
Transmission Dynamics, Heterogeneity and Controllability of SARS-CoV-2: A Rural–Urban Comparison



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Statistical Analysis
2.2.1. Inference about Transmission Characteristics
2.2.2. Estimation of Serial Interval
2.2.3. Assessment of Different Interventions
3. Results
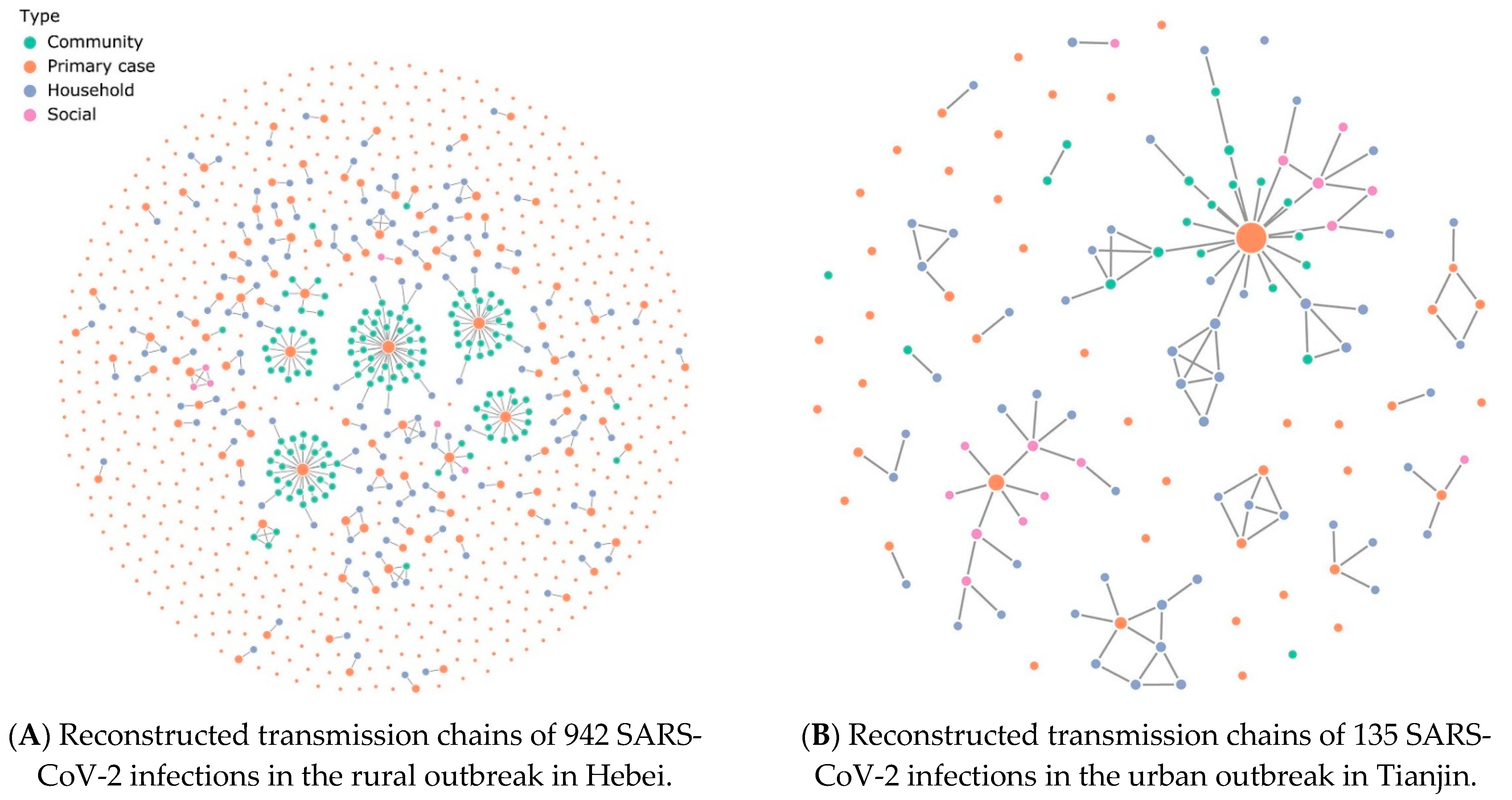
3.1. Characterizing SARS-CoV-2 Transmission Chains in Rural and Urban Areas
3.2. Comparison of SARS-CoV-2 Transmission Characteristics between the Rural and Urban Areas
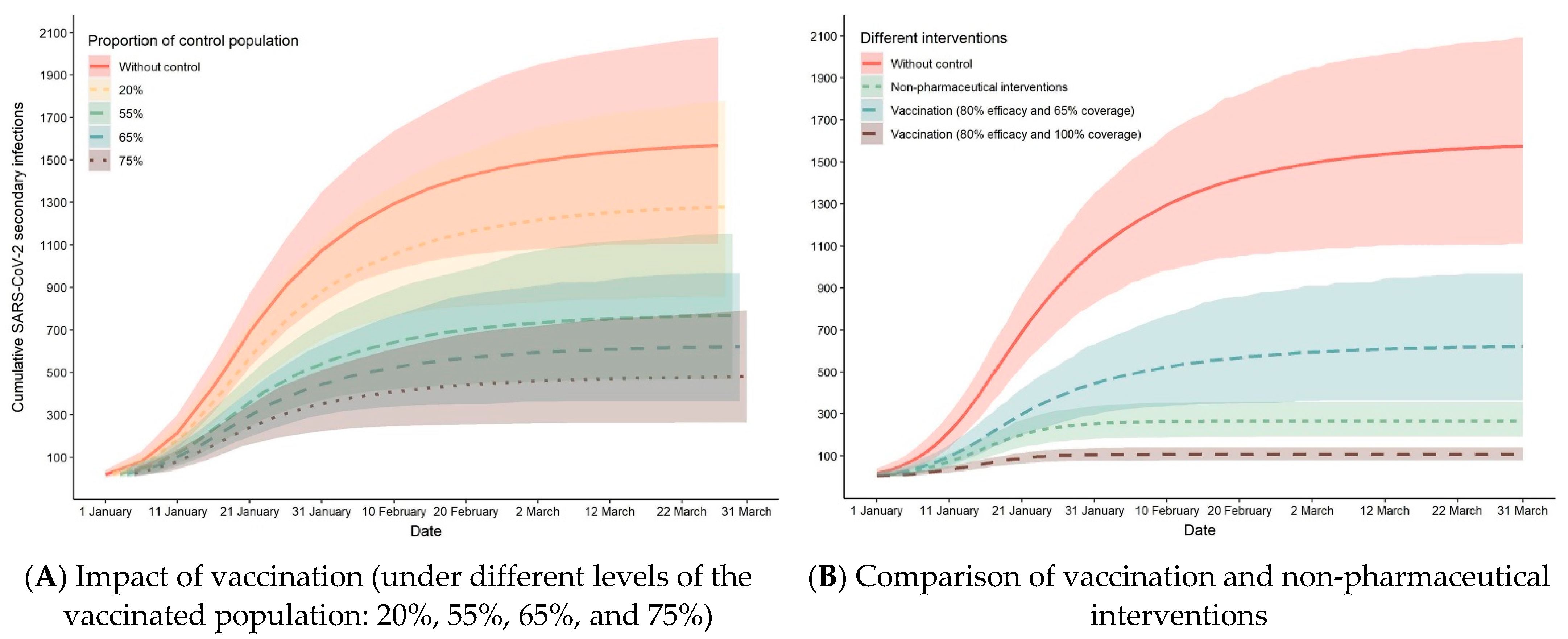
3.3. Assessment of NPIs and Vaccination in SARS-CoV-2 Transmission
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lloyd-Smith, J.O.; Schreiber, S.J.; Kopp, P.E.; Getz, W.M. Superspreading and the effect of individual variation on disease emergence. Nature 2005, 438, 355–359. [Google Scholar] [CrossRef]
- Park, B.J.; Peck, A.J.; Kuehnert, M.J.; Newbern, C.; Smelser, C.; Comer, J.A.; Jernigan, D.; McDonald, L.C. Lack of SARS Transmission among Healthcare Workers, United States. Emerg. Infect. Dis. 2004, 10, 244–248. [Google Scholar] [CrossRef]
- Ha, L.D.; Bloom, S.A.; Hien, N.Q.; Maloney, S.A.; Mai, L.Q.; Leitmeyer, K.C.; Anh, B.H.; Reynolds, M.G.; Montgomery, J.M.; Comer, J.A.; et al. Lack of SARS Transmission among Public Hospital Workers, Vietnam. Emerg. Infect. Dis. 2004, 10, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Lipsitch, M.; Cohen, T.; Cooper, B.; Robins, J.M.; Ma, S.; James, L.; Gopalakrishna, G.; Chew, S.K.; Tan, C.C.; Samore, M.H.; et al. Transmission dynamics and control of severe acute respiratory syndrome. Science 2003, 300, 1966–1970. [Google Scholar] [CrossRef]
