Courses on Basic Occupational Safety and Health: A Train-the-Trainer Educational Program for Rural Areas of Latin America

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Description of the Training Program
2.2. Program Evaluation
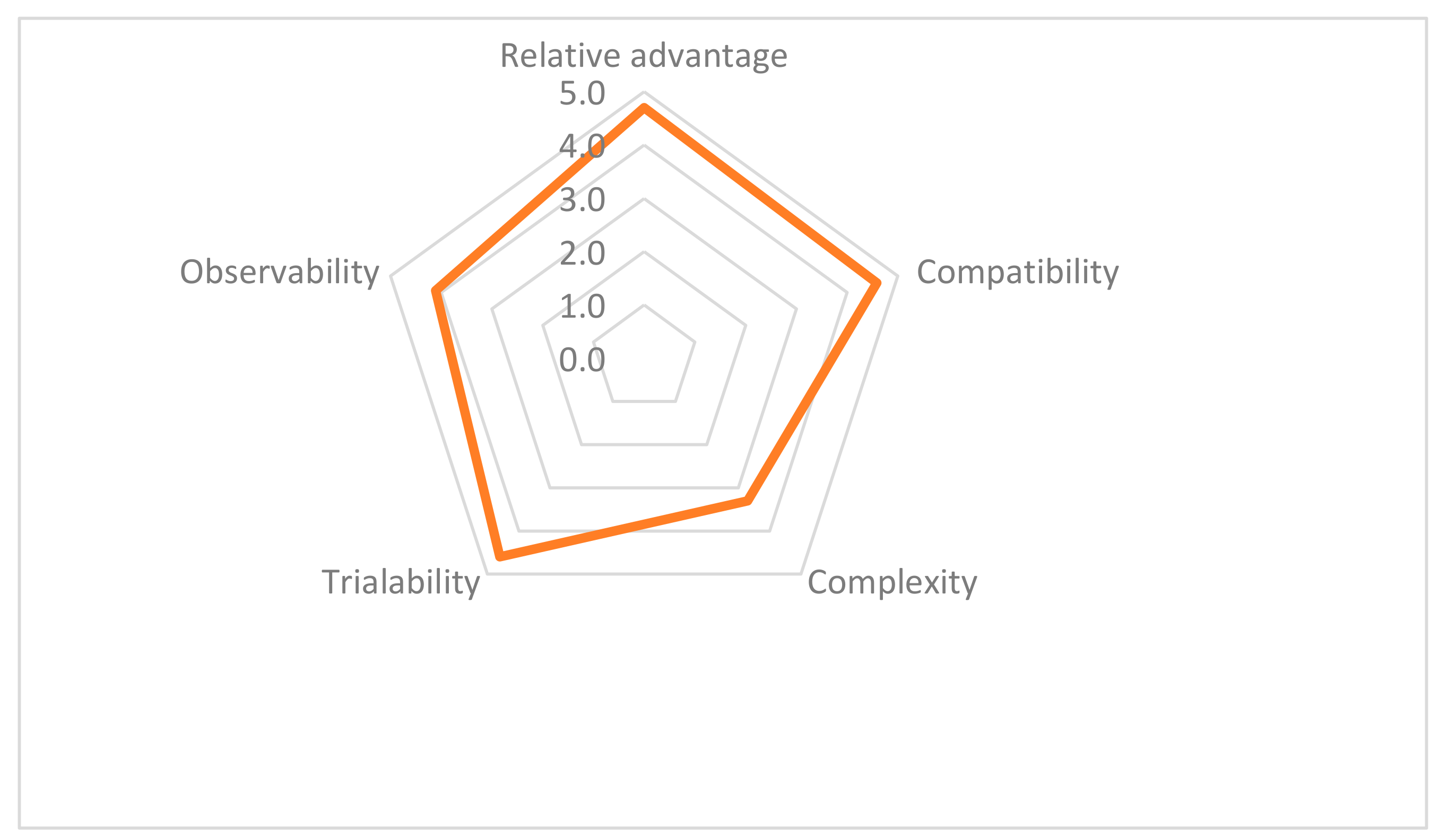
- relative advantage, as “the degree to which an innovation is perceived as being better than the idea it supersedes”;
- compatibility, as “the degree to which an innovation is perceived as consistent with the existing values, past experiences, and needs of potential adopters”;
- complexity, as “the degree to which an innovation is perceived as relatively difficult to understand and use”;
- trialability, as “the degree to which an innovation may be experimented with on a limited basis”;
- observability, as “the degree to which the results of an innovation are visible to others”.
