Health Consequences for E-Waste Workers and Bystanders—A Comparative Cross-Sectional Study

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
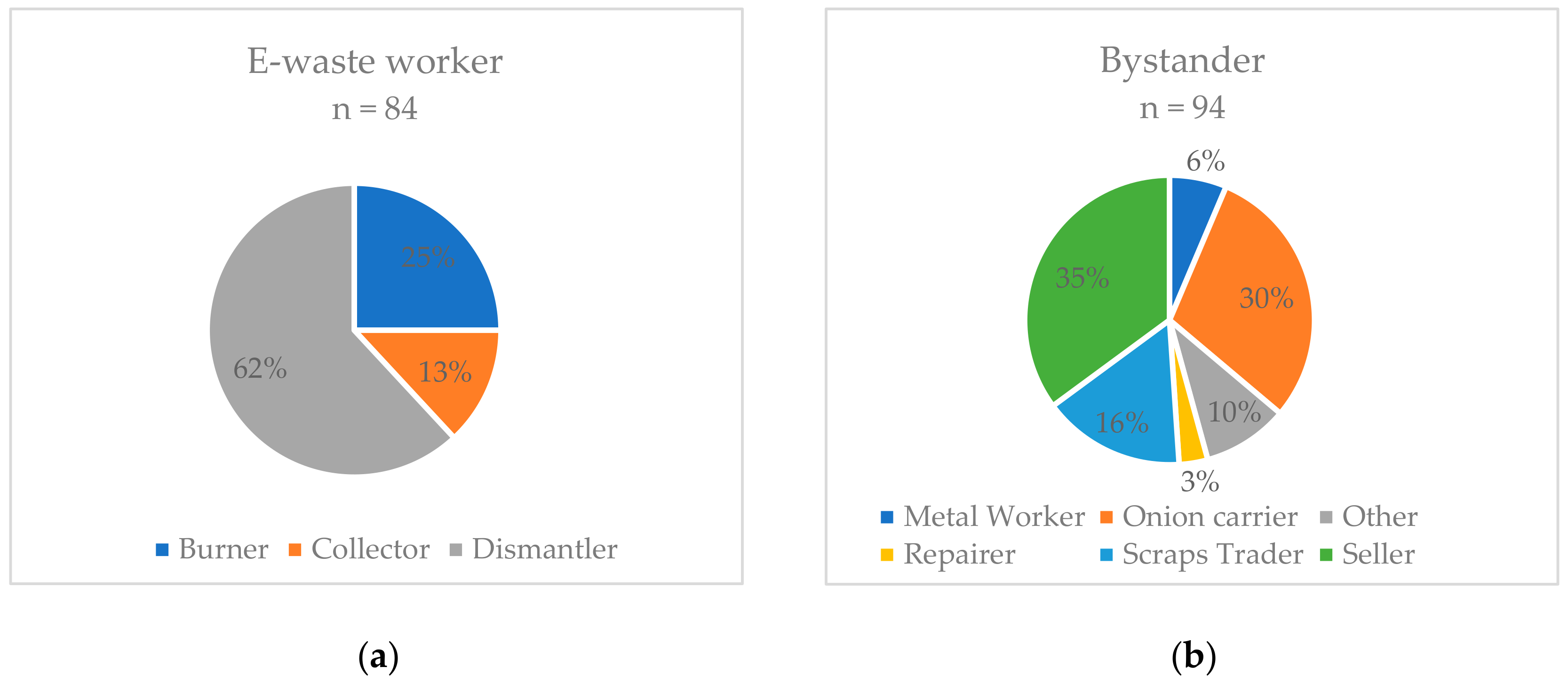
2.1. Study Population
2.2. Questionnaire
- Personal information: Age, sex, marital status, level of education, religion, and residency.
- Occupational information: Working with e-waste, specific task, duration of working, use of personal protection equipment, and specification of control group occupation.
- Habits/Lifestyle: Dietary habits, smoking, and drug use.
- Medical information: Current complaints, such as diseases of the skin, infections, psychiatric disorders, diseases of the eyes and ears, cardiovascular diseases, lung diseases, musculoskeletal diseases, and injuries.
