Perceptions and Experiences of the University of Nottingham Pilot SARS-CoV-2 Asymptomatic Testing Service: A Mixed-Methods Study

 ,
,  ,
,  ,
, 
 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Pilot Asymptomatic Testing Service (P-ATS)
- (a)
- SARS2-PCR tests offered weekly for the 12-week study period (10× swab and 2× saliva);
- (b)
- SARS2-antibody tests offered alternate weeks (6 x self-sampled finger-prick dried blood sample).
2.2. Participants, Recruitment and Sampling
2.3. Online Survey
2.4. Qualitative Interviews and Focus Groups
2.5. Reflexivity Statement
2.6. Data Analysis
2.7. Patient and Public Involvement
3. Results
3.1. Survey Results
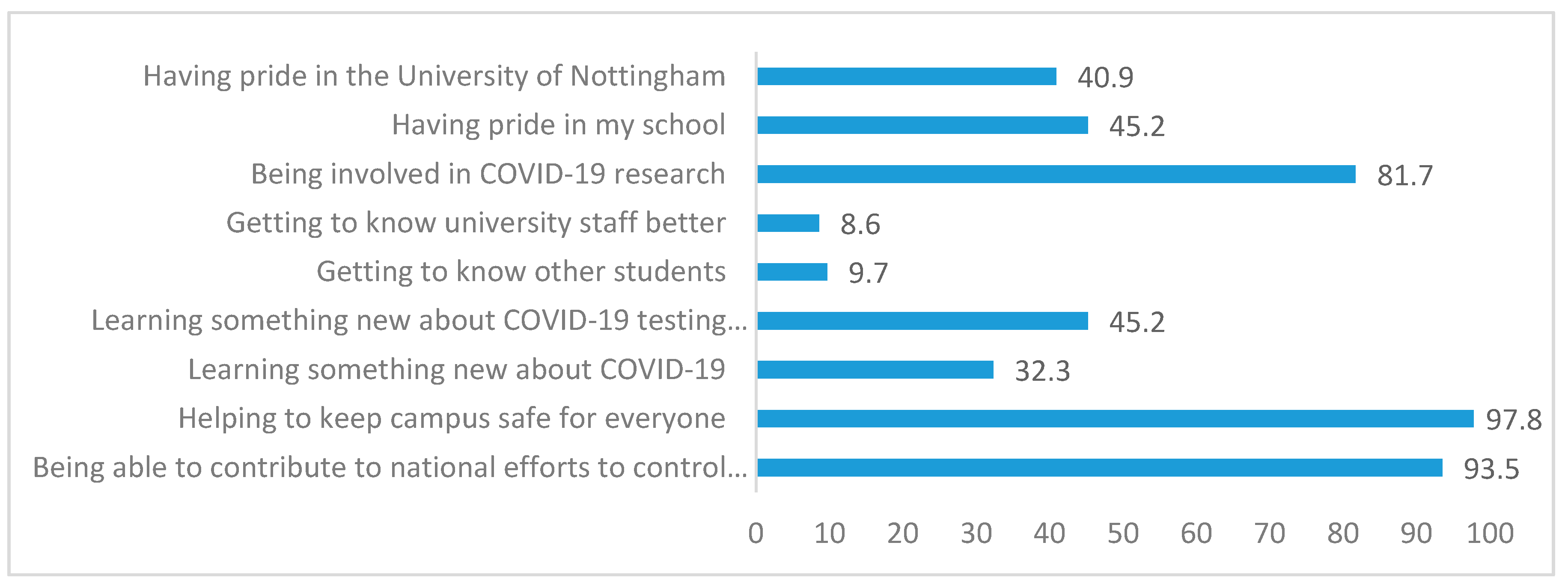
3.1.1. Reasons for Testing
3.1.2. Case Identification
3.1.3. Acceptability and Programme Satisfaction
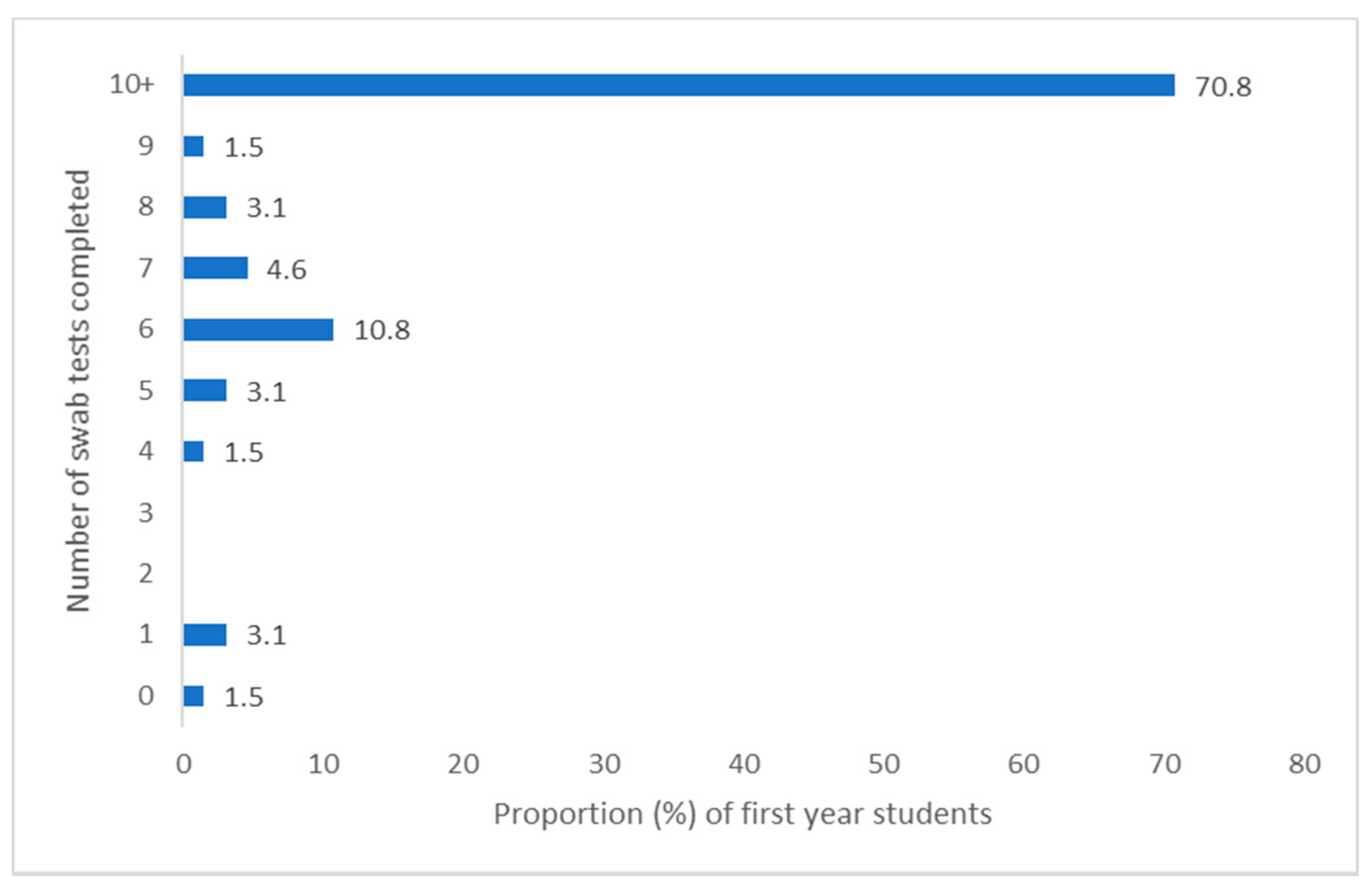
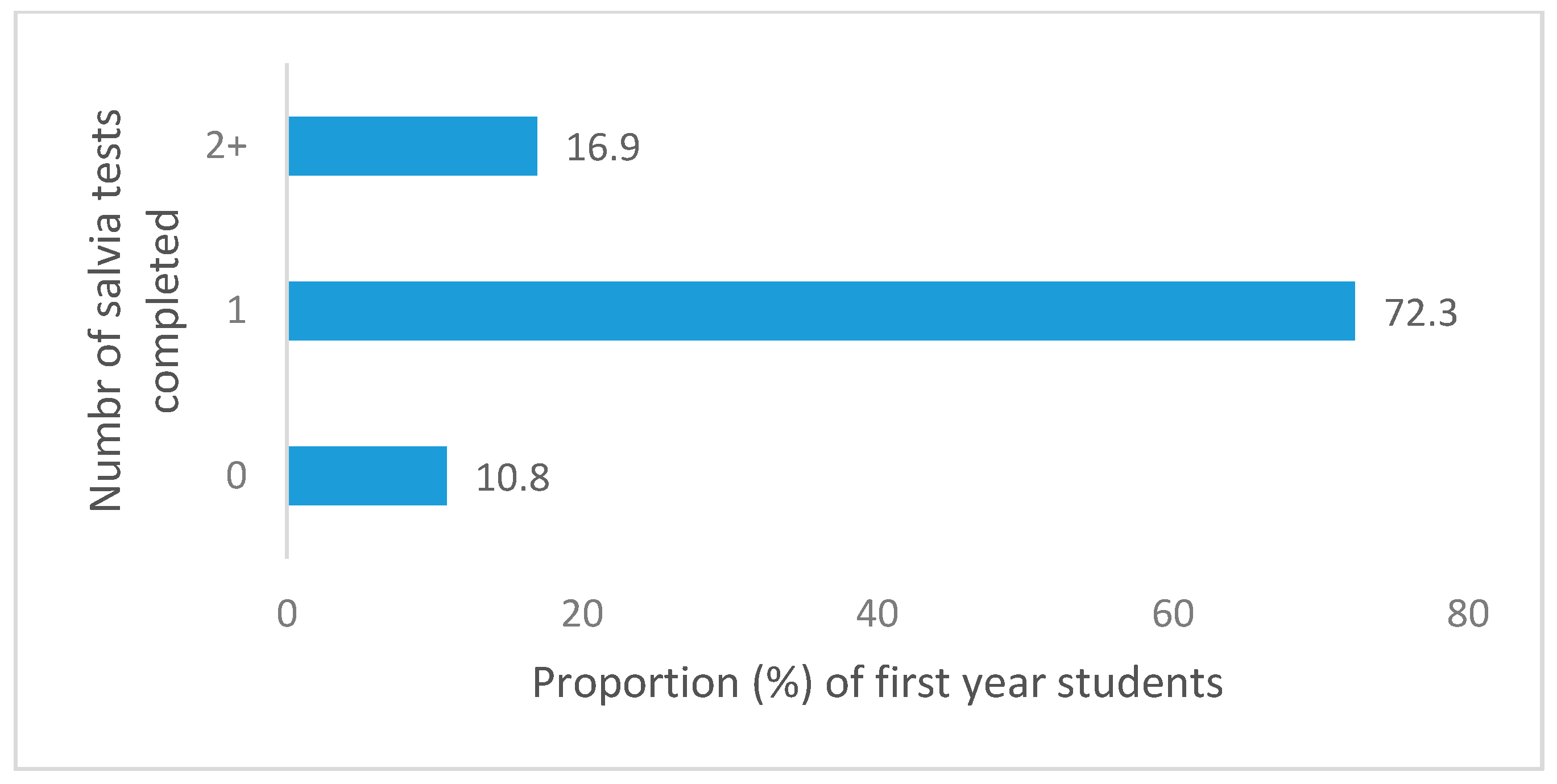
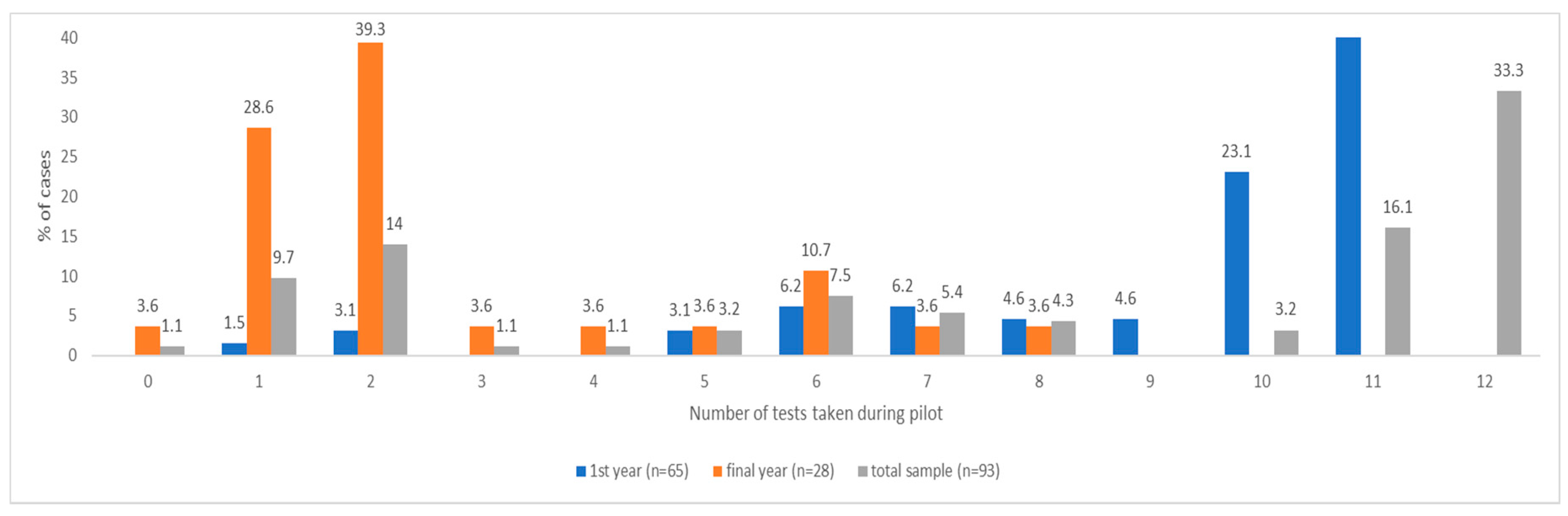
3.1.4. Testing Adherence
3.1.5. Correlates of Self-Testing
3.1.6. Correlates of Mental Health
3.1.7. Protective Health Behaviours
3.2. Qualitative Results
3.2.1. Theme 1: Emotional Responses to COVID-19
3.2.2. University Life during COVID-19
3.2.3. Theme 3: Influences on Testing Participation
3.2.4. Theme 4: Testing—Physical and Logistical Factors
3.2.5. Theme 5: Testing—Effects on Wellbeing
4. Discussion
4.1. Programme Evaluation
4.2. Adherence to Testing
4.3. Risk Perceptions and Protective Behaviours
4.4. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- BBC News Coronavirus: ‘It Reminds you Why You Want to be a Vet’. Available online: https://www.bbc.co.uk/news/av/uk-england-nottinghamshire-53560591 (accessed on 27 July 2020).
- Weedon, K.; Cornwell, B. The small-world network of college classes: Implications for epidemic spread on a university campus. J. Soc. Sci. 2020, 7, 222–241. [Google Scholar]
