
Analysis of the Relationship between Obesity Factors and Health-Related Physical Fitness Factors among People with Intellectual Disabilities in South Korea


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement
Body Composition
2.3. Health-Related Physical Fitness
2.3.1. Muscular Strength
2.3.2. Muscular Endurance
2.3.3. Flexibility
2.4. Data Analysis
3. Results
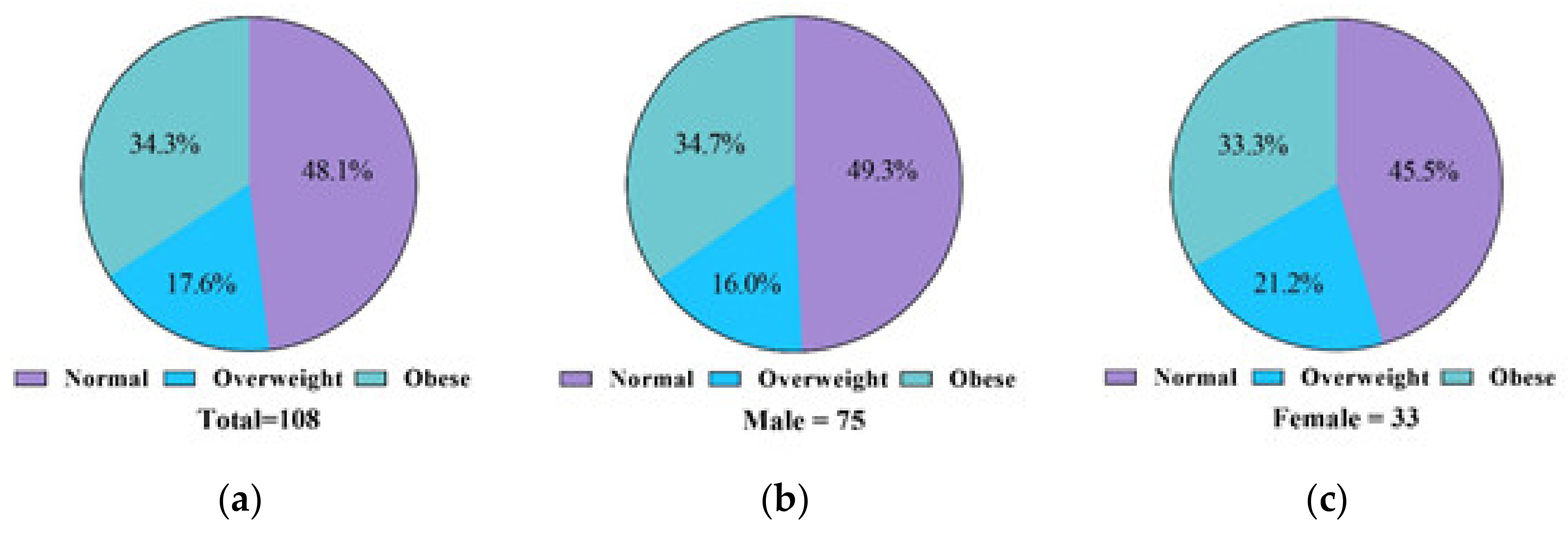
3.1. Analysis of Obesity Severity According to the Sex of People with Intellectual Disabilities
3.2. Analysis of Obesity Severity According to Age among People with Intellectual Disabilities
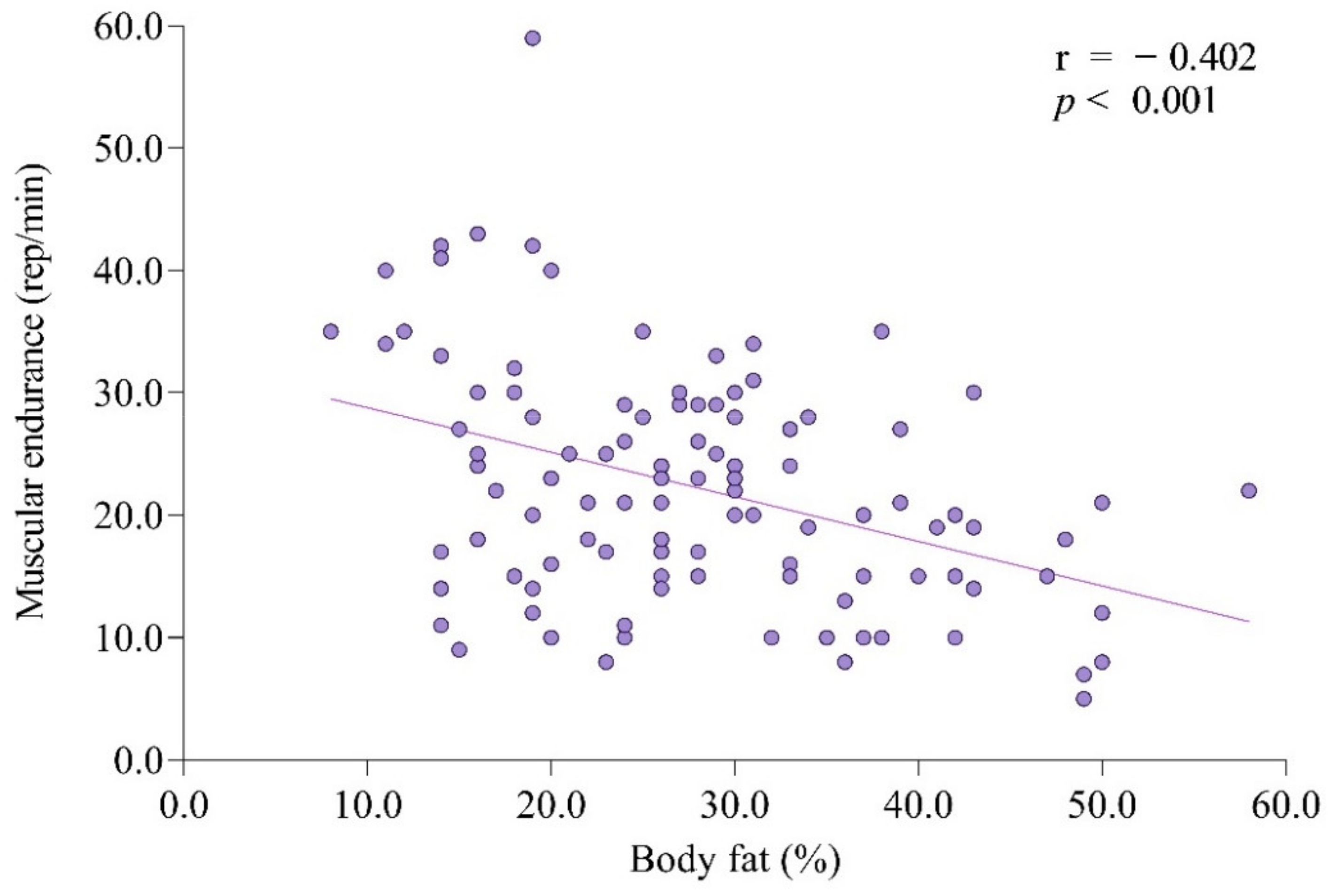
3.3. Correlation between Factors among People with Intellectual Disabilities
3.4. Factors Affecting the Body Fat Percentage of People with Intellectual Disabilities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; World Health Organization Technical Report Series; World Health Orhanization: Gneva, Switzerland, 2000; Volume 894, pp. i–xii, 1–253. [Google Scholar]
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Kopelman, P.G. Investigation of obesity. Clin. Endocrinol. 1994, 41, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Seo, M.H.; Lee, W.-Y.; Kim, S.S.; Kang, J.-H.; Kang, J.-H.; Kim, K.K.; Kim, B.-Y.; Kim, Y.-H.; Kim, W.-J.; Kim, E.M.; et al. 2018 Korean Society for the Study of Obesity Guideline for the Management of Obesity in Korea. Obes. Metab. Syndr. 2019, 28, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.B. The Effect of Obesity on health outcomes. Mol. Cell. Endocrinol. 2010, 316, 104–108. [Google Scholar] [CrossRef]
- Dong, B.; Wang, Z.; Wang, H.-J.; Ma, J. The association between resting heart rate and blood pressure among children and adolescents with different waist circumferences. Eur. J. Pediatr. 2015, 174, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, E.A.; daCosta DiBonaventura, M.; Burgess, S.M.; Hale, B.C. The costs of obesity in the workplace. J. Occup. Environ. Med. 2010, 52, 971–976. [Google Scholar] [CrossRef]
- Saner, C.; Simonetti, G.D.; Wühl, E.; Mullis, P.E.; Janner, M. Circadian and ultradian cardiovascular rhythmicity in obese children. Eur. J. Pediatr. 2016, 175, 1031–1038. [Google Scholar] [CrossRef]
- Wang, Y.; Beydoun, M.A.; Liang, L.; Caballero, B.; Kumanyika, S.K. Will All americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity 2008, 16, 2323–2330. [Google Scholar] [CrossRef] [PubMed]