- Pre-existing medical care: Location of medical care, frequency, and health insurance status.
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baldé, C.P.; Forti, V.; Gray, V.; Kuehr, R.; Stegmann, P. The Global E-Waste Monitor–2017; United Nations University (UNU), International Telecommunication Union (ITU) & International Solid Waste Association (ISWA): Bonn, Germany; Geneva, Switzerland; Vienna, Austria, 2017; pp. 4–7. Available online: http://collections.unu.edu/eserv/UNU:6341/Global-E-waste_Monitor_2017__electronic_single_pages_.pdf (accessed on 6 October 2019).
- Schluep, M.; Manhart, A.; Osibanjo, O.; Rochat, D.; Isarin, N.; Mueller, E. Where are WEee in Africa? Findings from the Basel Convention E-Waste Africa Program; Secretariat of the Basel Convention: Châtelaine, Switzerland, 2011; pp. 19–24. Available online: http://www.basel.int/Portals/4/download.aspx?d=UNEP-CHW-EWASTE-PUB-WeeAfricaReport.English.pdf (accessed on 6 October 2019).
- Blacksmith Institute. The World’s Worst 2013: The Top Ten Toxic Threats. Cleanup, Progress and Ongoing Challenges; Blacksmith Institute (now: Pure earth): New York, NY, USA, 2013; pp. 10–12. Available online: https://www.worstpolluted.org/docs/TopTenThreats2013.pdf (accessed on 6 October 2019).
- Amankwaa, E.F.; Tsikudo, A.K.A.; Bowman, J. Recyclers at Risk; E-33113-GHA-1 Working Paper; International Growth Centre, London School of Economic and Political Science: London, UK, 2016; Available online: https://www.theigc.org/wp-content/uploads/2016/11/Armankwaa-and-Tsikudo-2016-working-paper.pdf (accessed on 6 October 2019).
- Amoyaw-Osei, Y.; Agyekum, O.O.; Pwamand, J.A.; Mueller, E.; Fasko, R.; Schluep, M. Ghana e-Waste Country Assessment; SBC e-Waste Africa Project; Secretariat of the Basel Convention: Châtelaine, Switzerland, 2011; pp. 1–3. Available online: http://www.basel.int/Portals/4/Basel%20Convention/docs/eWaste/E-wasteAssessmentGhana.pdf (accessed on 6 October 2019).
- Akormedi, M.; Asampong, E.; Fobil, J.N. Working conditions and environmental exposures among electronic waste workers in Ghana. Int. J. Occup. Environ. Health 2013, 9, 278–286. [Google Scholar] [CrossRef]
- Caravanos, J.; Clarke, E.E.; Osei, C.S.; Amoyaw-Osei, Y. Exploratory Health Assessment of Chemical Exposures at E-Waste Recycling and Scrapyard Facility in Ghana. J. Heal. Pollut. 2013, 3, 11–22. [Google Scholar] [CrossRef]
- Oteng-Ababio, M.; Chama, M.A.; Amankwaa, E.F. Qualitative analysis of the presence of PBDE in ashes, soils and vegetables from Agbogbloshie e-waste recycling site. E3 J. Environ. Res. Manag. 2014, 5, 71–80, ISSN: 2141-7466. [Google Scholar]
- Brigden, K.; Labunska, I.; Santillo, D.; Johnston, P. Chemical Contamination at e-Waste Recycling and Disposal Sites in Accra and Korforidua, Ghana; Greenpeace International: Amsterdam, The Netherlands, 2008; Available online: http://www.greenpeace.to/publications/chemical-contamination-at-e-wa.pdf (accessed on 6 October 2019).
