
Relationship between Posture and Non-Contact Lower Limb Injury in Young Male Amateur Football Players: A Prospective Cohort Study



 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Posture Data Collection
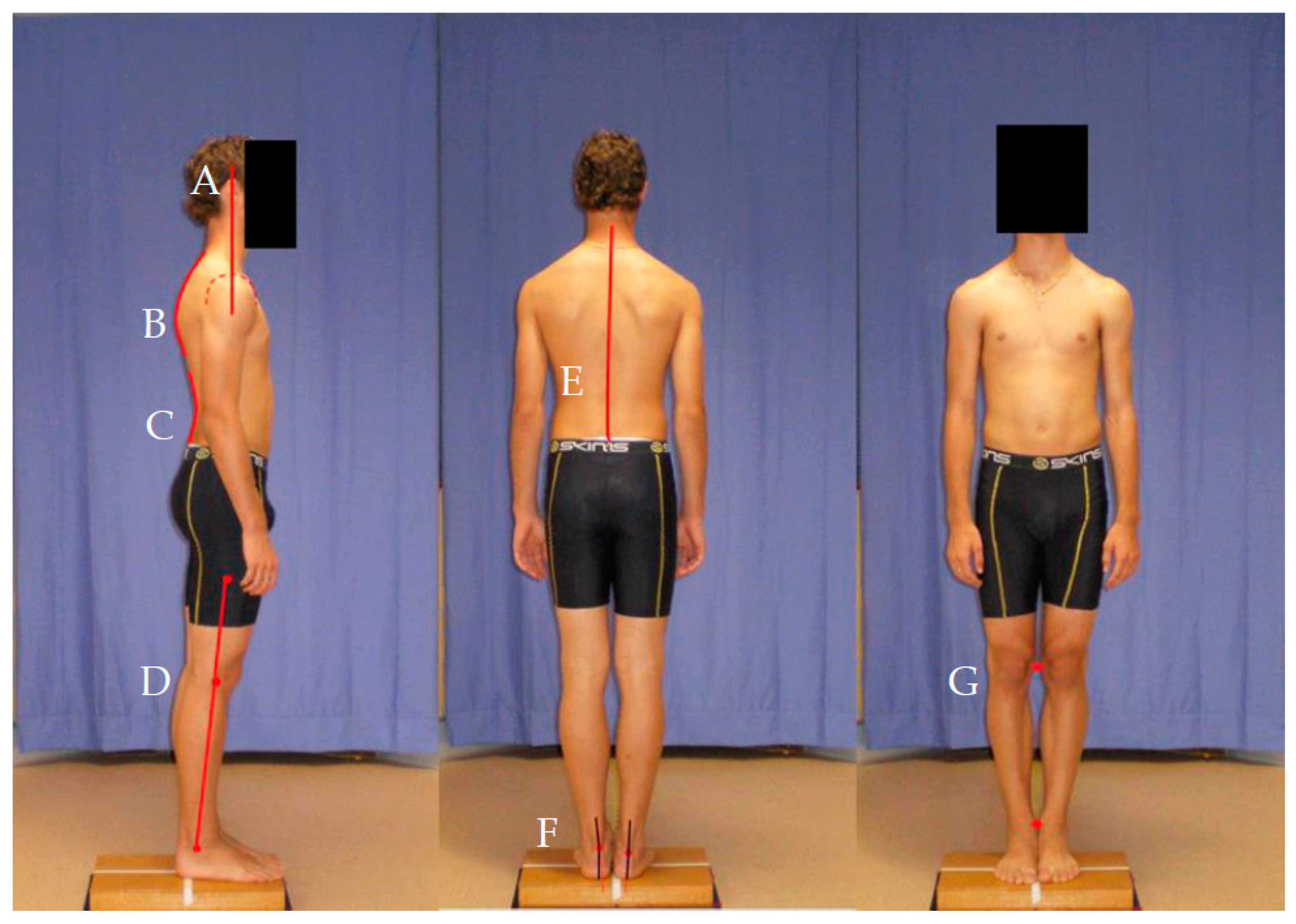
2.2. Assessment of Posture
2.3. Injury and Exposure Monitoring
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sadigursky, D.; Braid, J.A.; De Lira, D.N.; Machado, B.A.; Carneiro, R.J.; Colavolpe, P.O. The FIFA 11+ injury prevention program for soccer players: A systematic review. BMC Sports Sci. Med. Rehabil. 2017, 9, 1–8. [Google Scholar] [CrossRef]
- Stubbe, J.H.; Schmikli, S.L.; van de Port, I.G.; Backx, F.J. Differences in injury risk and characteristics between Dutch amateur and professional soccer players. J. Sci. Med. Sport 2015, 18, 145–149. [Google Scholar]
- Stubbe, J.H.; van Beijsterveldt, A.M.; van der Knaap, S.; Stege, J.; Verhagen, E.A.; Van Mechelen, W.; Backx, F.J. Injuries in professional male soccer players in the Netherlands: A prospective cohort study. J. Athl. Train. 2015, 50, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Grimm, N.L.; Jacobs Jr, J.C.; Kim, J.; Amendola, A.; Shea, K.G. Ankle injury prevention programs for soccer athletes are protective—A level-I meta-analysis. J. Bone Jt. Surg. 2016, 98, 1436–1443. [Google Scholar] [CrossRef]
- Al Attar, W.S.; Soomro, N.; Pappas, E.; Sinclair, P.J.; Sanders, R.H. Adding a post-training FIFA 11+ exercise program to the pre-training FIFA 11+ injury prevention program reduces injury rates among male amateur soccer players: A cluster-randomised trial. J. Physiother 2017, 63, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Eirale, C.; Gillogly, S.; Singh, G.; Chamari, K. Injury and illness epidemiology in soccer—Effects of global geographical differences—A call for standardized and consistent research studies. Biol. Sport 2017, 34, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Svensson, K.; Eckerman, M.; Alricsson, M.; Magounakis, T.; Werner, S. Muscle injuries of the dominant or non-dominant leg in male football players at elite level. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 933–937. [Google Scholar] [CrossRef]
- Moore, O.; Cloke, D.J.; Avery, P.J.; Beasley, I.; Deehan, D.J. English Premiership Academy knee injuries: Lessons from a 5 year study. J. Sports Sci. 2011, 29, 1535–1544. [Google Scholar] [CrossRef] [PubMed]
- Kofotolis, N.D.; Kellis, E.; Vlachopoulos, S.P. Ankle sprain injuries and risk factors in amateur soccer players during a 2-year period. Am. J. Sports Med. 2007, 35, 458–466. [Google Scholar] [CrossRef]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of injury incidences in male professional adult and elite youth soccer players: A systematic review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, T.D.; Freund, K.G.; Madsen, F.; Sandvej, K. Injuries in high-skilled and low-skilled soccer: A prospective study. Br. J. Sports Med. 1991, 25, 151–153. [Google Scholar] [CrossRef]
