A Literature Review on Psychosocial Support for Disaster Responders: Qualitative Synthesis with Recommended Actions for Protecting and Promoting the Mental Health of Responders


Abstract
1. Introduction
2. Material and Methods
2.1. Review Authors
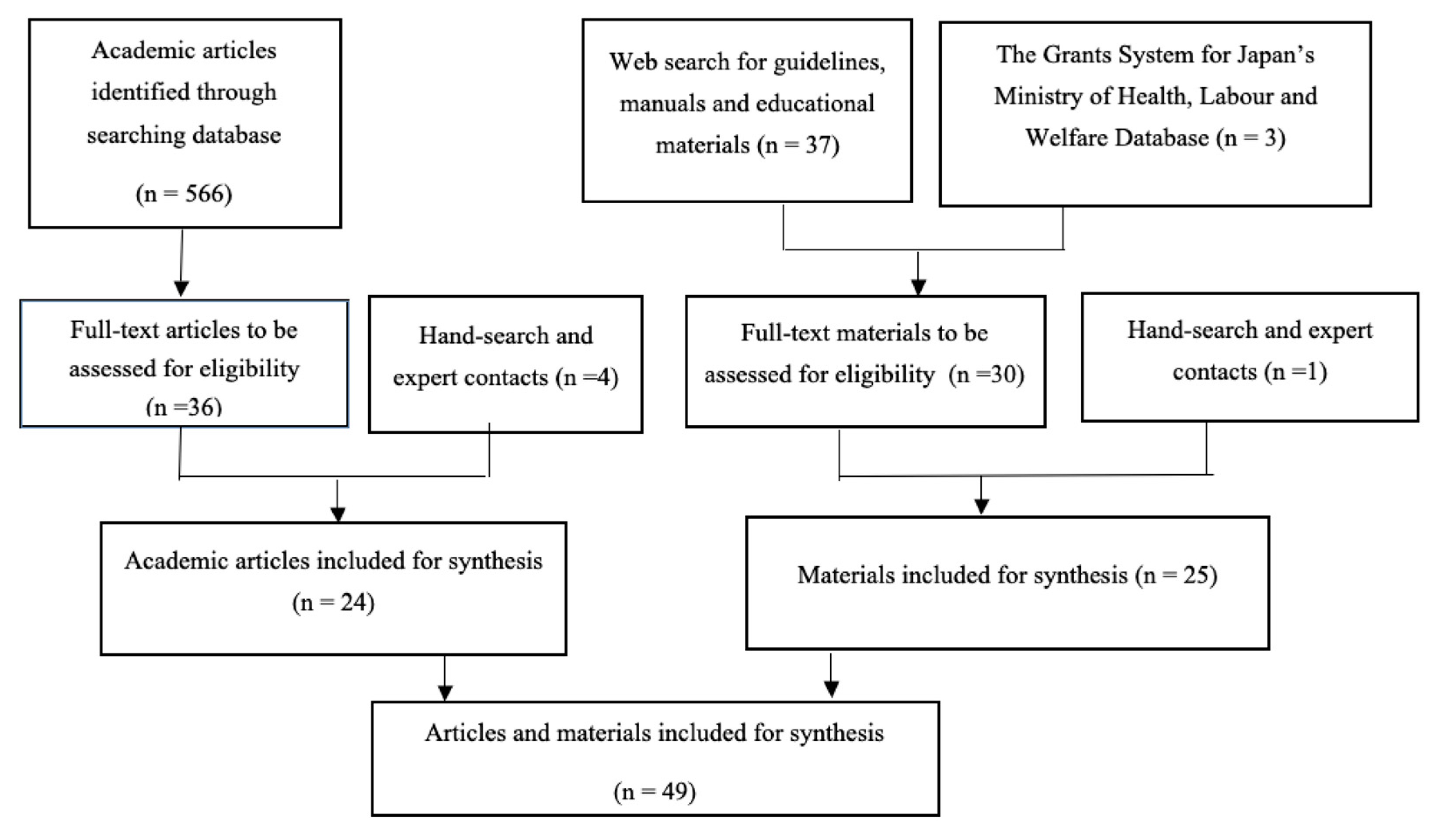
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Term Definitions
2.5. Analysis
3. Results
3.1. Goal 1: Understanding Stressors and Making them Manageable
3.2. Goal 2: Reducing Stressors and Preventing Chronically Stressful Situations
3.3. Goal 3: Alleviating Stressful Situations and Managing Crises
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Greenberg, N.; Rubin, G.J. Training and post-disaster interventions for the psychological impacts on disaster-exposed employees: A systematic review. J. Ment. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Dückers, M.L.A.; Thormar, S.B.; Juen, B.; Ajdukovic, D.; Newlove-Eriksson, L.; Olff, M. Measuring and modelling the quality of 40 post-disaster mental health and psychosocial support programmes. PLoS ONE 2018, 13, e0193285. [Google Scholar] [CrossRef] [PubMed]
- Leaning, J.; Guha-Sapir, D. Natural disasters, armed conflict, and public health. N. Engl. J. Med. 2013, 369, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Benedek, D.M.; Fullerton, C.; Ursano, R.J. First responders: Mental health consequences of natural and human-made disasters for public health and public safety workers. Annu. Rev. Public Health 2007, 28, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef] [PubMed]
- Shinfuku, N. Disaster mental health: Lessons learned from the Hanshin Awaji earthquake. World Psychiatry 2002, 1, 158–159. [Google Scholar]
- Beaglehole, B.; Mulder, R.T.; Frampton, C.M.; Boden, J.M.; Newton-Howes, G.; Bell, C.J. Psychological distress and psychiatric disorder after natural disasters: Systematic review and meta-analysis. Br. J. Psychiatry 2018, 213, 716–722. [Google Scholar] [CrossRef]
- Cox, R.S.; Danford, T. The need for a systematic approach to disaster psychosocial response: A suggested competency framework. Prehosp. Disaster Med. 2014, 29, 183–189. [Google Scholar] [CrossRef]
- Foa, E.B.; Stein, D.J.; McFarlane, A.C. Symptomatology and psychopathology of mental health problems after disaster. J. Clin. Psychiatry 2006, 67 (Suppl. 2), 15–25. [Google Scholar]
- Lee, J.S.; You, S.; Choi, Y.K.; Youn, H.; Shin, H.S. A preliminary evaluation of the training effects of a didactic and simulation-based psychological first aid program in students and school counselors in South Korea. PLoS ONE 2017, 12, e0181271. [Google Scholar] [CrossRef]
