Cluster Analysis of Health-Related Lifestyles in University Students

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample and Procedure
2.3. Measures
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. General Characteristics of Participants
3.2. Health-Related Lifestyles of Participants
3.3. Relationships of Mediterranean Diet and Physical Activity
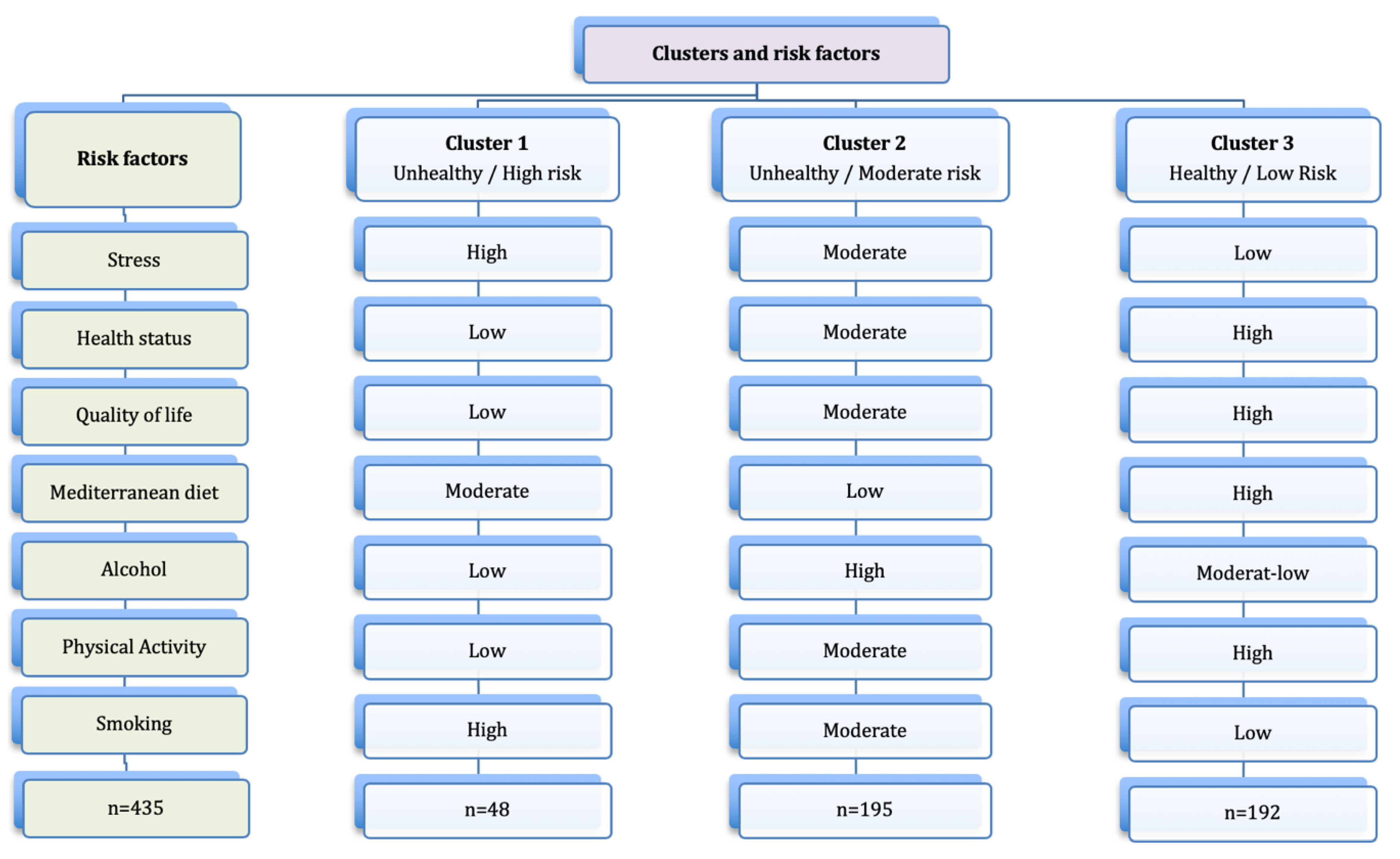
3.4. Cluster Analysis of Health-Related Lifestyles
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Joseph, P.; Leong, D.; McKee, M.; Anand, S.S.; Schwalm, J.-D.; Teo, K.; Mente, A.; Yusuf, S. Reducing the Global Burden of Cardiovascular Disease, Part 1. Circ. Res. 2017, 121, 677–694. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Daviglus, M.L.; Loria, C.M.; Colangelo, L.A.; Spring, B.; Moller, A.; Lloyd-Jones, D.M. Healthy lifestyle through young adulthood and the presence of low cardiovascular disease risk profile in middle age: The Coronary Artery Risk Development in (Young) Adults (CARDIA) study. Circulation 2012, 125, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Non-Communicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Hultgren, B.A.; Turrisi, R.; Cleveland, M.J.; Mallett, K.A.; Reavy, R.; Larimer, M.E.; Geisner, I.M.; Hospital, M. Transitions in drinking behaviors across the college years: A latent transition analysis. Addict. Behav. 2019, 92, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Deasy, C.; Coughlan, B.; Pironom, J.; Jourdan, D.; Mannix-McNamara, P. Psychological Distress and Coping amongst Higher Education Students: A Mixed Method Enquiry. PLoS ONE 2014, 9, e115193. [Google Scholar] [CrossRef]
- Deforche, B.; Van Dyck, D.; Deliens, T.; De Bourdeaudhuij, I. Changes in weight, physical activity, sedentary behaviour and dietary intake during the transition to higher education: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 16. [Google Scholar] [CrossRef]
- Dodd, L.J.; Al-Nakeeb, Y.; Nevill, A.M.; Forshaw, M.J. Lifestyle risk factors of students: A cluster analytical approach. Prev. Med. 2010, 51, 73–77. [Google Scholar] [CrossRef]
- Assaf, I.; Brieteh, F.; Tfaily, M.; El-Baida, M.; Kadry, S.; Balusamy, B. Students university healthy lifestyle practice: Quantitative analysis. Heal. Inf. Sci. Syst. 2019, 7, 7. [Google Scholar] [CrossRef]