- Arnason, A.; Sigurdsson, S.B.; Gudmundsson, A.; Holme, I.; Engebretsen, L.; Bahr, R. Physical fitness, injuries, and team performance in soccer. Med. Sci. Sports Exerc. 2004, 36, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Dvorak, J. Incidence of football injuries and complaints in different age groups and skill-level groups. Am. J. Sports Med. 2000, 28, S51–S57. [Google Scholar] [CrossRef] [PubMed]
- McNoe, B.M.; Chalmers, D.J. Injury in Community-Level Soccer. Am. J. Sports Med. 2010, 38, 2542–2551. [Google Scholar] [CrossRef]
- Gallo, P.O.; Argemi, R.; Batista, J.; Garcia, L.; Liotta, G. The epidemiology of injuries in a professional soccer team in Argentina. Int. Sportmed. J. 2006, 7, 255–265. [Google Scholar]
- Agel, J.; Evans, T.A.; Dick, R.; Putukian, M.; Marshall, S.W. Descriptive epidemiology of collegiate men’s soccer Injuries: National Collegiate Athletic Association injury surveillance system, 1988–1989 through 2002–2003. J. Athl. Train. 2007, 42, 270–277. [Google Scholar]
- Hawkins, R.D.; Fuller, C.W. A prospective epidemiological study of injuries in four English professional football clubs. Br. J. Sports Med. 1999, 33, 196–203. [Google Scholar] [CrossRef]
- Engebretsen, A.H.; Myklebust, G.; Holme, I.; Engebretsen, L.; Bahr, R. Intrinsic risk factors for acute ankle injuries among male soccer players: A prospective cohort study. Scand J. Med. Sci. Sports 2010, 20, 403–410. [Google Scholar] [CrossRef] [PubMed]
- McCunn, R.; aus der Fünten, K.; Whalan, M.; Sampson, J.A.; Meyer, T. Soccer injury movement screen (SIMS) composite score is not associated with injury among semiprofessional soccer players. J. Orthop. Sports Phys. Ther. 2018, 48, 630–636. [Google Scholar] [CrossRef]
- Chromik, K.; Burdukiewicz, A.; Pietraszewska, J.; Stachoń, A.; Wolański, P.; Goliński, D. Characteristics of anteroposterior curvatures of the spine in soccer and futsal players. Hum. Mov. Sci. 2017, 18, 49–54. [Google Scholar] [CrossRef]
- Ribeiro, C.Z.; Akashi, P.M.; Sacco, I.D.; Pedrinelli, A. Relationship between postural changes and injures of the locomotor system in indoor athletes. Rev. Bras. Med. Esporte 2003, 9, 98–103. [Google Scholar] [CrossRef]
- Hennessy, L.; Watson, A.W.S. Flexibility and posture assessment in relation to hamtring injury. Br. J. Sports Med. 1993, 27, 243–246. [Google Scholar] [CrossRef]
- Watson, A. Sports injuries in footballers related to defects of posture and body mechanics. J. Sports Med. Phys. Fitness 1995, 35, 289–294. [Google Scholar]