- Thorpe, L.E.; Assari, S.; Deppen, S.; Glied, S.; Lurie, N.; Mauer, M.P.; Mays, V.M.; Trapido, E. The role of epidemiology in disaster response policy development. Ann. Epidemiol. 2015, 25, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Fahim, C.; O’Sullivan, T.L.; Lane, D. Support needs for canadian health providers responding to disaster: New insights from a grounded theory approach. PLoS Curr. 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, T.L.; Dow, D.; Turner, M.C.; Lemyre, L.; Corneil, W.; Krewski, D.; Phillips, K.P.; Amaratunga, C.A. Disaster and emergency management: Canadian nurses’ perceptions of preparedness on hospital front lines. Prehosp. Disaster Med. 2008, 23, s11–s18. [Google Scholar] [CrossRef] [PubMed]
- Haugen, P.T.; Evces, M.; Weiss, D.S. Treating posttraumatic stress disorder in first responders: A systematic review. Clin. Psychol. Rev. 2012, 32, 370–380. [Google Scholar] [CrossRef]
- Matsui, Y.; Tatewaki, Y. Countermeasures for thecritical incident stress from occupational mental health perspective: The care for the critical incidentstress of firefighters, the critical incident stress careand crisis intervention system. Occup. Ment. Health 2013, 21, 24–30. [Google Scholar]
- Kobayashi, T.; Eguchi, M.; Imaki, H.; Saito, J.; Yoshinaga, Y.; Ishikawa, R.; Nakagaki, M.; Tuchiya, H. Effect of multidisciplinary training workshop related to mental health care after a disaster. Bull. Cent. Educ. Res. Tech. Dev. Shizuoka Univ. 2015, 24, 103–107. [Google Scholar]
- Reid, W.M.; Ruzycki, S.; Haney, M.L.; Brown, L.M.; Baggerly, J.; Mescia, N.; Hyer, K. Disaster mental health training in florida and the response to the 2004 hurricanes. J. Public Health Manag. Pract. 2005, 11, S57–S62. [Google Scholar] [CrossRef]
- Kuhls, D.A.; Chestovich, P.J.; Coule, P.; Carrison, D.M.; Chua, C.M.; Wora-Urai, N.; Kanchanarin, T. Basic Disaster Life Support (BDLS) training improves first responder confidence to face mass-casualty incidents in Thailand. Prehosp. Disaster Med. 2017, 32, 492–500. [Google Scholar] [CrossRef]
- Kamena, M.; Galvez, H. Intensive residential treatment program: Efficacy for emergency responders’ critical incident stress. J. Police Crim. Psych. 2019. [Google Scholar] [CrossRef]
- Miyamichi, R.; Ishikawa, S.; Omi, S. Efficacy of significant event analysis for stress management among disaster relief operation doctors: A non-blinded randomized control study. Nihon Kyukyu Igakukai Zasshi 2013, 24, 321–328. [Google Scholar] [CrossRef][Green Version]
