
Oral Health: Global Research Performance under Changing Regional Health Burdens

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Methodological Platform
2.2. Search Source and Strategy
2.3. Data Processing, Analyses, and Visualization
3. Results
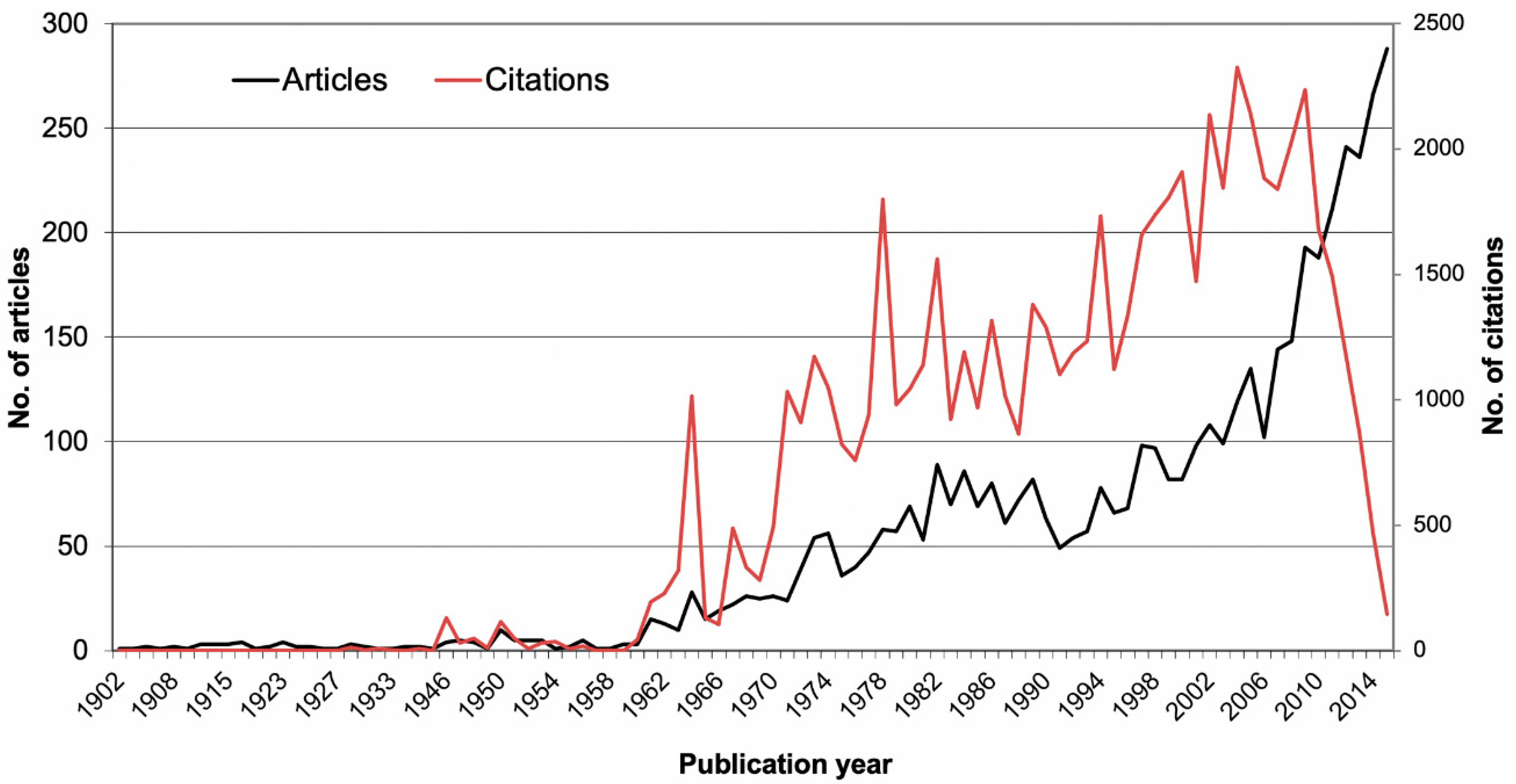
3.1. Chronological Analyses
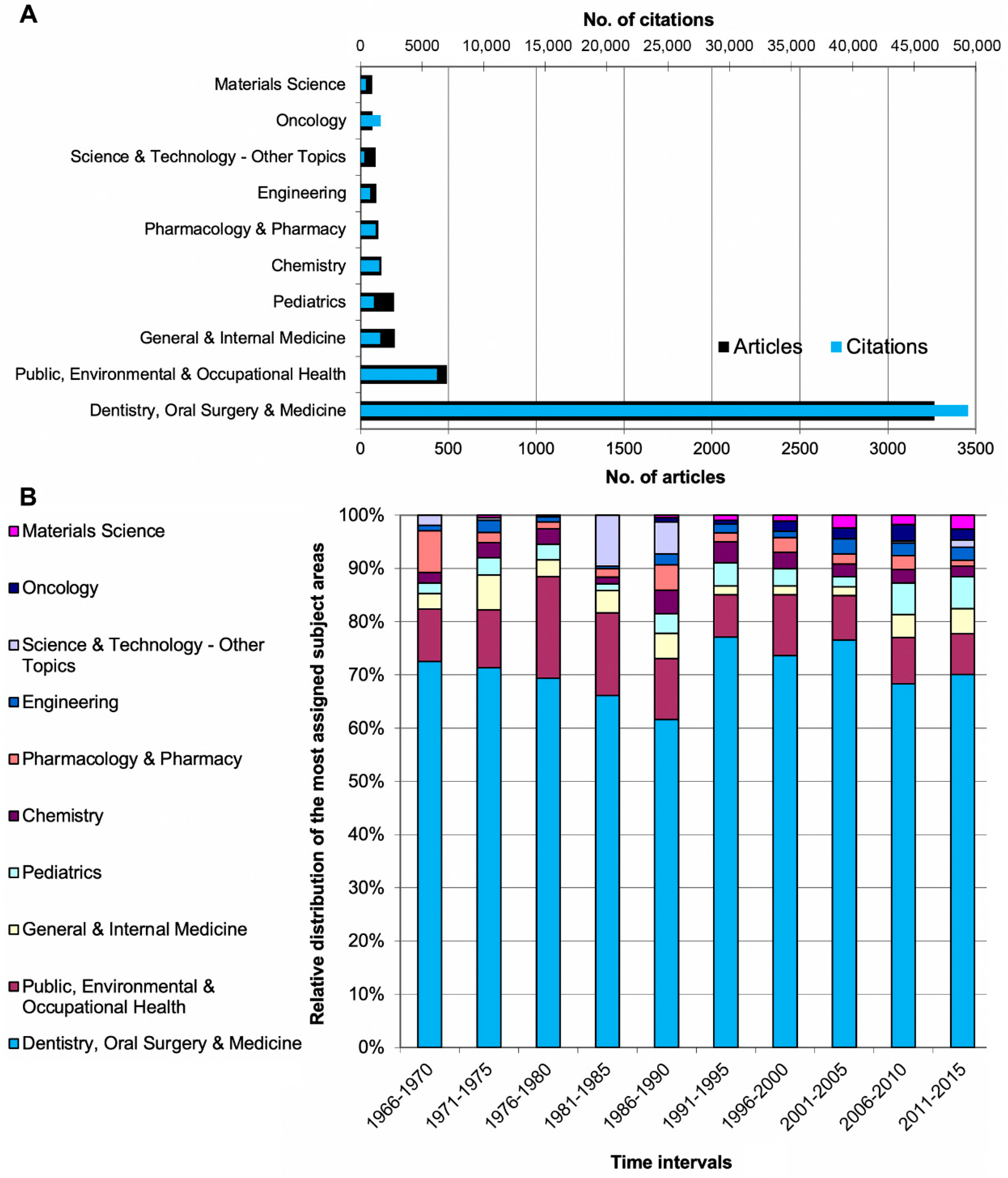
3.2. Geographical Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primers. 2017, 22, 17038. [Google Scholar] [CrossRef] [PubMed]
- Demke, R. Plaque inhibition: The science and application of oral rinses. Dent. Today 2012, 31, 96–101. [Google Scholar] [PubMed]
- Pitchika, V.; Jordan, R.; Micheelis, W.; Welk, A.; Kocher, T.; Holtfreter, B. Impact of Powered Toothbrush Use and Interdental Cleaning on Oral Health. J. Dent. Res. 2020, 20, 487–495. [Google Scholar]
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century-the approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–23. [Google Scholar] [CrossRef]
- Dye, B.A. The Global Burden of Oral Disease: Research and Public Health Significance. J. Dent. Res. 2017, 96, 361–363. [Google Scholar] [CrossRef]
- WHO. Oral Health. Fact Sheet No. 318. 2012. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 1 January 2020).
