
Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review




Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.1.1. Participants
2.1.2. Concept
2.1.3. Context
2.2. Types of Studies
2.3. Search Strategy
2.4. Selection Process
2.5. Data Charting
2.6. Synthesis of Results
3. Results
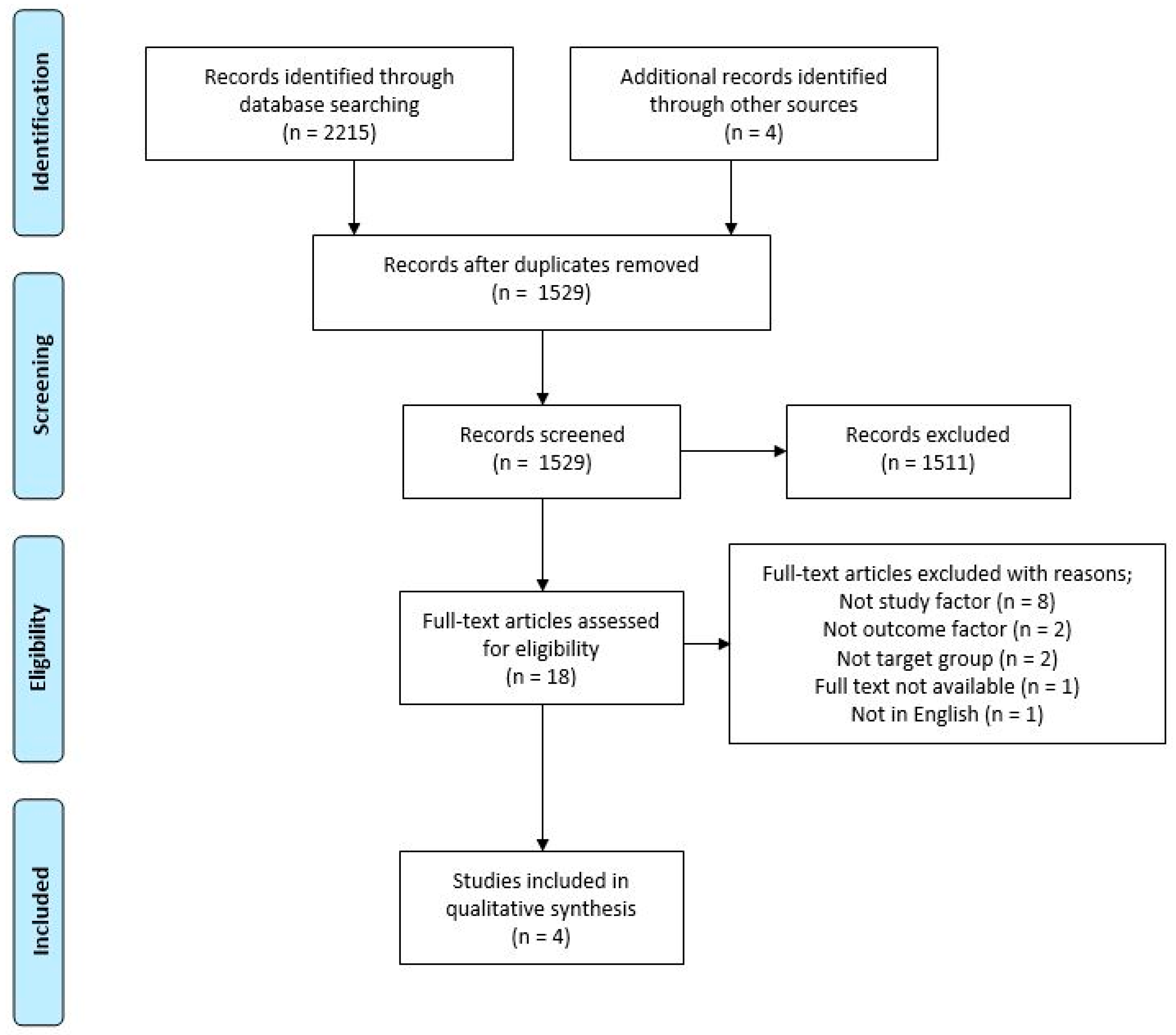
3.1. Search Results
3.2. Study Characteristics
3.3. Dietary Measures
3.4. Physical Activity Measures
3.5. Outcomes
3.5.1. Validity and Usability of Mobile Apps for Diet and Bone Health
3.5.2. Validity of Accelerometers for Physical Activity Assessment to Estimate Impact Loading
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewis, J.R.; Voortman, T.; Ioannidis, J.P. Evaluating and Strengthening the Evidence for Nutritional Bone Research: Ready to Break New Ground? J. Bone Miner. Res. 2021, 362, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; Zemel, B.S.; Wren, T.A.; Leonard, M.B.; Bachrach, L.K.; Rauch, F.; Gilsanz, V.; Rosen, C.J.; Winer, K.K. The Determinants of Peak Bone Mass. J. Pediatr. 2017, 180, 261–269. [Google Scholar] [CrossRef]
- Weaver, C.M.; Gordon, C.M.; Janz, K.F.; Kalkwarf, H.J.; Lappe, J.M.; Lewis, R.; O’Karma, M.; Wallace, T.C.; Zemel, B.S. The National Osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: A systematic review and implementation recommendations. Osteoporos. Int. 2016, 274, 1281–1386. [Google Scholar] [CrossRef]
- Pew Research Center. Smartphone Ownership and Internet Usage Continues to Climb in Emerging Economies. Available online: https://www.pewresearch.org/global/2016/02/22/internet-access-growing-worldwide-but-remains-higher-in-advanced-economies/ (accessed on 19 April 2021).
- Pew Research Center. Smartphone Ownership Is Growing Rapidly around the World, But Not Always Equally. 2019. Available online: https://www.pewresearch.org/global/2019/02/05/smartphone-ownership-is-growing-rapidly-around-the-world-but-not-always-equally/ (accessed on 19 April 2021).
- CMO. The State of Wearables in 2020. Available online: https://www.cmo.com.au/article/681977/state-wearables-2020/ (accessed on 21 December 2020).
- McClung, H.L.; Ptomey, L.T.; Shook, R.P.; Aggarwal, A.; Gorczyca, A.M.; Sazonov, E.S.; Becofsky, K.; Weiss, R.; Das, S.K. Dietary Intake and Physical Activity Assessment: Current Tools, Techniques, and Technologies for Use in Adult Populations. Am. J. Prev. Med. 2018, 55, e93–e104. [Google Scholar] [CrossRef]
- Chen, J.; Bauman, A.; Allman-Farinelli, M. A Study to Determine the Most Popular Lifestyle Smartphone Applications and Willingness of the Public to Share Their Personal Data for Health Research. Telemed. e-Health 2016, 22, 655–665. [Google Scholar] [CrossRef]
- Sharp, D.B.; Allman-Farinelli, M. Feasibility and validity of mobile phones to assess dietary intake. Nutrition 2014, 30, 1257–1266. [Google Scholar] [CrossRef]
- Allman-Farinelli, M. Using digital media to measure diet. CAB Rev. 2018, 13, 13034. [Google Scholar] [CrossRef]
