The Theory of Planned Behaviour in Medical Tourism: International Comparison in the Young Consumer Segment




Abstract
1. Introduction
2. Literature Review
2.1. Medical Tourism—Term and Research Gap
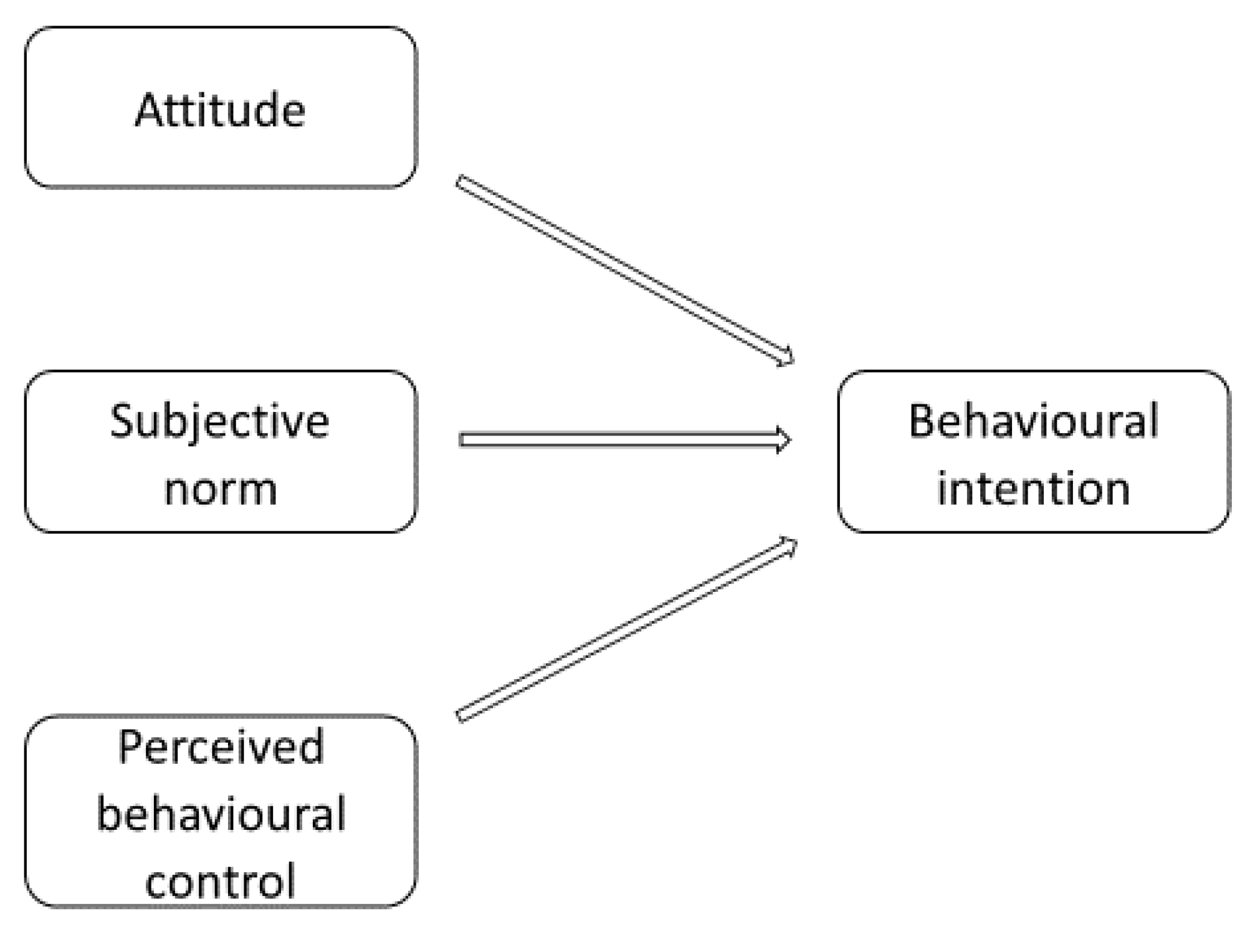
2.2. Theory of Planned Behaviour
2.3. Overview of Literature on TPB in Medical Tourism
3. Research Model and Hypotheses
4. Research Method
5. Data Analysis
6. Discussion
7. Conclusions
- there is a relationship between the intention to participate/consider participation in medical tourism and the three TPB factors (attitudes towards participation in medical tourism, subjective norms, and perceived behavioural control);
- the effect of the individual TPB factors on behavioural intentions as to medical tourism may vary among consumers from different countries.