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of untreated caries: A systematic review and metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- GBD 2017 Oral Disorders Collaborators; Bernabe, E.; Marcenes, W.; Hernandez, C.R.; Bailey, J.; Abreu, L.G.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [PubMed]
- Kassebaum, N.J.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W. GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [PubMed]
- Jordan, R.A.; Bodechtel, C.; Hertrampf, K.; Hoffmann, T.; Kocher, T.; Nitschke, I.; Schiffner, U.; Stark, H.; Zimmer, S.; Micheelis, W. DMS V Surveillance Investigators’ Group. The Fifth German Oral Health Study (Fünfte Deutsche Mundgesundheitsstudie, DMS V)-rationale, design, and methods. BMC Oral Health 2014, 29, 161. [Google Scholar]
- Schwendicke, F.; Krois, J.; Kocher, T.; Hoffmann, T.; Micheelis, W.; Jordan, R.A. More teeth in more elderly: Periodontal treatment needs in Germany 1997–2030. J. Clin. Periodontol. 2018, 45, 1400–1407. [Google Scholar] [CrossRef]
- Moynihan, P. Foods and factors that protect against dental caries. Nutr. Bull. 2000, 25, 281–286. [Google Scholar] [CrossRef]
- Gastner, M.T.; Newman, M.E. From the Cover: Diffusion-basedmethod for producing density-equalizing maps. Proc. Natl. Acad. Sci. USA 2004, 101, 7499–7504. [Google Scholar] [CrossRef]
- Groneberg-Kloft, B.; Fischer, T.C.; Quarcoo, D.; Scutaru, C. New quality and quantity indices in science (NewQIS): The study protocol of an international project. J. Occup. Med. Toxicol. 2009, 4, 16. [Google Scholar] [CrossRef]
- CIA. The World Factbook. Central Intelligence Agency. 2017; Volume 2014. Available online: https://www.cia.gov/the-world-factbook/ (accessed on 1 April 2014).
- Schoffel, N.; Kirchdorfer, M.; Bruggmann, D.; Bundschuh, M.; Ohlendorf, D.; Groneberg, D.A.; Bendels, M.H. Sarcoidosis: A Descriptive Approach to the Global Research Network and Recent Scientific Developments. Pneumologie 2016, 70, 28–36. [Google Scholar] [PubMed]
- Greene, J.C.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Broxo. 2015. Available online: https://eu.broxo.com/about-us (accessed on 17 March 2020).
- Axelsson, P.; Lindhe, J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults. J. Clin. Periodontol. 1978, 5, 133–151. [Google Scholar] [CrossRef] [PubMed]
- Barnes, C.M.; Russell, C.M.; Reinhardt, R.A.; Payne, J.B.; Lyle, D.M. Comparison of irrigation to floss as an adjunct to tooth brushing: Effect on bleeding, gingivitis, and supragingival plaque. J. Clin. Dent. 2005, 16, 71–77. [Google Scholar] [PubMed]
- Magri, M.H.; Solari, A. The SCI Journal Citation Reports: A Potential Tool for Studying Journals? Description of the JCR Journal Population Based on the Number of Citations Received, Number of Source Items, Impact Factor, Immediacy Index and Cited Half-Life. Scientometrics 1996, 35, 93–117. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; de Mello, A.L.F.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral health in the elderly patient and its impact on general well-being: A nonsystematic review. Clin. Interv. Aging 2015, 10, 461–467. [Google Scholar] [CrossRef] [PubMed]
- NIH. Funding to Schools and Institutions. 2017. Available online: https://www.nidcr.nih.gov/grants-funding/funding-to-schools-institutions/dental-schools/FY2017 (accessed on 27 February 2020).
- Cabrini-Gracio, M.C.; Tannuri-de Oliveira, E.F.; de Araujo-Gurgel, J.; Escalona, M.I.; Pulgarin-Guerrero, A. Dentistry scientometric analysis: A comparative study between Brazil and other most productive countries in the area. Scientometrics 2013, 95, 753–769. [Google Scholar] [CrossRef]
- UNESCO eAtlas of Research and Experimental Development, Gesamtausgaben für FuE. 2017. Available online: https://www.tellmaps.com/uis/rd/#!/tellmap/-680879682/1 (accessed on 4 March 2020).