- Bugg, W.G.; Lewis, M.; Juette, A.; Cahir, J.G.; Toms, A.P. Lumbar lordosis and pars interarticularis fractures: A case-control study. Skeletal Radiol. 2012, 41, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, C.J.; Norton, B.J.; Callaghan, J.P.; Hwang, C.T.; Van Dillen, L.R. Is lumbar lordosis related to low back pain development during prolonged standing? Man. Ther. 2015, 20, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, R.O.; Buist, I.; Parner, E.T.; Nohr, E.A.; Sørensen, H.; Lind, M.; Rasmussen, S. Foot pronation is not associated with increased injury risk in novice runner wearing a neutral shoe: A 1-year prospective cohort study. Br. J. Sports Med. 2014, 48, 440–447. [Google Scholar] [CrossRef]
- Ramskov, D.; Jensen, M.L.; Obling, K.; Nielsen, R.O.; Parner, E.T.; Rasmussen, S. No association between q-angle and foot posture with running-related injuries: A 10 week prospective follow-up study. Int. J. Sports Phys. Ther. 2013, 8, 407–415. [Google Scholar] [PubMed]
- Halabchi, F.; Angoorani, H.; Mirshahi, M.; Shahi, M.H.; Mansournia, M.A. The prevalence of selected intrinsic factors for ankle sprain among eite football and basketabll players. Asian J. Sports Med. 2016, 7, e35287. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Mac Donncha, C. A reliable technique for the assessment of posture: Assessment criteria for aspects of posture. J. Sports Med. Phys. Fitness 2000, 40, 260–270. [Google Scholar]
- Jackson, R.P.; Kanemura, T.; Kawakami, N.; Hales, C. Lumbopelvic lordosis and pelvic balance on repeated standing lateral radiographs of adult volunteers and untreated patients with constant low back pain. J. Spine 2000, 25, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Berglund, L.; Aasa, B.; Michaelson, P.; Aasa, U. Sagittal lumbopelvic alignment in patients with low back pain and the effects of a high-load lifting exercise and individualized low-load motor control exercises—A randomized controlled trial. J. Spine 2017, 18, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Xiaohua, M.H.; KyeongAh, J.; HanSuk, H.; JooHyun, K.H.; SungEun, K. A comparison of the validity and reliability between a digital radiographic imaging system and manual method in measuring the Cobb angle. Scoliosis Spinal Disord 2013, 8, 1–2. [Google Scholar] [CrossRef]
- Katzman, W.B.; Parimi, N.; Gladin, A.; Poltavskiy, E.A.; Schafer, A.L.; Long, R.K.; Fan, B.; Wong, S.S.; Lane, N.E. Sex differences in response to targeted kyphosis specific exercise and posture training in community-dwelling older adults: A randomized controlled trial. BMC Musculoskelet Disord 2017, 18, 509. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.C.C.; Romeiro, C.A.P.; Patrizzi, L.J. Evaluation of thoracic kyphosis in older adult women with osteoporosis by means of computerized biophotogrammetry. Braz. J. Phys. Ther. 2009, 13, 205–209. [Google Scholar] [CrossRef]