- Salita, C.; Liwanag, R.; Tiongco, R.E.; Kawano, R. Development, implementation, and evaluation of a lay responder disaster training package among school teachers in Angeles City, Philippines: Using Witte’s behavioral model. Public Health 2019, 170, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Brooks, J. The world trade center attack. Helping the helpers: The role of critical incident stress management. Crit. Care Lond. Engl. 2001, 5, 315–317. [Google Scholar] [CrossRef]
- Yajima, J. The role of clinical psychologist in the support for disaster workers after disaster. Jpn. J. Stress Sci. 2019, 33, 330–332. [Google Scholar]
- Yamamoto, T.; Tsunoda, T.; Yamashita, R. Operational stress management for members of Japan self-defense forces on the disaster relief mission of great east Japan earthquake. Trauma. Stress Stud. 2013, 11, 125–132. [Google Scholar]
- Inter-Agency Standing Committee. Guidelines on Mental Health and Psychosocial Support in Emergency Settings; Inter-Agency Standing Committee: Geneva, Switzerland, 2007; Available online: https://www.who.int/mental_health/emergencies/guidelines_iasc_mental_health_psychosocial_june_2007.pdf (accessed on 2 September 2019).
- Lazarus, R.S. Emotion and Adaptation; Oxford University Press: New York, NY, USA, 1991. [Google Scholar]
- Asada, T. Psychological Care on Disaster. Psychological Support, Medical and Welfare, Life Support. Procedure Manual Version 1.0. 2015. Available online: http://www.jrc.or.jp/vcms_lf/care2.pdf (accessed on 2 September 2019).
- Young, B.H.; Ford, J.D.; Ruzek, J.I.; Friedman, M.J.; Gusman, F.D. Disaster Mental Health Handbook: Disaster Services: A Guidebook for Clinician and Administrators; Department of Veterans Affairs, the National Center for Post-Traumatic Stress Disorder: California, USA, 2006; Available online: https://www.hsdl.org/?view&did=441325 (accessed on 18 March 2020).
- Japanese Red Cross Society. Mental Health Care in Disaster; Japanese Red Cross Society: Tokyo, Japan, 2004; Available online: http://www.jrc.or.jp/vcms_lf/care2.pdf (accessed on 2 September 2019).
- Japanese Red Cross Society. Training Manual of Mental Health Care in Disaster for Trainers of Relief Workers; Japanese Red Cross Society: Tokyo, Japan, 2012. Available online: http://ndrc.jrc.or.jp/infolib/cont/01/G0000001nrcarchive/000/070/000070821.pdf (accessed on 2 September 2019).
- Takahashi, Y. Principles of mental health among care providers. Hum. Mind 2016, 190, 92–96. [Google Scholar]
- United Nations High Commissioner for Refugees. Emergency Handbook: Staff Wellbeing Version 2.9; United Nations High Commissioner for Refugees: Geneva, Swizterland; Available online: https://emergency.unhcr.org/ (accessed on 2 September 2019).