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global burden of severe periodontitis in 1990–2010: A systematic review and meta-regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.; Marcenes, W. Global Burden of Severe Tooth Loss: A Systematic Review and Meta-analysis. J. Dent. Res. 2014, 93 (Suppl. 7), 20S–28S. [Google Scholar] [CrossRef]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Gil-Montoya, J.A.; Navarrete-Cortes, J.; Pulgar, R.; Santa, S.; Moya-Anegón, F. World dental research production: An ISI database approach (1999–2003). Eur. J. Oral Sci. 2006, 114, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Quality Indicators in Oral Health Care: A Nordic Project. 2019. Available online: https://www.helsedirektoratet.no/rapporter/quality-indicators-in-oral-health-care-a-nordic-project-proceedings-in-2012-018/2019%20Nordic%20quality%20indicators%20oral%20health.pdf/_/attachment/inline/c901a3c8-259b-4484-96d5-4bdf5d85b33:3c3f67502008c978f39e5c739b4157d0b98dd25f/2019%20Nordic%20quality%20indicators%20oral%20health.pdf (accessed on 17 March 2020).
- Fejerskov, O.; Thylstrup, A.; Larsen, M.J. Rational use of fluorides in caries prevention. A concept based on possible cariostatic mechanisms. Acta Odontol. Scand. 1981, 39, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Cumming, B.R.; Löe, H. Toothbrushing frequency as it relates to plaque development and gingival health. J. Periodontol. 1973, 44, 396–405. [Google Scholar] [CrossRef]
- Forner, L.; Larsen, T.; Kilian, M.; Holmstrup, P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J. Clin. Periodontol. 2006, 33, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, P.; Lindhe, J. The effect of a preventive programme on dental plaque, gingivitis and caries in schoolchildren. Results after one and two years. J. Clin. Periodontol. 1974, 1, 126–138. [Google Scholar] [CrossRef]
- Axelsson, P.; Lindhe, J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults: Results after 6 years. J. Clin. Periodontol. 1981, 8, 239–248. [Google Scholar] [CrossRef]
- Axelsson, P.; Lindhe, J. On the prevention of caries and periodontal disease. Results of a 15-year longitudinal study in adults. J. Clin. Periodontol. 1991, 18, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Addy, M.; Greenman, J.; Renton-Harper, P.; Newcombe, R.; Doherty, F. Studies on stannous fluoride toothpaste and gel (2). Effects on salivary bacterial counts and plaque regrowth in vivo. J. Clin. Periodontol. 1997, 24, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.C.; Goyal, C.R.; Qaqish, J.G.; Cugini, M.A.; Thompson, M.C.; Warren, P.R. Single-use plaque removal efficacy of three power toothbrushes. J. Dent. 2005, 33 (Suppl. 1), 11–15. [Google Scholar] [CrossRef]
- Warren, P.R.; Ray, T.S.; Cugini, M.; Chater, B.V. A practice-based study of a power toothbrush: Assessment of effectiveness and acceptance. J. Am. Dent. Assoc. 2000, 131, 389–394. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Year | Citations | Title | Journal |
|---|---|---|---|---|---|
| Greene, Vermillion | USA | 1964 | 646 | Simplified oral hygiene Index | The Journal of the American Dental Association |
| Axelsson, Lindhe | Sweden | 1978 | 375 | Effect of controlled oral hygiene procedures on caries and periontal-disease in adults | Journal of Clinical Periodontology |
| Suomi et al. | USA | 1971 | 308 | Effect of controlled oral hygiene procedures on progression of peridontal disease in adults—results after third and final year | Journal of Clinical Periodontology |
| Featherstone | USA | 2000 | 297 | The science and practice of caries prevention | Journal of American Dental Association |