- Srigboh, R.K.; Basu, N.; Stephens, J.; Asampong, E.; Perkins, M.; Neitzel, R.L.; Fobil, J. Multiple elemental exposures amongst workers at the Agbogbloshie electronic waste (e-waste) site in Ghana. Chemosphere 2016, 164, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Wittsiepe, J.; Feldt, T.; Till, H.; Burchard, G.; Wilhelm, M.; Fobil, J.N. Pilot study on the internal exposure to heavy metals of informal-level electronic waste workers in Agbogbloshie, Accra, Ghana. Environ. Sci. Pollut. Res. 2017, 24, 3097–3107. [Google Scholar] [CrossRef] [PubMed]
- Feldt, T.; Fobil, J.N.; Wittsiepe, J.; Wilhelm, M.; Till, H.; Zoufaly, A.; Burchard, G.; Göen, T. High levels of PAH-metabolites in urine of e-waste recycling workers from Agbogbloshie, Ghana. Sci. Total Environ. 2014, 466–467, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Asante, K.A.; Agusa, T.; Biney, C.A.; Agyekum, W.A.; Bello, M.; Otsuka, M.; Itai, T.; Takahashi, S.; Tanabe, S. Multi-trace element levels and arsenic speciation in urine of e-waste recycling workers from Agbogbloshie, Accra in Ghana. Sci. Total Environ. 2012, 424, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Grant, K.; Goldizen, F.C.; Sly, P.D.; Brune, M.; Neira, M.; van den Berg, M.; Norman, R.E. Health consequences of exposure to e-waste: A systematic review. Lancet Glob. Heal. 2013, 1, e350–e361. [Google Scholar] [CrossRef]
- Asampong, E.; Dwuma-Badu, K.; Stephens, J.; Srigboh, R.; Neitzel, R.; Basu, N.; Fobil, J.N. Health seeking behaviours among electronic waste workers in Ghana. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Burns, K.N.; Sun, K.; Fobil, J.N.; Neitzel, R.L. Heart rate, stress, and occupational noise exposure among electronic waste recycling workers. Int. J. Environ. Res. Public Health 2016, 13, 140. [Google Scholar] [CrossRef]
- Burns, K.N.; Sayler, S.K.; Neitzel, R.L. Stress, health, noise exposures, and injuries among electronic waste recycling workers in Ghana. J. Occup. Med. Toxicol. 2019, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ohajinwa, C.M.; Van Bodegom, P.M.; Vijver, M.G.; Olumide, A.O.; Osibanjo, O.; Peijnenburg, W.J.G.M. Prevalence and injury patterns among electronic waste workers in the informal sector in Nigeria. Inj. Prev. 2018, 24, 185–192. [Google Scholar] [CrossRef]