- Boushey, C.J.; Spoden, M.; Zhu, F.; Delp, E.J.; Kerr, D.A. New mobile methods for dietary assessment: Review of image-assisted and image-based dietary assessment methods. Proc. Nutr. Soc. 2017, 763, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Rangan, A.M.; O’Connor, S.; Giannelli, V.; Yap, M.L.; Tang, L.M.; Roy, R.; Louie, J.C.Y.; Hebden, L.; Kay, J.; Allman-Farinelli, M. Electronic Dietary Intake Assessment (e-DIA): Comparison of a Mobile Phone Digital Entry App for Dietary Data Collection With 24-Hour Dietary Recalls. JMIR mHealth uHealth. 2015, 34, e98. [Google Scholar] [CrossRef] [PubMed]
- Rangan, A.M.; Tieleman, L.; Louie, J.C.Y.; Tang, L.M.; Hebden, L.; Roy, R.; Kay, J.; Allman-Farinelli, M. Electronic Dietary Intake Assessment (e-DIA): Relative validity of a mobile phone application to measure intake of food groups. Br. J. Nutr. 2016, 115, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Wellard-Cole, L.; Chen, J.; Davies, A.; Wong, A.; Huynh, S.; Rangan, A.; Allman-Farinelli, M. Relative Validity of the Eat and Track (EaT) Smartphone App for Collection of Dietary Intake Data in 18-to-30-Year Olds. Nutrients 2019, 11, 621. [Google Scholar] [CrossRef]
- Boushey, C.J.; Spoden, M.; Delp, E.J.; Zhu, F.; Bosch, M.; Ahmad, Z.; Shvetsov, Y.B.; Delany, J.P.; Kerr, D.A. Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults. Nutrition 2017, 9, 312. [Google Scholar] [CrossRef] [PubMed]
- Evenson, R.E.; Goto, M.M.; Furberg, R.D. Systematic review of the validity and reliability of consumer-wearable activity trackers. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 159. [Google Scholar] [CrossRef]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Morseth, B.; Emaus, N.; Jørgensen, L. Physical activity and bone: The importance of the various mechanical stimuli for bone mineral density. A review. Nor. Epidemiol. 2011, 20. [Google Scholar] [CrossRef]
- Bigouette, J.; Simon, J.; Liu, K.; Docherty, C.L. Altered Vertical Ground Reaction Forces in Participants with Chronic Ankle Instability While Running. J. Athl. Train. 2016, 519, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Ernst, D.; Schott, S.; Riera, C.; Hattendorf, J.; Romkes, J.; Granacher, U.; Göpfert, B.; Kriemler, S. Validation of two accelerometers to determine mechanical loading of physical activities in children. J. Sports Sci. 2015, 33, 1–8. [Google Scholar] [CrossRef]
- Fabre, N.; Lhuisset, L.; Bernal, C.; Bois, J. Effect of epoch length on intensity classification and on accuracy of measurement under controlled conditions on treadmill: Towards a better understanding of accelerometer measurement. PLoS ONE 2020, 15, e0227740. [Google Scholar] [CrossRef]
- Ancillao, A.; Tedesco, S.; Barton, J.; O’Flynn, B. Indirect Measurement of Ground Reaction Forces and Moments by Means of Wearable Inertial Sensors: A Systematic Review. Sensors 2018, 18, 2564. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Vainionpää, A.; Korpelainen, R.; Sievänen, H.; Vihriälä, E.; Leppäluoto, J.; Jämsä, T. Effect of impact exercise and its intensity on bone geometry at weight-bearing tibia and femur. Bone 2007, 40, 604–611. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.; Morrongiello, B.; Simpson, J.R.; Meckling, K. Vitamin D Intake among Young Canadian Adults: Validation of a Mobile Vitamin D Calculator App. J. Nutr. Educ. Behav. 2015, 47, 242–247.e1. [Google Scholar] [CrossRef] [PubMed]
- Tay, I.; Garland, S.; Gorelik, A.; Wark, J.D. Development and Testing of a Mobile Phone App for Self-Monitoring of Calcium In-take in Young Women. JMIR mHealth uHealth 2017, 53, e27. [Google Scholar] [CrossRef]