- Van Blommestein, A.S.; MaCrae, S.; Lewis, J.S.; Morrissey, M.C. Reliability of measuring thoracic kyphosis angle, lumbar lordosis angle and straight leg raise with an inclinometer. Spine J. 2012, 4, 10–15. [Google Scholar] [CrossRef]
- D’Amico, M.; Kinel, E.; Roncoletta, P. Normative 3D opto-electronic stereo-photogrammetric posture and spine morphology data in young healthy adult population. PLoS ONE 2017, 12, e0179619. [Google Scholar] [CrossRef]
- Koo, T.K.; Kwok, W.E. A non-ionizing technique for three-dimensional measurement of the lumbar spine. J. Biomech. 2016, 49, 4073–4079. [Google Scholar] [CrossRef]
- Trimble, M.H.; Bishop, M.D.; Buckley, B.D.; Fields, L.C.; Rozea, G.D. The relationship between clinical measurements of lower extremity posture and tibial translation. Clin. Biomech. 2002, 17, 286–290. [Google Scholar] [CrossRef]
- Marfell-Jones, M. International Standards for Anthropometric Assessment, Rev. ed.; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2006. [Google Scholar]
- Neter, J.; Kutner, M.H.; Nachtsheim, C.J.; Wasserman, W. Applied Linear Regression Models; Irwin: Chicago, IL, USA, 1996. [Google Scholar]
- Lotfian, S.; Moghadam, N.; Hassnamirzaie, B.; Soltani, S.K. Are lower extremity injuries related to spinal form abnormalities in professional football players? A prospective cohort study. Asian J. Sports Med. 2017, 8, 9. [Google Scholar] [CrossRef]
- de Loës, M. Exposure data. Why are they needed? Sports Med. (Auckland NZ) 1997, 24, 172–175. [Google Scholar] [CrossRef]
- Rahnama, N.; Reilly, T.; Lees, A. Injury risk associated with playing actions during competitive soccer. Br. J. Sports Med. 2002, 36, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Janik, T.J.; Holland, B. Reliability of Centroid, Cobb, and Harrison posterior tangent methods: Which to choose for analysis of thoracic kyphosis. Spine 2001, 26, e227–e234. [Google Scholar] [CrossRef] [PubMed]
- Fortin, C.; Van Schaik, P.; Aubin-Fournier, J.F.; Bettany-Saltikov, J.; Bernard, J.C.; Feldman, D.E. The acceptance of the clinical photographic posture assessment tool (CPPAT). BMC Musculoskelet Disord 2018, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | All Players (n = 263) | Previous Injury | In-Season Non-Contact Injury |
|---|---|---|---|
| Age (y), mean (SD) | 18.3 (3.3) | 17.8 (3.1) | 17.8 (2.5) |
| Height (cm), mean (SD) | 176.9 (5.9) | 175.9 (5.7) | 175.8 (6.8) |
| Mass (kg), mean (SD) | 70.1 (10.2) | 68.9 (9.7) | 69.3 (10.2) |
| BMI (kg/m2), mean (SD) | 22.3 (2.6) | 22.2 (2.4) | 22.4 (2.8) |