- Bhaumik, S.; Watson, J.M.; Thorp, C.F.; Tyrer, F.; McGrother, C.W. Body mass index in adults with intellectual disability: Distribution, associations and service implications: A population-based prevalence study. J. Intellect. Disabil. Res. 2008, 52, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Krause, S.; Ware, R.; McPherson, L.; Lennox, N.; O’Callaghan, M. Obesity in adolescents with intellectual disability: Prevalence and associated characteristics. Obes. Res. Clin. Pract. 2016, 10, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Segal, M.; Eliasziw, M.; Phillips, S.; Bandini, L.; Curtin, C.; Kral, T.V.E.; Sherwood, N.E.; Sikich, L.; Stanish, H.; Must, A. Intellectual disability is associated with increased risk for obesity in a nationally representative sample of U.S. children. Disabil. Health J. 2016, 9, 392–398. [Google Scholar] [CrossRef]
- De Winter, C.F.; Bastiaanse, L.P.; Hilgenkamp, T.I.M.; Evenhuis, H.M.; Echteld, M.A. Overweight and obesity in older people with intellectual disability. Res. Dev. Disabil. 2012, 33, 398–405. [Google Scholar] [CrossRef]
- Yamaki, K. Body Weight Status among adults with intellectual disability in the community. Ment. Retard. 2005, 43, 1–10. [Google Scholar] [CrossRef]
- Maulik, P.K.; Mascarenhas, M.N.; Mathers, C.D.; Dua, T.; Saxena, S. Prevalence of intellectual disability: A meta-analysis of population-based studies. Res. Dev. Disabil. 2011, 32, 419–436. [Google Scholar] [CrossRef]
- Korea Ministry of Health and Welfare. Disabled Person Present Condition. Available online: https://www.index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd=2768 (accessed on 15 April 2021).
- Qi, L.; Cho, Y.A. Gene-environment interaction and obesity. Nutr. Rev. 2008, 66, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; Anderson, L.H.; Crain, A.L.; Martinson, B.C.; O’Connor, P.J.; Sherwood, N.E.; Whitebird, R.R. Meeting recommendations for multiple healthy lifestyle factors. prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am. J. Prev. Med. 2004, 27, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Salaun, L.; Berthouze-Aranda, S.E. Physical fitness and fatness in adolescents with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2012, 25, 231–239. [Google Scholar] [CrossRef]
- Oviedo, G.R.; Travier, N.; Guerra-Balic, M. Sedentary and physical activity patterns in adults with intellectual disability. Int. J. Environ. Res. Public Health 2017, 14, 1027. [Google Scholar] [CrossRef] [PubMed]
- Kolset, S.O.; Nordstrøm, M.; Hope, S.; Retterstøl, K.; Iversen, P.O. Securing rights and nutritional health for persons with intellectual disabilities—A pressing challenge. Food Nutr. Res. 2018, 62. [Google Scholar] [CrossRef]
- Draheim, C.C.; Williams, D.P.; McCubbin, J.A. Prevalence of physical inactivity and recommended physical activity in community-based adults with mental retardation. Ment. Retard. 2002, 40, 436–444. [Google Scholar] [CrossRef]
- He, Q.; Wong, T.; Du, L.; Jiang, Z.; Yu, T.I.; Qiu, H.; Gao, Y.; Liu, W.; Wu, J. Physical activity, cardiorespiratory fitness, and obesity among Chinese children. Prev. Med. 2011, 52, 109–113. [Google Scholar] [CrossRef]