- Cabinet Office Briefing Rooms. Policy Paper: Slides to Accompany Coronavirus Press Conference: 9 September 2020; Prime Minister’s Office: London, UK, 2020. [Google Scholar]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Bowen, M. Covid-19 has changed how we teach students. Vet. Record. 2020, 186, 14. [Google Scholar] [CrossRef] [PubMed]
- Berger Gillam, T.; Cole, J.; Gharbi, K.; Angiolini, E.; Barker, T.; Bickerton, P.; Brabbs, T.; Chin, J.; Coen, E.; Cossey, S.; et al. Norwich COVID-19 testing initiative pilot: Evaluating the feasibility of asymptomatic testing on a university campus. J. Public Health 2020, fdaa194. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- DHSC; Department of Health and Social Care. Coronavirus (COVID-19): Scaling Up Our Testing Programmes. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/878121/coronavirus-covid-19-testing-strategy.pdf (accessed on 16 November 2020).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- NHS England. Guide 09: Running Focus Groups for Patient and Public Engagement. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/07/bitesize-guide-focus-groups.pdf (accessed on 29 November 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Valentine-Graves, M.; Hall, E.; Guest, J.L.; Adam, E.; Valencia, R.; Shinn, K.; Hardee, I.; Sanchez, T.; Siegler, A.J.; Sullivan, P.S. At-home self-collection of saliva, oropharyngeal swabs and dried blood spots for SARS-CoV-2 diagnosis and serology: Post-collection acceptability of specimen collection process and patient confidence in specimens. PLoS ONE 2020, 15, e0236775. [Google Scholar] [CrossRef] [PubMed]
- Auschra, C.; Möller, J.; Berthod, O.; Mazheika, Y.; Borusiak, P. Communicating test results in a comprehensible manner: A randomized controlled trial of word usage in doctor-patient communication—Article in German. Z. Evid. Fortbild. Qual. Gesundhwes 2020, 156–157, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.M.; Tun, Z.M.; Kumar, V.; Quaye, S.E.D.; Offeddu, V.; Cook, A.R.; Lwin, M.O.; Jiang, S.; Tam, C.C. Population anxiety and positive behaviour change during the COVID-19 epidemic: Cross-sectional surveys in Singapore, China and Italy. Influenza Respir. Viruses 2020, 00, 1–11. [Google Scholar] [CrossRef]