Limitations and Future Studies
Author Contributions
Funding
Conflicts of Interest
References
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Sparks, B.; Pan, G.W. Chinese Outbound tourists: Understanding their attitudes, constraints and use of information sources. Tour. Manag. 2009, 30, 483–494. [Google Scholar] [CrossRef]
- Quintal, V.A.; Lee, J.A.; Soutar, G.N. Risk, uncertainty and the theory of planned behavior: A tourism example. Tour. Manag. 2010, 31, 797–805. [Google Scholar] [CrossRef]
- Lam, T.; Hsu, C.H.C. Predicting behavioral intention of choosing a travel destination. Tour. Manag. 2006, 27, 589–599. [Google Scholar] [CrossRef]
- Sparks, B. Planning a wine tourism vacation? Factors that help to predict tourist behavioural intentions. Tour. Manag. 2007, 28, 1180–1192. [Google Scholar] [CrossRef]
- Banberg, S.; Ajzen, I.; Schmidt, P. Choice of Travel Mode in the Theory of Planned Behaviour: The Roles of Past Behaviour, Habit, and Reasoned Action. Basic Appl. Sci. Psychol. 2003, 25, 175–188. [Google Scholar] [CrossRef]
- Kaplan, S.; Manca, F.; Nielsen, T.A.S.; Prato, C.G. Intentions to use bike-sharing for holiday cycling: An application of the Theory of Planned Behavior. Tour. Manag. 2015, 47, 34–46. [Google Scholar] [CrossRef]
- Doran, R.; Larsen, S. The Relative Importance of Social and Personal Norms in Explaining Intentions to Choose Eco-Friendly Travel Options. Int. J. Tour. Res. 2016, 18, 159–166. [Google Scholar] [CrossRef]
- Hu, H.; Zhang, J.; Wang, C.; Yu, P.; Chu, G. What influences tourists’ intention to participate in the Zero Litter Initiative in mountainous tourism areas: A case study of Huangshan National Park, China. Sci. Total Environ. 2019, 657, 1127–1137. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, J.; Cao, J.; Hu, H.; Yu, P. The influence of environmental background on tourists’ environmentally responsible behaviour. J. Environ. Manag. 2019, 231, 804–810. [Google Scholar] [CrossRef]
- Amaro, S.; Duarte, P. An integrative model of consumers’ intentions to purchase travel online. Tour. Manag. 2015, 46, 64–79. [Google Scholar] [CrossRef]
- Cheng, S.; Lam, T.; Hsu, C.H.C. Negative Word-of-Mouth Communication Intention: An Application of the Theory of Planned Behavior. J. Hosp. Tour. Res. 2006, 30, 95–116. [Google Scholar] [CrossRef]
- Francis, J.; Eccles, M.P.; Johnston, M.; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behaviour: A Manual for Health Services Researchers; Centre for Health Services Research, University of Newcastle upon Tyne This: Newcastle Upon Tyne, UK, 2004; ISBN 9781848211797. [Google Scholar]
- McEachan, R.R.C.; Conner, M.; Taylor, N.J.; Lawton, R.J. Prospective prediction of health-related behaviours with the theory of planned behaviour: A meta-analysis. Health Psychol. Rev. 2011, 5, 97–144. [Google Scholar] [CrossRef]
- Li, J.; Hsu, C.C.; Lin, C.T. Leisure participation behavior and psychological well-being of elderly adults: An empirical study of Tai Chi Chuan in China. Int. J. Environ. Res. Public Health 2019, 16, 3387. [Google Scholar] [CrossRef]
- Chan, K.; Tsang, L. Promote healthy eating among adolescents: A Hong Kong study. J. Consum. Mark. 2011, 28, 354–362. [Google Scholar] [CrossRef]
- Rezazadeh, A.; Solhi, M.; Azam, K. Determinants of responsibility for health, spiritual health and interpersonal relationship based on theory of planned behavior in high school girl students. Med. J. Islam. Repub. Iran 2015, 29, 204. [Google Scholar]
- Moshi, F.V.; Kibusi, S.M.; Fabian, F. The Effectiveness of Community-Based Continuous Training on Promoting Positive Behaviors towards Birth Preparedness, Male Involvement, and Maternal Services Utilization among Expecting Couples in Rukwa, Tanzania: A Theory of Planned Behavior Quasi-Experim. J. Environ. Public Health 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Amin, M.; Elyasi, M.; Bohlouli, B.; ElSalhy, M. Application of the theory of planned behavior to predict dental attendance and caries experience among children of newcomers. Int. J. Environ. Res. Public Health 2019, 16, 3661. [Google Scholar] [CrossRef]