- Yu, E.A.; Akormedi, M.; Asampong, E.; Meyer, C.G.; Fobil, J.N. Informal processing of electronic waste at Agbogbloshie, Ghana: workers’ knowledge about associated health hazards and alternative livelihoods. Glob. Health Promot. 2017, 24, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Bogale, D.; Kumie, A.; Tefera, W. Assessment of occupational injuries among Addis Ababa city municipal solid waste collectors: A cross-sectional study. BMC Public Health 2014, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gutberlet, J.; Baeder, A.M. Informal recycling and occupational health in Santo André, Brazil. Int. J. Environ. Health Res. 2008, 18, 1–15. [Google Scholar] [CrossRef]
- Norman, R.E.; Carpenter, D.O.; Scott, J.; Brune, M.N.; Sly, P.D. Environmental exposures: An underrecognized contribution to noncommunicable diseases. Rev. Environ. Health 2013, 28, 59–65. [Google Scholar] [CrossRef]
- Lichtenstein, P.; Holm, N.V.; Verkasalo, P.K.; Iliadou, A.; Kaprio, J.; Koskenvou, M.; Pukkala, E.; Skytthe, A.; Hemminki, K. Environmental and Heritable Factors in the Causation of Cancer—Analyses of Cohorts of Twins from Sweden, Denmark, and Finland. N. Engl. J. Med. 2000, 343, 78–85. [Google Scholar] [CrossRef]
- Soto-Martinez, M.; Sly, P.D. Relationship between environmental exposures in children and adult lung disease: The case for outdoor exposures. Chron. Respir. Dis. 2010, 7, 173–186. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Eviron. Health. Perspect. 2005, 113, 894–899. [Google Scholar] [CrossRef]
- Dirinck, E.; Jorens, P.G.; Covaci, A.; Geens, T.; Roosens, L.; Neels, H.; Mertens, I.; Van Gaal, L. Obesity and Persistent Organic Pollutants: Possible Obesogenic Effect of Organochlorine Pesticides and Polychlorinated Biphenyls. Obesity 2011, 19, 709–714. [Google Scholar] [CrossRef]
- Lee, D.; Lee, I.; Song, K.; Steffes, M.; Toscano, W.; Baker, B.A.; Jacobs, D.R. A strong dose-response relation between serum concentrations of persistent organic pollutants and diabetes: Results from the National Health and Examination Survey 1999–2002. Diabetes Care 2006, 29, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Goncharov, A.; Pavuk, M.; Foushee, H.R.; Carpenter, D.O. For the Anniston Environmental Health Research Consortium. Blood Pressure in Relation to Concentrations of PCB Congeners and Chlorinated Pesticides. Eviron. Health. Perspect. 