- Van, D.; McLaws, M.; Crimmins, J.; MacIntyre, C.R.; Seale, H. University life and pandemic influenza: Attitudes and intended behaviour of staff and students towards pandemic (H1N1). BMC Public Health 2010, 14, 130. [Google Scholar] [CrossRef]
- Généreux, M.; Schluter, P.J.; Hung, K.K.; Wong, C.S.; Pui Yin Mok, C.; O’Sullivan, T.; David, M.D.; Carignan, M.-E.; Blouin-Genest, G.; Champagne-Poirier, O.; et al. One Virus, Four Continents, Eight Countries: An Interdisciplinary and International Study on the Psychosocial Impacts of the COVID-19 Pandemic among Adults. Int. J. Environ. Res. Public Health 2020, 17, 8390. [Google Scholar] [CrossRef]
- Dratva, J.; Zysset, A.; Schlatter, N.; von Wyl, A.; Huber, M.; Volken, T. Swiss University Students’ Risk Perception and General Anxiety during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7433. [Google Scholar] [CrossRef]
- Meléndez, J.C.; Satorres, E.; Reyes-Olmedo, M.; Delhom, I.; Real, E.; Lora, Y. Emotion recognition changes in a confinement situation due to COVID-19. J. Environ. Psychol. 2020, 72, 101518. [Google Scholar] [CrossRef]
- Kaparounaki, C.K.; Patsali, D.P.V.; Mousa, E.V.; Papadopoulou, K.K.; Fountoulakis, K.N. University students’ mental health amidst the COVID-19 quarantine in Greece. Psychiatry Res. 2020, 290, 113111. [Google Scholar] [CrossRef]
- Odriozola, P.; Planchuelo, Á.; Irurtia, M.J.; de Luis, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef]
- VetFutures. Women in the Veterinary Profession 2014: Gender Statistics about Veterinary Surgeons in the UK. Available online: https://www.vetfutures.org.uk/download/gender-statistics-about-veterinary-surgeons-in-the-uk/ (accessed on 30 November 2020).