- Rowlands, A.; Stiles, V. Accelerometer counts and raw acceleration output in relation to mechanical loading. J. Biomech. 2012, 45, 448–454. [Google Scholar] [CrossRef]
- Higgins, S.; Higgins, L.Q.; Vallabhajosula, S. Site-specific Concurrent Validity of the ActiGraph GT9X Link in the Estimation of Activity-related Skeletal Loading. Med. Sci. Sports Exerc. 2021, 53, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Rollo, M.E.; Williams, R.L.; Burrows, T.; Kirkpatrick, S.I.; Bucher, T.; Collins, C.E. What Are They Really Eating? A Review on New Approaches to Dietary Intake Assessment and Validation. Curr. Nutr. Rep. 2016, 5, 307–314. [Google Scholar] [CrossRef]
- Zhu, F.; Bosch, M.; Khanna, N.; Boushey, C.J.; Delp, E.J. Multiple Hypotheses Image Segmentation and Classification with Application to Dietary Assessment. IEEE J. Biomed. Health Inform. 2015, 19, 377–388. [Google Scholar] [CrossRef]
- Daugherty, B.L.; Schap, T.E.; Ettienne-Gittens, R.; Zhu, F.M.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; Boushey, C.J.; Stumbo, P.; et al. Novel Technologies for Assessing Dietary Intake: Evaluating the Usability of a Mobile Telephone Food Record Among Adults and Adolescents. J. Med. Internet Res. 2012, 14, e58. [Google Scholar] [CrossRef]
- Martin, C.K.; Correa, J.; Han, H.; Allen, H.R.; Rood, J.C.; Champagne, C.M.; Gunturk, B.K.; Bray, G.A. Validity of the Remote Food Photography Method (RFPM) for Estimating Energy and Nutrient Intake in Near Real-Time. Obesity 2012, 20, 891–899. [Google Scholar] [CrossRef]
- Kouvari, M.; Mamalaki, E.; Bathrellou, E.; Poulimeneas, D.; Yannakoulia, M.; Panagiotakos, D.B. The validity of technology-based dietary assessment methods in childhood and adolescence: A systematic review. Crit. Rev. Food Sci. Nutr. 2021, 61, 1065–1080. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; Hurworth, M.; Giglia, R.; Trapp, G.; Strauss, P. Feasibility of a commercial smartphone application for dietary assessment in epidemiological research and comparison with 24-h dietary recalls. Nutr. J. 2018, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Mandic, I.; Lou, W.; Goodman, L.; Jacobs, I.; L’Abbe, M.R. Validation of a Tablet Application for Assessing Dietary In-takes Compared with the Measured Food Intake/Food Waste Method in Military Personnel Consuming Field Rations. Nutrients 2017, 93, 200. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-E.; Song, S.; Ahn, J.S.; Kim, Y.; Lee, J.E. Use of a Mobile Application for Self-Monitoring Dietary Intake: Feasibility Test and an Intervention Study. Nutrients 2017, 9, 748. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, V.; Voci, S.M.; Mendes-Netto, R.S.; Da Silva, D.G. The relative validity of a food record using the smartphone application MyFitnessPal. Nutr. Diet. 2017, 75, 219–225. [Google Scholar] [CrossRef]
- Svensson, Å.; Larsson, C. A Mobile Phone App for Dietary Intake Assessment in Adolescents: An Evaluation Study. JMIR mHealth uHealth 2015, 3, e93. [Google Scholar] [CrossRef]
- Bassey, E.J.; Rothwell, M.C.; Littlewood, J.J.; Pye, D.W. Pre- and Postmenopausal Women Have Different Bone Mineral Density Responses to the Same High-Impact Exercise. J. Bone Miner. Res. 1998, 1312, 1805–1813. [Google Scholar] [CrossRef]