- Aires, L.; Silva, P.; Silva, G.; Santos, M.P.; Ribeiro, J.C.; Mota, J. Intensity of physical activity, cardiorespiratory fitness, and body mass index in youth. J. Phys. Act. Health 2010, 7, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Fiori, F.; Bravo, G.; Parpinel, M.; Messina, G.; Malavolta, R.; Lazzer, S. Relationship between body mass index and physical fitness in Italian prepubertal schoolchildren. PLoS ONE 2020, 15, e0233362. [Google Scholar] [CrossRef]
- Fogelholm, M.; Stigman, S.; Huisman, T.; Metsämuuronen, J. Physical fitness in adolescents with normal weight and overweight. Scand. J. Med. Sci. Sports 2008, 18, 162–170. [Google Scholar] [CrossRef]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various inbody body composition analyzers as compared to dual-energy X-ray absorptiometry in healthy men and women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between dual-energy X-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef] [PubMed]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand grip strength: Age and gender stratified normative data in a population-based study. BMC Res. Notes 2011, 4, 127. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Bohannon, R.W.; Li, X.; Sindhu, B.; Kapellusch, J. Hand-grip strength: Normative reference values and equations for individuals 18 to 85 years of age residing in the United States. J. Orthop. Sports Phys. Ther. 2018, 48, 685–693. [Google Scholar] [CrossRef]
- Kong, Z.; Sze, T.M.; Yu, J.J.; Loprinzi, P.D.; Xiao, T.; Yeung, A.S.; Li, C.; Zhang, H.; Zou, L. Tai Chi as an alternative exercise to improve physical fitness for children and adolescents with intellectual disability. Int. J. Environ. Res. Public Health 2019, 16, 1152. [Google Scholar] [CrossRef] [PubMed]
- Milanovic, I.; Radisavljevic-Janic, S.; Zivkovic, M.Z.; Mirkov, D.M. Health-related physical fitness levels and prevalence of obesity in Serbian elementary schoolchildren. Nutr. Hosp. 2019, 36, 253–260. [Google Scholar] [CrossRef]
- Alcántara-Cordero, F.J.; Gómez-Píriz, P.T.; Sánchez-López, A.M.; Cabeza-Ruiz, R. Feasibility and reliability of a physical fitness tests battery for adults with intellectual disabilities: The SAMU DIS-FIT battery. Disabil. Health J. 2020, 13, 100886. [Google Scholar] [CrossRef]
- Daniel, M.V.; Rafael, M.M.; Jesús, V. Criterion-related validity of sit-and-reach tests for estimating hamstring and lumbar extensibility: A meta-analysis. J. Sports Sci. Med. 2014, 13, 1–14. [Google Scholar]
- Hsieh, K.; Rimmer, J.H.; Heller, T. Obesity and associated factors in adults with intellectual disability. J. Intellect. Disabil. Res. 2014, 58, 851–863. [Google Scholar] [CrossRef]