- Kelly, G. Veterinary Medicine Is a Woman’s World. Veterinarian’s Money Digest. 7 May 2017. Available online: https://www.vmdtoday.com/news/veterinary-medicine-is-a-womans-world (accessed on 30 November 2020).
- HESA. Higher Education Student Statistics: UK, 2017/18—Student Numbers and Characteristics. 17 January 2019. Available online: https://www.hesa.ac.uk/news/17-01-2019/sb252-higher-education-student-statistics/numbers (accessed on 30 November 2020).
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Raffle, A.E.; Pollock, A.M.; Harding-Edgar, L. Covid-19 mass testing programmes. BMJ 2020, 370, m3262. [Google Scholar] [CrossRef] [PubMed]
- Walke, H.T.; Honein, M.A.; Redfield, R.R. Preventing and responding to COVID-19 on college campuses. JAMA 2020, 324, 1727–1728. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Gender | Year of Study | Ind/SG/FG † | Date | Time | Duration (mins) |
|---|---|---|---|---|---|---|
| P101 | F | 5 | IND | 16 October 2020 | 16:30 | 36:31 |
| P106 | F | 5 | IND | 18 October 2020 | 18:00 | 44:56 |
| P116 | F | 1 | IND | 24 October 2020 | 19:00 | 48:33 |
| P112 | F | 1 | IND | 24 October 2020 | 10:30 | 17:50 |
| P117 | F | 1 | IND | 25 October 2020 | 14:30 | 50:47 |
| P121 | F | 1 | IND | 30 October 2020 | 11:00 | 13:12 |
| P91 | F | 1 | SG | 02 September 2020 | 14:00 | 32:50 |
| P92 | F | 1 | SG | 02 September 2020 | 14:00 | 32:50 |
| P93 | F | 1 | SG | 02 September 2020 | 14:00 | 32:50 |
| P99 | M | 1 | SG | 14 October 2020 | 14:00 | 32:50 |
| P100 | M | 1 | SG | 14 October 2020 | 14:00 | 32:50 |
| P104 | F | 1 | SG | 17 October 2020 | 16:30 | 45:30 |
| P105 | M | 1 | SG | 17 October 2020 | 16:30 | 45:30 |
| P102 | M | 5 | SG | 17 October 2020 | 10:30 | 43:55 |
| P103 | F | 5 | SG | 17 October 2020 | 10:30 | 43:55 |
| P107 | F | 1 | SG | 18 October 2020 | 11:30 | 42:06 |
| P108 | M | 5 | SG | 18 October 2020 | 11:40 | 42:06 |
| P109 | F | 5 | SG | 23 October 2020 | 16:30 | 48:19 |
| P110 | F | 1 | SG | 23 October 2020 | 16:30 | 48:19 |
| P111 | F | 1 | SG | 23 October 2020 | 16:30 | 48:19 |
| P113 | F | 5 | SG | 24 October 2020 | 16:30 | 48:48 |
| P114 | F | 5 | SG | 24 October 2020 | 16:30 | 48:48 |
| P115 | F | 5 | SG | 24 October 2020 | 16:30 | 48:48 |
| P118 | F | 1 | SG | 27 October 2020 | 19:00 | 48:51 |
| P119 | F | 5 | SG | 27 October 2020 | 19:00 | 48:51 |
| P120 | F | 1 | SG | 27 October 2020 | 19:00 | 48:51 |
| P94 | F | 1 | FG | 25 September 2020 | 13:00 | 53:49 |
| P95 | F | 1 | FG | 25 September 2020 | 13:00 | 53:49 |
| P96 | F | 1 | FG | 25 September 2020 | 13:00 | 53:49 |
| P97 | F | 1 | FG | 25 September 2020 | 13:00 | 53:49 |
| P98 | F | 1 | FG | 25 September 2020 | 13:00 | 53:49 |
| Staff Participants | ||||||
| ID | Gender | Job Role | Ind/SG/FG † | Date | Time | Duration (mins) |
| P127 | F | Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P129 | M | Senior Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P130 | F | Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P126 | F | Clinical academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P123 | F | Senior administrator | FG | 28 October 2020 | 15:00 | 70:58 |
| P128 | F | Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P125 | F | Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P124 | F | Clinical academic | FG | 28 October 2020 | 15:00 | 70:58 |
| P122 | F | Administrator | FG | 28 October 2020 | 15:00 | 70:58 |
| P131 | M | Senior Academic | FG | 28 October 2020 | 15:00 | 70:58 |
| Respondent Characteristics (N = 99) | Category | n (%) |
|---|---|---|
| Year of study | First year | 69 (69.7) |
| Final year | 30 (30.3) | |
| Gender | ||
| Male | 13 (13.1) | |
| Female | 84 (84.8) | |
| Prefer not to say | 2 (2.0) | |
| Ethnicity | ||
| Asian or Asian British | 3 (3.03) | |
| White | 91 (93.9) | |
| Prefer not to say | 3 (3.0) | |
| Student background | ||
| Home student | 91 (91.9) | |
| European student (EU) | 8 (8.1) | |
| Accommodation during term | Private accommodation with family | 4 (4.0) |
| Private accommodation with others | 32 (32.3) | |
| Halls of residence | 63 (63.6) |
| Mean (SD) | Group Mean Difference | ||
|---|---|---|---|
| Total sample | n = 99 | 7.21 (6.01); Range: 0–21 | |
| Year of study | First year (n = 69) | 6.73 (6.02) | n.s |
| Final year (n = 30) | 8.33 (5.92) | ||
| Students’ self-isolating | Yes (>=once; n = 36) | 7.39 (6.41) | n.s |
| No (n = 63) | 7.11 (5.82) | ||
| Positive cases | Yes (n = 4) | 6.50 (5.00) | |
| No (n = 89) | 7.18 (6.00) | n.s. | |
| Accommodation during term | Private accommodation (n = 36) | 8.89 (6.27) | * t (97) = 2.138, p = 0.035, Cohen’s d = 0.44 |
| Halls of residence (n = 63) | 6.25 (5.68) | ||
| P-ATS pilot | Pilot participants (n = 93) | 7.15 (6.00) | n.s.* |
| Non-pilot participants (n = 6) | 8.17 (7.52) |
| Pilot Procedure or Participant Experience | Response Options | Antibody Tests n (%) | Swab and Saliva Tests † n (%) | ||||
|---|---|---|---|---|---|---|---|
| Total Sample | First Year | Final Year | Total Sample | First Year | Final Year | ||