| Exposure (h), number (%) Low (0–122) | 37 (14.1) | 12 (15.0) | 2 (8.3) |
| Medium (123–166) | 163 (62.0) | 52 (65.0) | 16 (66.7) |
| High (>166) | 63 (24.0) | 16 (20.0) | 6 (25.0) |
| Competition Level (category), number (%) Low | 179 (68.1) | 56 (70.0) | 16 (66.7) |
| High | 84 (31.9) | 24 (30.0) | 8 (33.3) |
| Previous Injury (category), number (%) Any | 80 (30.4) * | 80 (100) † | 11 (13.8) † |
| Ankle | 31 (11.8) | 31 (38.8) | 4 (5.0) |
| Knee | 19 (7.2) | 19 (23.8) | 3 (3.8) |
| Hamstring | 13 (4.9) | 13 (16.3) | 1 (1.3) |
| Quadriceps | 9 (3.4) | 9 (11.3) | 2 (2.5) |
| Calf | 11 (4.2) | 11 (13.8) | 1 (1.3) |
| Groin | 10 (3.8) | 10 (12.5) | 2 (2.5) |
| In-Season Injury (category), number (%)Any | 24 (9.1) * | 11 (47.8) † | 24 (100) † |
| Any ankle | 10 (3.8) | 1 (4.3) | 10 (41.7) |
| Any knee | 7 (2.7) | 3 (13.0) | 7 (29.2) |
| Any hamstring | 3 (1.1) | 4 (17.4) | 3 (12.5) |
| Any quadriceps | 4 (1.5) | 0 (0) | 4 (16.7) |
| Any calf | 3 (1.1) | 3 (13.0) | 3 (12.5) |
| Any groin | 3 (1.1) | 1 (4.3) | 3 (12.5) |
| Postural Aspect | Intra-Rater N/20 Agreed on (%) | Inter-Rater N/20 Agreed on (%) |
|---|---|---|
| Left rearfoot | 17 (85) | 17 (85) |
| Right rearfoot | 16 (80) | 15 (75) |
| Knee interspace | 19 (95) | 17 (85) |
| Lateral knee posture | 18 (90) | 19 (95) |
| Lumbar lordosis | 19 (95) | 17 (85) |
| Thoracic kyphosis | 16 (80) | 16 (80) |
| Scoliosis C | 20 (100) | 19 (95) |
| Scoliosis S | 20 (100) | 20 (100) |
| Forward head | 20 (100) | 18 (90) |
| Lower Limb in-Season Injury | Knee Interspace | Lateral Knee | Lordosis | Kyphosis | Scoliosis C | Scoliosis S | Forward Head | Previous Injury |
|---|---|---|---|---|---|---|---|---|
| Ankle sprain | X | Knee strain | ||||||
| Ankle sprain | X (varus) | X | ||||||
| Ankle sprain | X | |||||||
| Ankle sprain | X | Hamstring strain | ||||||
| Ankle sprain | ||||||||
| Ankle sprain | X (extension) | X | X | Ankle sprain | ||||
| Ankle sprain | X | X | Ankle sprain, calf strain | |||||
| Ankle sprain, hamstring strain | X (varus) | X | X | |||||
| Ankle sprain, hamstring strain | X (flexion) | X | ||||||
| Ankle sprain, knee sprain | X (varus) | X | X | |||||
| Knee sprain | X | X | Calf strain | |||||
| Knee sprain | X | X | X | Calf strain | ||||
| Knee sprain | X | |||||||
| Knee sprain | X | |||||||
| Knee sprain | X | Hamstring strain | ||||||
| Knee sprain, calf strain | X | X | ||||||
| Quad strain | X | Knee strain | ||||||
| Quad strain | X (varus) | X | X | |||||
| Quad strain | ||||||||
| Quad strain, groin strain | X (varus) | X | X | Hamstring strain, calf strain | ||||
| Groin strain | X | X | Groin strain | |||||
| Groin strain, calf strain | X | X | ||||||
| Hamstring strain | X | X | Hamstring strain | |||||