- Stiles, V.H.; Griew, P.J.; Rowlands, A.V. Use of Accelerometry to Classify Activity Beneficial to Bone in Premenopausal Women. Med. Sci. Sports Exerc. 2013, 45, 2353–2361. [Google Scholar] [CrossRef]
- Vainionpää, A.; Korpelainen, R.; Vihriälä, E.; Rinta–Paavola, A.; Leppäluoto, J.; Jämsä, T. Intensity of exercise is associated with bone density change in premenopausal women. Osteoporos. Int. 2006, 17, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Ziebart, C.; Giangregorio, L.M.; Gibbs, J.C.; Levine, I.C.; Tung, J.; Laing, A.C. Measurement of peak impact loads differ between accelerometers—Effects of system operating range and sampling rate. J. Biomech. 2017, 58, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Allman-Farinelli, M.; Owen, K.; Signal, L.; Hosking, C.; Wang, L.; Bauman, A. Feasibility Study Comparing Physical Activity Classifications from Accelerometers with Wearable Camera Data. Int. J. Environ. Res. Public Health 2020, 17, 9323. [Google Scholar] [CrossRef] [PubMed]
- Doherty, A.; Jackson, D.; Hammerla, N.; Plötz, T.; Olivier, P.; Granat, M.H.; White, T.; Van Hees, V.T.; Trenell, M.I.; Owen, C.G.; et al. Large Scale Population Assessment of Physical Activity Using Wrist Worn Accelerometers: The UK Biobank Study. PLoS ONE 2017, 12, e0169649. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year, Country | Aims/Purpose | Lifestyle Factor/s | Sample Size (n) | Age in Years Range, Mean (SD) 1 | Sex, Female (%) | Funding |
|---|---|---|---|---|---|---|
| Goodman [27] 2015 Canada | To establish the validity and reproducibility of the dietary component of a mobile vitamin D calculator app | Vitamin D Calcium | Vitamin D (50) Calcium (48) | 18–25 22.0 (2.0) | 50 | Canadian Institutes for Health Research Frederick Banting Doctoral Scholarship (grant #596230) |
| Tay [28] 2017 Australia | To assess the usability and acceptability of Calci-app in young women to self-monitor dietary calcium intake and its potential for use in a bone health mHealth behavior change intervention | Calcium | 40 | 18–25 N/R 2 | 100 | Nowpos M-Solutions Pvt Ltd. (Hyderabad, India) for supporting the development of Calci-app; no conflicts of interest to declare. |
| Rowlands [29] 2012 UK | To assess the relationship of accelerometer output, in counts (ActiGraph GT1M) and as raw accelerations (ActiGraph GT3X+ and GENEA), with GRF 3 in adults | Physical Activity | 10 | N/R2 Males; 26.4 (4.0) Female; 32.4 (10.5) Overall; 29.4 (8.2) | 50 | No external funding was received for this research. None of the authors have a conflict of interest with ActivInsights or ActiGraph, the manufacturers of the technologies on which this article is based. |
| Higgins [30] 2020 USA | (1) To assess the concurrent validity of raw accelerometer outputs with GRF 3 and loading rates calculated from force plate across a range of simulated habitual physical activities. (2) To identify the optimal wear site among the ankle, hip and wrist with the strongest relationships between accelerometer and force plate and/or skeletal outcomes. | Physical Activity | 30 | 18–35 23.0 (4.5) | 50 | Faculty Research and Development funds from Elon University. The authors declare no conflict of interest. |