| How did you collect test kits? | Collected myself | 32 (34.4) | 18 (27.7) | 14 (50.0) | 36 (38.7) | 17 (26.2) | 19 (67.9) |
| Collected by others in household/bubble | 12 (12.9) | 11 (16.9) | 1 (3.6) | 9 (9.7) | 8 (12.3) | 1 (3.6) | |
| Mix of both | 36 (38.7) | 35 (53.8) | 1 (3.6) | 46 (49.5) | 39 (60.0) | 7 (25.0) | |
| Didn’t collect any test | 13 (14) | 1 (1.5) | 12 (42.9) | 2 (2.2) | 1 (1.5) | 1 (3.6) | |
| Were you able to return the completed test kit by requested time? | Yes, always | 58 (62.4) | 42 (64.6) | 16 (57.1) | 61 (65.6) | 39 (60.0) | 22 (78.6) |
| Yes sometimes | 19 (20.4) | 19 (29.2) | - | 31 (33.3) | 26 (40.0) | 5 (17.9) | |
| Didn’t complete any test | 16 (17.2) | 4 (6.2) | 12 (42.9) | 1 (1.1) | - | 1 (3.6) | |
| Were you satisfied with location of the drop-off? | Yes | 74 (79.6) | 59 (90.8) | 15 (53.6) | 88 (94.6) | 63 (96.9) | 25 (89.3) |
| No | 2 (2.2) | 1 (1.5) | 1 (3.6) | - | - | 1 (10.7) | |
| Didn’t drop off a completed kit myself | 17 (18.3) | 5 (7.7) | 12 (42.9) | 5 (5.4) | 2 (3.1) | - | |
| † Satisfied with the university approach to communicating positive test results | Yes | - | - | - | 86 (92.5) | 59 (90.8) | 27 (96.4) |
| † Satisfied with the university approach to communicating negative test results | Yes | - | - | - | 61 (65.6) | 49 (75.4) | 12 (42.9) |
| Item | Response Option | Total Sample (n = 99) | First Year (n = 69) | Final Year (n = 30) |
|---|---|---|---|---|
| Would take part in University testing in future if it was offered to me | Yes | 94 (94.9) | 66 (95.7) | 28 (93.3) |
| Would encourage others to take part in University testing | Yes | 97 (98.0) | 97 (97.1) | 30 (100) |
| P-ATS sample (n = 93) | P-ATS First year (n = 65) | P-ATS Final year (n = 28) | ||
| Satisfaction with information received | Very satisfied | 43 (46.2) | 34 (52.3) | 9 (32.1) |
| Somewhat satisfied | 46 (49.5) | 29 (44.6) | 17 (60.7) | |
| Somewhat dissatisfied | 4 (4.3) | 2 (3.1) | 2 (7.1) | |
| Very dissatisfied | - | - | - | |
| Satisfaction with programme communications | Very satisfied | 43 (46.2) | 34 (52.3) | 9 (32.1) |
| Somewhat satisfied | 40 (43) | 26 (40.0) | 14 (50.0) | |
| Somewhat dissatisfied | 9 (9.7) | 4 (6.2) | 5 (17.9) | |
| Very dissatisfied | 1 (1.1) | 1 (1.5) | - | |
| Gained new knowledge | Yes | 45 (51.6) | 39 (60.0) | 9 (32.1) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Frequency of COVID-19 test completion | 1 | −0.179 | −0.287 ** | −0.239 * | −0.001 | −0.267 * | −0.282 ** | −0.344 ** | −0.189 |
| 2. Worry about getting COVID-19 | 1 | 0.565 ** | −0.026 | −0.173 | 0.04 | −0.023 | 0.141 | −0.066 | |
| 3. Worry about friends and family getting COVID-19 | 1 | −0.009 | −0.19 | 0.092 | 0.005 | 0.124 | 0.163 | ||
| 4. Satisfaction with drop-off location + | 1 | 0.292 ** | 0.125 | 0.253 * | 0.177 | 0.153 | |||
| 5. Satisfaction with positive test result communication + | 1 | 0.133 | 0.281 ** | 0.311 ** | 0.051 | ||||
| 6. Satisfaction with negative test result communication + | 1 | 0.293 ** | 0.354 *** | 0.024 | |||||
| 7. Satisfaction with overall P-ATS information received | 1 | 0.564 ** | 0.058 | ||||||
| 8. Satisfaction with how overall P-ATS information was communicated | 1 | 0.016 | |||||||
| 9. Gained new knowledge through the pilot | 1 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Frequency of antibody tests completed | 1 | −0.071 | −0.220 * | −0.226 * | −0.318 ** | −0.169 | −0.137 | −0.533 ** |
| 2. Worry about getting COVID-19 | 1 | 0.533 ** | −0.014 | 0.148 | −0.065 | −0.042 | 0.152 | |
| 3. Worry about friends and family getting COVID-19 | 1 | 0.023 | 0.139 | 0.159 | −0.131 | 0.216 * | ||
| 4. Satisfaction with overall P-ATS information received | 1 | 0.608 ** | 0.07 | 0.317 ** | 0.259 * | |||
| 5. Satisfaction with how overall P-ATS information was communicated | 1 | 0.015 | 0.272 ** | 0.403 *** | ||||
| 6. Gained new knowledge through P-ATS | 1 | −0.01 | 0.194 | |||||
| 7. Confidence in test outcomes + | 1 | 0.013 | ||||||
| 8. Satisfaction with drop-off location + | 1 |
| Frequency of Swab Tests Completed | ||||
|---|---|---|---|---|
| Step | Predictor | β | B | Basis |
| Step 1 | ||||
| (force wise) | Gender | −0.088 | −0.815 | 0.538 |
| Year of Study | −0.848 *** | −1.952 | 0.134 | |
| ∆R2 | 0.707 *** | |||
| Step 2 | ||||
| (stepwise) | Gender | −0.070 | −0.648 | 0.513 |
| Year of Study | −0.821 *** | −1.891 | 0.129 | |
| Anxiety (GAD-7) | −0.180 ** | −0.129 | 0.040 | |
| ∆R2 | 0.031 ** | |||
| Step 3 | ||||
| (stepwise) | Gender | −0.115 * | −1.062 | 0.499 |
| Year of Study | −0.868 *** | −1.999 | 0.125 | |
| Anxiety (GAD-7) | −0.296 *** | −0.213 | 0.045 | |
| Worry about getting COVID-19 | 0.227 ** | 1.384 | 0.400 | |
| ∆R2 | 0.032 ** | |||
| Step 4 | ||||
| (stepwise) | Gender | −0.098 | −0.907 | 0.494 |
| Year of Study | −0.846 *** | −1.949 | 0.125 | |
| Anxiety (GAD-7) | −0.244 *** | −0.175 | 0.047 | |
| Worry about getting COVID-19 | 0.205 ** | 1.254 | 0.397 | |
| Satisfaction with the way information was communication | −0.118 * | −0.723 | 0.344 | |
| ∆R2 | 0.011 * | |||
| (Constant) | 17.623 *** | 1.22 | ||
| Frequency of Antibody Tests Completed | ||||