- Mo, D.; Xiang, M.; Luo, M.; Dong, Y.; Fang, Y.; Zhang, S.; Zhang, Z.; Liang, H. Using gamification and social incentives to increase physical activity and related social cognition among undergraduate students in Shanghai, China. Int. J. Environ. Res. Public Health 2019, 16, 858. [Google Scholar] [CrossRef]
- Chau, P.Y.; Jen-Hwa Hu, P. Investigating Healthcare Professionals Decisions to Accept Telemedicine Technology. Inf. Manag. 2002, 39, 297–311. [Google Scholar] [CrossRef]
- Scheinfeld, E.; Crook, B.; Perry, C.L. Understanding Young Adults’ E-cigarette Use through the Theory of Planned Behavior. Health Behav. Policy Rev. 2019, 6, 115–127. [Google Scholar] [CrossRef]
- Bhochhibhoya, A.; Branscum, P. The Application of the Theory of Planned Behavior and the Integrative Behavioral Model towards Predicting and Understanding Alcohol-Related Behaviors: A Systematic Review. J. Alcohol Drug Educ. 2018, 62, 39–63. [Google Scholar]
- Bohon, L.M.; Cotter, K.A.; Kravitz, R.L.; Cello, P.C.; Fernandez y Garcia, E. The Theory of Planned Behavior as it predicts potential intention to seek mental health services for depression among college students. J. Am. Coll. Health 2016, 64, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.S.; Ramamonjiarivelo, Z.; Martin, W.S. MEDTOUR: A scale for measuring medical tourism intentions. Tour. Rev. 2011, 66, 45–56. [Google Scholar] [CrossRef]
- Lee, M.; Han, H.; Lockyer, T. Medical tourism—Attracting Japanese tourists for medical tourism experience. J. Travel Tour. Mark. 2012, 29, 69–86. [Google Scholar] [CrossRef]
- Park, J.K.; Ahn, J.; Yoo, W.S. The Effects of Price and Health Consciousness and Satisfaction on the Medical Tourism Experience. J. Healthc. Manag. 2017, 62, 405–417. [Google Scholar] [CrossRef]
- Seow, A.N.; Choong, Y.O.; Chan, L.M. Travel Intentions among Foreign Tourists for Medical Treatment in Malaysia: An Empirical Study. Procedia Soc. Behav. Sci. 2016, 224, 546–553. [Google Scholar]
- Seow, A.N.; Choong, Y.O.; Moorthy, K.; Chan, L.M. Intention to visit Malaysia for medical tourism using the antecedents of Theory of Planned Behaviour: A predictive model. Int. J. Tour. Res. 2017, 19, 383–393. [Google Scholar] [CrossRef]
- Suki, A.A.; Putit, L.; Yusof, J.M.; Khan, N.R.M. Assessing medical tourists’ destination choice behavior: A conceptual perspective. Theory Pract. Hosp. Tour. Res. 2014, 519–523. [Google Scholar]
- Suki, A.A.; Putit, L.; Rita, N.; Khan, M. Assessing Sharia Compliance Medical Destination Behaviour: A Medical Tourism Perspective. Pertanika J. Soc. Sci. Hum 2017, 25, 203–214. [Google Scholar]
- Reddy, S.G.; York, V.K.; Brannon, L.A. Travel for treatment: Students’ perspective on medical tourism. Int. J. Tour. Res. 2010, 12, 510–522. [Google Scholar] [CrossRef]
- Ramamonjiarivelo, Z.; Martin, D.S.; Martin, W.S. The Determinants of Medical Tourism Intentions: Applying the Theory of Planned Behavior. Health Mark. Q. 2015, 32, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Lautier, M. International trade of health services: Global trends and local impact. Health Policy (N. Y.) 2014, 118, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Guy, B.S.; Henson, J.L.N.; Dotson, M.J. Characteristics of consumers likely and unlikely to participate in medical tourism. Int. J. Healthc. Manag. 2015, 8, 68–76. [Google Scholar] [CrossRef]
- Lubowiecki-Vikuk, A.; Dryglas, D. Central and Eastern Europe as a Medical Tourism Destination: A Case Study of Poland. Almatourism J. Tour. Cult. Territ. Dev. 2019, 10, 25–43. [Google Scholar]
- Marczak, M.; Zarębski, P. Potencjał turystyczny uzdrowisk bałtyckich w Polsce [Tourist Potential in Poland Baltic Spas]. Zesz. Nauk. Uniw. Szczecińskiego Nr 784, Ekon. Probl. Tur. 2013, 23, 225–238. [Google Scholar]