- World Health Organisation. War Trauma Foundation and World Vision International: Psychological First Aid: Facilitator’s Guide for Field Workers; WHO: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/44615/9789241548205_eng.pdf;jsessionid=0AB6486F31E96F87EBAEE6F4772388FE?sequence=1 (accessed on 2 September 2019).
- World Health Organization. War Trauma Foundation and World Vision International: Psychological First Aid: Facilitator’s Guide for Field Workers; WHO: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/bitstream/handle/10665/102380/9789241548618_eng.pdf?sequence=1&isAllowed=y (accessed on 2 September 2019).
- Yamada, H.; Kujyu, M.; Yoshida, H. The research on the mental health and body health condition toward public health nurses working for the victims of East Japan Great Earthquake. Jpn. Soc. Health Sci. Mind Body 2013, 9, 26–36. [Google Scholar]
- Office of Disaster Psychiatric Assistance Team. Activity Manual on Disaster Psychiatric Assistance Team: DPAT Version 2.0. Available online: http://www.dpat.jp/images/dpat_documents/3.pdf (accessed on 2 September 2019).
- Antares Foundation. Managing Stress in Humanitarian Workers: Guidelines for Good Practice; Published 2012; Antares Foundation: Amsterdam, Netherlands, 2012; Available online: http://www.socialserviceworkforce.org/resources/managing-stress-humanitarian-workers-guidelines-good-practice (accessed on 2 September 2019).
- Cabinet Office. Psychological Care for Disaster Survivors: Management Guidelines for Prefectural Governments; Cabinet Office: Tokyo, Japan, 2012.
- Fukaya, H.; Yamamoto, K. A study of care for the nonprofessional supporters during large regional disaster. Ritsumeikan Ningenkagaku Kenkyu 2013, 26, 77–83. [Google Scholar]
- Kim, Y.; Shimazu, K.; Kobayashi, M. Disaster Mental Health Activity Guidelines 2016: Review of domestic and international literature for developing a new comprehensive guidelines. In Report for Health Labour Sciences Research Grant; National Center of Neurology and Psychiatry: Tokyo, Japan, 2017. [Google Scholar]
- Local Government Officials Association for the Promotion of Safety and Health. Mental Health Promotion against Critical Incidence Stress in Disaster—Self-care and Organizational Measures; Health Promotion Series of Workplace 61; Local Government Officials Association for the Promotion of Safety and Health: Tokyo, Japan, 2011. [Google Scholar]
- Nagamine, M. Care for care providers during relief activities. Hum. Mind 2017, 194, 117–121. [Google Scholar]
- Nagano Mental Health and Welfare Center. Mental Health Care during Disasters—Manual for Disaster Responders, 3rd ed.; Nagano Mental Health and Welfare Center: Nagano, Japan, 2015. [Google Scholar]
- Narisawa, T.; Suzuki, Y.; Fukasawa, M. Toward development of a guideline for work-related stress management of care-providers in natural disasters; Consensus building through the Delphi process. Jpn. J. Trauma. Stress 2013, 10, 59–69. [Google Scholar]
- Ohtsuka, E.; Matsumoto, J. Secondary traumatization of rescue workers and the mental health care system. Bull. Nagano Coll. Nurs. 2007, 9, 19–27. [Google Scholar]
- Osawa, T. Critical Incident stress measures led by the fire and disaster management agency-from the Great Hanshin-Awaji Earthquake to the great east Japan earthquake, and future prospects. Jpn. J. Trauma. Stress 2013, 11, 17–24. [Google Scholar]
- Shimizu, K. Preparation ahead of the relief activities: Education and training. Hum. Mind 2017, 193, 124–129. [Google Scholar]
- International Recovery Platform Secretariat & United Nations Development Program. Guidance Note on Recovery: Psychosocial; International Recovery Platform Secretariat & United Nations Development Program: Hyogo, Japan, 2010; Available online: https://www.unisdr.org/files/18781_irppsychosocial.pdf (accessed on 2 September 2019).