|---|---|---|---|---|
| Step | Predictor | β | B | Basis |
| Step 1 | ||||
| (forced entry) | Gender + | 0.052 | 0.263 | 0.405 |
| Year of Study | −0.648 *** | −0.832 | 0.103 | |
| ∆R2 | 0.431 *** | |||
| Step 2 | ||||
| (stepwise) | Gender | 0.082 | 0.415 | 0.388 |
| Year of Study | −0.609 *** | −0.781 | 0.099 | |
| Anxiety (GAD-7) | −0.247 ** | −0.099 | 0.031 | |
| ∆R2 | 0.059 ** | |||
| Step 3 | ||||
| (stepwise) | Gender | 0.021 | 0.109 | 0.374 |
| Year of Study | −0.674 *** | −0.865 | 0.096 | |
| Anxiety (GAD-7) | −0.413 *** | −0.165 | 0.034 | |
| Worry about getting COVID-19 | 0.326 *** | 1.111 | 0.306 | |
| ∆R2 | 0.066 *** | |||
| Step 4 | ||||
| (stepwise) | Gender | 0.021 | 0.108 | 0.363 |
| Year of Study | −0.590 *** | −0.757 | 0.102 | |
| Anxiety (GAD-7) | −0.345 *** | −0.137 | 0.035 | |
| Worry about getting COVID-19 | 0.296 *** | 1.010 | 0.300 | |
| Satisfaction with the location of drop-off location | −0.203 * | −0.615 | 0.243 | |
| ∆R2 | 0.03 * | |||
| Step 5 | ||||
| (stepwise) | Gender | 0.078 | 0.395 | 0.382 |
| Year of Study | −0.584 *** | −0.749 | 0.100 | |
| Anxiety (GAD-7) | −0.310 *** | −0.124 | 0.035 | |
| Worry about getting COVID-19 | 0.257 ** | 0.876 | 0.301 | |
| Satisfaction with the location of drop-off location | −0.205 8 | −0.620 | 0.239 | |
| Confidence in outcome test result ++ | −0.153 8 | −0.895 | 0.431 | |
| ∆R2 | 0.02 * | |||
| (Constant) | 6.22 | 0.938 | ||
| Anxiety (GAD-7) | ||||
|---|---|---|---|---|
| Step | Predictor | β | B | Basis |
| Step 1 | ||||
| (forced entry) | Gender + | 0.122 | 1.544 | 1.323 |
| Year of study | 0.16 | 0.515 | 0.335 | |
| ∆R2 | 0.036 | |||
| Step 2 | ||||
| (stepwise) | Gender | −0.017 | −0.219 | 2.776 |
| Year of Study | 0.002 | 0.005 | 1.163 | |
| Worry about getting COVID-19 | 0.560 *** | 4.799 | 0.298 | |
| ∆R2 | 0.275 *** | |||
| Step 3 | ||||
| (stepwise) | Gender | −0.007 | −0.091 | 1.124 |
| Year of Study | −0.07 | −0.226 | 0.3 | |
| Worry about getting COVID-19 | 0.410 *** | 3.508 | 0.911 | |
| Worry about friends and family getting COVID-19 | 0.294 ** | 2.37 | 0.87 | |
| ∆R2 | 0.054 ** | |||
| Step 4 | ||||
| (stepwise) | Gender | −0.654 | 1.05 | −0.051 |
| Year of Study | −0.412 | 0.281 | −0.128 | |
| Worry about getting COVID-19 | 3.361 | 0.843 | 0.393 | |
| Worry about friends and family getting COVID-19 | 2.28 | 0.805 | 0.283 | |
| Satisfied with the way in which information was communicated to me. | 2.743 | 0.691 | 0.323 | |
| ∆R2 | 0.098 *** | |||
| (Constant) | 2.047 ** | 3.086 | ||
| Total Sample (n = 99) | Pilot Participants (n = 93) | Nonparticipants (n = 6) | Group Difference † | Negative Test (n = 89) | Positive Test (n = 4) | Group Difference † | Have self-Isolated (n = 36) | Have not Self-Isolated (n = 63) | Group Difference † | |
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived importance of protective behaviours for virus control (rated 1–10) | ||||||||||
| Social distancing | 8.24 (1.79) | 8.29 (1.75) | 7.50 (2.58) | n.s. | 8.33 (1.74) | 7.5 (2.08) | n.s. | 7.89 (1.98) | 8.44 (1.64) | n.s. |
| Regular hand washing | 9.04 (1.47) | 9.02 (1.50) | 9.33 (1.033) | n.s. | 9.03 (1.52) | 8.75 (.96) | n.s. | 8.69 (1.64) | 9.24 (1.34) | n.s. |
| Self-isolating | 9.04 (1.47ß) | 9.10 (1.714) | 8.83 (1.329) | n.s. | 9.16 (1.57) | 7.75 (3.86) | n.s. | 8.61 (n = 2.19) | 9.35 (n = 1.27) | n.s. |
| Wearing a face covering | 9.08 (1.69) | 8.39 (2.08) | 7.17 (1.722) | n.s. | 8.40 (2.06) | 8.00 (2.83) | n.s. | 8.25 (2.10) | 8.35 (2.7) | n.s. |
| Perceived risk of COVID-19 (pre-pilot; rated 1–10) | 5.56 (1.768) | 5.67 (1.71) | 3.83 (1.94) | t (92) = 2.53, p < 0.05 | 5.69 (1.72) | 5.25 (1.50) | n.s. | 5.42 (1.99) | 5.63 (1.64) | n.s. |
| Perceived risk of COVID-19 (post-pilot; rated 1–10) | 6.47 (2.01) | 6.54 (2.00) | 5.50 (2.08) | n.s. | 6.45 (1.98) | 8.50 (1.29) | t (91) = 2.043, p < 0.05 | 6.22 (2.28) | 6.62 (1.85) | n.s. |
| Theme | Subthemes | Representative Quotations |
|---|---|---|
| Emotional Responses to COVID-19 | Negative Feelings | I am definitely suffering from COVID fatigue, that is how much I think about COVID (P126, Female, Staff—Academic) I think it has been a lot of like adaptation but I think the most stressful part was when I came back and had to go on rotations because then you couldn’t avoid the thing that was stressing you, which was like seeing other people. (P101, Female, Yr5, Student). |
| COVID-19 Around Me | My eldest son has Asthma and I mean he is nine, so he is young, but it was still a concern that I was thinking crikey if he gets COVID is that going to be a massive deal? (P128, Female, Staff—Academic) My parents are both over 60, my mother in particular was shielding, I opted to stay at university, both for exams and for lockdown purposes (P106, Female, Yr5, Student) I had not left my house since March and so I didn’t know anyone who had had COVID or been out anywhere that I could get COVID really, so I was quite nervous moving here (P111, Female, Yr1, Student) | |