| Featherstone | USA | 1999 | 276 | Prevention and reversal of dental caries: role of low level fluoride | Community Dentistry and Oral Epidemiology |
| Axelsson, Lindhe | Sweden | 1981 | 266 | Effect of controlled oral hygiene procedures on caries and peridontal-disease in adults—results after 6 years | Journal of Clinical Periodontology |
| Axelsson, Lindhe | Sweden | 1974 | 241 | Effect of a preventive programme on dental plaque, gingivits and caries in schoolchildren—results after one and 2 years | Journal of Clinical Periodontology |
| Axelsson, Lindhe | Sweden | 1991 | 225 | On the prevention of caries and peridontal-disease—results of a 15-year longitudinal-study in adults | Journal of Clinical Periodontology |
| DeRiso et al. | USA | 1996 | 215 | Chlorhexidine gluconate 0.12% oral rinse reduces the incidence of total nosocomial respiratory infection and nonprophylactic systemic antibiotic use in patients undergoing heart surgery | Chest |
| Sönju, Rölla | Norway | 1973 | 209 | Chemical analysis of acquired pellicle formed in 2 h on cleaned human teeth in-vivo—rato of formation and amino-acid analysis | Caries research |
| Country | n | GDP in 1000 bn US-Dollar | Population in Mill. | RGPD | RPOP |
|---|---|---|---|---|---|
| Sweden | 276 | 570.1 | 9.72 | 484.13 | 28.40 |
| Finland | 139 | 271.2 | 5.26 | 512.54 | 26.43 |
| Norway | 116 | 500.2 | 5.14 | 231.91 | 22.57 |
| Denmark | 101 | 340.8 | 5.56 | 296.36 | 18.17 |
| Switzerland | 110 | 712.1 | 8.06 | 154.47 | 13.65 |
| Netherlands | 180 | 866.4 | 16.87 | 207.76 | 10.67 |
| UK | 634 | 2945 | 63.74 | 215.28 | 9.95 |
| New Zealand | 30 | 198.1 | 4.4 | 151.44 | 6.82 |
| Israel | 48 | 303.8 | 7.82 | 158.00 | 6.14 |
| Australia | 126 | 1444 | 22.5 | 87.26 | 5.60 |
| Canada | 161 | 1789 | 34.83 | 89.99 | 4.62 |
| Germany | 361 | 3860 | 80.99 | 93.52 | 4.46 |
| Belgium | 42 | 534.7 | 10.44 | 78.55 | 4.02 |
| USA | 1274 | 17,420 | 318.9 | 73.13 | 3.99 |
| Italy | 97 | 2148 | 61.68 | 45.16 | 1.57 |
| Japan | 182 | 4616 | 127.1 | 39.43 | 1.43 |
| Spain | 65 | 1407 | 47.73 | 46.20 | 1.36 |
| Brazil | 248 | 2353 | 202.6 | 105.40 | 1.22 |
| South Korea | 56 | 1410 | 49.03 | 39.72 | 1.14 |
| Turkey | 90 | 806.1 | 81.61 | 111.65 | 1.10 |
| Poland | 42 | 546.6 | 38.34 | 76.84 | 1.10 |
| France | 63 | 2847 | 66.25 | 22.13 | 0.95 |
| Iran | 41 | 404.1 | 80.84 | 101.46 | 0.51 |
| Thailand | 34 | 373.8 | 67.74 | 90.96 | 0.50 |
| China | 109 | 10,380 | 1355.7 | 10.50 | 0.08 |
| India | 84 | 2050 | 1236.3 | 40.98 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmadi, S.; Klingelhöfer, D.; Erbe, C.; Holzgreve, F.; Groneberg, D.A.; Ohlendorf, D. Oral Health: Global Research Performance under Changing Regional Health Burdens. Int. J. Environ. Res. Public Health 2021, 18, 5743. https://doi.org/10.3390/ijerph18115743
Ahmadi S, Klingelhöfer D, Erbe C, Holzgreve F, Groneberg DA, Ohlendorf D. Oral Health: Global Research Performance under Changing Regional Health Burdens. International Journal of Environmental Research and Public Health. 2021; 18(11):5743. https://doi.org/10.3390/ijerph18115743
Chicago/Turabian StyleAhmadi, Salim, Doris Klingelhöfer, Christina Erbe, Fabian Holzgreve, David A. Groneberg, and Daniela Ohlendorf. 2021. "Oral Health: Global Research Performance under Changing Regional Health Burdens" International Journal of Environmental Research and Public Health 18, no. 11: 5743. https://doi.org/10.3390/ijerph18115743
APA StyleAhmadi, S., Klingelhöfer, D., Erbe, C., Holzgreve, F., Groneberg, D. A., & Ohlendorf, D. (2021). Oral Health: Global Research Performance under Changing Regional Health Burdens. International Journal of Environmental Research and Public Health, 18(11), 5743. https://doi.org/10.3390/ijerph18115743