- How and to what extent were the program objectives achieved?
- What facilitated the achievement?
- Which obstacles were identified in the achievement of the objectives?
2.3. Ethical Considerations
3. Results
3.1. Participants and Implementation Experiences
3.2. Quantitative Evaluation Results
3.3. Qualitative Evaluation Results
3.3.1. Evaluation Form
- Relative advantage
“I think that with this, local knowledge is respected, validating the work of the people involved, which is complemented by technical knowledge.”(Translated from local language)
- 2.
- Compatibility
“Community beliefs and values were not altered with the implementation of the different stages of the project; the community vision of health-disease process is based on the Andean worldview where mother earth (Pachamama) intervenes as a source of life, gods such as Apus (tutelary hills) that influence the health-disease process … In this Andean society, the woman plays an important role in the family and at the same time, maintains a certain level of dependence on the male…”(Translated from local language)
“… Considering their work schedules, availability of time and with the participation of assistants of different ages … the educational session was designed (physical exercises) according to health conditions and age … that contribute to improve their ailments without altering their daily work activity.”(Translated from local language)
- 3.
- Complexity
- The isolation and difficult access to the communities due to the geographical remoteness and dispersion of the population within the territory.
- The political-institutional current situation in Latin America, which made it more difficult to carry out the interventions since in some cases, the local authority approved the intervention and when changed, approval had to be sought again from the successor.
- Time demand and management for adjusting interventions according to community characteristics, as pointed out by two trainers:
“It took time to define and prepare educational and audio-visual material because of the schooling and age of the participants.”(Translated from local language)
“The organization and assistance by fishermen were complex, 100% was not reached due to work activities of the participants.”(Translated from local language)
- Lack of policies in primary healthcare and lack of intersectoral action addressing workers’ health issues. Trainers stated:
“My view of being complex is based on the fact that it requires intense coordination of actions which are not always easy. Primary care does not have a work plan in the area [of occupational health]. Therefore, these efforts imply additional commitments, especially if a greater impact to be achieved”.(Translated from local language)
“I think skills for this kind of work could be strengthened in the healthcare team.”(Translated from local language)
“… I think it is necessary to incorporate follow-up and to develop other instances of intervention, like networking and intersectoral work.”(Translated from local language)
- Lack of financial support for teaching interventions (e.g., staff time, travel, and material costs).
“We had constant support from the university… this allowed us to have sufficient teaching hours, finance travel costs, coffee breaks, materials… Local primary healthcare center contemplated the necessary professional hours, as well as time for coordination of actions with social and institutional organizations.”(Translated from local language)
- 4.
- Trialability
“Since the disease model in general has changed, it is important to consider social factors in interventions. Participatory diagnosis and educational intervention models in communities are useful for the development of respectful strategies in which the community is involved.”(Translated from local language)
- 5.
- Observability
“I think we should work with local authorities on a results basis to achieve greater impact.”
“… for the community, the problems arising from the current legislation are more complex …”(Translated from local language)
3.3.2. Program Evaluation Workshop
“In general, the objectives were achieved, it was possible to make diagnosis of the community’s health problems and their occupational risks. No intervention was carried out.”(Translated from local language)
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Labour Organization. Thematic Labour Overview 3: Working in Rural Areas in the 21st Century. Reality and Prospects of Rural Employment in Latin America and the Caribbean. 2017. Available online: https://www.ilo.org/global/topics/economic-and-social-development/rural-development/WCMS_545431/lang--en/index.htm (accessed on 16 January 2020).
- International Labour Organization. Promoting Rural Development through Occupational Safety and Health. 2013. Available online: http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_222333.pdf (accessed on 15 November 2019).
- Benach, J.; Muntaner, C.; Chung, H.; Benavides, F.G. Immigration, employment relations, and health: Developing a research agenda. Am. J. Ind Med. 2010, 53, 338–343. [Google Scholar] [CrossRef] [PubMed]
- International Labour Organization. The Labour Situation of Indigenous Women in Peru—A Study. 2016. Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/publication/wcms_546285.pdf (accessed on 22 February 2020).