| Coping with COVID-19 | Sometimes I feel so much better if I just don’t watch the news and not even think about it because you turn the news on for a bit in the morning and it is just a bit depression” (P91, Female, Yr1, Student) Yes, I think isolation was all right, it was just erm trying to keep busy really. Not get too bored (P105, Male, Yr1, Student) | |
| University Life during COVID-19 | Adapting to a new normal | You kind of get used to studying online and then you go there, and you get used to studying there, and then you come back and then you’re thinking like you are virtually (P117, Female, Yr1, Student) If you’re in a household where you don’t really get along, or you don’t really socialise and you have the option to go and see I don’t know the football team or some friends that you went to university with, or somebody is having a get together and you don’t want to feel left out. It is much more challenging to say no in those types of situations (P106, Female, Yr5, Student) Because a lot of my release is going outside, riding horses and just going for walks and stuff and when you can’t do that, and you don’t really even have a window to lean out of. It drives you a bit nuts (P107, Female, Yr1, Student) |
| Improving University Life | Means of having food delivered is a big one, potentially access to some sort of entertainment, be it you know a subscription package or… or like just some form of entertainment. Additionally I think they are the big ones, people get bored and people feel that they need to go out and get stuff and if you have that then… the people that will adhere would adhere much more happily (P106, Female, Yr5, Student) Just helping to make the university a safer place and just keeping, erm, COVID levels as low as possible by making people isolate… I think all we need is like shopping deliveries and any post etcetera. I think that is all in place as it is (P112, Female, Yr1, Student) | |
| Influences on Testing Participation | Testing Freedom | I just wanted to know if I was positive so that I could take steps not to spread it and to kind of know that I was you know at risk and people near me were at risk so that was my main driver (P128, Female, Staff—Academic) I have opted just to do the testing for my own peace of mind (P106, Female, Yr5, Student) |
| External Influences | I guess you could say I was influenced by the university really pressing us to do it as a good idea (P100, Male, Yr1, Student) I did it because all of my flat did it and we just decided that we would do it together, erm and also I just wanted to help out and be part of the research (P112, Female, Yr1, Student) | |
| Curiosity | We are scientists really and I think we should be doing these things, we should be pushing ourselves, we should be seeing what we can do and how we can do it, so curiosity, but also you know we were the very first people who actually designed something like that and went through the pain because there was loads of pain on behalf of people who are doing it. It is not you know it wasn’t that easy to take off, so I think that is something to be proud of. (P126, Female, Staff—Academic) I thought the study [research] was quite interesting so I guess the interest would drive me to continue doing the study. (P94, Female, Yr1, Student) | |
| Testing—Physical and Logistical Factors | Communication | Yes, it was good, we didn’t get told when we had negative results but then we got an email at the end of the day saying that anyone who was positive had been contacted so obviously you knew that you were negative. Erm which I think worked absolutely fine like I don’t think you need to be notified if you’re negative if there is a lot of people doing the study, I guess it takes a lot of time. (P121, Female, Yr1, Student) I think it would have been better if you got an email every time, just because then you’re kind of like well did they do my test? Or did I just… like you’re just unsure there is always a little thing in the back of your head like did it actually test negative? Or did my test not get there? (P101, Female, Yr5, Student) I don’t know about antibody’s but with regards to that I… we still haven’t heard. Antibody testing, I did the one in the second week, I didn’t do the first one and I didn’t do the last antibody but I did every other one and I haven’t got a clue if I had or haven’t had COVID at any point. I think they are lost in the system somewhere (P116, Female, Yr1, Student) |
| Physical testing | I thought it all worked very well and I know some people were worried about sticking swabs in various different places, I didn’t think there was any problem with that at all (P129, Male, Staff—Academic) I personally felt that actually, erm, doing different tests was very useful for students, because they will understand how the animals feel when they are having certain things done so that was definitely something which I even considered that they should be doing (P126, Female, Staff—Academic) You can’t really get around the whole finger pricking thing because I know some people just don’t like the whole needle, getting stabbed aspect of that but the spitting in to a tube is kind of disgusting but I think it is easier than like the whole swab in the back of your throat (P91, Female, Yr1, Student) | |