2011, 119, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Y.; Liu, Q.; Wang, F.; Nie, J.; Qian, Y. Examining the relationship between brominated flame retardants (BFR) exposure and changes of thyroid hormone levels around e-waste dismantling sites. Int. J. Environ. Health 2010, 213, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huo, X.; Liu, J.; Peng, L.; Li, W.; Xu, X. Assessment of cadmium exposure for neonates in Guiyu, an electronic waste pollution site of China. Environ. Monit. Assess. 2011, 177, 343–351. [Google Scholar] [CrossRef]
- Wu, K.; Xu, X.; Peng, L.; Liu, J.; Guo, Y.; Huo, X. Association between maternal exposure to perfluorooctanoic acid (PFOA) from electronic waste recycling and neonatal health outcomes. Environ. Int. 2012, 48, 1–8. [Google Scholar] [CrossRef]
- Xu, X.; Yang, H.; Chen, A.; Zhou, Y.; Wu, K.; Liu, J.; Zhang, Y.; Huo, X. Birth outcomes related to informal e-waste recycling in Guiyu, China. Reprod. Toxicol. 2012, 33, 94–98. [Google Scholar] [CrossRef]
- Liu, J.; Xu, X.; Wu, K.; Piao, Z.; Huang, J.; Guo, Y.; Li, W.; Zhang, Y.; Chen, A.; Huo, X. Association between lead exposure from electronic waste recycling and child temperament alterations. Neurotoxicology 2011, 32, 458–464. [Google Scholar] [CrossRef]
- Li, Y.; Xu, X.; Wu, K.; Chen, G.; Liu, J.; Chen, S.; Gu, C.; Zhang, B.; Zheng, L.; Zheng, M.; et al. Monitoring of lead load and its effect on neonatal behavioral neurological assessment scores in Guiyu, an electronic waste recycling town in China. J. Environ. Monit. 2008, 10, 1233–1238. [Google Scholar] [CrossRef]
- Zheng, G.; Xu, X.; Li, B.; Wu, K.; Yekeen, T.A.; Huo, X. Association between lung function in school children and exposure to three transition metals from an e-waste recycling area. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 67–72. [Google Scholar] [CrossRef]
- Liu, Q.; Cao, J.; Li, K.Q.; Miao, X.H.; Li, G.; Fan, F.Y.; Zhao, Y.C. Chromosomal aberrations and DNA damage in human populations exposed to the processing of electronics waste. Environ. Sci. Pollut. Res. 2009, 16, 329–338. [Google Scholar] [CrossRef]
- Otsuka, M.; Itai, T.; Asante, K.A.; Muto, M.; Tanabe, S. Trace Element Contamination around the E-waste Recycling Site at Agbogbloshie, Accra City, Ghana. Interdiscip. Stud. Environ. Chem. 2012, 6, 161–167. [Google Scholar]