- Molineri, A.I.; Signorini-Porchietto, M.L.; Tarabla, H.D. Hazards for women and children in rural settings. Rev. Salud Publica 2015, 17, 22–32. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Xavier, D.M.; Cezar-Vaz, M.R.; Bonow, C.A.; Schimith, M.D. Work accidents with children and youth in a rural environment in southern Brazil. Rev. Lat.-Am. Enferm. 2020, 28, e3243. [Google Scholar] [CrossRef] [PubMed]
- Pinedo Herrera, C.; Zambrano Carrillo, M.F.; Castro, K. Prácticas de salud ocupacional y niveles de biomarcadores séricos en aplicadores de plaguicidas de cultivos de arroz en Natagaima-Tolima, Colombia. Rev. Tox. 2015, 32, 102–106. [Google Scholar]
- Mathez-Stiefel, S.-L.; Vandebroek, I.; Rist, S. Can Andean medicine coexist with biomedical healthcare? A comparison of two rural communities in Peru and Bolivia. J. Ethnobiol. Ethnomed. 2012, 8, 26. [Google Scholar] [CrossRef]
- Guile, L.; Graham, D.; Jachmann, A. Health and demographic characteristics of patients attending a newly-opened medical facility in a remote Amazonian community: A descriptive study. Med. Sci. 2018, 6, 106. [Google Scholar] [CrossRef]
- Laborde, A.; Tomasina, F.; Bianchi, F.; Brune, M.N.; Buka, I.; Comba, P.; Corra, L.; Cori, L.; Duffert, C.M.; Harari, R.; et al. Children’s health in Latin America: The influence of environmental exposures. Environ. Health Perspect. 2015, 123, 201–209. [Google Scholar] [CrossRef]
- Gibb, H.; O’Leary, K.G. Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: A comprehensive review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef]
- Schwartz, N.A.; von Glascoe, C.A.; Torres, V.; Ramos, L.; Soria-Delgado, C. “Where they (live, work and) spray”: Pesticide exposure, childhood asthma and environmental justice among Mexican-American farmworkers. Health Place 2015, 32, 83–92. [Google Scholar] [CrossRef]
- International Labour Organization. Decent Work and the 2030 Agenda for Sustainable Development. 2017. Available online: http://ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/documents/publication/wcms_436923.pdf (accessed on 14 November 2019).
- International Labour Organization. Decent Work. 2015. Available online: https://www.ilo.org/global/topics/decent-work/lang--en/index.htm (accessed on 19 February 2020).
- Food and Agriculture Organization of the United Nations. Incorporating Decent Rural Employment in the Strategic Planning for Agricultural Development. 2016. Available online: http://www.fao.org/3/a-i5471e.pdf (accessed on 16 January 2020).
- Buijs, P.C.; Gunnyeon, B.; van Weel, C. Primary health care: What role for occupational health? Br. J. Gen. Pract. 2012, 62, 623–624. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Plan of Action on Worker’s Health 2008–2017. Universal Health Coverage for the Working Poor. 2007. Available online: https://www.who.int/occupational_health/activities/flyer_universal_health_coverage2013.pdf?ua=1 (accessed on 21 February 2020).
- World Health Organization. Connecting Health and Labour. Bringing Together Occupational Health and Primary Care to Improve the Health of Working People. 2012. Available online: https://www.who.int/occupational_health/publications/the-hague-summary-040512-A4web.pdf?ua=1 (accessed on 22 February 2020).
- Scheil-Adlung, X. Global Evidence on Inequities in Rural Health Protection: New Data on Rural Deficits in Health Coverage for 174 Countries. 2015. Available online: http://www.ilo.org/secsoc/information-resources/publications-and-tools/Workingpapers/WCMS_383890/lang--en/index.htm (accessed on 9 March 2020).
- Van Dijk, F.J.; Bubas, M.; Smits, P.B. Evaluation studies on education in occupational safety and health: Inspiration for developing economies. Ann. Glob. Health 2015, 81, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization; World Health Organization—Regional Office for the Americas. Plan of Action on Workers’ Health 2015–2025. 2015. Available online: http://iris.paho.org/xmlui/bitstream/handle/123456789/33986/CD54_10Rev.1-eng.pdf?sequence=1&isAllowed=y (accessed on 21 February 2020).
- Nogueira, D.P. Incorporação da saúde ocupacional à rede primária de saúde. Rev. Saude Publ. 1984, 18, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Bombardi, L.M. Geografia do uso de agrotóxicos no Brasil e conexões com a União Europeia. 2017. Available online: http://conexaoagua.mpf.mp.br/arquivos/agrotoxicos/05-larissa-bombardi-atlas-agrotoxico-2017.pdf (accessed on 22 February 2020).
