A Systematic Literature Review of E-Cigarette-Related Illness and Injury: Not Just for the Respirologist

Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
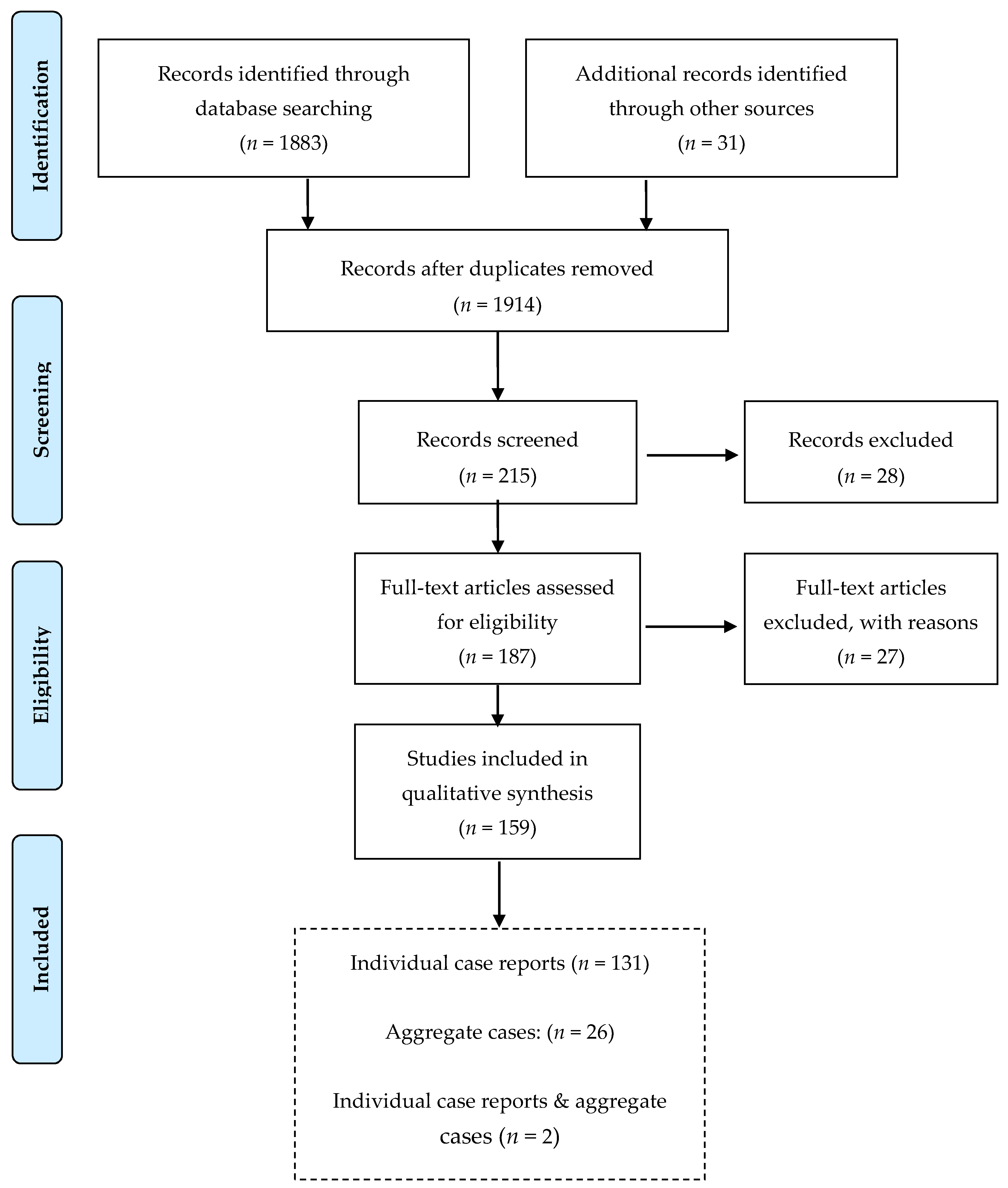
2.2. Search Results
2.3. Statistical Analysis
3. Results
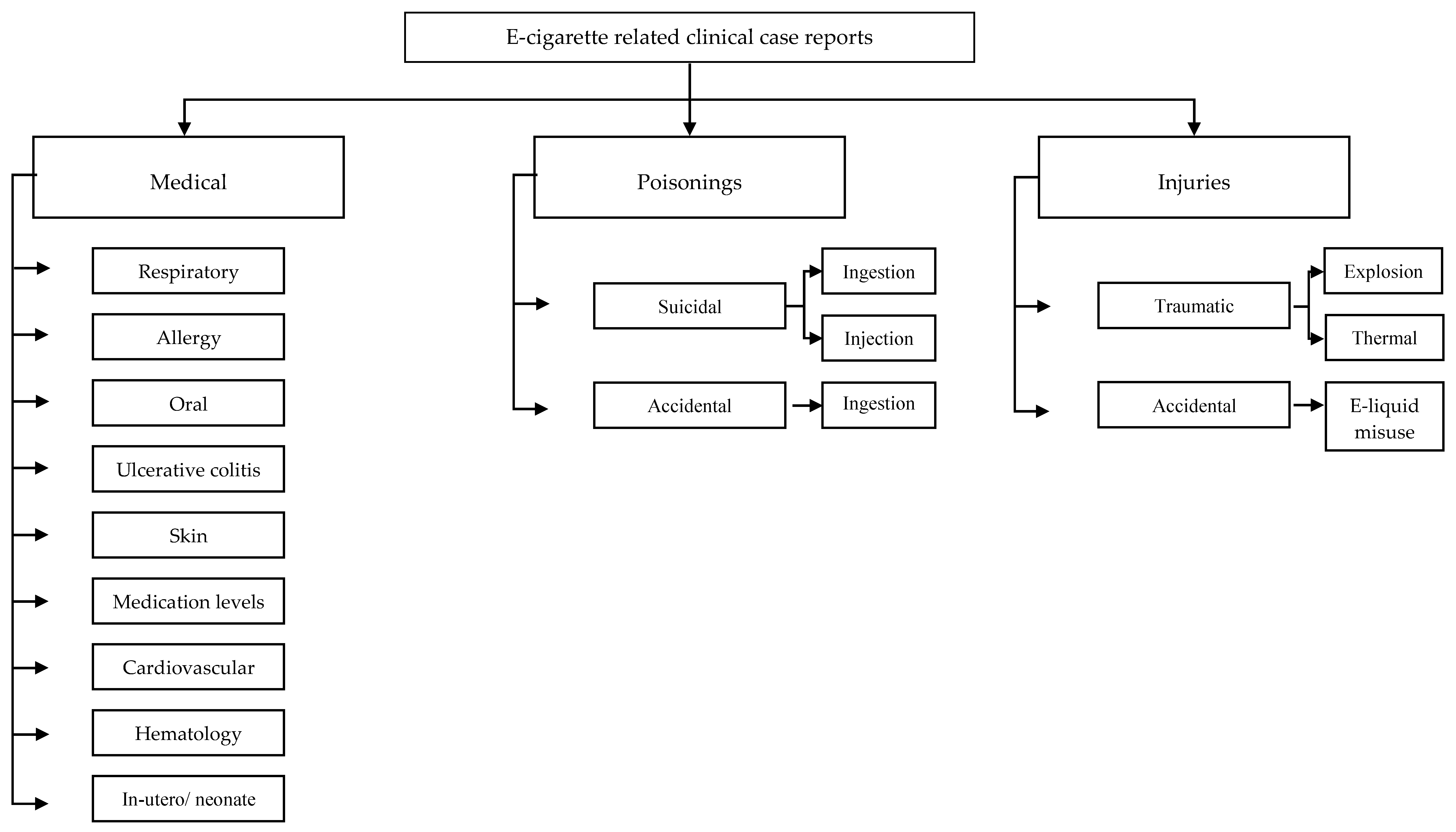
3.1. Classification of Cases
3.2. Respiratory
3.3. CDC Reports on Respiratory Cases
3.4. Traumatic Injury
3.5. Poisoning
3.6. Allergy
3.7. Effect on Medication Metabolism and Plasma Levels
3.8. Ulcerative Colitis
3.9. Misuse of E-liquid
3.10. Injury Caused by Falling with E-cigarette in Mouth
3.11. Additional Diagnoses and Health Effects Attributed to Electronic Cigarette Use
4. Discussion
4.1. Respiratory Injuries
4.2. Accidents
4.3. Poisonings
4.4. Substance Abuse
4.5. Seizures and Effect on Medication Metabolism
4.6. Regulatory Gap
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Patel, D.; Davis, K.; Cox, S.; Brian, B.; King, B.A.; Sfaher, P.; Caraballo, R.; Rebecca, B. Reasons for Current E-Cigarette Use among U.S. Adults. Prev. Med. 2016, 93, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Pinkston, R.; McLemore, B.; Dorsey, W.C.; Batra, S. Immunological and Toxicological Risk Assessment of E-Cigarettes. Eur. Respir. Rev. 2018, 27, 170119. [Google Scholar] [CrossRef] [PubMed]
- Kaisar, M.A.; Prasad, S.; Liles, T.; Cucullo, L. A Decade of E-Cigarettes: Limited Research & Unresolved Safety Concerns. Physiol. Behav. 2016, 365, 67–75. [Google Scholar] [CrossRef]
- Fernández, E.; Fu, M.; Martinez-Sanchez, J. Exposure to Aerosol from Smoking-Proxy Electronic Inhaling Systems: A Systematic Review. World Heal. Organ. Tob. Free Initiave 2016, 1–70. [Google Scholar]
- Fernández, E.; Ballbè, M.; Sureda, X.; Fu, M.; Saltó, E.; Martínez-Sánchez, J.M. Particulate Matter from Electronic Cigarettes and Conventional Cigarettes: A Systematic Review and Observational Study. Curr. Environ. Heal. Rep. 2015, 2, 423–429. [Google Scholar] [CrossRef]
- Ghinai, I.; Pray, I.W.; Navon, L.; Laughlin, K.O.; Saathoff-huber, L.; Hoots, B.; Kimball, A.; Tenforde, M.W.; Chevinsky, J.R.; Layer, M.; et al. E-Cigarette Product Use, or Vaping, Among Persons with Associated Lung Injury—Illinois and Wisconsin, April—September 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Stratton, K.; Kwan, L.Y.; Eaton, D.L. Public Health Consequences of E-Cigarettes: A Consesus Study Report of the National Academies of Sciences, Health, Medicine. J. Public Health Policy 2018, 39, 379–381. [Google Scholar] [CrossRef]
- Jenssen, B.P.; Boykan, R. Electronic Cigarettes and Youth in the United States: A Call to Action (at the Local, National and Global Levels). Children 2019, 6, 30. [Google Scholar] [CrossRef]
- Pisinger, C.; Døssing, M. A Systematic Review of Health Effects of Electronic Cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef]
- Hua, M.; Talbot, P. Potential Health Effects of Electronic Cigarettes: A Systematic Review of Case Reports. Prev. Med. Rep. 2016, 4, 169–178. [Google Scholar] [CrossRef]
- McCauley, L.; Markin, C.; Hosmer, D. An Unexpected Consequence of Electronic Cigarette Use. Chest 2012, 141, 1110–1113. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Girvalaki, C.; Filippidis, F.T.; Oder, M.; Kastanje, R.; De Vries, I.; Scholtens, L.; Annas, A.; Plackova, S.; Turk, R.; et al. Characteristics and Outcomes of E-Cigarette Exposure Incidents Reported to 10 European Poison Centers: A Retrospective Data Analysis. Tob. Induc. Dis. 2017, 15, 2010–2013. [Google Scholar] [CrossRef] [PubMed]
- Vakkalanka, J.P.; Hardison, L.S.; Holstege, C.P. Epidemiological Trends in Electronic Cigarette Exposures Reported to U.S. Poison Centers. Clin. Toxicol. 2014, 52, 542–548. [Google Scholar] [CrossRef]
- ICD-10-CM Official Coding Guidelines—Supplement Coding Encounters Related to E-Cigarette, or Vaping, Product Use; ICD-10-CM Coding Guidance Vaping related disorders; Centers for Disease Control and Prevention; Available online: https://www.cdc.gov/nchs/data/icd/Vapingcodingguidance2019_10_17_2019.pdf (accessed on 17 October 2019).