- Hosoda, J.; Ofosu-Anim, J.; Sabi, E.B.; Akita, L.G.; Onwona-Agyeman, S.; Yamashita, R.; Takada, H. Monitoring of organic micropollutants in Ghana by combination of pellet watch with sediment analysis: E-waste as a source of PCBs. Mar. Pollut. Bull. 2014, 86, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Z.; Gao, Y.; Wu, S.C.; Zhang, H.B.; Cheung, K.C.; Wong, M.H. Distribution of polycyclic aromatic hydrocarbons in soils at Guiyu area of China, affected by recycling of electronic waste using primitive technologies. Chemosphere 2006, 65, 1500–1509. [Google Scholar] [CrossRef]
- Wong, C.S.C.; Duzgoren-Aydin, N.S.; Aydin, A.; Wong, M.H. Evidence of excessive releases of metals from primitive e-waste processing in Guiyu, China. Environ. Pollut. 2007, 148, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, A.; Schluep, M.; Renaud, F.G.; Streicher, M.; Kuehr, R.; Hagelüken, C.; Gerecke, A.C. A review of the environmental fate and effects of hazardous substances released from electrical and electronic equipments during recycling: Examples from China and India. Environ. Impact Assess. Rev. 2010, 30, 28–41. [Google Scholar] [CrossRef]
- Robinson, B.H. E-waste: An assessment of global production and environmental impacts. Sci. Total Environ. 2009, 408, 183–191. [Google Scholar] [CrossRef]
- Alabi, O.A.; Bakare, A.A. Perceived public health effects of occupational and residential exposure to electronic waste in Lagos, Nigeria. Zoologist 2015, 13, 62–71, ISSN 1596 972X. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | All (n = 178) | E-Waste Workers (n = 84) | Bystanders (n = 94) | p-Value (Chi-Square) | |
|---|---|---|---|---|---|
| Age (years) | mean | 28 | 27 | 28 | ns |
| Sex | male | 149 (83.7) | 82 (97.6) | 67 (71.3) | <0.05 |
| Marital status n (%) | Divorced | 5 (2.8) | 3 (3.6) | 2 (2.1) | ns |
| Married | 93 (52.3) | 44 (52.4) | 49 (52.1) | ||
| Single | 80 (44.9) | 37 (44.1) | 43 (45.7) | ||
| Education n (%) | n = 177 | n = 84 | n = 93 | <0.05 | |
| None | 62 (35.0) | 22 (26.2) | 40 (43.0) | ||
| Primary | 38 (21.5) | 20 (23.8) | 18 (19.4) | ||
| Junior High | 47 (26.6) | 30 (35.7) | 17 (18.3) | ||
| Senior High | 26 (14.7) | 11 (13.1) | 15 (16.1) | ||
| Tertiary | 4 (2.3) | 1 (1.2) | 3 (3.2) | ||
| Origin n (%) | Ghana | 140 (78.7) | 84 (100.0) | 56 (59.6) | <0.05 |
| Other countries | 38 (21.4) | 0 (0.0) | 38 (40.4) | ||
| Health Characteristics | All (n = 178, n (%)) | EW (n = 84, n (%)) | BY (n = 94, n (%)) | p-Value (Chi-Square) | |