- Moor, I.; Spallek, J.; Richter, M. Explaining socioeconomic inequalities in self-rated health: A systematic review of the relative contribution of material, psychosocial and behavioural factors. J. Epidemiology Community Heal. 2016, 71, 565–575. [Google Scholar] [CrossRef]
- Campos-Matos, I.; Russo, G.; Perelman, J. Connecting the dots on health inequalities--a systematic review on the social determinants of health in Portugal. Int. J. Equity Heal. 2016, 15, 26. [Google Scholar] [CrossRef]
- Arsandaux, J.; Michel, G.; Tournier, M.; Tzourio, C.; Galéra, C. Is self-esteem associated with self-rated health among French college students? A longitudinal epidemiological study: The i-Share cohort. BMJ Open 2019, 9, e024500. [Google Scholar] [CrossRef]
- Schmidt, M. Predictors of Self-rated Health and Lifestyle Behaviours in Swedish University Students. Glob. J. Heal. Sci. 2012, 4, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Pietz, K.; Petersen, L.A. Comparing Self-Reported Health Status and Diagnosis-Based Risk Adjustment to Predict 1- and 2 to 5-Year Mortality. Heal. Serv. Res. 2007, 42, 629–643. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Ciecierski, C.C.; Malin, E.L.; Carroll, A.J.; Gidea, M.; Craft, L.L.; Spring, B.; Hitsman, B. A latent class analysis of cancer risk behaviors among U.S. college students. Prev. Med. 2014, 64, 121–125. [Google Scholar] [CrossRef] [PubMed]
- El Ansari, W.; Ssewanyana, D.; Stock, C. Behavioral Health Risk Profiles of Undergraduate University Students in England, Wales, and Northern Ireland: A Cluster Analysis. Front. Public Heal. 2018, 6, 120. [Google Scholar] [CrossRef] [PubMed]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Heal. 2016, 16, 657. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.J.; MacDonncha, C.; Murphy, M.; Murphy, N.; Timperio, A.; Leech, R.; Woods, C. Identification of health-related behavioural clusters and their association with demographic characteristics in Irish university students. BMC Public Heal. 2019, 19, 121. [Google Scholar] [CrossRef]
- Lawrence, E.M.; Mollborn, S.; Hummer, R.A. Health lifestyles across the transition to adulthood: Implications for health. Soc. Sci. Med. 2017, 193, 23–32. [Google Scholar] [CrossRef]
- Luo, J.; Agley, J.; Hendryx, M.; Gassman, R.; Lohrmann, D. Risk patterns among college youth: Identification and implications for prevention and treatment. Health Promot. Pract. 2015, 16, 132–141. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Encuesta Nacional de Salud de España; Ministerio de Sanidad: Madrid, Spain, 2016.