| Ref | Technology Type | Study Type | Outcome Measures | Important Results |
|---|---|---|---|---|
| [27] | Mobile app Intake of vitamin D and calcium containing foods, beverages and supplements in app. Immediate nutrient feedback is provided relative to recommendations (3 days over 1 month; 2 weekdays and 1 weekend). Three multiple-pass 24-h dietary recalls. | Validity and Reproducibility | Differences in mean vitamin D and calcium between app and recall (paired-sample t-tests). Agreement between app and recall for vitamin D and calcium (Bland–Altman plot and Pearson correlation). Classification of mean intakes between app and recall (Wilcoxon signed-rank and intra-class correlations). Reproducibility of intakes estimated by the app over three time points (intra-class correlations, single measures, 2-way mixed and absolute agreement and Wilcoxon signed-rank tests). | Validity Correlations Vitamin D (IU/d); calcium (mg/g) agreement (app, recall); difference (app, recall) Food: (r = 0.84, p < 0.001; difference p = 0.20); (r = 0.63, p < 0.001; difference p = 0.49) Supplements: (r = 0.98, p < 0.001; difference p = 0.23); (r = 0.98, p < 0.001; difference p = 0.32) All sources: (r = 0.92, p < 0.001; difference p = 0.08); (r = 0.65, p < 0.001; difference p = 0.49) Intra-class correlations (ICC) Comparing binary classification 1 of 3-day mean recall vs. app ICC = 0.88 (95% CI: 0.80, 0.93; p< 0.001) (vitamin D) ICC = 0.50 (95% CI: 0.25, 0.68; p < 0.001) (calcium) Bland–Altman The percentage of points within LOA; 44% (vitamin D), 60% (calcium) Wilcoxon signed-rank tests Assessing quartile classification 2 of 3-day mean recall vs. app Z = –0.50, p = 0.62 (vitamin D); Z = –0.46, p = 0.65 (calcium) Reproducibility Intra-class correlations (ICC) Comparing app recording day 1 vs. 3 for mean intakes: ICC = 0.40 (95% CI: 0.14, 0.61; p = 0.002 (vitamin D) ICC = 0.22 (95% CI: –0.06, 0.47; p = 0.06 (calcium) Wilcoxon signed-rank tests Quartile mean intakes comparing days 1 vs. 2, 2 vs. 3 and 1 vs. 3 Vitamin D or calcium (p > 0.05 for all) Mean intakes for app recording day 1 vs. 3: Z = –1.19, p = 0.24 (vitamin D); Z = –1.76, p = 0.08 (calcium) |
| [28] | Mobile app A dietary app to self-monitor calcium consumption, to report the actual calcium levels in food and beverages that are typical of an Australian diet (5 days over 2-week period, 3 non-consecutive weekdays and 2 non-consecutive weekend days). | Usability | 5-item usability questionnaire using 5-point Likert scales (strongly agree to strongly disagree). | Completed the usability questionnaire (n = 33, 83%). Easy and convenient to use (n = 20, 61%), app design intuitive and not confusing to use (n = 26, 79%), time-consuming (n = 14, 42%) Useful (n = 10, 30%) |