| Calf strain | X | Knee sprain |
| Variable | N in Categories N (%) | N Players Injured in Each Group N (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age (y) * | Not injured: 18.2 (3.1) Injured: 17.8 (3.1) | - | 0.96 (0.86–1.06) | 0.37 |
| Height (cm) * | Not injured: 177.0 (5.8) Injured: 175.9 (5.7) | - | 0.96 (0.92–1.01) | 0.13 |
| Mass (kg) * | Not injured: 70.0 (10.1) Injured: 68.9 (9.7) | - | 0.99 (0.96–1.02) | 0.46 |
| BMI (kg/m2) * | Not injured: 22.3 (2.7) Injured: 22.2 (2.4) | - | 1.0 (0.89–1.11) | 0.93 |
| Exposure | ||||
| Low (ref) 0–122 h | 37 (14.1) | 12 (32.4) | 1 | 0.72 |
| Medium 123–166 h | 163 (62.0) | 52 (31.9) | 1.46 (0.56–3.77) | 0.44 |
| High > 166 h | 63 (24.0) | 16 (25.4) | 1.08 (0.55–2.15) | 0.82 |
| Competition Level | 1.02 (0.57–1.85) | 0.76 | ||
| Low | 179 (68.1) | 56 (31.3) | ||
| High | 84 (31.9) | 24 (28.6) | ||
| Left rearfoot posture | 0.79 (0.20–3.14) | 0.74 | ||
| Deviated | 11 (4.2) | 3 (27.3) | ||
| Not deviated | 252 (95.8) | 77 (30.6) | ||
| Right rearfoot posture | 1.96 (0.71–5.43) | 0.20 | ||
| Deviated | 17 (6.5) | 8 (47.1) | ||
| Not deviated | 246 (93.5) | 72 (29.3) | ||
| Knee interspace | 0.85 (0.45–1.61) | 0.61 | ||
| Deviated | 61 (23.2) | 18 (29.5) | ||
| Not deviated | 202 (76.8) | 62 (30.7) | ||
| Lateral knee posture | 0.70 (0.28–1.75) | 0.44 | ||
| Deviated | 26 (9.9) | 7 (26.9) | ||
| Not deviated | 237 (90.1) | 73 (30.8) | ||
| Lordosis | 0.82 (0.47–1.42) | 0.48 | ||
| Deviated | 105 (39.9) | 31 (29.5) | ||
| Not deviated | 158 (60.1) | 49 (31.0) | ||
| Kyphosis | 1.41 (0.82–2.44) | 0.22 | ||
| Deviated | 139 (52.9) | 46 (33.1) | ||
| Not deviated | 124 (47.1) | 34 (27.4) | ||
| Scoliosis C | 0.76 (0.26–2.24) | 0.62 | ||
| Deviated | 17 (6.5) | 5 (29.4) | ||
| Not deviated | 246 (93.5) | 75 (30.5) | ||
| Forward head | 1.22 (0.70–2.14) | 0.49 | ||
| Deviated | 160 (60.8) | 51 (31.9) | ||
| Not deviated | 103 (39.2) | 29 (28.2) |
| Variable | N in Categories (%) | N Players Injured in Each Group (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age (y) * | Not injured: 18.3 (3.3) Injured: 17.8 (2.5) | - | 0.5 (0.81–1.12) | 0.56 |
| Height (cm) * | Not injured: 177.0 (5.8) Injured: 175.8 (6.8) | - | 0.97 (0.90–1.04) | 0.37 |
| Mass (kg) * | Not injured: 70.1 (10.2) Injured: 69.3 (10.2) | - | 0.99 (0.95–1.04) | 0.69 |
| BMI (kg/m2) * | Not injured: 22.3 (2.6) Injured: 22.4 (2.8) | - | 1.01 (0.85–1.18) | 0.96 |
| Exposure | 1 | 0.70 | ||
| Low (ref) 0–122 h | 37 (14.1) | 2 (5.4) | ||
| Medium 123–166 h | 163 (62.0) | 16 (9.8) | 0.54 (0.10–2.84) | 0.47 |
| High > 166 h | 63 (24.0) | 6 (9.5) | 1.03 (0.39–2.77) | 0.95 |
| Previous lower limb injury | 2.75 (1.10–6.83) | 0.03 | ||
| Injured | 80 (30.4) | 12 (15.0) | ||