- Craig, C.L.; Marshall, A.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. New Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. New Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and managing the global epidemic; Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Lundberg, O.; Manderbacka, K. Assessing reliability of a measure of self-rated health. Scand. J. Soc. Med. 1996, 24, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Manor, O.; Matthews, S.; Power, C. Self-rated health and limiting longstanding illness: Inter-relationships with morbidity in early adulthood. Int. J. Epidemiol. 2001, 30, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Salvany, A.; Bacigalupe, A.; Carrasco, J.M.; Espelt, A.; Ferrando, J.; Borrell, C.; del Grupo de Determinantes Sociales de Sociedad Espanola de Epidemiología. [Proposals for social class classification based on the Spanish National Classification of Occupations 2011 using neo-Weberian and neo-Marxist approaches]. Gac. Sanit. 2013, 27, 263–272. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-De-Mesquita, B.; Ocke, M.C.; Peeters, P.H.; Van Der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef]
- Eekhout, I.; de Boer, R.M.; Twisk, J.W.; de Vet, H.C.; Heymans, M.W. Missing data: A systematic review of how they are reported and handled. Epidemiology 2012, 23, 729–732. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regresion; John Willey and Sons: New York, NY, USA, 2000. [Google Scholar]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5nd ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Aceijas, C.; Waldhäusl, S.; Lambert, N.; Cassar, S.; Bello-Corassa, R. Determinants of health-related lifestyles among university students. Perspect. Public Heal. 2016, 137, 227–236. [Google Scholar] [CrossRef]
- Keller, S.; Maddock, J.E.; Hannöver, W.; Thyrian, J.R.; Basler, H.-D. Multiple health risk behaviors in German first year university students. Prev. Med. 2008, 46, 189–195. [Google Scholar] [CrossRef]
- Moreno-Gómez, C.; Romaguera, D.; Tauler-Riera, P.; Bennasar-Veny, M.; Pericas-Beltrán, J.; Martinez-Andreu, S.; Aguilo-Pons, A. Clustering of lifestyle factors in Spanish university students: The relationship between smoking, alcohol consumption, physical activity and diet quality. Public Heal. Nutr. 2012, 15, 2131–2139. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Tauler, P.; Bennasar, M.; Pericàs, J.; Moreno, C.; Martínez, S.; Aguiló, A.; Bennasar-Veny, M. Determinants and patterns of physical activity practice among Spanish university students. J. Sports Sci. 2011, 29, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Nikolaidis, P.; Martins, F.M.L.; Mendes, R. Physical Activity Patterns in University Students: Do They Follow the Public Health Guidelines? PLoS ONE 2016, 11, e0152516. [Google Scholar] [CrossRef] [PubMed]