- Bennett, E.A.; Kolko, R.P.; Chia, L.; Elliott, J.P.; Kalarchian, M.A. Treatment of obesity among youth with intellectual and developmental disabilities: An emerging role for telenursing. West J. Nurs. Res. 2017, 39, 1008–1027. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.L.; Schieve, L.A.; Visser, S.; Boulet, S.; Sharma, A.J.; Kogan, M.D.; Boyle, C.A.; Yeargin-Allsopp, M. Prevalence and impact of unhealthy weight in a national sample of US adolescents with autism and other learning and behavioral disabilities. Matern. Child Health J. 2014, 18, 1964–1975. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.Y.; Kim, S.E.; Houtrow, A.J.; Newacheck, P.W. Prevalence of obesity among children with chronic conditions. Obesity 2010, 18, 210–213. [Google Scholar] [CrossRef]
- Westrop, S.C.; Melville, C.A.; Muirhead, F.; McGarty, A.M. Gender differences in physical activity and sedentary behaviour in adults with intellectual disabilities: A systematic review and meta-analysis. J. Appl. Res. Intellect. Disabil. 2019, 32, 1359–1374. [Google Scholar] [CrossRef]
- Gonzalez-Suarez, C.B.; Grimmer-Somers, K. The association of physical activity and physical fitness with pre-adolescent obesity: An observational study in Metromanila, Philippines. J. Phys. Act. Health 2011, 8, 804–810. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Hurtig-Wennlöf, A.; Vicente-Rodríguez, G.; Rizzo, N.S.; Castillo, M.J.; Sjöström, M. Cardiovascular fitness modifies the associations between physical activity and abdominal adiposity in children and adolescents: The European Youth Heart Study. Br. J. Sports Med. 2010, 44, 256–262. [Google Scholar] [CrossRef]
- Lee, Y.G.; Oh, S.H. The Relationship of obesity to health-related physical fitness of secondary school boys and girls a study on. Korean J. Meas. Eval. Phys. Educ. Sports Sci. 2012, 14, 29–43. [Google Scholar] [CrossRef]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; LWW: Philadelphia, PA, USA, 2017; ISBN 978-1-4963-3907-2. [Google Scholar]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Fernhall, B.; Mendonca, G.V.; Baynard, T. reduced work capacity in individuals with down syndrome: A consequence of autonomic dysfunction? Exerc. Sport Sci. Rev. 2013, 41, 138–147. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; Brazo-Sayavera, J.; Yuste Lucas, J.L.; Renato Cavichiolli, F. Weight status is related to health-related physical fitness and physical activity but not to sedentary behaviour in children. Int. J. Environ. Res. Public Health 2020, 17, 4518. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, N.; Miyachi, M.; Tabata, I.; Sakano, N.; Hirao, T.; Numata, T. Relationship between muscle strength and anthropometric, body composition parameters in Japanese adolescents. Health 2012, 4, 16989. [Google Scholar] [CrossRef]