- Silverio, A.C.P.; Martins, I.; Nogueira, D.A.; Mello, M.A.S.; Loyola, E.A.C.; Graciano, M.M.C. Assessment of primary health care for rural workers exposed to pesticides. Rev. Saude Publ. 2020, 54, 09. [Google Scholar] [CrossRef] [PubMed]
- Simmons, J.M.; Liebman, A.K.; Sokas, R.K. Occupational health in community health centers: Practitioner challenges and recommendations. New Solut. 2018, 28, 110–130. [Google Scholar] [CrossRef]
- Colon-Gonzalez, M.C.; El Rayess, F.; Guevara, S.; Anandarajah, G. Successes, challenges and needs regarding rural health medical education in continental Central America: A literature review and narrative synthesis. Rural Remote Health 2015, 15, 3361. [Google Scholar]
- Siribie, M.; Ajayi, I.O.; Nsungwa-Sabiiti, J.; Afonne, C.; Balyeku, A.; Falade, C.O.; Gansane, Z.; Jegede, A.S.; Ojanduru, L.; Oshiname, F.O.; et al. Training community health workers to manage uncomplicated and severe malaria: Experience from 3 rural malaria-endemic areas in Sub-Saharan Africa. Clin. Infect. Dis. 2016, 63, S264–S269. [Google Scholar] [CrossRef]
- Amerson, R.; Hall-Clifford, R.; Thompson, B.; Comninellas, N. Implementation of a training program for low-literacy promotoras in oral rehydration therapy. Public Health Nurs. 2015, 32, 177–185. [Google Scholar] [CrossRef]
- Quandt, S.A.; Grzywacz, J.G.; Talton, J.W.; Trejo, G.; Tapia, J.; D’Agostino, R.B., Jr.; Mirabelli, M.C.; Arcury, T.A. Evaluating the effectiveness of a lay health promoter-led, community-based participatory pesticide safety intervention with farmworker families. Health Promot. Pract. 2013, 14, 425–432. [Google Scholar] [CrossRef]
- Baron, S.L.; Beard, S.; Davis, L.K.; Delp, L.; Forst, L.; Kidd-Taylor, A.; Liebman, A.K.; Linnan, L.; Punnett, L.; Welch, L.S. Promoting integrated approaches to reducing health inequities among low-income workers: Applying a social ecological framework. Am. J. Ind. Med. 2014, 57, 539–556. [Google Scholar] [CrossRef]
- Arenas-Monreal, L.; Cortez-Lugo, M.; Parada-Toro, I.; Pacheco-Magana, L.E.; Magana-Valladares, L. Population health diagnosis with an ecohealth approach. Rev. Saude Publ. 2015, 49, s0034–s8910. [Google Scholar] [CrossRef]
- Anchundia, L.; Mendoza, J.; Anton, A. Educación en salud, seguridad y formación ocupacional. Rev. Arbitr. Interdiscip. Cienc. 2019, 3, 453. [Google Scholar] [CrossRef]
- Tamayo-Ortiz, M.; Navia-Antezana, J. Reduced lead exposure following a sensitization program in rural family homes producing traditional mexican ceramics. Ann. Glob. Health 2018, 84, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Vilchis-Rea, M.; López-Hernández, E. Factores de riesgo laboral en bomberos mexicanos de cuatro estaciones: Investigación- acción participativa. Rev. Colomb. Salud Ocup. 2016, 6, 124–131. [Google Scholar] [CrossRef]
- Federal Ministry for Economic Cooperation and Development. Available online: http://www.bmz.de/en (accessed on 9 March 2020).
- German Academic Exchange Service. Available online: https://www.daad.de/en/ (accessed on 9 March 2020).
- Center for International Health at the Ludwig-Maximilians-Universität München. Available online: www.cih.lmu.de (accessed on 9 March 2020).
- Kenny, A.; Farmer, J.; Dickson-Swift, V.; Hyett, N. Community participation for rural health: A review of challenges. Health Expect. 2015, 18, 1906–1917. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.; Baghri, S.; Reed, B. Community participation. In Emergency Sanitation: Assessment and Programme Design; WEDC Publications; Loughborough University: Loughborough, UK, 2002; p. 177. [Google Scholar]
- Betancourt, O.; Mertens, F.; Parra, M. Ecosistemas y salud humana. In Enfoques Ecosistémicos en Salud y Ambiente, 1st ed.; Ediciones Abya-Yala: Quito, Ecuador, 2016. [Google Scholar]
- Garrido, M.A.; Parra, M.; Diaz, J.; Medel, J.; Nowak, D.; Radon, K. Occupational safety and health in a community of shellfish divers: A community-based participatory approach. J. Community Health 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- CASUS – E-learning & E-teaching software for virtual patients. Available online: https://www.instruct.eu/ (accessed on 9 March 2020).