- Siegel, D.A.; Jatlaoui, T.C.; Koumans, E.H.; Kiernan, E.A.; Layer, M.; Cates, J.E.; Kimball, A.; Weissman, D.N.; Petersen, E.E.; Reagan-Steiner, S.; et al. Update: Interim Guidance for Health Care Providers Evaluating and Caring for Patients with Suspected E-Cigarette, or Vaping, Product Use Associated Lung Injury—United States, October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 919–927. [Google Scholar] [CrossRef] [PubMed]
- 2019 Lung Injury Surveillance Primary Case Definitions; U.S. Department of Health and Human Services: Washington, DC, USA; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Ghinai, I.; Navon, L.; Gunn, J.K.L.; Duca, L.M.; Brister, S.; Love, S.; Brink, R. Characteristics of Persons Who Report Using Only Nicotine-Containing Products Among Interviewed Patients with E-Cigarette, or Vaping, Product Use—Associated Lung Injury—Illinois, August—December 2019. Morb. Mortal. Wkly. Rep. 2020, 69, 84–89. [Google Scholar] [CrossRef]
- Chalmers, S.; Von Buchwald, C.L.; Gajic, O. VpALI—Vaping-Related Acute Lung Injury: A New Killer Around the Block. Mayo Clin. Proc. 2019, 1–12. [Google Scholar] [CrossRef]
- Gotts, J.E.; Jordt, S.-E.; McConnell, R.; Tarran, R. What Are the Respiratory Effects of E-Cigarettes? BMJ 2019, 366, l5275. [Google Scholar] [CrossRef]
- Maessen, G.C.; Wijnhoven, A.M.; Neijzen, R.L.; Paulus, M.C.; van Heel, D.A.M.; Bomers, B.H.A.; Boersma, L.E.; Konya, B.; van der Heyden, M.A.G. Nicotine Intoxication by E-Cigarette Liquids: A Study of Case Reports and Pathophysiology. Clin. Toxicol. 2019, 58, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Seitz, C.M.S.; Kabir, Z. Burn Injuries Caused by E-Cigarette Explosions: A Systematic Review of Published Cases. Tob. Prev. Cessat. 2018, 4, 1–8. [Google Scholar] [CrossRef]
- Arnaout, A.; Khashaba, H.; Dobbs, T.; Dewi, F.; Pope-Jones, S.; Sack, A.; Estela, C.; Nguyen, D. The Southwest UK Burns Network (SWUK) Experience of Electronic Cigarette Explosions and Review of Literature. Burns 2017, 43, e1–e6. [Google Scholar] [CrossRef]
- Henry, T.S.; Kligerman, S.J.; Raptis, C.A.; Mann, H.; Sechrist, J.W.; Kanne, J.P. Imaging Findings of Vaping-Associated Lung Injury. Am. J. Roentgenol. 2020, 214, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Butt, Y.M.; Smith, M.L.; Tazelaar, H.D.; Vaszar, L.T.; Swanson, K.L.; Cecchini, M.J.; Boland, J.M.; Bois, M.C.; Boyum, J.H.; Froemming, A.T.; et al. Pathology of Vaping-Associated Lung Injury. N. Engl. J. Med. 2019, 381, 1780–1781. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Boloña, E.; Felix, M.; Vanegas, E.; Vera Paz, C.; Cherrez Ojeda, I. A Case of Vaping Associated Pulmonary Illness in South America: Highlighting the Need for Awareness and Surveillance Programs in the Region. Am. J. Respir. Crit. Care Med. Ja 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tan, Q.; Saccone, N.M.; Lindner, D.H. A Case of Vaping TCH Oil Leading to Vaping Associated Pulmonary Injury: Our Approach to Its Diagnosis, Management, and Recommendations. Case Rep. Pulmonol. 2020. [Google Scholar] [CrossRef]
- Abeles, M.; Popofsky, S.; Wen, A.; Valsamis, C.; Webb, A.; Halaby, C.; Pirzada, M. Vaping-Associated Lung Injury Caused by Inhalation of Cannabis Oil. Pediatr. Pulmonol. 2019, 55, 226–228. [Google Scholar] [CrossRef]
- Buus, D.; Alzoubaidi, M.; Jamous, F. Vaping Induced Lung Injury: A Case Report. South Dakota Med. 2019, 72, 446–449. [Google Scholar]
- Casanova, G.S.; Amaro, R.; Soler, N.; Sánchez, M.; Badía, J.R.; Barberà, A.; Agustí, A. An Imported Case of E-Cigarette or Vaping Associated Lung Injury (EVALI) in Barcelona. Eur. Respir. J. 2019, 55, 1902076. [Google Scholar] [CrossRef]
- Pokhrel, K.; Goldman, C.; Smith, T.C.; Smith, T.C. Cannabinoid Oil Vaping Associated Lung Injury and Its Radiographic Appearance. Am. J. Med. 2019. [Google Scholar] [CrossRef]
- Ocampo-Gonzalez, F.A.; Park, J.W. Cytologic Features of Vaping-Induced Lung Injury: A Case Report. Diagn. Cytopathol. 2019, 1–3. [Google Scholar] [CrossRef]
- Itoh, M.; Aoshiba, K.; Herai, Y.; Nakamura, H.; Takemura, T. Lung Injury Associated with Electronic Cigarettes Inhalation Diagnosed by Transbronchial Lung Biopsy. Respirol. Case Rep. 2018, 6, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Qarajeh, R.; Kitchen, J. THC Vaping-Induced Acute Respiratory Distress Syndrome. Am. J. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Aftab, G.; Mudassar, A.; Douglas, F. Vaping-Associated Lung Injury. Cureus 2019. [Google Scholar] [CrossRef]
- Sakla, N.; Gattu, R.; Singh, G.; Sadler, M. Vaping-Associated Acute Respiratory Distress Syndrome. Emerg. Radiol. 2019, 27, 103–106. [Google Scholar] [CrossRef]
- Sharma, M.; Anjum, H.; Bulathsinghala, C.P.; Buch, M.; Surani, S.R. A Case Report of Secondary Spontaneous Pneumothorax Induced by Vape. Cureous 2019, 11. [Google Scholar] [CrossRef]
- He, T.; Oks, M.; Esposito, M.; Steinberg, H.; Makaryus, M. “Tree-in-Bloom”: Severe Acute Lung Injury Induced by Vaping Cannabis Oil. Ann. Am. Thoracic Soc. 2017, 14, 468–470. [Google Scholar] [CrossRef]
- Landman, S.T.; Dhaliwal, I.; Mackenzie, C.A.; Martinu, T.; Steele, A.; Bosma, K.J. Life-Threatening Bronchiolitis Related to Electronic Cigarette Use in a Canadian Youth. CMAJ 2019, 191, E1321–E1331. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Mehrad, M.; Dammert, P.; Arrossi, A.V.; Sarda, R.; Brenner, D.S.; Maldonado, F.; Choi, H.; Ghobrial, M. Lung Biopsy Findings in Severe Pulmonary Illness Associated with E-Cigarette Use (Vaping). Am. J. Clin. Pathol. 2019, 153, 30–39. [Google Scholar] [CrossRef]
- Khan, M.S.; Khateeb, F.; Akhtar, J.; Khan, Z.; Lal, A.; Kholodovych, V.; Hammersley, J. Organizing Pneumonia Related to Electronic Cigarette Use: A Case Report and Review of Literature. Clin. Respir. J. 2018, 12, 1295–1299. [Google Scholar] [CrossRef]
- Layden, J.E.; Ghinai, I.; Pray, I.; Kimball, A.; Layer, M.; Tenforde, M.; Navon, L.; Hoots, B.; Salvatore, P.P.; Elderbrook, M.; et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin—Preliminary Report. N. Engl. J. Med. 2019, 1–14. [Google Scholar] [CrossRef]
- Flower, M.; Nandakumar, L.; Singh, M.; Wyld, D.; Windsor, M.; Fielding, D. Respiratory Bronchiolitis-Associated Interstitial Lung Disease Secondary to Electronic Nicotine Delivery System Use Confirmed with Open Lung Biopsy. Respirol. Case Rep. 2017, 5, 3–5. [Google Scholar] [CrossRef]
- Lu, M.A.; Jabre, N.A.; Mogayzel, P.J., Jr. Vaping-Related Lung Injury in an Adolescent. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef]
- Mantilla, R.D.; Darnell, R.T.; Sofi, U. Vapor Lung: Bronchiolitis Obliterans Organizing Pneumonia (BOOP) in Patient with E-Cigarette Use; American Thoracic Society Conferences, USA Publisher: Philadelphia, PA, USA, 2016. [Google Scholar]