- Stankiewicz, B. Makroekonomiczny model turystyki medycznej w Polsce—Podstawowe uwarunkowania badań. Pr. Nauk. Uniw. Ekon. Wrocławiu 2012, 245, 488–496. [Google Scholar]
- Carrera, P.M.; Bridges, J.F. Globalization and healthcare: Understanding health and medical tourism. Expert Rev. Pharm. Outcomes Res. 2006, 6, 447–454. [Google Scholar] [CrossRef]
- Rab-Przybyłowicz, J. Tworzenie produktu dla turystyki medycznej w Szczecinie. Zesz. Nauk. Uniw. Szczecińskiego. Ekon. Probl. Usług 2010, 591, 695–706. [Google Scholar]
- Rab-Przybyłowicz, J. Determinanty popytowe wpływające na rozwój turystyki medycznej [demand-side determinants of medical tourism development]. Zesz. Nauk. Uniw. Szczecińskiego Ekon. Probl. Usług 2012, 698, 208–221. [Google Scholar]
- Crooks, V.A.; Kingsbury, P.; Snyder, J.; Johnston, R. What is known about the patient’s experience of medical tourism? A scoping review. BMC Health Serv. Res. 2010, 10, 266. [Google Scholar] [CrossRef]
- Jagyasi, P. Defining medical tourism. Another approach. Med. Tour. Mag. 2008, 6, 9–11. [Google Scholar]
- Hopkins, L.; Labonté, R.; Runnels, V.; Packer, C. Medical tourism today: What is the state of existing knowledge. J. Public Health Policy 2010, 31, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Lubowicki-Vikuk, A.P. Turystyka medyczna przejawem współczesnych trendów i tendencji w turystyce [medical tourism as a form of manifestation of contemporary trends and tendencies in tourism]. Zesz. Nauk. Uniw. Szczecińskiego Ekon. Probl. Usług 2012, 699, 553–568. [Google Scholar]
- Cormany, D.; Baloglu, S. Medical travel facilitator websites: An exploratory study of web page contents and services offered to the prospective medical tourist. Tour. Manag. 2011, 32, 709–716. [Google Scholar] [CrossRef]
- Kim, S.; Arcodia, C.; Kim, I. Critical Success Factors of Medical Tourism: The Case of South Korea. Int. J. Environ. Res. Public Health 2019, 16, 4964. [Google Scholar] [CrossRef]
- Białk-Wolf, A. Turystyka Medyczna. Perspektywy rozwoju w woj. Pomorskim [Medical tourism. Development prospects in the Pomeranian Voivodeship]; Gdańska Organizacja Turystyczna: Gdańsk, Poland, 2014. [Google Scholar]
- Borzyszkowski, J. Organizacje Zarządzające Obszarami Recepcji Turystycznej. Istota, Funkcjonowanie, Kierunki Zmian [Destination Management Organizations. The Idea, Functioning, Changes]; Wydawnictwo Uczelniane Politechniki Koszalińskiej: Koszalin, Poland, 2015. [Google Scholar]
- Lunt, N.; Carrera, P. Medical tourism: Assessing the evidence on treatment abroad. Maturitas 2010, 66, 27–32. [Google Scholar] [CrossRef]
- Al-Amin, M.; Makarem, S.C.; Pradhan, R. Hospital ability to attract international patients: A conceptual framework. Int. J. Pharm. Healthc. Mark. 2011, 5, 205–221. [Google Scholar] [CrossRef]
- Lunt, N.; MacHin, L.; Green, S.; Mannion, R. Are there implications for quality of care for patients who participate in international medical tourism? Expert Rev. Pharm. Outcomes Res. 2011, 11, 133–136. [Google Scholar] [CrossRef][Green Version]
- Snyder, J.; Crooks, V.A.; Johnston, R.; Kingsbury, P. What do we know about Canadian involvement in medical tourism? A scoping review. Open Med. 2011, 5, 139–148. [Google Scholar]
- Klich, J. Global medical tourism management: A needed research agenda. Adv. Manag. 2012, 5, 5–7. [Google Scholar]
- Connell, J. Contemporary medical tourism: Conceptualisation, culture and commodification. Tour. Manag. 2013, 34, 1–13. [Google Scholar] [CrossRef]
- Menvielle, L.; Menvielle, W.; Tournois, N. Purchasing behavior of consumers for foreign medical services: An approach using the soft laddering method. Qual. Mark. Res. 2014, 17, 264–282. [Google Scholar] [CrossRef]
- Whittaker, A. Pleasure and pain: Medical travel in Asia. Glob. Public Health 2008, 3, 271–290. [Google Scholar] [CrossRef]