- Hadjimbei, E.; Botsaris, G.; Gekas, V.; Panayiotou, A.G. Adherence to the Mediterranean Diet and Lifestyle Characteristics of University Students in Cyprus: A Cross-Sectional Survey. J. Nutr. Metab. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Franco, A.J.-M.; Agustín, A.B.S.; Marqueta, A.; Valero, P.G.; De La Puerta, I.N. [Addictive substance use among first-year university students]. Adicciones 2009, 21, 21–28. [Google Scholar]
- Foxcroft, D.; Moreira, M.T.; Santimano, N.M.; Smith, L.A. Social norms information for alcohol misuse in university and college students. Cochrane Database Syst. Rev. 2015, CD006748. [Google Scholar]
- Tarrant, M.; Smith, J.; Ball, S.; Winlove, C.; Gul, S.; Charles, N. Alcohol consumption among university students in the night-time economy in the UK: A three-wave longitudinal study. Drug Alcohol Depend. 2019, 204, 107522. [Google Scholar] [CrossRef]
- Cabrera, S.G.; Fernández, N.H.; Hernández, C.R.; Nissensohn, M.; Roman-Viñas, B.; Serra-Majem, L. Kidmed test, prevalence of low adherence to the mediterranean diet in children and young: A systematic review. Nutr. Hosp. 2015, 32, 2390–2399. [Google Scholar]
- García-Meseguer, M.J.; Burriel, F.C.; García-Meseguer, M.J.; Serrano-Urrea, R. Adherence to Mediterranean diet in a Spanish university population. Appetite 2014, 78, 156–164. [Google Scholar] [CrossRef] [PubMed]
- De-Mateo-Silleras, B.; Camina-Martín, M.A.; Cartujo-Redondo, A.; Carreño-Enciso, L.; De La Cruz, S.; Redondo-Del-Río, M.P. Health Perception According to the Lifestyle of University Students. J. Community Heal. 2018, 44, 74–80. [Google Scholar] [CrossRef]
- Sprake, E.F.; Russell, J.M.; Cecil, J.E.; Cooper, R.J.; Grabowski, P.; Pourshahidi, K.; Barker, M. Dietary patterns of university students in the UK: A cross-sectional study. Nutr. J. 2018, 17, 90. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.-P.; Pestoni, G.; Cabaset, S.; Brombach, C.; Sych, J.M.; Schader, C.; Faeh, D.; Rohrmann, S. Dietary Patterns and Their Sociodemographic and Lifestyle Determinants in Switzerland: Results from the National Nutrition Survey menuCH. Nutrients 2018, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Arabshahi, S.; Lahmann, P.H.; Williams, G.; Marks, G.C.; Van Der Pols, J. Longitudinal Change in Diet Quality in Australian Adults Varies by Demographic, Socio-Economic, and Lifestyle Characteristics. J. Nutr. 2011, 141, 1871–1879. [Google Scholar] [CrossRef] [PubMed]
- Dowler, E. Inequalities in diet and physical activity in Europe. Public Heal. Nutr. 2001, 4, 701–709. [Google Scholar] [CrossRef]
- Noble, N.; Paul, C.; Turon, H.; Oldmeadow, C. Which modifiable health risk behaviours are related? A systematic review of the clustering of Smoking, Nutrition, Alcohol and Physical activity (‘SNAP’) health risk factors. Prev. Med. 2015, 81, 16–41. [Google Scholar] [CrossRef] [PubMed]
