Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume

Abstract
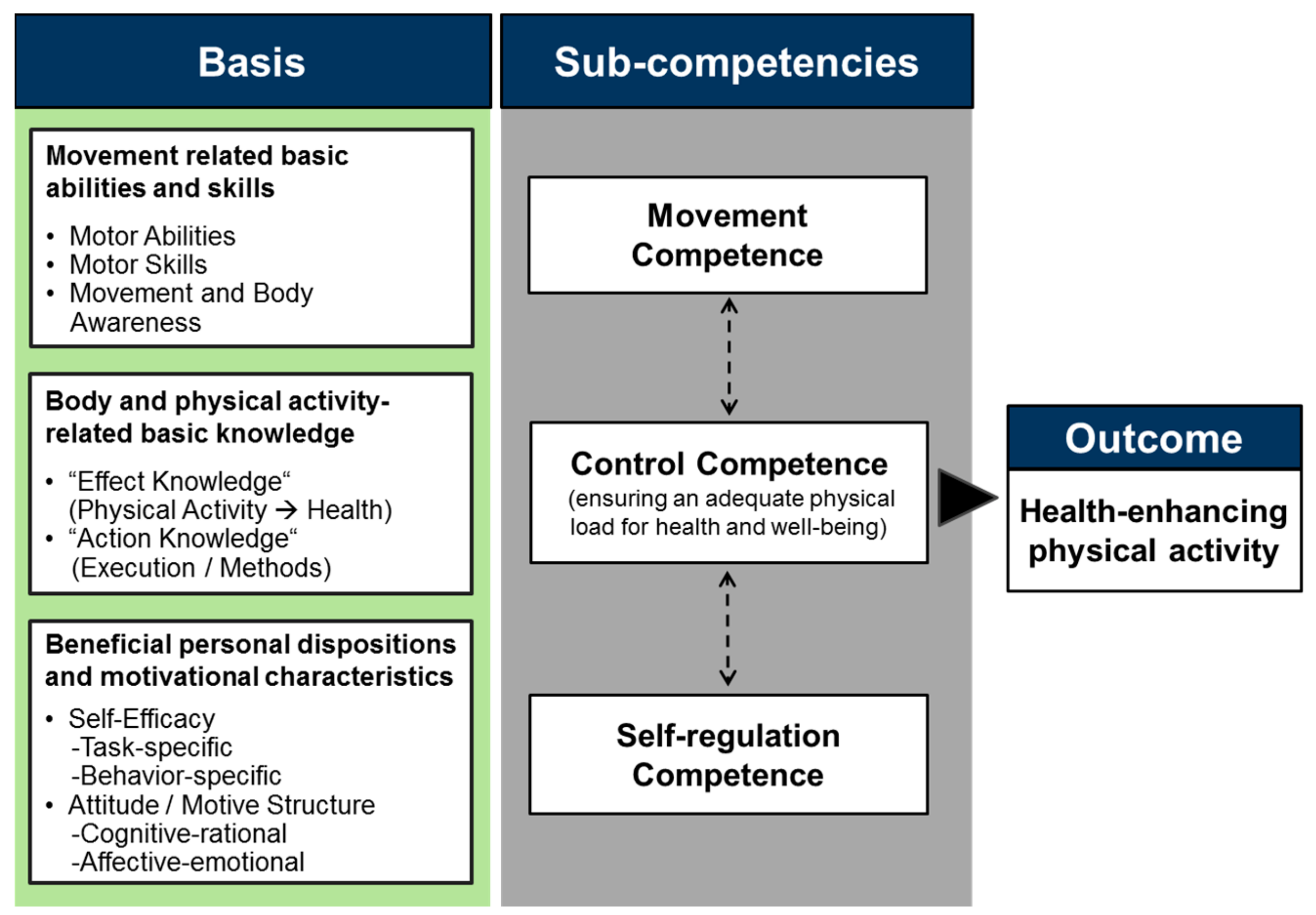
1. Introduction
2. Study A
2.1. Background
2.2. Methodology
2.2.1. Participants and Measurement
2.2.2. Data Analysis
2.2.3. Informed Consent and Ethics
2.3. Results
2.4. Discussion
3. Study B
3.1. Background
3.2. Methodology
3.2.1. Participants and Measurement
3.2.2. Data Analysis
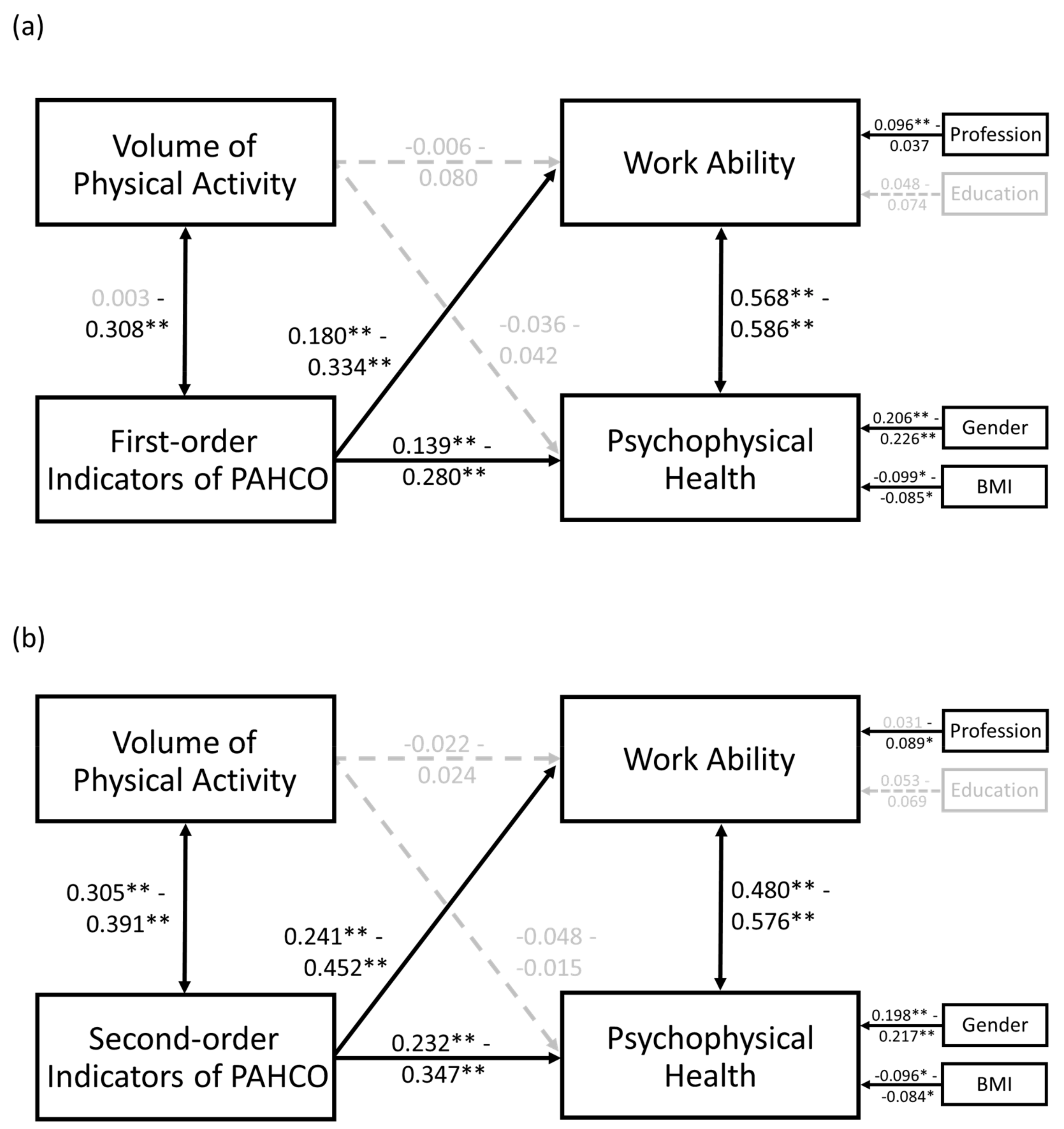
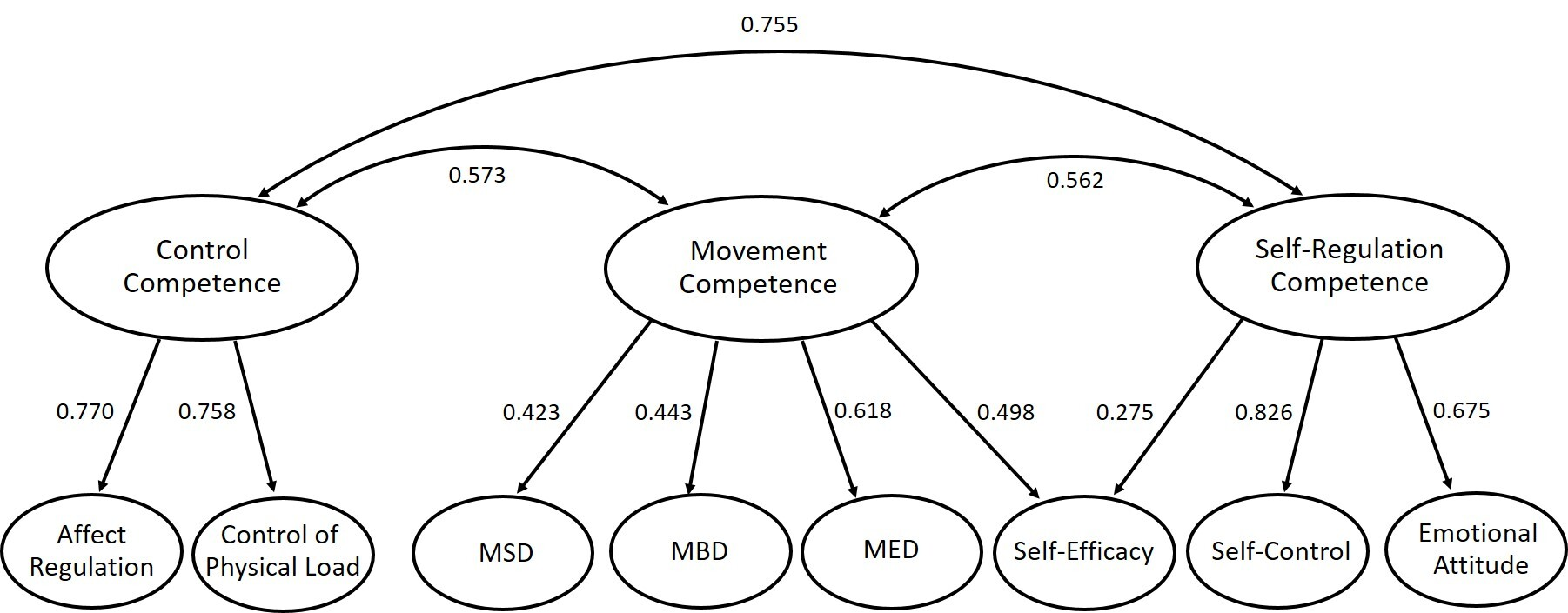
3.3. Results
3.4. Discussion
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
| Covariate Model | Statistics of the Predictors | |||
|---|---|---|---|---|
| Outcome Variable | Potential Covariate | β | t | p |
| Work Ability | Profession | 0.130 | 2.33 | 0.020 * |
| Age | −0.057 | −1.38 | 0.168 | |
| Level of Education | 0.098 | 2.35 | 0.019 * | |
| Sex | −0.007 | −0.133 | 0.894 | |
| BMI | −0.004 | 0.106 | 0.916 | |
| Psychophysical Health | Profession | 0.088 | 1.62 | 0.105 |
| Age | −0.045 | −1.09 | 0.314 | |