- Lunt, N.; Hardey, M.; Mannion, R. Nip, Tuck and Click: Medical Tourism and the Emergence of Web-Based Health Information. Open Med. Inform. J. 2010, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.; Crooks, V.A.; Snyder, J. ‘I didn’t even know what I was looking for’: A qualitative study of the decision-making processes of Canadian medical tourists. Global. Health 2012, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.M.; Ting, D.H. Healthcare marketing: Contemporary salient issues and future research directions. Int. J. Healthc. Manag. 2012, 5, 3–11. [Google Scholar] [CrossRef]
- Eissler, L.A.; Casken, J. Seeking health care through international medical tourism. J. Nurs. Scholarsh. 2013, 45, 177–184. [Google Scholar] [CrossRef]
- Gan, L.L.; Frederick, J.R. Medical Tourists: Who Goes and What Motivates Them? Health Mark. Q. 2013, 30, 177–194. [Google Scholar] [CrossRef]
- Lunt, N.; Mannion, R.; Exworthy, M. A Framework for Exploring the Policy Implications of UK Medical Tourism and International Patient Flows. Soc. Policy Adm. 2013, 47, 1–25. [Google Scholar] [CrossRef]
- Henson, J.N.; Guy, B.S.; Dotson, M.J. Should I stay or should I go? Motivators, decision factors, and information sources influencing those predisposed to medical tourism. Int. J. Healthc. Manag. 2015, 8, 4–14. [Google Scholar] [CrossRef]
- Boguszewicz-Kreft, M. The Consumer’s Perspective in Medical Tourism—Identification of Research Gaps. Handel Wewnętrzny 2017, 5, 63–71. [Google Scholar]
- Nagashima, A. A Comparison of Japanese and U. S. Attitudes toward Foreign Products. J. Mark. 1970, 34, 68. [Google Scholar]
- Narayana, C. Aggregate images of American and Japanese products. Columbia J. World Bus. 1981, 16, 31–35. [Google Scholar]
- Harrison-Walker, L.J. The relative effects of national stereotype and advertising information on the selection of a service provider: An empirical study. J. Serv. Mark. 1995, 9, 47–59. [Google Scholar] [CrossRef]
- Verlegh, P.W.J.; Steenkamp, J.B. A Review and Meta-Analysis of Country-of-Origin Research. A Rev. Meta Anal. Ctry. Orig. Res. 1999, 20, 521–546. [Google Scholar] [CrossRef]
- Gürhan-Canali, Z.; Mahaswaran, D. Cultural Variations in Country of Origin Effects. J. Mark. Res. 2000, 37, 309–317. [Google Scholar] [CrossRef]
- Javalgi, R.G.R.; Cutler, B.D.; Winans, W.A. At your service! Does country of origin research apply to services? J. Serv. Mark. 2001, 15, 565–582. [Google Scholar] [CrossRef]
- Pharr, J.M. Synthesizing Country-of-Origin Research from the Last Decade: Is the Concept Still Salient in an Era of Global Brands? J. Mark. Theory Pract. 2005, 13, 34–45. [Google Scholar] [CrossRef]
- Lee, J.A.; Garbarino, E.; Lerman, D.; Steenkamp, J.-B.E.M.; Yeniyurt, S.; Townsend, J.D. How cultural differences in uncertainty avoidance affect product perceptions. Int. Mark. Rev. 2007, 24, 330–349. [Google Scholar]
- Chattalas, M.; Kramer, T.; Takada, H. The impact of national stereotypes on the country of origin effect: A conceptual framework. Int. Mark. Rev. 2008, 25, 54–74. [Google Scholar] [CrossRef]
- D’Astous, A.; Voss, Z.G.; Colbert, F.; Carù, A.; Caldwell, M.; Courvoisier, F. Product-country images in the arts: A multi-country study. Int. Mark. Rev. 2008, 25, 379–403. [Google Scholar] [CrossRef]
- Sharma, P. Demystifying cultural differences in country-of-origin effects: Exploring the moderating roles of product type, consumption context, and involvement. J. Int. Consum. Mark. 2011, 23, 344–364. [Google Scholar] [CrossRef]
- Boguszewicz-Kreft, M.; Sokołowska, K.; Magier-Łakomy, E.; Janiunaite, B. The country of origin of services and consumers as the determinants of purchase intentions in medical tourism. J. East Eur. Manag. Stud. 2019, 24, 464–481. [Google Scholar] [CrossRef]
- Ajzen, I. Theory of Planned Behavior (TPB). Available online: https://people.umass.edu/aizen/index.html (accessed on 31 August 2019).