- Chacón-Cuberos, R.; Zurita-Ortega, F.; Olmedo, E.; Castro-Sánchez, M. Relationship between Academic Stress, Physical Activity and Diet in University Students of Education. Behav. Sci. 2019, 9, 59. [Google Scholar] [CrossRef]
- Havigerova, J.M.; Dosedlova, J.; Buresova, I. One health behavior or many health-related behaviors? Psychol. Res. Behav. Manag. 2019, 12, 23–30. [Google Scholar] [CrossRef]
- Mawditt, C.; Sacker, A.; Britton, A.; Kelly, Y.J.; Cable, N. Social influences on health-related behaviour clustering during adulthood in two British birth cohort studies. Prev. Med. 2018, 110, 67–80. [Google Scholar] [CrossRef]
- Galán, I.; Rodríguez-Artalejo, F.; Zorrilla, B. [Telephone versus face-to-face household interviews in the assessment of health behaviors and preventive practices]. Gac. Sanit. 2004, 18, 440–450. [Google Scholar] [CrossRef]
- Bes-Rastrollo, M.; Pérez Valdivieso, J.R.; Sánchez-Villegas, A.; Alonso, A.; Martínez González, M. Validación del peso e índice de masa corporal auto-declarados de los participantes en una cohorte de graduados universitarios. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Pedisic, Z.; Rakovac, M.; Titze, S.; Jurakić, D.; Oja, P. Domain-specific physical activity and health-related quality of life in university students. Eur. J. Sport Sci. 2013, 14, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Wanden-Berghe, C.; Martín-Rodero, H.; Rodríguez-Martín, A.; Ruiz, J.P.N.; De Victoria, E.M.; Sanz-Valero, J.; González Ángela, G.; Vila, A.; Alonso, M.V.; Marí, J.A.T.; et al. [Quality of life and its determinants in Spanish university students of health sciences factors]. Nutr. Hosp. 2014, 31, 952–958. [Google Scholar] [PubMed]
- Martinez-Riera, J.R.; Gallardo Pino, C.; Aguilo Pons, A.; Granados Mendoza, M.C.; Lopez-Gomez, J.; Arroyo Acevedo, H.V. [The university as a community: Health-promoting universities. SESPAS Report 2018]. Gac. Sanit. 2018, 32, 86–91. [Google Scholar] [PubMed]
- Whatnall, M.C.; Patterson, A.J.; Chiu, S.; Oldmeadow, C.; Hutchesson, M.J. Feasibility and Preliminary Efficacy of the Eating Advice to Students (EATS) Brief Web-Based Nutrition Intervention for Young Adult University Students: A Pilot Randomized Controlled Trial. Nutrients 2019, 11, 905. [Google Scholar] [CrossRef] [PubMed]
- Plotnikoff, R.C.; Costigan, S.; Haslam, R.; Hutchesson, M.J.; Kennedy, S.; Robards, S.L.; Allen, J.; Collins, C.E.; Callister, R.; Germov, J. Effectiveness of interventions targeting physical activity, nutrition and healthy weight for university and college students: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 45. [Google Scholar] [CrossRef]