- Ansari-Gilani, K.; Petraszko, A.M.; Teba, C.V.; Reeves, A.R.; Gupta, A.; Gupta, A.; Ramaiya, N.H.; Gilkeson, R.C. E-Cigarette Use Related Lung Disease, Review of Clinical and Imaging Findings in 3 Cases. Hear. Lung 2020, 1–5. [Google Scholar] [CrossRef]
- Modi, S.; Sangani, R.; Alhajhusain, A. Acute Lipoid Pneumonia Secondary to E-Cigarettes Use: An Unlikely Replacement for Cigarettes. Chest 2015, 148, 382A. [Google Scholar] [CrossRef]
- Abbara, S.; Fernando, M.; Kay, U. Electronic Cigarette or Vaping-Associated Lung Injury (EVALI): The Tip of the Iceberg. Radiol. Cardiothorac. Imaging 2019, 1, e190212. [Google Scholar] [CrossRef]
- Maddock, S.D.; Cirulis, M.M.; Callahan, S.J.; Keenan, L.M.; Pirozzi, C.S.; Raman, S.M.; Aberegg, S.K. Pulmonary Lipid-Laden Macrophages and Vaping. N. E. J. Med. 2019, 381, 1488–1489. [Google Scholar] [CrossRef]
- Viswam, D.; Trotter, S.; Burge, P.S.; Walters, G.I. Respiratory Failure Caused by Lipoid Pneumonia from Vaping E-Cigarettes. BMJ Case Rep. 2018, 2018, 1–4. [Google Scholar] [CrossRef]
- Dicpinigaitis, P.V.; Trachuk, P.; Fakier, F.; Teka, M.; Suhrland, M.J. Vaping - Associated Acute Respiratory Failure Due to Acute Lipoid Pneumonia. Lung 2019, 10–12. [Google Scholar] [CrossRef]
- Bonilla, A.; Blair, A.J.; Alamro, S.M.; Ward, R.A.; Feldman, M.B.; Dutko, R.A.; Karagounis, T.K.; Johnson, A.L.; Folch, E.E.; Vyas, J.M. Recurrent Spontaneous Pneumothoraces and Vaping in an 18-Year-Old Man: A Case Report and Review of the Literature. J. Med. Case Rep. 2019, 13, 4–9. [Google Scholar] [CrossRef]
- Lo, T. Vaping and Tension Pneumothorax: A Life-Threatening Association; American Thoracic Society Conferences: Philadelphia, PA, USA, 2017. [Google Scholar]
- Skertich, N.J.; Sullivan, G.A.; Madonna, M.B.; Shah, A.N. Vaping Is a Risk Factor for Spontaneous Pneumothorax: Two Cases. J. Pediatr. Surg. Case Rep. 2019, 50, 101305. [Google Scholar] [CrossRef]
- Bradford, L.E.; Rebuli, M.E.; Ring, B.J.; Jaspers, I.; Clement, K.C.; Loughlin, C.E. Danger in the Vapor? ECMO for Adolescents with Status Asthmaticus after Vaping. J. Asthma 2019, 1–5. [Google Scholar] [CrossRef]
- Arter, Z.L.; Wiggins, A.; Hudspath, C.; Kisling, A.; Hostler, D.C.; Hostler, J.M. Acute Eosinophilic Pneumonia Following Electronic Cigarette Use. Respir. Med. Case Rep. 2019, 27, 100825. [Google Scholar] [CrossRef]
- Thota, D.; Latham, E. Case Report of Electronic Cigarettes Possibly Associated with Eosinophilic Pneumonitis in a Previously Healthy Active-Duty Sailor. J. Emerg. Med. 2014, 47, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Salzman, G.A.; Alqawasma, M.; Asad, H. Vaping Associated Lung Injury (EVALi): An Explosive United States Epidemic. Mo. Med. 2019, 116, 492–496. [Google Scholar] [PubMed]
- Antwi-Amoabeng, D.; Islam, R. Vaping Is Not Safe: A Case of Acute Eosinophilic Pneumonia Following Cannabis Vapor Inhalation. Case Rep. Pulmonol. 2020. [Google Scholar] [CrossRef]
- Sommerfeld, C.G.; Weiner, D.J.; Nowalk, A.; Larkin, A. Hypersensitivity Pneumonitis and Acute Respiratory Distress Syndrome from E-Cigarette Use. Pediatrics 2018, 141. [Google Scholar] [CrossRef]
- Attis, M.; King, J.; Hardison, D.; Bridges, B. The Journey to ECMO Could Start with a Single Vape: A Case of Severe Hypersensitivity Pneumonitis in a Pediatric Patient. ASAIO 2018, 14. [Google Scholar] [CrossRef]
- Agustin, M.; Yamamoto, M.; Cabrera, F.; Eusebio, R. Diffuse Alveolar Hemorrhage Induced by Vaping. Case Rep. Pulmonol. 2018, 2018, 1–3. [Google Scholar] [CrossRef]
- Gutsche, J.; Pasternak, R.; Campbell, D.; Schili, J.L.; Boyle, P.J.; Tilney, P. A 19-Year-Old Man with Vaping-Associated Lung Injury. Air Med. J. 2020, 39, 6–8. [Google Scholar] [CrossRef]
- Youmans, A.J.; Harwood, J. Gross and Histopathological Findings in the First Reported Vaping-Induced Lung Injury Death in the United States. Am. J. ForensicMed. Pathol. 2020, 41, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bozzella, M.J.; Magyar, M.; DeBiasi, R.L.; Ferrer, K. Epiglottitis Associated With Intermittent E-Cigarette Use: The Vagaries of Vaping Toxicity. Pediatrics 2020, 145, e20192399. [Google Scholar] [CrossRef] [PubMed]
- Thakrar, P.D.; Boyd, K.P.; Swanson, C.P.; Wideburg, E.; Kumbhar, S.S. E-Cigarette, or Vaping, Product Use-Associated Lung Injury in Adolescents: A Review of Imaging Features. Pediatr. Radiol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllou, G.A.; Tiberio, P.J.; Zou, R.H.; Lamberty, P.E.; Lynch, M.J.; Kreit, J.W.; Gladwin, M.T.; Morris, A.; Chiarchiaro, J. Vaping-Associated Acute Lung Injury: A Case Series. Am. J. Respir. Crit. Care Med. 2019, 200, 1430–1431. [Google Scholar] [CrossRef] [PubMed]
- Kalininskiy, A.; Bach, C.T.; Nacca, N.E.; Ginsberg, G.; Marraffa, J.; Navarette, K.A.; McGraw, M.D.; Croft, D.P. E-Cigarette, or Vaping, Product Use Associated Lung Injury (EVALI): Case Series and Diagnostic Approach. Lancet. Respir. Med. 2019, 7, 1017–1026. [Google Scholar] [CrossRef]
- Henry, T.S.; Kanne, J.P.; Kligerman, S.J. Imaging of Vaping-Associated Lung Disease. N. Engl. J. Med. 2019, 381, 1486–1487. [Google Scholar] [CrossRef]
- Zou, R.H.; Tiberio, P.J.; Ph, D.; Kreit, J.W. Clinical Characterization of E-Cigarette, or Vaping, Product Use Associated Lung Injury in 36 Patients in Pittsburgh, PA. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef]
- Blagev, D.P.; Harris, D.; Dunn, A.C.; Guidry, D.W.; Grissom, C.K.; Lanspa, M.J. Clinical Presentation, Treatment, and Short-Term Outcomes of Lung Injury Associated with e-Cigarettes or Vaping: A Prospective Observational Cohort Study. Lancet 2019, 6736, 1–11. [Google Scholar] [CrossRef]
- Schier, J.G.; Meiman, J.G.; Layden, J.; Mikosz, C.A.; Vanfrank, B.; King, B.A. Severe Pulmonary Disease Associated with Electronic-Cigarette–Product Use—Interim Guidance. Morb. Mortal. Wkly. Rep. Sev. 2019, 68, 787–790. [Google Scholar] [CrossRef]
- Siegel, D.A.; Jatlaoui, T.C.; Koumans, E.H.; Kiernan, E.A.; Layer, M.; Cates, J.E.; Kimball, A.; Weissman, D.N.; Petersen, E.E.; Reagan-Steiner, S.; et al. Update: Interim Guidance for Health Care Providers for Managing Patients with Suspected E-Cigarette, or Vaping, Product Use—Associated Lung Injury—United States, November 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1081–1086. [Google Scholar] [CrossRef]
- Evans, M.E.; Twentyman, E.; Click, E.S.; Goodman, A.B. Update: Interim Guidance for Health Care Professionals Evaluating and Caring for Patients with Suspected E-Cigarette, or Vaping, Product Use—Associated Lung Injury and for Reducing the Risk for Rehospitalization and Death Following Hospital Discharge. Morb. Mortal. Wkly. Rep. 2020, 68, 1189–1194. [Google Scholar] [CrossRef]