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Malhotra, N.K. Marketing Research, an Applied Orientation; Pearson Education: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Harrell, F.E.J. Regression Modeling Strategies; Springer: Heidelberg, Germany, 2015. [Google Scholar]
- Aczel, A.D.; Sounderpandian, J. Complete Business Statistics; McGraw-Hill Higher Education: Boston, MA, USA, 2009. [Google Scholar]
- Scheffé, H. The Analysis of Variance; John Wiley & Sons: Hoboken, NJ, USA, 1999. [Google Scholar]
- Yuzhanin, S.; Fisher, D. The efficacy of the theory of planned behavior for predicting intentions to choose a travel destination: A review. Tour. Rev. 2016, 71, 135–147. [Google Scholar] [CrossRef]
- Holliday, R.; Bell, D.; Jones, M.; Hardy, K.; Hunter, E.; Probyn, E.; Taylor, J.S. Beautiful face, beautiful place: Relational geographies and gender in cosmetic surgery tourism websites. Gender Place Cult. 2015, 22, 90–106. [Google Scholar] [CrossRef]
- Lubowiecki-Vikuk, A.; Dryglas, D. Medical tourism services and medical tourism destinations in Central and Eastern Europe—The opinion of Britons and Germans. Econ. Res. Istraz. 2019, 32, 1256–1274. [Google Scholar] [CrossRef]


{kind=link}
| Dependent Variable | Descriptive Statistics | Multiple Regression Results | ||||
|---|---|---|---|---|---|---|
| Mean | Std. dev. | Coefficient | Std. Error | t | p-Value | |
| Behavioural intention | 1.20 | 1.57 | - | - | - | - |
| (Intercept) | - | - | 0.299 | 0.106 | 2.81 | 0.005 |
| Attitude | 1.07 | 1.5 | 0.439 | 0.055 | 7.92 | 0.000 |
| Subjective norms | 1.09 | 1.1 | 0.206 | 0.044 | 4.64 | 0.000 |
| Perceived control | 1.12 | 1.4 | 0.191 | 0.044 | 4.38 | 0.000 |
| Gender (male) | 0.53 | - | −0.029 | 0.117 | 0.25 | 0.804 |
| TPB Component | Country | n | Mean | Std. dev. | ANOVA | Groups Based on Scheffé Test * |
|---|---|---|---|---|---|---|
| Behavioural intention | Poland | 213 | 1.39 | 1.53 | F(2, 518) = 2.78, p = 0.063 | - |
| Turkey | 125 | 1.08 | 1.55 | - | ||
| Jordan | 183 | 1.05 | 1.61 | - | ||
| Attitude | Poland | 213 | 1.17 | 1.13 | F(2, 518) = 1.64, p = 0.196 | - |
| Turkey | 125 | 1.08 | 1.28 | - | ||
| Jordan | 183 | 0.96 | 1.08 | - | ||
| Subjective norms | Poland | 213 | 0.93 | 1.51 | F(2, 518) = 3.12, p = 0.045 | b |
| Turkey | 125 | 1.34 | 1.58 | a | ||
| Jordan | 183 | 1.12 | 1.43 | ab | ||
| Perceived control | Poland | 213 | 1.32 | 1.51 | F(2, 518) = 5.55, p = 0.004 | a |
| Turkey | 125 | 0.75 | 1.68 | b | ||
| Jordan | 183 | 1.14 | 1.43 | ab |
| Dependent Variable | Country | Coefficient | Std. Error | t | p-Value |
|---|---|---|---|---|---|
| (Intercept) | Poland | 0.156 | 0.159 | 0.98 | 0.328 |
| Turkey | 0.436 | 0.231 | 1.89 | 0.062 | |
| Jordan | 0.280 | 0.184 | 1.53 | 0.129 | |