| Practicalities of testing | The location was convenient because it was sort of on our way to most of our practical sessions so if we happened to have a practical that day we could drop them off on the way... I think it was pretty much all positive, the only thing was the timings. It was a bit annoying rushing through like some lecture or like running over to put them in before the deadline” (P94, Female, Yr1, Student) The only issue that we had with it was like if we were on rotations, sometimes the tests wouldn’t be brought to the rotation site because they were supposed to be, but by our vet school they were supposed to deliver them to the rotation site because you couldn’t go to uni, do the test, drop it off and still get to your rotation on time. So that was the only kind of issue we had with it (P101, Female, Yr5, Student) I think once a week was OK to be fair (P121, Female, Yr1, Student) I think the weekly thing was just about right (P100, Male, Yr1, Student) | |
| Testing—Effects on Wellbeing | Improved Mental Wellbeing | I think it is just for kind of peace of mind it helped a bit, not having to worry about it all of the time and everyone said oh you’re going to university are you not worried? It was just kind of nice to know that there is awareness, and it is not just you know social distancing, you are actively trying to help as well I think. (P92, Female, Yr1, Student) I think [name 6] I just found it hugely reassuring, I was really, really keen to take part when I heard about that it was going to happen and I just… it made me feel well yes just that word it was just really reassuring to know that I was getting regularly tested and in a way I know you can’t directly say that everybody in my immediate family is OK but it was almost like I could act like the canary going down the mine and that there was a certain amount of reassurance as well that if I was negative there was a high chance that my children and my husband were also negative (P124, Female, Staff—Academic) |
| Behavioural change | I mean I guess testing negative maybe made me a bit more comfortable to go to like go and play football and things like that but I am not a massive sort of go out person anyway. I was only really sort of the gym and that so… I guess it is a more sort of like oh it is all right I can go play football with a group of people and stuff but again I think… it was like the prospect of a potential positive test the week after so I think overall I probably stayed about the same really. (P105, Male, Yr1, Student) It makes you kind of think more about who you’ve been in contact with, give people [unclear 15:04] tested positive then you’re suddenly a bit more aware of who you have met up with that week and stuff. Making sure that you are within the guidelines and not seeing more then the number of people you can be meeting with or households and things. Just in case (P104, Female, Yr1, Student) Yes, and if there was any social events on and if there was any lectures and stuff, I would just say well you can’t come in until you have had the test. I don’t know that sounds really and it is difficult because you can’t make someone have it but at the same time, why should that person put everyone else at an increased risk? (P102, Male, Yr5, Student) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, H.; Corner, J.; Cirelli, C.; Hassard, J.; Briggs, L.; Daly, J.M.; Bennett, M.; Chappell, J.G.; Fairclough, L.; McClure, C.P.; et al. Perceptions and Experiences of the University of Nottingham Pilot SARS-CoV-2 Asymptomatic Testing Service: A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 188. https://doi.org/10.3390/ijerph18010188
Blake H, Corner J, Cirelli C, Hassard J, Briggs L, Daly JM, Bennett M, Chappell JG, Fairclough L, McClure CP, et al. Perceptions and Experiences of the University of Nottingham Pilot SARS-CoV-2 Asymptomatic Testing Service: A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(1):188. https://doi.org/10.3390/ijerph18010188
Chicago/Turabian StyleBlake, Holly, Jessica Corner, Cecilia Cirelli, Juliet Hassard, Lydia Briggs, Janet M. Daly, Malcolm Bennett, Joseph G. Chappell, Lucy Fairclough, C. Patrick McClure, and et al. 2021. "Perceptions and Experiences of the University of Nottingham Pilot SARS-CoV-2 Asymptomatic Testing Service: A Mixed-Methods Study" International Journal of Environmental Research and Public Health 18, no. 1: 188. https://doi.org/10.3390/ijerph18010188
APA StyleBlake, H., Corner, J., Cirelli, C., Hassard, J., Briggs, L., Daly, J. M., Bennett, M., Chappell, J. G., Fairclough, L., McClure, C. P., Tarr, A., Tighe, P., Favier, A., Irving, W., & Ball, J. (2021). Perceptions and Experiences of the University of Nottingham Pilot SARS-CoV-2 Asymptomatic Testing Service: A Mixed-Methods Study. International Journal of Environmental Research and Public Health, 18(1), 188. https://doi.org/10.3390/ijerph18010188