- Sawaguchi, R.; Misao, H. Support activities for care providers: Lessons learned from the Great East Japan Earthquake. Nursing (London) 2014, 34, 108–115. [Google Scholar]
- Suzuki, Y.; Fukasawa, M.; Nakajima, S.; Narasawa, T.; Kono, K.; Kim, Y. Manual for Disaster Mental Health; National Institute of Mental Health, National Center of Neurology and Psychiatry: Tokyo, Japan, 2011; Available online: https://www.ncnp.go.jp/nimh/seijin/H22DisaManu110311.pdf (accessed on 2 September 2019).
- Abe, Y. Yuragi of volunteer operating in distressed areas and her/his need of care: In terms of volunteer as learner. Waseda Educ. Res. 2012, 3, 27–41. [Google Scholar]
- Fujishiro, T. Critical incident stress management in Japanese police. Jpn. J. Trauma. Stress 2013, 11, 41–49. [Google Scholar]
- Nakanobu, R. How to support nurses who provided disaster nursing care in affected area. Kochi Women Univ. J. Nurs. Acad. 2012, 37, 7–11. [Google Scholar]
- Setou, N. Challenges in supporting the aid workers at the areas afflicted by the Great East Japan earthquake and tsunami -findings through support activities for the bereaved in the disaster areas. Konan Womens Coll. Res. 2013, 7, 49–55. [Google Scholar]
- Yamazaki, T. Support for nurses who experienced critical incident stress in the line of duty. Occup. Ment. Health 2013, 21, 4–8. [Google Scholar]
- Ministry of Health, Labor and Welfare. About the Disaster Health Emergency Assistance Team; Ministry of Health, Labor and Welfare: Tokyo Japan. Available online: http://www.mhlw.go.jp/file/05-Shingikai-10901000-Kenkoukyoku-Soumuka/0000131931.pdf (accessed on 2 September 2019).
- Kato, H. Helper’s help following major disaster. J. Clin. Psychiatry 2013, 55, 1011–1016. [Google Scholar]
- Takahashi, S. Follow up for care providers. Hum. Mind 2017, 196, 113–119. [Google Scholar]
- Mental Health Working Group of Osaka Center for Disabled. Osaka Disabled Liaison Conference for Countermeasure for Emergencies in Great East Japan Earthquake. Available online: http://www.ritsumei.ac.jp/~kohei-y/lab/staff.pdf (accessed on 2 September 2019).
- Ministry of Health, Labor and Welfare. Guidelines for Activities of Child Guidance Center at the Time of Disaster; Ministry of Health, Labor and Welfare: Tokyo, Japan, 2013. Available online: https://www.mhlw.go.jp/bunya/kodomo/pdf/dv130424_1.pdf (accessed on 2 September 2019).
- Ito, T.; Tsukada, Y.; Suzuki, S. Briefing to the nursing staff to be dispatched for the disaster assistance—Attempt of the briefing in Graduate School of Nursing, Chiba University at the 2016 Kumamoto Earthquake. J. Grad. Sch. Nurs. Chiba Univ. 2017, 39, 59–63. [Google Scholar]
- Occupational Safety and Health Administration (OSHA): Outreach Training Program, Disaster Site Worker Procedures. Available online: https://www.osha.gov/dte/outreach/disaster/disaster_procedures.pdf (accessed on 2 September 2019).
- Sato, D.; Shimoyama, M.; Yoshida, T. Evaluation of fatigue among staff in areas stricken by the Great East Japan Earthquake for disaster-related condition nursing. J. Jpn. Soc. Disaster Nurs. 2017, 18, 24–35. [Google Scholar]
- Fuji, N. Group-based support for care providers. Hum. Mind 2017, 192, 68–72. [Google Scholar]
- Osawa, T.; Kato, H. Disaster Stress and Mental Health Countermeasures in Disaster Relief Organization Past and Future; Hyogo Institute for Traumatic Stress: Hyogo, Japan, 2016; Available online: http://www.j-hits.org/function/research/pdf/28_4chouki.pdf (accessed on 2 September 2019).
- UNICEF: Staff Well-Being Guidelines and Good Practice. Available online: http://unicefinemergencies.com/downloads/eresource/docs/3.3%20Human%20Resources/Staff%20Well-Being%20Guidelines%20and%20Good%20Practices%20-%207%20December%202009.pdf (accessed on 2 September 2019).