- Siff, M. Biomechanical foundations of strength and power training. In Biomechanics in Sport; Zatsiorsky, V., Ed.; Blackwell Scientific Ltd.: London, UK, 2001; pp. 103–139. [Google Scholar]
- Stone, M.H. Position statement: Explosive exercises and training. Natl. Strength Cond. Assoc. J. 1993, 15, 7–15. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Stone, M.H. The importance of muscular strength in athletic performance. Sports Med. 2016, 46, 1419–1449. [Google Scholar] [CrossRef]
- Shields, N.; Taylor, N.F.; Fernhall, B. A study protocol of a randomised controlled trial to investigate if a community based strength training programme improves work task performance in young adults with Down syndrome. BMC Pediatr. 2010, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Yao, M.; Kang, M.; Duan, G. Improving Physical Fitness of Children with Intellectual and Developmental Disabilities through an Adapted Rhythmic Gymnastics Program in China. BioMed Res. Int. 2020, 2345607. [Google Scholar] [CrossRef]
- Benetti, F.A.; Bacha, I.L.; Junior, A.B.G.; Greve, J.M.D. Analyses of balance and flexibility of obese patients undergoing bariatric surgery. Clinics 2016, 71, 78–81. [Google Scholar] [CrossRef]
- Oliveira, A.; Monteiro, Â.; Jácome, C.; Afreixo, V.; Marques, A. Effects of group sports on health-related physical fitness of overweight youth: A systematic review and meta-analysis. Scand. J. Med. Sci. Sports 2017, 27, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Shore, S.M.; Sachs, M.L.; DuCette, J.P.; Libonati, J.R. Step-count promotion through a school-based intervention. Clin. Nurs. Res. 2014, 23, 402–420. [Google Scholar] [CrossRef] [PubMed]
- Nahas, M.V. Atividade Física, Saúde e Qualidade de Vida: Conceitos e Sugestões para um Estilo de Vida Ativo, 3rd ed.; Midiograf: Londrina, Brazil, 2003. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Total (N = 108) | Male (n = 75) | Female (n = 33) |
|---|---|---|---|
| Age | 24.40 ± 8.45 | 24.99 ± 7.92 | 23.06 ± 9.56 |
| Height (cm) | 163.97 ± 9.48 | 166.88 ± 8.66 | 157.34 ± 7.87 |
| Weight (kg) | 63.67 ± 14.61 | 64.38 ± 14.71 | 62.06 ± 14.48 |
| BMI (kg/m2) | 23.62 ± 4.97 | 22.98 ± 4.43 | 25.08 ± 5.82 |
| % Body fat (%) | 27.94 ± 10.46 | 24.24 ± 8.41 | 36.62 ± 9.71 |
| Variables | Age 10–19 (n = 31) | Age 20–29 (n = 56) | Age 30–39 (n = 13) | Age 40–49 (n = 8) | x2 |
|---|---|---|---|---|---|
| Normal | 21 (67.7%) | 25 (44.6%) | 5 (38.5%) | 1 (12.5%) | 11.829 (p = 0.066) |
| Overweight | 4 (12.9%) | 11 (19.6%) | 3 (23.1%) | 1 (12.5%) | |
| Obese | 6 (19.4%) | 20 (35.7%) | 5 (38.5%) | 6 (75.0%) |
| Variables | n | Mean | SD | SE | Min | Max | Range | 95%CI |
|---|---|---|---|---|---|---|---|---|
| Age | 108 | 24.38 | 8.49 | 0.82 | 12.00 | 46.00 | 34.00 | (22.76; 26.01) |