- Perrine, C.G.; Pickens, C.M.; Boehmer, T.K.; King, B.A.; Jones, C.M. Characteristics of a Multistate Outbreak of Lung Injury Associated with E-Cigarette Use, or Vaping—United States, 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Lewis, N.; McCaffrey, K.; Sage, K.; Cheng, C.J.; Green, J.; Goldstein, L.; Campbell, H.; Ferrell, D.; Malan, N.; LaCross, N.; et al. E-Cigarette Use, or Vaping, Practices and Characteristics Among Persons with Associated Lung Injury—Utah, April-October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 953–956. [Google Scholar] [CrossRef] [PubMed]
- Moritz, E.D.; Zapata, L.B.; Lekiachvili, A.; Glidden, E.; Annor, F.B.; Werner, A.K.; Ussery, E.N.; Hughes, M.M.; Kimball, A.; DeSisto, C.L.; et al. Update: Characteristics of Patients in a National Outbreak of E-Cigarette, or Vaping, Product Use-Associated Lung Injuries—United States, October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 985–989. [Google Scholar] [CrossRef]
- Chatham-Stephens, K.; Roguski, K.; Jang, Y.; Cho, P.; Jatlaoui, T.C.; Kabbani, S.; Glidden, E.; Ussery, E.N.; Trivers, K.F.; Evans, M.E.; et al. Characteristics of Hospitalized and Nonhospitalized Patients in a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use–Associated Lung Injury—United States, November 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Wiens, T.; Peterson, J.; Saravia, S.; Lunda, M.; Hanson, K.; Wogen, M.; D’Heilly, P.; Margetta, J.; Bye, M.; et al. Characteristics of E-Cigarette, or Vaping, Products Used by Patients with Associated Lung Injury and Products Seized by Law Enforcement—Minnesota, 2018 and 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- Lozier, M.J.; Wallace, B.; Anderson, K.; Ellington, S.; Jones, C.M. Update: Demographic, Product, and Substance-Use Characteristics of Hospitalized Patients in a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use—Associated Lung Injuries—United States, December 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1142–1148. [Google Scholar] [CrossRef]
- Gaub, K.L.; Hallyburton, S.; Samanic, C.; Paddack, D.; Clark, C.R.; Pence, S.; Brown, J.A.; Hawkins, E. Patient Characteristics and Product Use Behaviors Among Persons with E-Cigarette, or Vaping, Product Use-Associated Lung Injury-Indiana, June–October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1139–1141. [Google Scholar] [CrossRef]
- Mikosz, C.A.; Danielson, M.; Anderson, K.N.; Pollack, L.A.; Currie, D.W.; Njai, R. Characteristics of Patients Experiencing Rehospitalization or Death After Hospital Discharge in a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use—Associated Lung Injury—United States, 2019. Morb. Mortal. Wkly. Rep. 2020, 68, 1183–1188. [Google Scholar] [CrossRef]
- Lozier, M.J.; Wallace, B.; Anderson, K.; Ellington, S.; Jones, C.M.; Rose, D.; Baldwin, G.; King, B.A.; Briss, P.; Mikosz, C.A. Update: Product, Substance-Use, and Demographic Characteristics of Hospitalized Patients in a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use—Associated Lung Injury—United States, August 2019–January 2020. Morb. Mortal. Wkly. Rep. 2019, 69, 44–49. [Google Scholar] [CrossRef]
- He, T.; Oks, M.; Esposito, M.; Steinberg, H.; Makaryus, M. Outbreak of Electronic-Cigarette—Associated Acute Lipoid Pneumonia—North Carolina, July–August 2019. Morb. Mortal. Wkly. Rep. 2019, 68. [Google Scholar] [CrossRef]
- Navon, L.; Jones, C.M.; Ghinai, I.; King, B.A.; Briss, P.A.; Hacker, K.A.; Layden, J.E. Risk Factors for E-Cigarette, or Vaping, Product Use-Associated Lung Injury (EVALI) Among Adults Who Use E-Cigarette, or Vaping, Products-Illinois, July-October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Blount, B.C.; Karwowski, M.P.; Morel-Espinosa, M.; Rees, J.; Sosnoff, C.; Cowan, E.; Gardner, M.; Wang, L.; Valentin-Blasini, L.; Silva, L.; et al. Evaluation of Bronchoalveolar Lavage Fluid from Patients in an Outbreak of E-Cigarette, or Vaping, Product Use-Associated Lung Injury-10 States, August-October 2019. Morb. Mortal. Wkly. Rep. 2019, 68, 1040–1041. [Google Scholar] [CrossRef]
- Krishnasamy, V.P.; Hallowell, B.D.; Ko, J.Y.; Board, A.; Hartnett, K.P.; Salvatore, P.P.; Melstrom, P.; Haag, B.; King, B.A.; Briss, P.; et al. Update: Characteristics of a Nationwide Outbreak of E-Cigarette, or Vaping, Product Use—Associated Lung Injury—United States, August 2019–January 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 90–94. [Google Scholar] [CrossRef]
- Moore, J.; Mihalache, G.; Messahel, A. “Exploding” Electronic Cigarette: A Case Report. Br. J. Oral Maxillofac. Surg. 2016, 54, 1056–1057. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.J.S.; Eshraghi, N.; Kemalyan, N.A.; Mueller, C. Electronic Cigarette Burns: A Case Series. Trauma 2018, 21, 103–106. [Google Scholar] [CrossRef]
- Brooks, J.K.; Kleinman, J.W.; Brooks, J.B.; Reynolds, M.A. Electronic Cigarette Explosion Associated with Extensive Intraoral Injuries. Dent. Traumatol. 2016, 33, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Kumetz, E.A.; Hurst, N.D.; Cudnik, R.J.; Rudinsky, S.L. Electronic Cigarette Explosion Injuries. Am. J. Emerg. Med. 2016, 34, 2252.e1–2252.e3. [Google Scholar] [CrossRef] [PubMed]
- Norii, T.; Plate, A. Electronic Cigarette Explosion Resulting in a C1 and C2 Fracture: A Case Report. J. Emerg. Med. 2016, 52, 86–88. [Google Scholar] [CrossRef]
- Harrison, R.; Hicklin, D. Electronic Cigarette Explosions Involving the Oral Cavity. J. Am. Dent. Assoc. 2016, 147, 891–896. [Google Scholar] [CrossRef]
- Smith, S.L.; Smith, C.; Cheatham, M.; Smith, H.G. Electronic Cigarettes: A Burn Case Series. J. Nurse Pract. 2017, 13, 693–699. [Google Scholar] [CrossRef]
- Shastry, S.; Langdorf, M.I. Electronic Vapor Cigarette Battery Explosion Causing Shotgun-like Superficial Wounds and Contusion. West. J. Emerg. Med. 2016, 17, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Vaught, B.; Spellman, J.; Shah, A.; Stewart, A.; Mullin, D. Facial Trauma Caused by Electronic Cigarette Explosion. Ear Nose Throat J. 2017, 96, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Khairudin, M.N.; Zahidin, A.Z.M.; Bastion, M.L.C. Front to Back Ocular Injury from a Vaping-Related Explosion. BMJ Case Rep. 2016, 2016, 1–4. [Google Scholar] [CrossRef]
- Foran, I.; Oak, N.R.; Meunier, M.J. High-Pressure Injection Injury Caused by Electronic Cigarette Explosion: A Case Report. JBJS Case Connect. 2017, 7, e36. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, N.; Beavers, K.; Yu, A.; Gardner, K. 2016: ELECTRONIC CIGARETTES AND THERMAL INJURY: A CASE REPORT ON THE DANGERS OF VAPING. Crit. Care Med. 2016, 44, 578. [Google Scholar] [CrossRef]
- Colaianni, C.A.; Tapias, L.F.; Cauley, R.; Sheridan, R.; Schulz, J.T.; Goverman, J. Injuries Caused by Explosion of Electronic Cigarette Devices; Interesting Case, 2016; 16: ic9; 2016; Available online: www.ePlasty.com (accessed on 29 February 2016).