- Riley, S.; Fraser, C.; Donnelly, C.A.; Ghani, A.C.; Abu-Raddad, L.J.; Hedley, A.J.; Leung, G.M.; Ho, L.M.; Lam, T.H.; Thach, T.Q.; et al. Transmission dynamics of the etiological agent of SARS in Hong Kong: Impact of public health interventions. Science 2003, 300, 1961–1966. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, R.; He, Q.; Pascual, M. Quantifying asymptomatic infection and transmission of COVID-19 in New York City using observed cases, serology and testing capacity. MedRxiv 2020, 1–10. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.-M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef]
- He, J.; Guo, Y.; Mao, R.; Zhang, J. Proportion of asymptomatic coronavirus disease 2019: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 820–830. [Google Scholar] [CrossRef]
- Asghar, Z.; Ward, D.; Huntly, P.; Inghels, M.; Tanser, F. COVID-19 (SARS-CoV-2) Outbreaks in Rural United Kingdom: Patterns of Spread and Empirical Evidence for the “Rule of Six”. Lancet 2021. [Google Scholar] [CrossRef]
- Lau, M.S.Y.; Grenfell, B.; Thomas, M.; Bryan, M.; Nelson, K.; Lopman, B. Characterizing superspreading events and age-specific infectiousness of SARS-CoV-2 transmission in Georgia, USA. Proc. Natl. Acad. Sci. USA 2020, 117, 22430–22435. [Google Scholar] [CrossRef]
- Sherman, J. Rural Poverty in the United States; Tickamyer, A.R., Warlick, J., Eds.; Columbia University Press: New York, NY, USA, 2017; ISBN 9780231172226. [Google Scholar]
- Green, G.P. 15. The Opportunities and Limits of Economic Growth. In Rural Poverty in the United States; Tickamyer, A.R., Sherman, J., Warlick, J., Eds.; Columbia University Press: New York, NY, USA, 2017; pp. 416–438. ISBN 0231544715. [Google Scholar]
- Bailey, C.; Jensen, L.; Ransom, E. Rural America in a Globalizing World; West Virginia University Press: Morgantown, WV, USA, 2014; ISBN 1940425107. [Google Scholar]