- Deasy, C.; Coughlan, B.; Pironom, J.; Jourdan, D.; Mannix-McNamara, P. Psychological distress and lifestyle of students: Implications for health promotion. Heal. Promot. Int. 2014, 30, 77–87. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All (n = 444) | Men (n = 143) | Women (n = 301) | p-Value | |
|---|---|---|---|---|
| Mean (SD) or n (%) | ||||
| Age, years | 23.1 (5.7) | 23.0 (5.5) | 23.0 (5.7) | 0.681 |
| Weight, kg | 64.2 (12.9) | 75.8 (11.5) | 58.7 (9.4) | <0.001 |
| Height, cm | 168.5 (8.7) | 177.5 (6.6) | 154.1 (5.8) | <0.001 |
| BMI, kg/m2 | 22.5 (3.5) | 24.0 (3.5) | 21.8 (3.2) | <0.001 |
| BMI classification * | <0.001 | |||
| Underweight | 34 (7.7%) | 1 (0.7%) | 33 (11.0%) | |
| Normal weight | 326 (73.4%) | 101 (70.6%) | 225 (74.7%) | |
| Overweight | 68 (15.3%) | 35 (24.5%) | 33 (11.0%) | |
| Obese | 16 (3.6%) | 6 (4.2%) | 10 (3.3%) | |
| Social class | 0.044 | |||
| High | 105 (23.7%) | 44 (30.8%) | 61 (20.3%) | |
| Medium | 271 (61.0%) | 79 (55.2%) | 192 (63.8%) | |
| Low | 68 (15.3%) | 20 (14.0%) | 48 (15.9%) | |
| Working | ||||
| Yes | 130 (29.4%) | 101 (29.4%) | 211 (29.4%) | 0.990 |
| All (n = 444) | Men (n = 143) | Women (n = 301) | p-Value | |
|---|---|---|---|---|
| Mean (SD) or n (%) | ||||
| Stress High or very high | 225 (50.6%) | 56 (39.2%) | 169 (56.7%) | <0.001 |
| Health status Good or very good | 401 (91.0%) | 130 (91.6%) | 271 (90.7%) | 0.061 |
| Quality of life Good or very good | 394 (88.9%) | 129 (90.2%) | 265 (88.4%) | 0.711 |
| Diet | ||||
| Meals/day | 2.7 (0.9) | 2.5 (1.0) | 2.7 (0.9) | 0.024 |
| Breakfast every day | 279 (63.1%) | 89 (62.2%) | 190 (63.5%) | 0.790 |
| Diet quality | ||||
| PREDIMED score | 5.4 (1.8) | 4.8 (1.8) | 5.6 (1.8) | <0.001 |
| MDS | 5.3 (1.8) | 4.8 (1.9) | 5.5 (1.7) | <0.001 |
| Physical activity | ||||
| Yes | 294 (66.2%) | 103 (72.0%) | 191 (63.5%) | <0.001 |
| Mets-min/week | 1867.7 (2798.5) | 2835.0 (3991.4) | 1408.2 (1834.6) | <0.001 |
| Minutes/week | 186.6 (89.1) | 210.0 (99.4) | 174.3 (80.9) | 0.009 |
| Parent’s physical activity | 0.311 | |||
| Yes, both | 79 (19.7%) | 28 (20.9%) | 51 (19.0%) | |
| Yes, mother only | 49 (12.2%) | 15 (11.2%) | 34 (12.7%) | |
| Yes, father only | 63 (15.7%) | 15 (11.2%) | 48 (17.9%) | |
| Smoking | ||||
| Yes | 86 (19.5%) | 22 (15.5%) | 64 (21.3%) | 0.148 |
| Cigarettes/day | 7.1 (7.0) | 8.4 (9.2) | 6.6 (6.1) | |
| Alcohol consumption | ||||
| Yes | 41.2 (59.6%) | 56.2 (73.8%) | 34.1 (50.0%) | <0.001 |
| g ethanol /week | 41.2 (59.6) | 56.2 (73.8) | 34.1 (50.0) | <0.001 |
| Drug consumption | ||||
| Yes | 65 (14.6%) | 18 (12.6%) | 47 (15.6%) | 0.399 |
| Sedentary habits | ||||
| Study (h/day) | 3.5 (2.3) | 3.3 (3.4) | 3.6 (2.4) | 0.047 |
| Computer (h/day) | 3.6 (2.5) | 3.8 (2.6) | 3.6 (2.4) | 0.694 |
| Physical Activity | Yes (n = 294) | No (n = 150) | OR | 95% CI | aOR | 95% CI |