- Cason, D.E.; Morgan, D.E.; Pietryga, J.A. Injuries from an Exploding E-Cigarette: A Case Report. Ann. Intern. Med. 2016, 165, 678–679. [Google Scholar] [CrossRef]
- Katz, M.G.; Russell, K.W. Injury from E-Cigarette Explosion. N. Engl. J. Med. 2019, 380, 2460. [Google Scholar] [CrossRef]
- Rogér, J.M.; Abayon, M.; Elad, S.; Kolokythas, A. Oral Trauma and Tooth Avulsion Following Explosion of E-Cigarette. J. Oral Maxillofac. Surg. 2016, 74, 1181–1185. [Google Scholar] [CrossRef]
- Jiwani, A.Z.; Williams, J.F.; Rizzo, J.A.; Chung, K.K.; King, B.T.; Cancio, L.C. Thermal Injury Patterns Associated with Electronic Cigarettes. Int. J. Burns Trauma 2017, 7, 1–5. [Google Scholar]
- Maraqa, T.; Mohamed, M.A.T.; Salib, M.; Morris, S.; Mercer, L.; Sachwani-Daswani, G.R. Too Hot for Your Pocket! Burns from E-Cigarette Lithium Battery Explosions: A Case Series. J. Burn Care Res. 2018, 39, 1043–1047. [Google Scholar] [CrossRef]
- Ackley, E.; Williams, J.T.B.; Kunrath, C.; Monson, M.; Ignatiuk, A.; Gaensbauer, J. Too Hot to Handle? When Vaporizers Explode. J. Pediatr. 2018, 196, 320.e1. [Google Scholar] [CrossRef]
- Chi, A.C.; Neville, B.W.; Ravenel, M. Electronic Cigarette Explosion: Case Report of an Emerging Cause of Orofacial Trauma. Trauma 2018, 20, 62–67. [Google Scholar] [CrossRef]
- Patterson, S.B.; Beckett, A.R.; Lintner, A.; Leahey, C.; Greer, A.; Brevard, S.B.; Simmons, J.D.; Kahn, S.A. A Novel Classification System for Injuries after Electronic Cigarette Explosions. J. Burn Care Res. 2016, 38, e95–e100. [Google Scholar] [CrossRef]
- Anderson, H.; Richie, C.; Bernard, A. A Surprisingly Volatile Smoking Alternative: Explosion and Burns as Risks of E-Cigarette Use. J. Burn Care Res. 2017, 38, e884. [Google Scholar] [CrossRef] [PubMed]
- Ban, C.; Krishnan, D.G.; Abdallah, Y. Ballistic Trauma from an Exploding Electronic Cigarette: Case Report. Oral Maxillofac. Surg. Cases 2017, 3, 61–63. [Google Scholar] [CrossRef]
- Kite, A.C.; Le, B.Q.; Cumpston, K.L.; Hieger, M.A.; Feldman, M.J.; Pozez, A.L. Blast Injuries Caused by Vape Devices 2 Case Reports. Ann. Plast. Surg. 2016, 77, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Paley, G.L.; Echalier, E.; Eck, T.W.; Hong, A.R.; Farooq, A.V.; Gregory, D.G.; Lubniewski, A.J. Corneoscleral Laceration and Ocular Burns Caused by Electronic Cigarette Explosions. Cornea 2016, 35, 1015–1018. [Google Scholar] [CrossRef]
- Herlin, C.; Bekara, F.; Bertheuil, N.; Frobert, P.; Carloni, R.; Chaput, B. Deep Burns Caused by Electronic Vaping Devices Explosion. Burns 2016, 42, 1875–1877. [Google Scholar] [CrossRef]
- Archambeau, B.A.; Young, S.; Lee, C.; Pennington, T.; Vanderbeek, C.; Miulli, D.; Culhane, J.; Neeki, M. E-Cigarette Blast Injury: Complex Facial Fractures and Pneumocephalus. West. J. Emerg. Med. 2016, 17, 805–807. [Google Scholar] [CrossRef]
- Quiroga, L.; Asif, M.; Lagziel, T.; Bhat, D.; Caffrey, J. E-Cigarette Battery Explosions: Review of the Acute Management of the Burns and the Impact on Our Population. Cureus 2019, 11. [Google Scholar] [CrossRef]
- Treitl, D.; Solomon, R.; Davare, D.L.; Sanchez, R.; Kiffin, C. Full and Partial Thickness Burns from Spontaneous Combustion of E-Cigarette Lithium-Ion Batteries with Review of Literature. J. Emerg. Med. 2017, 53, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, K.J.; Rose, A.M.; Khan, M.A.A.; Quaba, O.; Lowrie, A.G. Thigh Burns from Exploding E-Cigarette Lithium Ion Batteries: First Case Series. Burns 2016, 42, e42–e46. [Google Scholar] [CrossRef] [PubMed]
- Hickey, S.; Goverman, J.; Friedstat, J.; Sheridan, R.; Schulz, J. Thermal Injuries from Exploding Electronic Cigarettes. Burns 2018, 44, 1294–1301. [Google Scholar] [CrossRef]
- Harshman, J.; Vojvodic, M.; Rogers, A.D. Burns Associated with E-Cigarette Batteries: A Case Series and Literature Review. Can. J. Emerg. Med. 2018, 20, S20–S28. [Google Scholar] [CrossRef]
- Bauman, Z.M.; Roman, J.; Singer, M.; Vercruysse, G.A. Canary in the Coal Mine—Initial Reports of Thermal Injury Secondary to Electronic Cigarettes. Burns 2017, 43, e38–e42. [Google Scholar] [CrossRef]
- Walsh, K.; Sheikh, Z.; Johal, K.; Khwaja, N. Rare Case of Accidental Fire and Burns Caused by E-Cigarette Batteries. BMJ Case Rep. 2016, 2016, 2015–2017. [Google Scholar] [CrossRef]
- Jablow, L.M.; Sexton, R.J. Spontaneous Electronic Cigarette Explosion: A Case Report. Am. J. Med. Case Reports 2015, 3, 93–94. [Google Scholar] [CrossRef][Green Version]
- Sheckter, C.; Chattopadhyay, A.; Paro, J.; Karanas, Y. Burns Resulting from Spontaneous Combustion of Electronic Cigarettes: A Case Series. Burn. Trauma 2016, 4, 4–7. [Google Scholar] [CrossRef]
- Michael, R.; Ebraheim, N.; Maier, J.; Tanios, M.; Kouri, A. Electronic Cigarette Burns: A Case Report and Review of Current Literature. Case Rep. Orthop. 2019, 2019, 1–5. [Google Scholar] [CrossRef]
- Serror, K.; Chaouat, M.; De Runz, A.; Mimoun, M.; Boccara, D. Thigh Deep Burns Caused by Electronic Vaping Devices (e-Cigarettes): A New Mechanism. Burns 2017, 43, 1133–1135. [Google Scholar] [CrossRef]
- Bohr, S.; Almarzouqi, F.; Pallua, N. Extensive Burn Injury Caused by Fundamental Electronic Cigarette Design Flaw. Ann. Burns Fire Disasters 2016, 29, 231–233. [Google Scholar] [PubMed]
- Satteson, E.S.; Walker, N.J.; Tuohy, C.J.; Molnar, J.A. Extensive Hand Thermal and Blast Injury from Electronic Cigarette Explosion: A Case Report. Hand 2018. [Google Scholar] [CrossRef] [PubMed]
- Arnaout, A.; Dewi, F.; Nguyen, D. Re: Burn Injuries from Exploding Electronic Cigarette Batteries: An Emerging Public Health Hazard. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 981–982. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.; Anwar, M.U.; Muthayya, P.; Jivan, S. Burn Injuries from Exploding Electronic Cigarette Batteries: An Emerging Public Health Hazard. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 1716–1718. [Google Scholar] [CrossRef]
- Ramirez, J.I.; Ridgway, C.A.; Lee, J.G.; Potenza, B.M.; Sen, S.; Palmieri, T.L.; Greenhalgh, D.G.; Maguina, P. The Unrecognized Epidemic of Electronic Cigarette Burns. J. Burn Care Res. 2017, 38, 220–224. [Google Scholar] [CrossRef]
- Toy, J.; Dong, F.; Lee, C.; Zappa, D.; Le, T.; Archambeau, B.; Culhane, J.T.; Neeki, M.M. Alarming Increase in Electronic Nicotine Delivery Systems-Related Burn Injuries: A Serious Unregulated Public Health Issue. Am. J. Emerg. Med. 2017, 35, 1781–1782. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Topol, E.J. Explosion Injuries from E-Cigarettes. N. Engl. J. Med. 2016, 375, 1400. [Google Scholar] [CrossRef]
- Serror, K.; Chaouat, M.; Legrand, M.M.; Depret, F.; Haddad, J.; Malca, N.; Mimoun, M.; Boccara, D. Burns Caused by Electronic Vaping Devices (e-Cigarettes): A New Classification Proposal Based on Mechanisms. Burns 2018, 44, 544–548. [Google Scholar] [CrossRef]
- Rudy, S.F.; Durmowicz, E.L. Electronic Nicotine Delivery Systems: Overheating, Fires and Explosions. Tob. Control 2017, 26, 10–18. [Google Scholar] [CrossRef]
- McKenna, L.A., Jr. Electronic Cigarette Fires and Explosions in the United States 2009–2016; US Fire Administration: Emmitsburg, MD, USA, 2017. [Google Scholar]
- Rossheim, M.E.; Livingston, M.D.; Soule, E.K.; Zeraye, H.A.; Thombs, D.L. Electronic Cigarette Explosion and Burn Injuries, US Emergency Departments 2015–2017. Tob. Control 2019, 28, 472–474. [Google Scholar] [CrossRef]
- Corey, C.G.; Chang, J.T.; Rostron, B.L. Electronic Nicotine Delivery System (ENDS) Battery-Related Burns Presenting to US Emergency Departments, 2016. Inj. Epidemiol. 2018, 5, 1–4. [Google Scholar] [CrossRef]
- Howard, C. A New Source for Nicotine Exposures in Pediatric Patients: Electronic Cigarettes. J. Emerg. Nurs. 2016, 42, 451–453. [Google Scholar] [CrossRef]
- Seo, A.D.; Kim, D.C.; Yu, H.J.; Kang, M.J. Accidental Ingestion of E-Cigarette Liquid Nicotine in a 15-Month-Old Child: An Infant Mortality Case of Nicotine Intoxication. Korean J. Pediatr. 2016, 59, 490–493. [Google Scholar] [CrossRef]
- Gupta, S.; Gandhi, A.; Manikonda, R. Accidental Nicotine Liquid Ingestion: Emerging Paediatric Problem. Arch. Dis. Child. Educ. Pract. Ed. 2014, 99, 1149. [Google Scholar] [CrossRef]