| Not injured | 149 (56.7) | 9 (6.0) | ||
| Competition Level | 1.07 (0.44–2.62) | 0.88 | ||
| Low | 179 (68.1) | 16 (8.9) | ||
| High | 84 (31.9) | 8 (9.5) | ||
| Left rearfoot posture | _ | 1.0 | ||
| Deviated | 11 (4.2) | 0 (0) | ||
| Not deviated | 252 (95.8) | 24 (9.5) | ||
| Right rearfoot posture | _ | 1.0 | ||
| Deviated | 17 (6.5) | 0 (0) | ||
| Not deviated | 246 (93.5) | 24 (9.5) | ||
| Knee interspace | 0.86 (0.31–2.41) | 0.77 | ||
| Deviated | 61 (23.2) | 5 (8.2) | ||
| Not deviated | 202 (76.8) | 19 (9.4) | ||
| Lateral knee posture | 0.81 (0.18–3.68) | 0.79 | ||
| Deviated | 26 (9.9) | 2 (7.7) | ||
| Not deviated | 237 (90.1) | 22 (9.3) | ||
| Lordosis | 0.59 (0.24–1.48) | 0.26 | ||
| Deviated | 105 (39.9) | 7 (6.7) | ||
| Not deviated | 158 (60.1) | 17 (10.8) | ||
| Kyphosis | 0.41 (0.17–1.00) | 0.05 | ||
| Deviated | 139 (52.9) | 8 (5.8) | ||
| Not deviated | 124 (47.1) | 16 (12.9) | ||
| Scoliosis C | 0.61 (0.08–4.78) | 0.64 | ||
| Deviated | 17 (6.5) | 1 (5.9) | ||
| Not deviated | 246 (93.5) | 23 (9.3) | ||
| Forward head | 2.64 (0.95–7.31) | 0.06 | ||
| Deviated | 160 (60.8) | 19 (11.9) | ||
| Not deviated | 103 (39.2) | 5 (4.9) |
| Variable | N in Categories (%) | N Players Injured in Each Group (%) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Previous injury | 3.04 (1.20–7.68) | 0.02 | ||
| Injured | 80 (30.4) | 11 (13.8) | ||
| Not injured | 149 (56.7) | 9 (6.0) | ||
| Kyphosis | 0.38 (0.15–1.00) | 0.05 | ||
| Deviated | 139 (52.9) | 7 (5.0) | ||
| Not deviated | 124 (47.1) | 16 (12.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Snodgrass, S.J.; Ryan, K.E.; Miller, A.; James, D.; Callister, R. Relationship between Posture and Non-Contact Lower Limb Injury in Young Male Amateur Football Players: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 6424. https://doi.org/10.3390/ijerph18126424
Snodgrass SJ, Ryan KE, Miller A, James D, Callister R. Relationship between Posture and Non-Contact Lower Limb Injury in Young Male Amateur Football Players: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(12):6424. https://doi.org/10.3390/ijerph18126424
Chicago/Turabian StyleSnodgrass, Suzanne J., Kathleen E. Ryan, Andrew Miller, Daphne James, and Robin Callister. 2021. "Relationship between Posture and Non-Contact Lower Limb Injury in Young Male Amateur Football Players: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 12: 6424. https://doi.org/10.3390/ijerph18126424
APA StyleSnodgrass, S. J., Ryan, K. E., Miller, A., James, D., & Callister, R. (2021). Relationship between Posture and Non-Contact Lower Limb Injury in Young Male Amateur Football Players: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 18(12), 6424. https://doi.org/10.3390/ijerph18126424