2004, 11, 177–185. [Google Scholar]
- Laskar, A.R.; Garg, S. Community-based monitoring: Key to success of national health programs. Indian J. Community Med. 2010, 35, 214–216. [Google Scholar] [CrossRef]
- Mswia, R.; Lewanga, M.; Moshiro, C.; Whiting, D.; Wolfson, L.; Hemed, Y.; Alberti, K.G.M.M.; Kitange, H.; Mtasiwa, D.; Setel, P. Community-based monitoring of safe motherhood in the United Republic of Tanzania. Bull. World Health Organ. 2003, 81, 87–94. [Google Scholar]
- Björkman, M.; Svensson, J. Power to the People: Evidence from a Randomized Field Experiment on Community-Based Monitoring in Uganda. Q. J. Econ. 2009, 124, 735–769. [Google Scholar] [CrossRef] [Green Version]
- Kruger, M.A.S.L.E. Getting to Know Ourselves and Our Places Through Participation in Civic Social Assessment. Soc. Nat. Resour. 2000, 13, 461–478. [Google Scholar] [CrossRef]
- Loh, P.; Sugerman-Brozan, J.; Wiggins, S.; Noiles, D.; Archibald, C. From asthma to AirBeat: Community-driven monitoring of fine particles and black carbon in Roxbury, Massachusetts. Environ. Health Perspect. 2002, 110, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Walker, D.; Forsythe, N.; Parkin, G.; Gowing, J. Filling the observational void: Scientific value and quantitative validation of hydrometeorological data from a community-based monitoring programme. J. Hydrol. 2016, 538, 713–725. [Google Scholar] [CrossRef] [Green Version]
- Khair, N.K.M.; Lee, K.E.; Mokhtar, M. Community-based monitoring for environmental sustainability: A review of characteristics and the synthesis of criteria. J. Environ. Manag. 2021, 289, 112491. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Zuliani, G.; Rigatelli, A.; Mazza, A.; Roncon, L. Arterial hypertension and risk of death in patients with COVID-19 infection: Systematic review and meta-analysis. J. Infect. 2020, 81, e84–e86. [Google Scholar] [CrossRef] [PubMed]
- De Venecia, T.; Lu, M.; Figueredo, V.M. Hypertension in young adults. Postgrad. Med. 2016, 128, 201–207. [Google Scholar] [CrossRef]
- MOSTI. MyTrace, a Preventive Counter Measure and Contact Tracing Application for COVID-19. 2020. Available online: https://www.mosti.gov.my/web/en/mytrace/ (accessed on 6 September 2020).
- Perimbanayagam, K.; Chan, D. RMCO: Many Continue to Violate SOPs. 2020. Available online: https://www.nst.com.my/news/nation/2020/10/633294/rmco-many-continue-violate-sops/ (accessed on 18 October 2020).
- Scudellari, M. How the pandemic might play out in 2021 and beyond. Nat. Cell Biol. 2020, 584, 22–25. [Google Scholar] [CrossRef]
- New Straits Times. Dengue: 50,511 Cases, 88 Deaths Registered Nationwide. 2020. Available online: https://www.nst.com.my/news/nation/2020/06/600815/dengue-50511-cases-88-deaths-registered-nationwide/ (accessed on 12 December 2020).
| EMCO | TEMCO | AEMCO | |
|---|---|---|---|
| Coverage area | Specific localities, such as district or a village | Small and specific areas, such as residential complex | Specific localities, such as district or a village |
| Days of quarantine | 14 days | 28 days | 14 days |
| Standard Operating Procedure (SOP) |
|
|
|
| Enforcement | Residents strictly needed to stay at home | Residents strictly needed to stay at home | Residents allowed to move within the area |
| Screening and testing for COVID-19 | Home to the home screening | Home to the home screening | All residents need to undergo screening at the nearby clinics |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhamad Khair, N.K.; Lee, K.E.; Mokhtar, M. Community-Based Monitoring in the New Normal: A Strategy for Tackling the COVID-19 Pandemic in Malaysia. Int. J. Environ. Res. Public Health 2021, 18, 6712. https://doi.org/10.3390/ijerph18136712
Muhamad Khair NK, Lee KE, Mokhtar M. Community-Based Monitoring in the New Normal: A Strategy for Tackling the COVID-19 Pandemic in Malaysia. International Journal of Environmental Research and Public Health. 2021; 18(13):6712. https://doi.org/10.3390/ijerph18136712
Chicago/Turabian StyleMuhamad Khair, Nur Khairlida, Khai Ern Lee, and Mazlin Mokhtar. 2021. "Community-Based Monitoring in the New Normal: A Strategy for Tackling the COVID-19 Pandemic in Malaysia" International Journal of Environmental Research and Public Health 18, no. 13: 6712. https://doi.org/10.3390/ijerph18136712
APA StyleMuhamad Khair, N. K., Lee, K. E., & Mokhtar, M. (2021). Community-Based Monitoring in the New Normal: A Strategy for Tackling the COVID-19 Pandemic in Malaysia. International Journal of Environmental Research and Public Health, 18(13), 6712. https://doi.org/10.3390/ijerph18136712