- Gill, N.; Sangha, G.; Poonai, N.; Lim, R. E-Cigarette Liquid Nicotine Ingestion in a Child: Case Report and Discussion. Can. J. Emerg. Med. 2015, 17, 699–703. [Google Scholar] [CrossRef]
- De Pieri, C.; Brisotto, S.; Marzona, F.; Dolcemascolo, V.; Cogo, P.E. Liquid Nicotine Intoxication Due to Dangerous Packaging. Pediatr. Emerg. Care 2019, 1. [Google Scholar] [CrossRef]
- Yuji, K.; Tanimoto, T.; Oshima, Y. Nicotine Poisoning in an Infant. N. Engl. J. Med. 2014, 370, 2248. [Google Scholar] [CrossRef]
- Eggleston, W.; Nacca, N.; Stork, C.M.; Marraffa, J.M. Pediatric Death after Unintentional Exposure to Liquid Nicotine for an Electronic Cigarette. Clin. Toxicol. 2016, 54, 890–891. [Google Scholar] [CrossRef]
- Demir, E.; Topal, S. Sudden Sensorineural Hearing Loss Associated with Electronic Cigarette Liquid: The First Case in the Literature. Int. J. Pediatr. Otorhinolaryngol. 2018, 114, 26–28. [Google Scholar] [CrossRef]
- Noble, M.J.; Longstreet, B.; Hendrickson, R.G.; Gerona, R. Unintentional Pediatric Ingestion of Electronic Cigarette Nicotine Refill Liquid Necessitating Intubation. Ann. Emerg. Med. 2017, 69, 94–97. [Google Scholar] [CrossRef]
- Schipper, E.M.; De Graaff, L.C.G.; Koch, B.C.P.; Brkic, Z.; Wilms, E.B.; Alsma, J.; Schuit, S.C.E. A New Challenge: Suicide Attempt Using Nicotine Fillings for Electronic Cigarettes. Br. J. Clin. Pharmacol. 2014, 78, 1469–1471. [Google Scholar] [CrossRef]
- Chen, B.C.; Bright, S.B.; Trivedi, A.R.; Valento, M. Death Following Intentional Ingestion of E-Liquid. Clin. Toxicol. 2015, 53, 914–916. [Google Scholar] [CrossRef]
- Park, E.J.; Min, Y.G. The Emerging Method of Suicide by Electronic Cigarette Liquid: A Case Report. J. Korean Med. Sci. 2018, 33, e52. [Google Scholar] [CrossRef]
- Christensen, L.B.; Van’t Veen, T.; Bang, J. Three Cases of Attempted Suicide by Ingestion of Nicotine Liquid Used in E-Cigarettes. Clin. Toxicol. 2013, 51, 290. [Google Scholar]
- Morley, S.; Slaughter, J.; Smith, P.R. Death from Ingestion of E-Liquid. J. Emerg. Med. 2017, 53, 862–864. [Google Scholar] [CrossRef]
- You, G.; Rhee, J.; Park, Y.; Park, S. Determination of Nicotine, Cotinine and Trans-3′-Hydroxycotinine Using LC/MS/MS in Forensic Samples of a Nicotine Fatal Case by Oral Ingestion of e-Cigarette Liquid. J. Forensic Sci. 2016, 61, 1149–1154. [Google Scholar] [CrossRef]
- Sommerfeld, K.; Łukasik-Głebocka, M.; Kulza, M.; Druzdz, A.; Panieński, P.; Florek, E.; Zielińska-Psuja, B. Intravenous and Oral Suicidal E-Liquid Poisonings with Confirmed Nicotine and Cotinine Concentrations. Forensic Sci. Int. 2016, 262, e15–e20. [Google Scholar] [CrossRef]
- Garat, A.; Nisse, P.; Kauv, M.; Mathieu-Nolf, M.; Allorge, D.; Mathieu, D. Lactic Acidosis Due to Voluntary E-Liquid Ingestion. Toxicol. Anal. Clin. 2016, 28, 329–332. [Google Scholar] [CrossRef]
- Bartschat, S.; Mercer-Chalmers-Bender, K.; Beike, J.; Rothschild, M.A.; Jübner, M. Not Only Smoking Is Deadly: Fatal Ingestion of e-Juice—A Case Report. Int. J. Legal Med. 2014, 129, 481–486. [Google Scholar] [CrossRef]
- Eberlein, C.K.; Frieling, H.; Köhnlein, T.; Hillemacher, T.; Bleich, S. Suicide Attempt by Poisoning Using Nicotine Liquid for Use in Electronic Cigarettes. Am. J. Psychiatry 2014, 171, 891. [Google Scholar] [CrossRef]
- Lam, R.P.K.; Tang, M.H.Y.; Leung, S.C.; Chong, Y.K.; Tsui, M.S.H.; Mak, T.W.L. Supraventricular Tachycardia and Acute Confusion Following Ingestion of E-Cigarette Fluid Containing AB-FUBINACA and ADB-FUBINACA: A Case Report with Quantitative Analysis of Serum Drug Concentrations. Clin. Toxicol. 2017, 55, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Paik, J.H.; Kang, S.; Durey, A.; Kim, J.H.; Kim, A.J. Symptomatic Bradycardia Due to Nicotine Intoxication. Rev. Bras. Ter. Intensiva 2017, 30, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Aoki, Y.; Ikeda, T.; Tani, N.; Shida, A.; Oritani, S.; Ishikawa, T. Evaluation of the Distribution of Nicotine Intravenous Injection: An Adult Autopsy Case Report with a Review of Literature. Int. J. Legal Med. 2019, 134, 243–249. [Google Scholar] [CrossRef]
- Caponnetto, P.; Campagna, D.; Papale, G.; Russo, C.; Polosa, R. Fatal Intravenous Injection of Electronic Nicotine Delivery System Refilling Solution. J. Med. Toxicol. 2014, 10, 202–204. [Google Scholar] [CrossRef]
- Belkoniene, M.; Socquet, J.; Njemba-Freiburghaus, D.; Pellaton, C. Near Fatal Intoxication by Nicotine and Propylene Glycol Injection: A Case Report of an e-Liquid Poisoning. BMC Pharmacol. Toxicol. 2019, 20, 14–18. [Google Scholar] [CrossRef]
- Cervellin, G.; Luci, M.; Bellini, C.; Lippi, G. Bad News about an Old Poison. A Case of Nicotine Poisoning Due to Both Ingestion and Injection of the Content of an Electronic Cigarette Refill. Emerg. Care J. 2013, 9, 18. [Google Scholar] [CrossRef]
- Asma, S.; Song, Y.; Cohen, J.; Eriksen, M.; Pechacek, T.; Cohen, N.; Iskander, J. Notes from the Field: Calls to Poison Centers for Exposures to Electronic Cigarettes--United States, September 2010–February 2014. Morb. Mortal. Wkly. Rep. 2014, 63, 277–280. [Google Scholar]
- Wang, B.; Liu, S.; Persoskie, A. Poisoning Exposure Cases Involving E-Cigarettes and e-Liquid in the United States, 2010–2018. Clin. Toxicol. 2019, 1–7. [Google Scholar] [CrossRef]
- Ordonez, J.E.; Kleinschmidt, K.C.; Forrester, M.B. Electronic Cigarette Exposures Reported to Texas Poison Centers. Nicotine Tob. Res. 2015, 17, 209–211. [Google Scholar] [CrossRef]
- Horth, R.Z.; Crouch, B.; Horowitz, B.Z.; Prebish, A.; Slawson, M.; McNair, J.; Elsholz, C.; Gilley, S.; Robertson, J.; Risk, I.; et al. Acute Poisonings from a Synthetic Cannabinoid Sold as Cannabidiol—Utah, 2017–2018. Morb. Mortal. Wkly. Rep. 2018, 67, 587–588. [Google Scholar] [CrossRef]
- Ang, E.; Tuthill, D.; Thompson, J. E-Cigarette Liquid Ingestion: A Fast Growing Accidental Issue in Children. Arch. Dis. Child. 2018, 103, 1091. [Google Scholar] [CrossRef]
- Chang, J.T.; Wang, B.; Chang, C.M.; Ambrose, B.K. National Estimates of Poisoning Events Related to Liquid Nicotine in Young Children Treated in US Hospital Emergency Departments, 2013–2017. Inj. Epidemiol. 2019, 6, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.T.; Rostron, B.L. Electronic Nicotine Delivery System (ENDS) Liquid Nicotine Exposure in Young Children Presenting to US Emergency Departments, 2018. Inj. Epidemiol. 2019, 5, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Shim, T.N.; Kosztyuova, T. Allergic Contact Dermatitis to Electronic Cigarette. Dermatitis 2018, 29, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Ormerod, E.; Stone, N. Contact Allergy and Electronic Cigarettes (and Eyelash Curlers). Clin. Exp. Dermatol. 2017, 42, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Maridet, C.; Atge, B.; Amici, J.M.; Taïeb, A.; Milpied, B. The Electronic Cigarette: The New Source of Nickel Contact Allergy of the 21st Century? Contact Dermat. 2015, 73, 49–50. [Google Scholar] [CrossRef] [PubMed]
- Holland, T.E.; De La Feld, S. E-Cigarette Dermatitis. Dermatitis 2019, 30, 272. [Google Scholar] [CrossRef]
- Khorassani, F.; Kaufman, M.; Lopez, L. Supatherapeutic Serum Clozapine Concentration After Transition from Traditional to Electronic Cigarettes. Arthritis Rheum. 2018, 38, 391–392. [Google Scholar] [CrossRef]
- Kocar, T.; Freudenmann, R.W.; Spitzer, M.; Graf, H. G. Switching from Tobacco Smoking to Electronic Cigarettes and the Impact on Clozapine Levels. J. Clin. Psychopharmacol. 2018, 38, 528–529. [Google Scholar] [CrossRef]
- Wharton, J.D.; Kozek, L.K.; Carson, R.P. Increased Seizure Frequency Temporally Related to Vaping: Where There’s Vapor, There’s Seizures? Pediatr. Neurol. 2019. [Google Scholar] [CrossRef]
- Han, C.; Yan, N.; Sun, C. E-Cigarettes as Salvage Therapy for Medically Refractory Ulcerative Colitis. Inflamm. Bowel Dis. 2013, (suppl.1). [Google Scholar] [CrossRef]
- Camus, M.; Gallois, G.; Marteau, P. Ulcerative Colitis and Electronic Cigarette: What’s the Matter? Am. J. Gastroenterol. 2014, 109, 608–609. [Google Scholar] [CrossRef] [PubMed]