| Height (cm) | 108 | 164.13 | 9.36 | 0.91 | 135.50 | 187.20 | 51.70 | (162.34; 165.93) |
| Weight (kg) | 108 | 63.59 | 14.66 | 1.42 | 33.20 | 108.90 | 75.70 | (60.78; 66.40) |
| BMI (kg/m2) | 108 | 23.53 | 4.89 | 0.47 | 15.22 | 39.33 | 24.11 | (22.59; 24.46) |
| % Body fat (%) | 108 | 27.94 | 4.89 | 1.01 | 7.60 | 58.30 | 50.70 | (22.59; 24.46) |
| Sit-up | 108 | 22.22 | 9.52 | 0.92 | 5.00 | 59.00 | 54.00 | (20.40; 24.05) |
| Sit and reach | 108 | 0.21 | 11.94 | 1.15 | −30.00 | 23.20 | 53.20 | (−2.08; 2.50) |
| Grip strength | 108 | 20.66 | 8.73 | 0.84 | 6.40 | 43.30 | 36.90 | (18.99; 22.33) |
| Variables | Age | Height | Weight | BMI | Body Fat Percentage | Sit-Up | Sit and Reach | Grip Strength |
|---|---|---|---|---|---|---|---|---|
| Age | 1 | |||||||
| Height | 0.160 | 1 | ||||||
| Weight | 0.309 ** | 0.459 ** | 1 | |||||
| BMI | 0.275 ** | −0.021 | 0.873 ** | 1 | ||||
| Body fat percentage | 0.162 | −0.263 ** | 0.560 ** | 0.789 ** | 1 | |||
| Sit-up | −0.282 ** | 0.045 | −0.222 * | −0.306 ** | −0.402 ** | 1 | ||
| Sit and reach | −0.014 | −0.132 | −0.162 | −0.110 | −0.120 | 0.285 ** | 1 | |
| Grip strength | 0.270 ** | 0.386 ** | 0.235 * | 0.028 | −0.173 | 0.318 ** | 0.312 ** | 1 |
| Variables | Non-Standardized Coefficients | Standardized Coefficients | t | p | VIF | |
|---|---|---|---|---|---|---|
| B | SE | β | ||||
| Constant | 116.28 | 9.833 | 11.825 | 0.000 | ||
| Height | −0.735 | 0.066 | −0.658 | −11.078 | 0.000 | 1.319 |
| Weight | 0.591 | 0.043 | 0.828 | 13.616 | 0.000 | 1.383 |
| Sit-up | −0.239 | 0.059 | −0.218 | −4.075 | 0.000 | 1.067 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, G.; Chun, B. Analysis of the Relationship between Obesity Factors and Health-Related Physical Fitness Factors among People with Intellectual Disabilities in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 6533. https://doi.org/10.3390/ijerph18126533
Jeong G, Chun B. Analysis of the Relationship between Obesity Factors and Health-Related Physical Fitness Factors among People with Intellectual Disabilities in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(12):6533. https://doi.org/10.3390/ijerph18126533
Chicago/Turabian StyleJeong, Guyeol, and Buongo Chun. 2021. "Analysis of the Relationship between Obesity Factors and Health-Related Physical Fitness Factors among People with Intellectual Disabilities in South Korea" International Journal of Environmental Research and Public Health 18, no. 12: 6533. https://doi.org/10.3390/ijerph18126533
APA StyleJeong, G., & Chun, B. (2021). Analysis of the Relationship between Obesity Factors and Health-Related Physical Fitness Factors among People with Intellectual Disabilities in South Korea. International Journal of Environmental Research and Public Health, 18(12), 6533. https://doi.org/10.3390/ijerph18126533