- Hyogo Nursing Association. Disaster Support Nurse: Manual for Nursing Practice; Hyogo Nursing Association, 2012. Available online: https://www.hna.or.jp/archives/001/201512/saigai_manual.pdf (accessed on 2 September 2019).
- Study Group of Press Workers’ Stress. Manual for Responding Critical Incidence Stress; Study Group of Press Workers’ Stress: Ibaraki, Japan, 2016; Available online: http://www.human.tsukuba.ac.jp/~ymatsui/disaster_manual3.html (accessed on 2 September 2019).
- Suzuki, Y.; Fukasawa, M.; Nakajima, S.; Narisawa, T.; Kim, Y. Development of disaster mental health guidelines through the Delphi process in Japan. Int. J. Ment. Health Syst. 2012, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T. Care for care providers after relief activities. Hum. Mind 2017, 195, 92–96. [Google Scholar]
- Ozaki, A.; Osaka, T.; Ikeda, M.A. Systematic review of psychosocial support by clinical psychologists in disaster. Obirin Psychol. Res. 2016, 7, 33–41. [Google Scholar]
- Japan Psychiatric Hospitals Association. In Guide for Manual Preparation of Disaster Countermeasures at Psychiatric Hospital; Japan Psychiatric Hospitals Association: Tokyo, Japan, 2015.
- King, R.V.; North, C.S.; Larkin, G.L.; Downs, D.L.; Klein, K.R.; Fowler, R.L.; Swienton, R.E.; Pepe, P.E. Attributes of effective disaster responders: Focus group discussions with key emergency response leaders. Disaster Med. Public Health Prep. 2010, 4, 332–338. [Google Scholar] [CrossRef]
- Guilaran, J.; de Terte, I.; Kaniasty, K.; Stephens, C. Psychological outcomes in disaster responders: A systematic review and meta-analysis on the effect of social support. Int. J. Disaster Risk Sci. 2018, 9, 344–358. [Google Scholar] [CrossRef]


{kind=link}
| Disaster Time | Actors | Actions | References |
|---|---|---|---|
| Before | Individual Actions | 1. Gather information on one’s duties and area of operation. 2. Identify possible challenges on site. 3. Assess the readiness of one’s health, work, and family for enrolment. 4. Make an honest decision on whether they could join a disaster-response team. | [27,28,29,30,31,32,33,34,35] |
| Organisational Actions | 1. Train responders in monitoring their stress levels. 2. Address potential work-related stressors. 3. Consider thoroughly who should or should not be dispatched to disaster-affected areas. | [23,24,27,28,31,32,35,36,37,38,39,40,41,42,43,44,45,46,47] | |
| During | Individual Actions | 1. Use a stress checklist to assess the impact of stressors. 2. Accept one’s own emotional reactions and tensions. 3. Re-conceptualise one’s experience during duties, and feelings about them, from different angles. | [29,30,41,48,50] |
| Organisational Actions | 1. Enable responders to monitor their level of stress. 2. Monitor the physical and mental health of responders. | [25,27,37,38,41,43,45,49,50] | |
| After | Individual Actions | 1. Look back on what they experienced and take an objective view of those experiences. 2. Monitor one’s mental health over the long term. | [29,30,35,41,59] |
| Organisational Actions | 1. Recognise disaster-response activities as a contribution to the missions of organisation. 2. Provide responders with opportunities for frankly talking about their experience and feelings. 3. Monitor responder’s mental health over the long term. | [25,28,35,38,41,43,50,51,52,53,54,55,56,57,58,60] |
| Disaster Time | Actors | Actions | References |
|---|---|---|---|
| Before | Individual Actions | 1. Promote and maintain one’s physical and mental states. 2. Develop one’s own self-care plan. 3. Explain to family members about the duties, and set up support and communication. 4. Disentangle one’s concerns at home and at work. | [28,32,40,41,50] |
| Organisational Actions | 1. Improve responders’ basic knowledge and skills of stress management. 2. Improve responders’ teamwork skills. 3. Give responders a concrete idea of what their duties will be. 4. Develop means of communication with responders’ family. 5. Develop an efficient operational system with a clear command chain. 6. Have a written and active policy for preventing and managing the stress of responders. | [23,25,27,28,29,32,35,37,38,39,41,44,47,48,50,60,61,70] | |