- García Gómez, M.M. Los mapas de riesgos. Concepto y metodologia para su elaboración. Rev. Esp. Salud Publica 2008, 68, 11. [Google Scholar]
- Felder, R.M.; Brent, R. Teaching and Learning STEM: A Practical Guide, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 2016. [Google Scholar]
- Städeli, C.; Grassi, A.; Rhiner, K.; Obrist, W. Kompetenzorientiert Unterrichten-das AVIVA Modell, 2nd ed.; Hep Verlag AG: Bern, Switzerland, 2013. [Google Scholar]
- Rogers, E.M. Elements of diffusion. In Diffusion of Innovations, 3rd ed.; The Free Press: New York, NY, USA, 1983; pp. 10–16. [Google Scholar]
- Smith, J.; Firth, J. Qualitative data analysis: The framework approach. Nurse Res. 2011, 18, 52–62. [Google Scholar] [CrossRef]
- Anderson, B.T.; Johnson, G.J.; Wheat, J.R.; Wofford, A.S.; Wiggins, O.S.; Downey, L.H. Farmers’ concerns: A qualitative assessment to plan rural medical education. J. Rural Health 2012, 28, 115–121. [Google Scholar] [CrossRef]
- Kaewboonchoo, O.; Silpasuwan, P.; Jirapongsuwan, A.; Rawiworrakul, T.; Hansing, S. Participatory capacity building in occupational disease surveillance among primary care unit health personnel. Southeast Asian J. Trop. Med. Public Health 2011, 42, 1262–1268. [Google Scholar]
- Pena, P.G.; Gomez, C.M. Health of subsistence fishermen and challenges for occupational health surveillance. Cien Saude Colet 2014, 19, 4689–4698. [Google Scholar] [CrossRef]
- Buijs, P.C.; Weel, A.N.; Nauta, N.P.; Anema, H.R.; Schoonheim, P.L.; Helsloot, R.S. Teaching general practitioners and occupational physicians to cooperate: Joint training to provide better care for European workers. Eur. J. Gen. Pract. 2009, 15, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Hussey, L.; Turner, S.; Thorley, K.; McNamee, R.; Agius, R. Comparison of work-related ill health reporting by occupational physicians and general practitioners. Occup. Med. 2010, 60, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Ahonen, E.Q.; Fujishiro, K.; Cunningham, T.; Flynn, M. Work as an inclusive part of population health inequities research and prevention. Am. J. Public Health 2018, 108, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Cole, D.C.; McLaughlin, J.E.; Hennebry, J.L.; Tew, M.A. Precarious patients: Health professionals’ perspectives on providing care to Mexican and Jamaican migrants in Canada’s Seasonal Agricultural Worker Program. Rural Remote Health 2019, 19, 5313. [Google Scholar] [CrossRef] [PubMed]
- Sastre, F.; Rojas, P.; Cyrus, E.; De La Rosa, M.; Khoury, A.H. Improving the health status of Caribbean people: Recommendations from the Triangulating on Health Equity summit. Glob. Health Promot. 2014, 21, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Jors, E.; Konradsen, F.; Huici, O.; Morant, R.C.; Volk, J.; Lander, F. Impact of training Bolivian farmers on integrated pest management and diffusion of knowledge to neighboring farmers. J. Agromedicine 2016, 21, 200–208. [Google Scholar] [CrossRef]
- Kim, J.; Arrandale, V.H.; Kudla, I.; Mardell, K.; Lougheed, D.; Holness, D.L. Educational intervention among farmers in a community health care setting. Occup. Med. 2012, 62, 458–461. [Google Scholar] [CrossRef][Green Version]
- Nilvarangkul, K.; Arphorn, S.; Smith, J.; Phajan, T.; Kessomboon, N.; Thaewnongiew, K. Developing primary care occupational health services for informal sector workers in Thailand. Action Res. 2015, 14, 113–131. [Google Scholar] [CrossRef]
- Rafiei, M.; Ezzatian, R.; Farshad, A.; Sokooti, M.; Tabibi, R.; Colosio, C. Occupational health services integrated in primary health care in Iran. Ann. Glob. Health 2015, 81, 561–567. [Google Scholar] [CrossRef]
- Lucchini, R.G.; McDiarmid, M.; Van der Laan, G.; Rosen, M.; Placidi, D.; Radon, K.; Ruchirawat, M.; Kurtz, L.; Landrigan, P. Education and training: Key factors in global occupational and environmental health. Ann. Glob. Health 2018, 84, 436–441. [Google Scholar] [CrossRef]