- McCague, Y. Ocular Chemical Burns Secondary to Accidental Administration of E-Cigarette Liquid. Adv. Emerg. Nurs. J. 2018, 40, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Jamison, A.; Lockington, D. Ocular Chemical Injury Secondary to Electronic Cigarette Liquid Misuse. JAMA Ophthalmol. 2016, 134, 1443. [Google Scholar] [CrossRef] [PubMed]
- Andresen, N.S.; Lee, D.J.; Kowalski, C.E.; Bayon, R. Fall with E-Cigarette in Mouth Resulting in Pharyngeal and Esophageal Burns. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Farinha, H.; Martins, V. Lingua Villosa Nigra Associated with the Use of Electronic Cigarette. Acta Med. Port. 2015, 28, 393. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bartram, A.; Jones, N.; Endersby, S. Lichenoid Eruption Associated with Use of an E-Cigarette. Br. J. Oral Maxillofac. Surg. 2016, 54, 475. [Google Scholar] [CrossRef]
- Cant, A.; Collard, B.; Cunliffe, D. Electronic Cigarettes: Necrotic Ulcer. Br. Dent. J. 2017, 222, 226. [Google Scholar] [CrossRef]
- Frossard, S.M.; Volansky, P.M.; Endara-Bravo, A.S. Acute Uvulitis Secondary to Electronic Cigarette Use. Am. J. Respir. Crit. Care Med. 2015, 191, A1556. [Google Scholar]
- Fracol, M.; Dorfman, R.; Janes, L.; Kulkarni, S.; Bethke, K.; Hansen, N.; Kim, J. The Surgical Impact of E-Cigarettes: A Case Report and Review of the Current Literature. Arch. Plast. Surg. 2017, 44, 477–481. [Google Scholar] [CrossRef]
- Agochukwu, N.; Liau, J.Y. Debunking the Myth of E-Cigarettes: A Case of Free Flap Compromise Due to e-Cigarette Use within the First 24 Hours. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Kivrak, T.; Durmus, E.; Dervisova, R.; Sari, I.; Yesildag, O.; Sunbul, M. Acute Myocardial Infarction Due to Liquid Nicotine in a Young Man. Ther. Adv. Cardiovasc. Dis. 2014, 8, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Mehta, J.J.; Mahendran, A.K.; Bajaj, R.K.; Doshi, A.R. Myocardial Ischemia with Cannabinoid Use in an Adolescent. Cureus 2017, 2, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Gillen, S.; Saltzman, D. Antenatal Exposure to E-Cigarette Vapor as a Possible Etiology to Total Colonic Necrotizing Enterocolitits: A Case Report. J. Pediatr. Surg. Case Rep. 2014, 2, 536–537. [Google Scholar] [CrossRef][Green Version]
- Okuni-Watanabe, M.; Kurata, K.; Yakushijin, K. The First Case of E-Cigarette-Induced Polycythemia. Case Rep. Hematol. 2019, 2019, 2084325. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Romagna, G. Chronic Idiopathic Neutrophilia in A Smoker, Relieved after Smoking Cessation with the Use of Electronic Cigarette: A Case Report. Clin. Med. Insights Case Rep. 2013, 6. [Google Scholar] [CrossRef]
- Miler, J.A.; Hajek, P. Resolution of Recurrent Tonsillitis in a Non-Smoker Who Became a Vaper. A Case Study and New Hypothesis. Med. Hypotheses 2017, 109, 17–18. [Google Scholar] [CrossRef]
- Miler, J.A.; Hajek, P. Resolution of Chronic Nasal Staphylococcus Aureus Infection in a Non-Smoker Who Started to Use Glycerine Based e-Cigarettes: Antibacterial Effects of Vaping? Med. Hypotheses 2018, 118, 42–43. [Google Scholar] [CrossRef]
- England, L.J.; Aagaard, K.; Bloch, M.; Conway, K.; Cosgrove, K.; Grana, R.; Gould, T.J.; Hatsukami, D.; Jensen, F.; Kandel, D.; et al. Developmental Toxicity of Nicotine: A Transdisciplinary Synthesis and Implications for Emerging Tobacco Products. Neurosci. Biobehav. Rev. 2017, 72, 176–189. [Google Scholar] [CrossRef]
- Christiani, D.C. Vaping-Induced Lung Injury. N. Engl. J. Med. 2019, 1–2. [Google Scholar] [CrossRef]
- Pambuccian, S.E. Testing for Lipid-Laden Macrophages in Bronchoalveolar Lavage Fluid to Diagnose Vaping-Associated Pulmonary Injury. Are We There Yet? J. Am. Soc. Cytopathy 2019. [Google Scholar] [CrossRef] [PubMed]
- Hadda, V.; Khilnani, G.C. Lipoid Pneumonia: An Overview. Expert Rev. Respir. Med. 2010, 4, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, S.L.; Martinez-Jimenez, S.; Rossi, S.E.; Truong, M.T.; Carrillo, J.; Erasmus, J.J. Lipoid Pneumonia: Spectrum of Clinical and Radiologic Manifestations. Am. J. Roentgenol. 2010, 194, 103–109. [Google Scholar] [CrossRef]
- De Giacomi, F.; Vassallo, R.; Yi, E.S.; Ryu, J.H. Acute Eosinophilic Pneumonia. Am. J. Respir. Crit. Care Med. 2018, 197, 728–736. [Google Scholar] [CrossRef] [PubMed]
- De Giacomi, F.; Decker, P.; Vassallo, R.; Ryu, J. Smoking-Related Acute Eosinophilic Pneumonia Compared to Idiopathic and Drug-Related Forms. A42. NEW DEVELOPMENTS IN ILD RESEARCH. Available online: https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2017.195.1_MeetingAbstracts.A1571 (accessed on 21 January 2020).
- Lappas, A.S.; Tzortzi, A.S.; Konstantinidi, E.M.; Teloniatis, S.I.; Tzavara, C.K.; Gennimata, S.A.; Koulouris, N.G.; Behrakis, P.K. Short-Term Respiratory Effects of e-Cigarettes in Healthy Individuals and Smokers with Asthma. Respirology 2018, 23, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Underner, M.; Urban, T.; Perriot, J.; Peiffer, G.; Harika-Germaneau, G.; Jaafari, N. Spontaneous Pneumothorax and Lung Emphysema in Cannabis Users. Rev. Pneumol. Clin. 2018, 74, 400–415. [Google Scholar] [CrossRef]
- Coetzee, C.; Levendal, R.A.; van de Venter, M.; Frost, C.L. Anticoagulant Effects of a Cannabis Extract in an Obese Rat Model. Phytomedicine 2007, 14, 333–337. [Google Scholar] [CrossRef]
- Cordier, J.F. Cryptogenic Organising Pneumonia. Eur. Respir. J. 2006, 28, 422–446. [Google Scholar] [CrossRef]
- Van Rooy, F.G.B.G.J.; Rooyackers, J.M.; Prokop, M.; Houba, R.; Smit, L.A.M.; Heederik, D.J.J. Bronchiolitis Obliterans Syndrome in Chemical Workers Producing Diacetyl for Food Flavorings. Am. J. Respir. Crit. Care Med. 2007, 176, 498–504. [Google Scholar] [CrossRef]
- Harber, P.; Saechao, K.; Boomus, C.; Reports, C. Diacetyl-Induced Lung Disease. Toxicol. Rev. 2006, 25, 261–272. [Google Scholar] [CrossRef]
- Hubbs, A.F.; Goldsmith, W.T.; Kashon, M.L.; Frazer, D.; Mercer, R.R.; Battelli, L.A.; Kullman, G.J.; Schwegler-Berry, D.; Friend, S.; Castranova, V. Respiratory Toxicologic Pathology of Inhaled Diacetyl in Sprague-Dawley Rats. Toxicol. Pathol. 2008, 36, 330–344. [Google Scholar] [CrossRef]
- Vas, C.A.; Porter, A.; McAdam, K. Acetoin Is a Precursor to Diacetyl in E-Cigarette Liquids. Food Chem. Toxicol. 2019, 133, 110727. [Google Scholar] [CrossRef] [PubMed]
- Blount, B.C.; Karwowski, M.P.; Shields, P.G.; Morel-Espinosa, M.; Valentin-Blasini, L.; Gardner, M.; Braselton, M.; Brosius, C.R.; Caron, K.T.; Chambers, D.; et al. Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI. N. Engl. J. Med. 2019, 382, 697–705. [Google Scholar] [CrossRef]
- Martin, E.M.; Clapp, P.W.; Rebuli, M.E.; Pawlak, E.A.; Glista-Baker, E.; Benowitz, N.L.; Fry, R.C.; Jaspers, I. E-Cigarette Use Results in Suppression of Immune and Inflammatory-Response Genes in Nasal Epithelial Cells Similar to Cigarette Smoke. Am. J. Physiol. Lung Cell. Mol. Physiol. 2016, 311, L135–L144. [Google Scholar] [CrossRef]
- Ghosh, A.; Coakley, R.C.; Mascenik, T.; Rowell, T.R.; Davis, E.S.; Rogers, K.; Webster, M.J.; Dang, H.; Herring, L.E.; Sassano, M.F.; et al. Chronic E-Cigarette Exposure Alters the Human Bronchial Epithelial Proteome. Am. J. Respir. Crit. Care Med. 2018, 198, 67–76. [Google Scholar] [CrossRef]
- Madison, M.C.; Landers, C.T.; Gu, B.H.; Chang, C.Y.; Tung, H.Y.; You, R.; Hong, M.J.; Baghaei, N.; Song, L.Z.; Porter, P.; et al. Electronic Cigarettes Disrupt Lung Lipid Homeostasis and Innate Immunity Independent of Nicotine. J. Clin. Investig. 2019, 129, 4290–4304. [Google Scholar] [CrossRef] [PubMed]
- Franke, F.E.; Thomas, J.E. The treatment of acute nicotine poisoning. J. Am. Med. Assoc. 2015, 106, 509–512. [Google Scholar] [CrossRef]
- Lazutka, F.A.; Vasiliauskene, A.P.; Gefen, S.G. On the toxicological assessment of the insecticide nicotine sulfate TT-K toksikologicheskoĭ otsenke insektitsida nikotin-sul’fata. Gig. Sanit. 1969, 34, 30–33. [Google Scholar] [PubMed]
- Mayer, B. How Much Nicotine Kills a Human? Tracing Back the Generally Accepted Lethal Dose to Dubious Self-Experiments in the Nineteenth Century. Arch. Toxicol. 2014, 88, 5–7. [Google Scholar] [CrossRef]
- European Commission. Revision of the Tobacco Products Directive. Available online: https://ec.europa.eu/health/tobacco/products/revision_en (accessed on 1 March 2014).