- Henning-Smith, C. The Unique Impact of COVID-19 on Older Adults in Rural Areas. J. Aging Soc. Policy. 2020, 32, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Peters, D.J. Community Susceptibility and Resiliency to COVID-19 Across the Rural-Urban Continuum in the United States. J. Rural Heal. 2020, 36, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Richards, J.S.; Li, Z.-H.; Gong, Y.-F.; Zhang, S.-Z.; Xiao, N. A framework for assessing local transmission risk of imported malaria cases. Infect. Dis. Poverty 2019, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Zhou, Y.; Ye, J.; Abdullah AL-maskri, A.A.; Kang, Y.; Zeng, S.; Cai, S. Recent advances and perspectives of nucleic acid detection for coronavirus. J. Pharm. Anal. 2020, 10, 97–101. [Google Scholar] [CrossRef]
- Giordano, G.; Colaneri, M.; Di Filippo, A.; Blanchini, F.; Bolzern, P.; De Nicolao, G.; Sacchi, P.; Colaneri, P.; Bruno, R. Modeling vaccination rollouts, SARS-CoV-2 variants and the requirement for non-pharmaceutical interventions in Italy. Nat. Med. 2021, 1–6. [Google Scholar] [CrossRef]
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Health Commision of Hebei Province. Outbreak Notification. Available online: http://wsjkw.hebei.gov.cn/xgyqtb/index.jhtml (accessed on 2 January 2021).
- Health Commission of Tianjin. Outbreak Notification. Available online: http://wsjk.tj.gov.cn/ZTZL1/ZTZL750/YQFKZL9424/ (accessed on 21 January 2020).
- Government of China. China, T.C.G. of the P.R. of Guiding Opinions on Scientific Prevention and Control, Precise Measures, and Divisional Levels for the Prevention and Control of the COVID-19. Available online: http://www.gov.cn/zhengce/2020-02/18/content_5480514.htm (accessed on 18 February 2020).