|---|---|---|---|---|---|
| Smoking | 46 (25.8) | 19 (22.6) | 27 (28.7) | ns | |
| Drug use | 27 (15.2) | 21 (25.0) | 6 (6.4) | <0.05 | |
| Medication | 100 (57.5) n = 174 | 46 (57.5) n = 80 | 54 (57.5) n = 94 | ns | |
| pain | 80 (79.2) | 34 (73.9) | 46 (83.6) | ns | |
| Access to medical care via | Hospital | 76 (44.4) n = 171 | 34 (42.5) n = 80 | 42 (46.2) n = 91 | |
| Pharmacy | 132 (77.2) | 66 (82.5) | 66 (72.5) | ||
| Traditional Healer | 62 (36.3) | 37 (46.3) | 25 (27.5) | ||
| National health insurance | 56 (35.0) n = 160 | 25 (33.8) n = 74 | 31 (36.1) n = 86 | ns | |
| Use of PPE (only e-waste workers) | 21 (25.3) n = 83 | ||||
| safety glasses | 2 (9.5) | ||||
| safety boots | 12 (57.1) | ||||
| dust masks | 2 (9.5) | ||||
| helmet | 2 (9.5) |
| Symptoms and Diseases | All n = 178 n (%) | EW n = 84 n (%) | BY n = 94 n (%) | p-Value (Chi-Square) | |
|---|---|---|---|---|---|
| Infections | 10 (5.6) | 4 (4.8) | 6 (6.4) | ns | |
| Tuberculosis | 7 (3.9) | 2 (2.4) | 5 (5.3) | ||
| Malaria last 12 months | 134 (77.0) n = 174 | 66 (79.5) n = 83 | 68 (74.7) n = 91 | ns | |
| Diabetes | 2 (1.1) | 1 (1.2) | 1 (1.1) | ns | |
| Digestive problems | 112 (62.9) | 57 (67.9) | 55 (58.5) | ns | |
| Hypertension | 28 (15.8) n = 177 | 15 (17.9) n = 84 | 13 (14.0) n = 93 | ns | |
| Other cardiac symptoms | 52 (29.6) n = 176 | 22 (26.5) n = 83 | 30 (32.3) n = 93 | ns | |
| Palpitations | 28 (15.9) | 16 (19.3) | 12 (12.9) | ||
| Chest pain | 21 (11.9) | 5 (6.0) | 15 (16.1) | ||
| Cough | 113 (64.2) n = 176 | 53 (63.9) n = 83 | 60 (64.5) n = 93 | ns | |
| Mental disorders | Symptoms of anxiety | 68 (38.4) n = 177 | 38 (45.2) n = 84 | 30 (32.3) n = 93 | ns |
| Symptoms of depression | 61 (34.5) | 30 (35.7) | 31 (33.3) | ns | |
| Symptoms of posttraumatic stress disorder | 83 (46.9) | 44 (52.4) | 39 (41.9) | ns | |
| Skin symptoms | 65 (36.7) n = 177 | 36 (43.4) n = 83 | 29 (30.9) n = 94 | ns | |
| itching | 55 (31.1) | 33 (39.8) | 22 (23.4) | ||
| light sensitivity | 6 (3.4) | 1 (1.2) | 5 (5.3) | ||
| pain | 13 (7.4) | 3 (3.6) | 10 (10.6) | ||
| caused by work 1 | 21 (32.3) | 15 (41.7) | 6 (20.7) | ||
| Shortness of breath | 49 (27.8) n = 176 | 25 (30.1) n = 83 | 24 (25.8) n = 93 | ns | |
| caused by work 1 | 24 (49.0) | 12 (48.0) | 12 (50.0) | ||
| Red itchy eyes | 105 (59.3) n = 177 | 57 (67.9) n = 84 | 48 (51.6) n = 93 | <0.05 | |