| Attitude | Poland | 0.430 | 0.091 | 4.70 | 0.000 |
| Turkey | 0.219 | 0.097 | 2.25 | 0.027 | |
| Jordan | 0.588 | 0.102 | 5.80 | 0.000 | |
| Subjective norms | Poland | 0.086 | 0.066 | 1.31 | 0.193 |
| Turkey | 0.406 | 0.091 | 4.46 | 0.000 | |
| Jordan | 0.191 | 0.080 | 2.40 | 0.018 | |
| Perceived control | Poland | 0.374 | 0.069 | 5.42 | 0.000 |
| Turkey | 0.016 | 0.084 | 0.19 | 0.849 | |
| Jordan | 0.086 | 0.079 | 1.09 | 0.277 | |
| Gender (male–female) | Poland | 0.239 | 0.166 | 1.44 | 0.152 |
| Turkey | −0.287 | 0.246 | −1.16 | 0.247 | |
| Jordan | −0.275 | 0.215 | −1.28 | 0.202 |
| Dependent Variable | Comparison | Coefficient | Std. Error | t | p-Value |
|---|---|---|---|---|---|
| Attitude | Turkey-Poland | −0.211 | 0.138 | −1.53 | 0.127 |
| Jordan-Poland | 0.159 | 0.139 | 1.14 | 0.254 | |
| Jordan-Turkey | 0.370 | 0.132 | 2.80 | 0.005 | |
| Subjective norms | Turkey-Poland | 0.320 | 0.114 | 2.81 | 0.005 |
| Jordan-Poland | 0.105 | 0.104 | 1.01 | 0.315 | |
| Jordan-Turkey | −0.215 | 0.114 | −1.89 | 0.059 | |
| Perceived control | Turkey-Poland | −0.358 | 0.111 | −3.22 | 0.001 |
| Jordan-Poland | −0.288 | 0.106 | −2.71 | 0.007 | |
| Jordan-Turkey | 0.070 | 0.108 | 0.65 | 0.518 | |
| Gender (male–female) | Turkey-Poland | −0.525 | 0.299 | −1.76 | 0.080 |
| Jordan-Poland | −0.513 | 0.272 | −1.89 | 0.060 | |
| Jordan-Turkey | 0.012 | 0.307 | 0.04 | 0.969 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boguszewicz-Kreft, M.; Kuczamer-Kłopotowska, S.; Kozłowski, A.; Ayci, A.; Abuhashesh, M. The Theory of Planned Behaviour in Medical Tourism: International Comparison in the Young Consumer Segment. Int. J. Environ. Res. Public Health 2020, 17, 1626. https://doi.org/10.3390/ijerph17051626
Boguszewicz-Kreft M, Kuczamer-Kłopotowska S, Kozłowski A, Ayci A, Abuhashesh M. The Theory of Planned Behaviour in Medical Tourism: International Comparison in the Young Consumer Segment. International Journal of Environmental Research and Public Health. 2020; 17(5):1626. https://doi.org/10.3390/ijerph17051626
Chicago/Turabian StyleBoguszewicz-Kreft, Monika, Sylwia Kuczamer-Kłopotowska, Arkadiusz Kozłowski, Ali Ayci, and Mohammd Abuhashesh. 2020. "The Theory of Planned Behaviour in Medical Tourism: International Comparison in the Young Consumer Segment" International Journal of Environmental Research and Public Health 17, no. 5: 1626. https://doi.org/10.3390/ijerph17051626
APA StyleBoguszewicz-Kreft, M., Kuczamer-Kłopotowska, S., Kozłowski, A., Ayci, A., & Abuhashesh, M. (2020). The Theory of Planned Behaviour in Medical Tourism: International Comparison in the Young Consumer Segment. International Journal of Environmental Research and Public Health, 17(5), 1626. https://doi.org/10.3390/ijerph17051626