|---|---|---|---|---|---|---|
| n (%) or Mean (SD) | ||||||
| Gender | ||||||
| Male | 105 (35.7%) | 38 (25.7%) | 1 | 1 | ||
| Female | 191 (65.0%) | 110 (73.3%) | 0.62 * | 0.40–0.96 | 0.49 * | 0.29–0.85 |
| Age (years) | 22.9 (5.6) | 23.3 (5.7) | 0.99 | 0.96–1.02 | 0.99 | 0.95–1.04 |
| BMI (kg/m2) | 22.6 (3.1) | 22.4 (4.2) | 1.01 | 0.96–1.07 | 1.02 | 0.95–1.09 |
| Social class | ||||||
| High | 72 (24.5%) | 35 (23.3%) | 1 | |||
| Medium | 83 (28.2%) | 43 (28.7%) | 1.07 | 0.65–1.77 | ||
| Low | 139 (47.3%) | 72 (48.0%) | 1.01 | 0.63–1.62 | ||
| Mediterranean Diet Score | 5.5 (1.8) | 5.0 (1.7) | 1.13 * | 1.01–1.26 | 1.16 * | 1.02–1.32 |
| Parent’s physical activity | ||||||
| No | 143 (48.6%) | 89 (59.3%) | 1 | 1 | ||
| Yes, both | 69 (23.5%) | 19 (12.7%) | 2.24 ** | 1.24–4.06 | 1.82 | 0.96–3.47 |
| Yes, mother only | 39 (13.3%) | 16 (10.7%) | 1.50 | 0.77–2.92 | 1.78 | 0.83–3.82 |
| Yes, father only | 43 (14.6%) | 26 (17.3%) | 1.00 | 0.57–1.79 | 0.84 | 0.45–1.55 |
| Computer use (h/day) | 3.1 (2.1) | 3.8 (2.2) | 0.87 *** | 0.80–0.96 | 0.85 ** | 0.76–0.95 |
| Studying (h/day) | 3.3 (2.0) | 3.7 (2.0) | 0.89 * | 0.81–0.98 | 0.92 | 0.81–1.04 |
| Tobacco consumption | ||||||
| No | 236 (80.3%) | (80.8%) | 1 | |||
| Yes | 58 (19.7%) | (19.2%) | 1.02 | 0.62–1.69 | ||
| Alcohol consumption | ||||||
| No | 39 (13.3%) | 29 (19.3%) | 1 | |||
| Yes | 255 (86.7%) | 121 (80.7%) | 1.54 | 0.91–2.61 | ||
| Drug consumption | ||||||
| No | 243 (82.7%) | 121 (80.7%) | 1 | |||
| Yes | 51 (17.3%) | 29 (19.3%) | 0.90 | 0.54–1.49 | ||
| Mediterranean Diet Score (MDS) | Low Adherence(MDS < 5)(n = 229) | High Adherence(MDS ≥ 5)(n = 202) | OR | 95% CI | aOR | 95% CI |
|---|---|---|---|---|---|---|
| n (%) or Mean (SD) | ||||||
| Sex | ||||||
| Male | 104 (45.4%) | 54 (26.7%) | 1 | 1 | ||
| Female | 125 (54.6%) | 148 (73.3%) | 2.26 *** | 1.47–3.47 | 2.98 *** | 1.80–4.93 |
| Age (years) | 21.9 (4.4) | 23.4 (5.9) | 1.06 * | 1.01–1.11 | 1.08 ** | 1.02–1.14 |
| BMI (kg/m2) | 22.4 (3.8) | 22.6 (3.4) | 1.02 | 0.96–1.08 | 1.05 | 0.98–1.13 |
| Social class | ||||||
| High social class | 51 (22.3%) | 51 (25.2%) | 1 | |||
| Medium social class | 73 (31.9%) | 53 (26.2%) | 0.71 | 0.40–1.27 | ||
| Low social class | 105 (45.8%) | 98 (48.6%) | 0.93 | 0.54–1.58 | ||
| Physical activity † | ||||||
| No | 95 (41.5%) | 62 (30.7%) | 1 | 1 | ||
| Yes | 134 (58.5%) | 140 (69.3%) | 1.61 * | 1.05–2.47 | 1.75 * | 1.09–2.80 |
| Breakfast every day | ||||||
| No | 114 (49.8%) | 62 (30.7%) | 1 | 1 | ||
| Yes | 115 (50.2%) | 140 (69.3%) | 2.24 *** | 1.46–3.42 | 1.70 * | 1.05–2.76 |
| Meals/day | 2.4 (0.9) | 2.8 (0.9) | 1.61 *** | 1.27–2.05 | 1.43 ** | 1.10–1.87 |
| Tobacco consumption | ||||||
| No | 173 (75.5%) | 168 (83.2%) | 1 | 1 | ||
| Yes | 56 (24.5%) | 34 (16.8%) | 0.61 | 0.37–1.01 | 0.52* | 0.30–0.91 |