| During | Individual Actions | 1. Maintain routines for one’s health. 2. Get enough rest and refresh oneself using the self-care plan. 3. Refrain from too much alcohol, tobacco, and caffeine. 4. Create mutually supportive teams with co-workers. 5. Keep connected with family and friends. 6. Keep a positive attitude in one’s role. | [24,27,28,29,30,31,32,38,41,42,45,48,50,53,59,63,67,68] |
| Organisational Actions | 1. Control the volume and content of work given to responders. 2. Hold a defusing meeting to normalise responders’ reactions to stressors. 3. Support responders’ informal communication with their peers. 4. Develop a peer support system within the team (buddy system). | [25,27,28,29,30,37,38,43,44,45,46,48,50,54,60,64,65,66] | |
| After | Individual Actions | 1. Switch from a disaster-response to routine mode. 2. Take time off from work to recover from physical and psychological fatigue. 3. Spend time with family and friends. | [27,29,30,59,67,68,69] |
| Organisational Actions | 1. Clearly announce the end of disaster-response activities. 2. Ensure that responders can take time off work before returning to their routine there. 3. Provide responders with information on self-care. | [24,25,27,28,35,37,39,41,48,50,57,70,72] |
| Disaster Time | Actors | Actions | References |
|---|---|---|---|
| Before | Individual Actions | Develop personal indicators for extreme fatigue or crisis. | [32] |
| Organisational Actions | 1. Provide training of psychological first aid to make it immediately available to all responders in times of crisis. 2. Develop a system that responds to the traumatic experiences of responders. | [28,36,37,43,45,47,50,56] | |
| During | Individual Actions | 1. Ask for help from mental health professionals. 2. Make a decision as to whether to continue with or resign one’s duties. | [28,30,37,50,55] |
| Organisational Actions | 1. Give the responder time off, or lighten the volume and content of work. 2. Provide support that is specific to the crisis of that responder. 3. Ensure access to professional support from external organisations. 4. Make a decision as to whether the stressed-out responder should remain at the site or be replaced. | [24,25,28,31,37,42,46,48,56,66] | |
| After | Individual Actions | 1. Ask for help from professionals. 2. Take rest until recovery from the mental health crisis. | [37,48,53,56,57,61,71] |
| Organisational Actions | Link responders and their families to social resources, including mental health professionals, to provide the responder with mental health care. | [24,25,27,28,30,36,41,48,49,57,59,72] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umeda, M.; Chiba, R.; Sasaki, M.; Agustini, E.N.; Mashino, S. A Literature Review on Psychosocial Support for Disaster Responders: Qualitative Synthesis with Recommended Actions for Protecting and Promoting the Mental Health of Responders. Int. J. Environ. Res. Public Health 2020, 17, 2011. https://doi.org/10.3390/ijerph17062011
Umeda M, Chiba R, Sasaki M, Agustini EN, Mashino S. A Literature Review on Psychosocial Support for Disaster Responders: Qualitative Synthesis with Recommended Actions for Protecting and Promoting the Mental Health of Responders. International Journal of Environmental Research and Public Health. 2020; 17(6):2011. https://doi.org/10.3390/ijerph17062011
Chicago/Turabian StyleUmeda, Maki, Rie Chiba, Mie Sasaki, Eni Nuraini Agustini, and Sonoe Mashino. 2020. "A Literature Review on Psychosocial Support for Disaster Responders: Qualitative Synthesis with Recommended Actions for Protecting and Promoting the Mental Health of Responders" International Journal of Environmental Research and Public Health 17, no. 6: 2011. https://doi.org/10.3390/ijerph17062011
APA StyleUmeda, M., Chiba, R., Sasaki, M., Agustini, E. N., & Mashino, S. (2020). A Literature Review on Psychosocial Support for Disaster Responders: Qualitative Synthesis with Recommended Actions for Protecting and Promoting the Mental Health of Responders. International Journal of Environmental Research and Public Health, 17(6), 2011. https://doi.org/10.3390/ijerph17062011