- Center for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19)—2020 Interim Case Definition, Approved 5 April 2020. Available online: https://wwwn.cdc.gov/nndss/conditions/coronavirus-disease-2019-covid-19/case-definition/2020/ (accessed on 7 May 2021).
- Sun, K.; Wang, W.; Gao, L.; Wang, Y.; Luo, K.; Ren, L.; Zhan, Z.; Chen, X.; Zhao, S.; Huang, Y.; et al. Transmission heterogeneities, kinetics, and controllability of SARS-CoV-2. Science 2021, 371. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Coronavirus Disease (COVID-19): Situation Report, 200. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 7 August 2020).
- Harris, T.E. The Theory of Branching Processes; Springer: Berlin/Heidelberg, Germany, 1963; Volume 6. [Google Scholar]
- Blumberg, S.; Lloyd-Smith, J.O. Inference of R0 and Transmission Heterogeneity from the Size Distribution of Stuttering Chains. PloS Comput. Biol. 2013, 9. [Google Scholar] [CrossRef]
- Blumberg, S.; Funk, S.; Pulliam, J.R.C. Detecting Differential Transmissibilities That Affect the Size of Self-Limited Outbreaks. PloS Pathog. 2014, 10. [Google Scholar] [CrossRef]
- Ng, S.H.X.; Kaur, P.; Kremer, C.; Tan, W.S.; Tan, A.L.; Hens, N.; Toh, M.P.; Teow, K.L.; Kannapiran, P. Estimating transmission parameters for COVID-19 clusters by using symptom onset data, Singapore, January–April 2020. Emerg. Infect. Dis. 2021, 27, 582–585. [Google Scholar] [CrossRef]
- Iboi, E.A.; Ngonghala, C.N.; Gumel, A.B. Will an imperfect vaccine curtail the COVID-19 pandemic in the U.S.? Infect. Dis. Model. 2020, 5, 510–524. [Google Scholar] [CrossRef] [PubMed]
- Kohavi, R. A study of Cross-Validation and Bootstrap for Accuracy Estimation and Model Selection. In Proceedings of the International Joint Conference on AI (IJCAI), Montreal, QC, Canada, 20–25 August 1995; Volume 14, pp. 1137–1145. [Google Scholar]
- Qi, S.; Zhao, X.; Hao, P.; Liu, N.; Gao, G.F.; Song, Y.; Xu, W.; Li, Q. Two Reemergent Cases of COVID-19—Hebei Province, China, January 2, 2021. China CDC Wkly. 2021, 3, 25–27. [Google Scholar] [CrossRef]
- Laboratory Testing Group; Song, Y.; Zhao, X.; Li, X.; Xu, W. A Case of COVID-19—Tianjin Municipality, China, November 7, 2020. China CDC Wkly. 2020, 2, 884–885. [Google Scholar] [CrossRef]
- Rivera-Hernandez, M.; Ferdows, N.B.; Kumar, A. The Impact of the Covid-19 Epidemic on Older Adults in Rural and Urban Areas in Mexico. J. Gerontol. Ser. B 2020. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Wang, W.; Wang, Y.; Litvinova, M.; Luo, K.; Ren, L.; Sun, Q.; Chen, X.; Zeng, G.; Li, J. Infectivity, susceptibility, and risk factors associated with SARS-CoV-2 transmission under intensive contact tracing in Hunan, China. MedRxiv 2020. [Google Scholar] [CrossRef]
- Liu, L. Emerging study on the transmission of the Novel Coronavirus (COVID-19) from urban perspective: Evidence from China. Cities 2020, 103, 102759. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, T.; Lueck, J.A.; Trujillo, K.L.; Ferdinand, A.O. Rural and Urban Differences in COVID-19 Prevention Behaviors. J. Rural Health 2021, 37, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Mahale, P.; Rothfuss, C.; Bly, S.; Kelley, M.; Bennett, S.; Huston, S.L.; Robinson, S. Multiple COVID-19 Outbreaks Linked to a Wedding Reception in Rural Maine—August 7–September 14, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1686. [Google Scholar] [CrossRef]