| Alcohol consumption | ||||||
| No | 32 (14.0%) | 31 (15.4%) | 1 | |||
| Yes | 197 (86.0%) | 171 (84.6%) | 0.89 | 0.49–1.60 | ||
| Drugs consumption | ||||||
| No | 185 (80.8%) | 168 (83.2%) | 1 | |||
| Yes | 44 (19.2%) | 34 (16.8%) | 0.86 | 0.50–1.46 | ||
| Cluster 1 (n = 195, 44.83%) Unhealthy, High Risk | Cluster 2 (n = 48, 11.03%) Unhealthy, Moderate Risk | Cluster 3 (n = 192, 44.14%) Healthy, Low Risk | |
|---|---|---|---|
| Health-Related Behaviors | n(%) or Mean (SD) | ||
| Stress ** | 4.14 (0.76) | 3.58 (1.07) | 2.78 (0.89) |
| Health status ** | 1.18 (0.53) | 0.83 (0.43) | 0.47 (0.52) |
| Quality of life ** | 1.20 (0.58) | 0.98 (0.53) | 0.60 (0.51) |
| Mediterranean diet | 5.34 (1.74) | 4.82 (1.56) | 5.42 (1.83) |
| Physical activity ** | 1071 (1519) | 2086 (2549) | 2473 (2547) |
| Smoking ** | 37 (19.0%) | 32 (66.7%) | 15 (7.9%) |
| Alcohol consumption** | 30.05 (2.15) | 109.66 (15.83) | 35.23 (2.54) |
| Sociodemographic factors | |||
| Age ** | 23.4 (5.7) | 26.6 (7.8) | 21.9 (4.4) |
| Gender * | |||
| Female | 148 (75.9%) | 29 (60.4%) | 117 (60.9%) |
| Male | 47 (24.1%) | 19 (39.6%) | 75 (39.1%) |
| BMI * | |||
| Normal weight | 150 (77.7%) | 36 (75.0%) | 166 (87.4%) |
| Obesity or overweight | 43 (22.3%) | 12 (25.0%) | 24 (12.6%) |
| Social class | |||
| Blue collar | 96 (50.8%) | 26 (56.5%) | 80 (43.0%) |
| White collar | 93 (49.2%) | 20 (43.5%) | 106 (57.0%) |
| Residence ** | |||
| Parents | 130 (66.7%) | 20 (42.6%) | 146 (76.0%) |
| Others | 65 (33.3%) | 27 (57.4%) | 46 (24.0%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennasar-Veny, M.; Yañez, A.M.; Pericas, J.; Ballester, L.; Fernandez-Dominguez, J.C.; Tauler, P.; Aguilo, A. Cluster Analysis of Health-Related Lifestyles in University Students. Int. J. Environ. Res. Public Health 2020, 17, 1776. https://doi.org/10.3390/ijerph17051776
Bennasar-Veny M, Yañez AM, Pericas J, Ballester L, Fernandez-Dominguez JC, Tauler P, Aguilo A. Cluster Analysis of Health-Related Lifestyles in University Students. International Journal of Environmental Research and Public Health. 2020; 17(5):1776. https://doi.org/10.3390/ijerph17051776
Chicago/Turabian StyleBennasar-Veny, Miquel, Aina M. Yañez, Jordi Pericas, Lluis Ballester, Juan Carlos Fernandez-Dominguez, Pedro Tauler, and Antoni Aguilo. 2020. "Cluster Analysis of Health-Related Lifestyles in University Students" International Journal of Environmental Research and Public Health 17, no. 5: 1776. https://doi.org/10.3390/ijerph17051776
APA StyleBennasar-Veny, M., Yañez, A. M., Pericas, J., Ballester, L., Fernandez-Dominguez, J. C., Tauler, P., & Aguilo, A. (2020). Cluster Analysis of Health-Related Lifestyles in University Students. International Journal of Environmental Research and Public Health, 17(5), 1776. https://doi.org/10.3390/ijerph17051776