- Hege, I.; Ropp, V.; Adler, M.; Radon, K.; Masch, G.; Lyon, H.; Fischer, M.R. Experiences with different integration strategies of case-based e-learning. Med. Teach. 2007, 29, 791–797. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Phase | Activity | Topic | Content/Activities for the Trainers | Time Period |
|---|---|---|---|---|
| Participatory diagnosis | 1-h problem-based e-learning for trainers | Work-related hazards and risks in rural areas | Basic information on:
| March–April 2018 |
| Three-day face-to-face workshop for trainers | Participatory diagnosis of working conditions and health |
| April 2018 | |
| One-day workshop for community members offered by trainers | Implementation of the participatory diagnosis of working conditions and health |
| May–July 2018 | |
| Teaching intervention | 2-h problem-based e-learning for trainers | Introduction to teaching interventions |
| July–August 2018 |
| Three-day face-to-face workshop for trainers | Teaching interventions to address work-related health challenges in rural communities |
| August 2018 | |
| Half-day workshop for community members offered by trainers | Implementation of the teaching interventions |
| September–November 2018 | |
| Evaluation | Online questionnaire for trainers | November 2018 | ||
| Evaluation workshop for trainers | September 2019 | |||
| Trainers’ Teams | Communities/ Country | Phase I: Participatory Diagnosis | Phase II: Teaching Intervention | Further Activities | ||
|---|---|---|---|---|---|---|
| Community Participants | Work-Related Risks and Resulting Health Problems Identified | Community Participants | Content | |||
| 1 1 | Artisanal fishermen/Peru | N = 6 (3 women) Representatives of
|
| N = 11 men (0 women)Representatives of:
| Self-control of mental distress in artisanal fishermen |
|
| 2 2 | Potato and quinoa farmers/Peru | N = 20 (6 women) Representatives of:
|
| N = 26 (13 women)Representatives of:
| Prevention of lower back musculoskeletal disorders |
|
| 3 3 | Pottery makers/Chile | N = 17 (14 women)Representatives of:
|
| Session 1: N = 16 (14 women)Representatives of:
| Prevention of musculoskeletal disorders | Since 2018, best practices in health projects including:
|
| 4 4 | Artisanal fishermen/Chile | N = 5 (2 women) Representatives of:
|
| Not implemented due to time constraints of the team of trainers and community members | Prevention of musculoskeletal disorders | None |
| Facilitating Factors | Situations to Which These Factors Applied |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Hindering factors | Situations to which these factors applied and potential solutions. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrido, M.A.; Encina, V.; Solis-Soto, M.T.; Parra, M.; Bauleo, M.F.; Meneses, C.; Radon, K. Courses on Basic Occupational Safety and Health: A Train-the-Trainer Educational Program for Rural Areas of Latin America. Int. J. Environ. Res. Public Health 2020, 17, 1842. https://doi.org/10.3390/ijerph17061842
Garrido MA, Encina V, Solis-Soto MT, Parra M, Bauleo MF, Meneses C, Radon K. Courses on Basic Occupational Safety and Health: A Train-the-Trainer Educational Program for Rural Areas of Latin America. International Journal of Environmental Research and Public Health. 2020; 17(6):1842. https://doi.org/10.3390/ijerph17061842
Chicago/Turabian StyleGarrido, Marie Astrid, Verónica Encina, María Teresa Solis-Soto, Manuel Parra, María Fernanda Bauleo, Claudia Meneses, and Katja Radon. 2020. "Courses on Basic Occupational Safety and Health: A Train-the-Trainer Educational Program for Rural Areas of Latin America" International Journal of Environmental Research and Public Health 17, no. 6: 1842. https://doi.org/10.3390/ijerph17061842
APA StyleGarrido, M. A., Encina, V., Solis-Soto, M. T., Parra, M., Bauleo, M. F., Meneses, C., & Radon, K. (2020). Courses on Basic Occupational Safety and Health: A Train-the-Trainer Educational Program for Rural Areas of Latin America. International Journal of Environmental Research and Public Health, 17(6), 1842. https://doi.org/10.3390/ijerph17061842