- Doing, B.Y. Vaping-Induced Acute Lung Injury: An Epidemic That Could Have Been Prevented. AJRCCM 2019, 1–7. [Google Scholar] [CrossRef]
- Rong, L.; Frontera, A.T.; Benbadis, S.R. Tobacco Smoking, Epilepsy, and Seizures. Epilepsy Behav. 2014, 31, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Iha, H.A.; Kunisawa, N.; Shimizu, S.; Tokudome, K.; Mukai, T.; Kinboshi, M.; Ikeda, A.; Ito, H.; Serikawa, T.; Ohno, Y. Nicotine Elicits Convulsive Seizures by Activating Amygdalar Neurons. Front. Pharmacol. 2017, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Blacker, C.J. Clinical Issues to Consider for Clozapine Patients Who Vape: A Case Illustration. Focus (Am. Psychiatr. Publ). 2020, 18, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Grigg, J. E-Cigarette Regulation: Getting It Wrong Costs Lives. Lancet Respir. Med. 2019, 7, 994–995. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Injury | USA | UK | EU-Other | Other |
|---|---|---|---|---|
| Respiratory | 36 (88%) | 1 (2%) | - | 4 (10%) |
| Traumatic injury | 32 (76%) | 5 (12%) | 3 (7%) | 2 (5%) |
| Poisoning | 6 (24%) | 2 (8%) | 9 (36%) | 8 (32%) |
| Allergy | 1 (25%) | 2 (50%) | 1 (25%) | - |
| Effect on medication metabolism and plasma levels | 2 (67%) | - | 1 (33%) | - |
| Ulcerative colitis | 1 (50%) | - | 1 (50%) | - |
| Misuse of e-liquid | - | - | 2 (100%) | - |
| Injury caused by falling with e-cigarette in mouth | 1 (100%) | - | - | - |
| Additional diagnoses and health effects attributed to electronic cigarette use | 5 (38%) | 4 (31%) | 2 (15%) | 2 (15%) |
| Variable | n = 58 |
|---|---|
| Sex (%) | |
| Male | 69% |
| Female | 31% |
| Age in years median (IQR) | 23 (19–33) |
| Dual user (e-cig+ combustible cigarette) | |
| Yes | 10% |
| No | 16% |
| Unspecified | 74% |
| E-cig for cessation | |
| Yes | 13% |
| No | 71% |
| Unspecified | 16% |
| Medical history (%) | |
| No medical history | 66% |
| Asthma/ Allergy | 21% |
| Other * | 14% |
| Substances used (%) | |
| CBD/THC | 36% |
| CBD/THC and Nicotine | 10% |
| CBD/THC and unknown liquid | 10% |
| Nicotine | 3% |
| Unknown/unspecified liquid | 40% |
| Symptoms (%) | |
| Dyspnea | 83% |
| Cough | 59% |
| Dyspnea and Cough | 53% |
| Chest pain | 22% |
| Hemoptysis | 9% |
| Fever | 40% |
| Respiratory arrest | 5% |
| Gastrointestinal symptoms | 26% |
| CT (%)—available for 52 cases | |
| GGO | 38% |
| GGO + consolidation | 12% |
| Opacities | 10% |
| Multiple nodules | 6% |
| GGO + multiple nodules | 6% |
| Other | 28% |
| Interventions | |
| High flow nasal cannula therapy | 18% |
| Intubation/ mechanical ventilation | 31% |
| ECMO | 15% |
| Bronchoscopy | 78% |
| Diagnosis | |
| EVALI | 26% |
| Organizing pneumonia/BOOP/Respiratory bronchiolitis | 21% |
| Lipoid pneumonia | 16% |
| Eosinophilic pneumonia | 7% |
| Pneumothorax | 7% |
| Hypersensitivity pneumonitis | 5% |
| Organizing pneumonia and lipoid pneumonia | 5% |
| Asthma exacerbation | 3% |
| ARDS | 2% |
| ARDS-DAD-Organizing pneumonia | 2% |
| DAH | 2% |
| EVALI and secondary pneumothorax | 2% |
| Epiglottitis | 2% |
| Possible EVALI on asthma grounds | 2% |
| Corticosteroid administration | 73% |
| Outcome | |
| Recovered | 83% |
| Discharged but hospitalized again | 5% |
| Persisting complications | 10% |
| Deceased | 2% |
| Paper | Country | Bronchoalveolar Lavage (BAL) | Transbronchial Biopsy | Open Lung Biopsy |
|---|---|---|---|---|
| He et al., 2017 [38] | USA | Possible DAH | Organizing pneumonia | |
| Modi et al., 2015 [47] | USA | LLM (Oil Red O positive) | ||
| Mantilla et al., 2016 [45] | USA | No cytology information | BOOP | |
| Mukhopadhyay et al., 2019 [40] | USA | Macrophage predominant | DAD (acute and organizing) | |
| None obtained | Organizing pneumonia | |||
| LLM (Oil Red O positive) | Organizing ALI | |||
| LLM (Oil Red O positive) | Organizing pneumonia | |||
| LLM (Oil Red O positive) | Organizing ALI | |||
| Macrophage predominant | Organizing pneumonia | |||
| Macrophage predominant | Organizing pneumonia | |||
| Arter et al., 2019 [56] | USA | 26% eosinophils | ||
| Agustin et al., 2018 [62] | USA | Recurrent DAH | ||
| Sommerfeld et al., 2018 [60] | USA | LLM (Oil Red O positive) | ||
| Khan et al., 2018 [41] | USA | Organizing pneumonia | ||
| Flower et al., 2017 [43] | Australia | Non-diagnostic | Non-diagnostic | RUL: black pigmentation and bullae |
| Thota D and Latham E, 2014 [57] | USA | Negative cultures | ||
| McCauley et al., 2012 [11] | USA | LLM (Oil Red O positive) | ||
| Itoh et al., 2018 [33] | Japan | LLM (Oil Red O positive) | Acute alveolitis intra-alveolar fibrosis | |
| Dicpinigaitis et al., 2019 [51] | USA | LLM (Oil Red O positive) | ||
| Landman et al., 2019 [39] | Canada | Negative cultures | Non-specific acute inflammation and reactive changes | |
| Viswam et al., 2018 [50] | UK | Pink cloudy fluid Negative microbiology and cytology | LLM and cholesterol clefts | |
| Maddock et al., 2019 [49] | USA | 49% neutrophils, >50% LLM (Oil Red O positive) | ||
| ~50% LLM (Oil Red O positive) | ||||
| ~30% LLM (Oil Red O positive) | ||||
| ~75% LLM (Oil Red O positive) | ||||
| Layden et. al, 2019 [42] | USA | 78% neutrophils, some LLM (Oil Red O positive) | ||
| Sharma et al., 2019 [37] | USA | Lymphocytes predominance and rare eosinophils | ||
| Pokhrel et al., 2019 [31] | USA | LLM predominance | ||
| Neutrophil predominance | ||||
| LLM predominance | ||||
| Abeles et al., 2019 [28] | USA | 51% PMN, negative cultures, rare LLMs | ||
| Casanova et al. 2019 [30] | USA | 55% LLMs | ||
| Ocampo-Gonzalez and Park, 2019 [32] | USA | 80% LLM (Oil Red O positive) | ||
| Attis et al., 2018 [61] | USA | Macrophage predominance | ||
| Aftab et al., 2019 [35] | USA | 91% neutrophils | ||
| Buus et al., 2019 [29] | USA | Macrophages/ neutrophils/ lymphocytes | ||
| Lu et al., 2020 [44] | USA | Ιntra-alveolar fibrin and neutrophils | ||
| Youmans et al., 2020 [64] | USA | 50% monocytes, 40% lymphocytes, 10% neutrophils | Non-diagnostic | Acute and organizing DAD with foamy macrophages |
| Antwi-Amoabeng et al., 2020 [59] | USA | 75% eosinophils | ||
| Ansari-Gilani et al., 2020 [46] | USA | Unremarkable | Poorly define granulomas | |
| Unremarkable | ||||
| Abbara et al., 2019 [48] | USA | Lipoid pneumonia |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzortzi, A.; Kapetanstrataki, M.; Evangelopoulou, V.; Behrakis, P. A Systematic Literature Review of E-Cigarette-Related Illness and Injury: Not Just for the Respirologist. Int. J. Environ. Res. Public Health 2020, 17, 2248. https://doi.org/10.3390/ijerph17072248
Tzortzi A, Kapetanstrataki M, Evangelopoulou V, Behrakis P. A Systematic Literature Review of E-Cigarette-Related Illness and Injury: Not Just for the Respirologist. International Journal of Environmental Research and Public Health. 2020; 17(7):2248. https://doi.org/10.3390/ijerph17072248
Chicago/Turabian StyleTzortzi, Anna, Melpo Kapetanstrataki, Vaso Evangelopoulou, and Panagiotis Behrakis. 2020. "A Systematic Literature Review of E-Cigarette-Related Illness and Injury: Not Just for the Respirologist" International Journal of Environmental Research and Public Health 17, no. 7: 2248. https://doi.org/10.3390/ijerph17072248
APA StyleTzortzi, A., Kapetanstrataki, M., Evangelopoulou, V., & Behrakis, P. (2020). A Systematic Literature Review of E-Cigarette-Related Illness and Injury: Not Just for the Respirologist. International Journal of Environmental Research and Public Health, 17(7), 2248. https://doi.org/10.3390/ijerph17072248