| Eye injuries | 42 (23.7) n = 177 | 24 (28.6) n = 84 | 18 (19.4) n = 93 | ns | |
| Hearing loss | 28 (15.8) n = 177 | 14 (16.7) n = 84 | 14 (15.1) n = 93 | ns | |
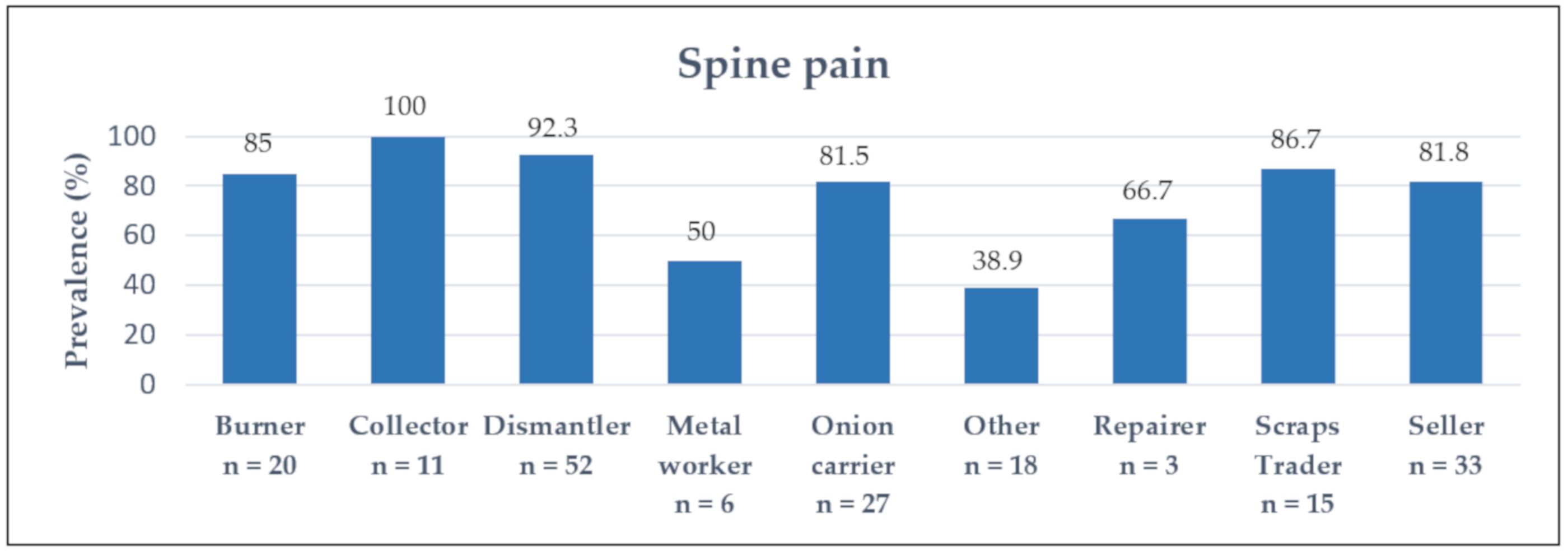
| Back pain | 150 (85.2) n = 176 | 76 (91.6) n = 83 | 74 (79.6) n = 93 | <0.05 | |
| neck | 77 (43.8) | 37 (44.6) | 40 (43.0) | ||
| back | 138 (78.4) | 73 (88.0) | 65 (69.9) | ||
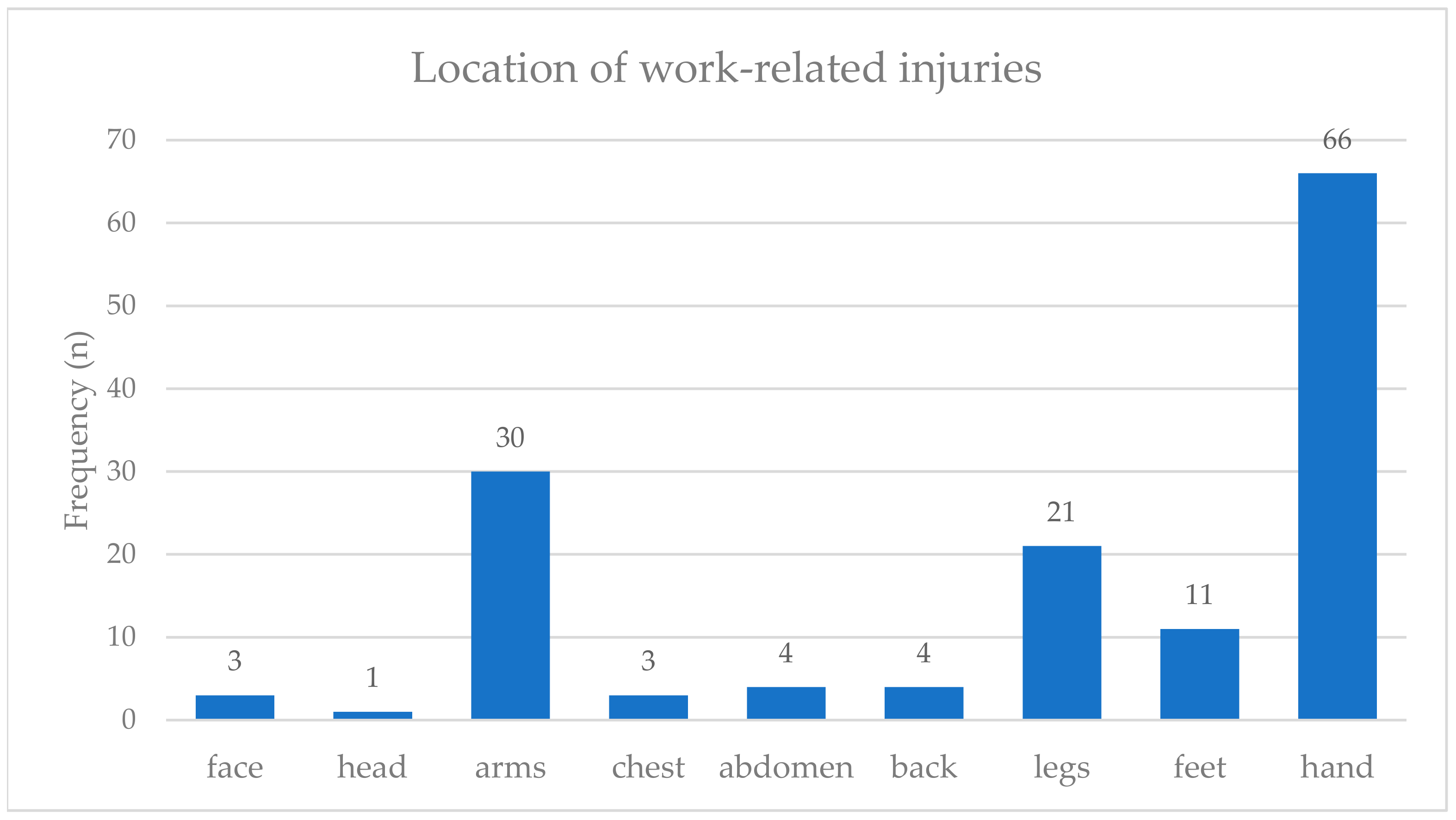
| Work-related injuries | 103 (57.9) | 63 (75.0) | 40 (42.6) | <0.05 | |
| cuts | 95 (53.4) | 60 (71.4) | 35 (37.2) | ||
| burns | 35 (19.7) | 23 (27.4) | 12 (12.8) |
| Occupational Exposure | Sum n (%) | p-Value (Chi-Square) | ||
|---|---|---|---|---|
| Yes n (%) | No n (%) | |||
| Dermal contact to chemicals or metals | ||||
| Skin symptoms | 44 (43.1) | 20 (27.0) | 64 (36.0) | <0.05 |
| Hard physical work | ||||
| Back pain | 136 (85.0) | 14 (87.5) | 150 (84.3) | ns |
| Numbness | 67 (49.2) | 5 (35.7) | 72 (40.4) | ns |
| Volume exposure | ||||
| Hearing loss | 22 (15.6) | 6 (16.7) | 28 (15.7) | ns |
| Inhalation of smoke | ||||
| Shortness of breath | 45 (28.5) | 4 (23.5) | 49 (27.5) | ns |
| Drug Use | ||||
| Yes (%) | No (%) | |||
| Work-related injuries | 21 (77.8) | 82 (54.3) | 103 (57.9) | <0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fischer, D.; Seidu, F.; Yang, J.; Felten, M.K.; Garus, C.; Kraus, T.; Fobil, J.N.; Kaifie, A. Health Consequences for E-Waste Workers and Bystanders—A Comparative Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 1534. https://doi.org/10.3390/ijerph17051534
Fischer D, Seidu F, Yang J, Felten MK, Garus C, Kraus T, Fobil JN, Kaifie A. Health Consequences for E-Waste Workers and Bystanders—A Comparative Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(5):1534. https://doi.org/10.3390/ijerph17051534
Chicago/Turabian StyleFischer, Damian, Fatima Seidu, Jennie Yang, Michael K. Felten, Cyryl Garus, Thomas Kraus, Julius N. Fobil, and Andrea Kaifie. 2020. "Health Consequences for E-Waste Workers and Bystanders—A Comparative Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 5: 1534. https://doi.org/10.3390/ijerph17051534
APA StyleFischer, D., Seidu, F., Yang, J., Felten, M. K., Garus, C., Kraus, T., Fobil, J. N., & Kaifie, A. (2020). Health Consequences for E-Waste Workers and Bystanders—A Comparative Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(5), 1534. https://doi.org/10.3390/ijerph17051534