| [29] | Wearable device Three tri-axial accelerometers. Right Hip: GT1M, GT3X+ and GENEA. Left wrist: GT3X+. Right wrist: GENEA. GT1M 1 s epoch GT3X+ sampling rate 100 Hz. GENEAs sampling rate 80 Hz. Operating range 6 g. GRF 960 Hz using force plates. | Validity | Raw output between GT3X+ and GENA differed by activity and/or monitor (series of fully repeated measures ANOVAs—monitor × activity). Resultant peak g differed by hip or wrist across activities (ANOVAs (location × activity × monitor). Relationships between accelerometer output variables and force plate output variables (correlations, Fisher’s zr transformation). | Relationship between GRF 3 variables and GT1M counts: Peak impact force (r = 0.85, p < 0.05) Average resultant force (r = 0.73, p < 0.05) Peak loading rate (r = 0.76, p < 0.05). Relationship between GRF 3 variables and raw acceleration output: Hip vertical axis (GT3X+; GENEA) Peak impact force (r = 0.73, NS 4; r = 0.74, NS 4) Average resultant (r = 0.85, p < 0.05; r = 0.82, p < 0.05) Peak loading rate (r = 0.76, p < 0.05; r = 0.70, p < 0.05) Hip resultant (GT3X+; GENEA) Peak impact force (r = 0.73, NS 4; r = 0.73, NS 4) Average resultant (r = 0.87, p < 0.05; r = 0.85, p < 0.05) Peak loading rate (r = 0.70, p < 0.05; r = 0.63, p < 0.05) Wrist resultant (GT3X+; GENEA) Peak impact force GT3X+ (r = 0.59, NS 4); GENEA (r = 0.58, NS 4) Average resultant GT3X+ (r = 0.82, p < 0.05); GENEA (r = 0.87, p < 0.05) Peak loading rate GT3X+ (r = 0.79, p < 0.05); GENEA (r = 0.81, p < 0.05) |
| [30] | Wearable device Actigraph GT9X Link tri-axial accelerometers (right ankle, hip and wrist). Operating range ±8 g. Sampling rate 100 Hz. GRF 1000 Hz using force plates. | Validity | Accelerometer output and force plate output across wear sites (repeated measures correlations to assess concurrent validity). | Combined activities Hip Peak hip resultant acceleration and resultant loading rate (r = 0.74, p < 0.001, 95% CI: 0.718, 0.769) Peak hip resultant accelerations and resultant GRF 3 (r = 0.69, p < 0.001, 95% CI: 0.660, 0.720) Peak hip vertical accelerations and vertical GRF 3 (r = 0.50, p < 0.001, 95% CI: 0.455, 0.541) Peak hip vertical accelerations and loading rate (r = 0.57, p < 0.001, 95% CI: 0.525, 0.603) Wrist Peak wrist resultant accelerations and resultant loading rate (r = 0.17, p < 0.001, 95% CI: 0.113, 0.224) Peak wrist resultant acceleration and resultant GRF3 (r = 0.01, p = 0.815, 95% CI: −0.051, 0.064) Ankle Peak vertical acceleration and vertical GRF 3 (r = −0.09, p = 0.003, 95% CI: −0.145, −0.031) Peak vertical acceleration and vertical loading rate (r = 0.10, p = 0.001, 95% CI: 0.041, 0.155) Peak resultant acceleration and resultant GRF 3 (r = −0.09, p = 0.001, 95% CI: −0.151, −0.038) Peak resultant acceleration and resultant loading rate (r = 0.05, p = 0.063, 95% CI: −0.003, 0.111) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davies, A.; Shi, Y.; Bauman, A.; Allman-Farinelli, M. Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 5688. https://doi.org/10.3390/ijerph18115688
Davies A, Shi Y, Bauman A, Allman-Farinelli M. Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(11):5688. https://doi.org/10.3390/ijerph18115688
Chicago/Turabian StyleDavies, Alyse, Yumeng Shi, Adrian Bauman, and Margaret Allman-Farinelli. 2021. "Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 11: 5688. https://doi.org/10.3390/ijerph18115688
APA StyleDavies, A., Shi, Y., Bauman, A., & Allman-Farinelli, M. (2021). Validity of New Technologies That Measure Bone-Related Dietary and Physical Activity Risk Factors in Adolescents and Young Adults: A Scoping Review. International Journal of Environmental Research and Public Health, 18(11), 5688. https://doi.org/10.3390/ijerph18115688