- Yang, Q.; Xiao, X.; Gu, X.; Liang, D.; Cao, T.; Mou, J.; Huang, C.; Chen, L.; Liu, J. Surveillance of common respiratory infections during COVID-19 pandemic demonstrates preventive effectiveness of non-pharmaceutical interventions. Int. J. Infect. Dis. 2021, 105, 442–447. [Google Scholar] [CrossRef]
- Markel, H.; Lipman, H.B.; Navarro, J.A.; Sloan, A.; Michalsen, J.R.; Stern, A.M.; Cetron, M.S. Nonpharmaceutical interventions implemented by US cities during the 1918–1919 influenza pandemic. JAMA 2007, 298, 644–654. [Google Scholar] [CrossRef]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J. Durability of responses after SARS-CoV-2 mRNA-1273 vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Urban Area (Tianjin, n = 135) | Rural Area (Hebei, n = 942) | p-Value | |
|---|---|---|---|
| Age, years | <0.001 | ||
| Median (IQR) | 49 (36–62) | 46 (30–60) | |
| <20 | 5 (3.7%) | 155 (16.4%) | |
| 20–64 | 110 (81.4%) | 633 (67.2%) | |
| ≥65 | 20 (14.8%) | 152 (16.1%) | |
| Sex | 0.01 | ||
| Female | 63 (46.7%) | 553 (58.7%) | |
| Male | 72 (53.3%) | 387 (41.1%) | |
| Contact type | <0.001 | ||
| Household | 55 (61.1%) | 147 (51.4%) | |
| Social | 15 (16.7%) | 6 (2.1%) | |
| Community | 20 (22.2%) | 133 (46.5%) | |
| Median of serial interval | 5.5 (IQR: 3.6–7.8) | 6.0 (IQR: 3.6–9.0) | 0.73 |
| Transmission dynamics † | |||
| R | 0.74 | 0.55 | 0.16 |
| LRT 95% CI | (0.51, 1.10) | (0.45, 0.68) | |
| BCa bootstrap 95% CI | (0.53, 3.49) | (0.44, 0.69) | |
| k | 0.35 | 0.14 | 0.09 |
| LRT 95% CI | (0.13, 1.21) | (0.10, 0.20) | |
| BCa bootstrap 95% CI | (0.12, 0.95) | (0.10, 0.19) |
| R (95% CI) | k (95% CI) | |
|---|---|---|
| Before first round citywide NAT (<1/09) | 0.81 (0.65, 1.02) | 0.27 (0.14, 0.56) |
| During first to second round citywide NAT (1/09–1/14) | 0.33 (0.22, 0.50) | 0.13 (0.07, 0.23) |
| After second round citywide NAT (>1/14) | 0.36 (0.25, 0.55) | 0.17 (0.10, 0.31) |
| R | k | |
|---|---|---|
| Null asymptomatic infections (p = 0) | 0.51 | 0.13 |
| 20% asymptomatic infections (p = 0.2) | 0.56 | 0.14 |
| 40% asymptomatic infections (p = 0.4) | 0.63 | 0.17 |
| 60% asymptomatic infections (p = 0.6) | 1.62 | 0.09 |
| 80% asymptomatic infections (p = 0.8) | 1.78 | 0.10 |
| All asymptomatic infections (p = 1) | 1.95 | 0.13 |
| Mean (SD) for 10-fold cross-validation | 0.55 (0.02) | 0.14 (0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Hu, T.; Gai, X.; Zhang, Y.; Zhou, X. Transmission Dynamics, Heterogeneity and Controllability of SARS-CoV-2: A Rural–Urban Comparison. Int. J. Environ. Res. Public Health 2021, 18, 5221. https://doi.org/10.3390/ijerph18105221
Li Y, Hu T, Gai X, Zhang Y, Zhou X. Transmission Dynamics, Heterogeneity and Controllability of SARS-CoV-2: A Rural–Urban Comparison. International Journal of Environmental Research and Public Health. 2021; 18(10):5221. https://doi.org/10.3390/ijerph18105221
Chicago/Turabian StyleLi, Yuying, Taojun Hu, Xin Gai, Yunjun Zhang, and Xiaohua Zhou. 2021. "Transmission Dynamics, Heterogeneity and Controllability of SARS-CoV-2: A Rural–Urban Comparison" International Journal of Environmental Research and Public Health 18, no. 10: 5221. https://doi.org/10.3390/ijerph18105221
APA StyleLi, Y., Hu, T., Gai, X., Zhang, Y., & Zhou, X. (2021). Transmission Dynamics, Heterogeneity and Controllability of SARS-CoV-2: A Rural–Urban Comparison. International Journal of Environmental Research and Public Health, 18(10), 5221. https://doi.org/10.3390/ijerph18105221