| Level of Education | 0.044 | 1.07 | 0.287 | |
| Sex | 0.180 | 3.57 | <0.001 ** | |
| BMI | −0.093 | −2.41 | 0.016 * | |
References
- OECD. OECD Employment Outlook 2019: The Future of Work; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Federal Ministry of Education and Research. Zukunft der Arbeit—Innovationen für die Arbeit von morgen. [The future of workInnovations for the work of tomorrow]; Federal Ministry of Education and Research: Bonn, Germany, 2016. [Google Scholar]
- Hanvold, T.N.; Kines, P.; Nykänen, M.; Thomée, S.; Holte, K.A.; Vuori, J.; Wærsted, M.; Veiersted, K.B. Occupational safety and health among young workers in the Nordic countries: A systematic literature review. Saf. Health Work 2019, 10, 3–20. [Google Scholar] [CrossRef]
- Betz, M.; Graf-Weber, G.; Kapelke, C.; Wenchel, K. Gesundheitsförderung in der überbetrieblichen Ausbildung am Beispiel des Kfz-Handwerks [Health promotion in intervocational education using the automotive trade as an example]. Dtsch med Wochenschr 2012, 137. [Google Scholar] [CrossRef]
- Bomball, J.; Schwanke, A.; Stöver, M.; Görres, S. Gesunde Pflege beginnt in der Pflegeausbildung [Healthy care begins with nursing training]. Die Schwester Der Pfleger 2010, 49, 1048–1054. [Google Scholar]
- Bonevski, B.; Guillaumier, A.; Paul, C.; Walsh, R. The vocational education setting for health promotion: A survey of students’ health risk behaviours and preferences for help. Health Promot. J. Austr. 2013, 24, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, F.; von Lindeman, K.; Klewer, J.; Kugler, J. BMI, physical inactivity, cigarette and alcohol consumption in female nursing students: A 5-year comparison. BMC Med. Educ. 2014, 21, 82. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Proper, K.I.; van Oostrom, S.H. The effectiveness of workplace health promotion interventions on physical and mental health outcomes—a systematic review of reviews. Scand. J. Work Environ. Health 2019. [Google Scholar] [CrossRef]
- Kuoppala, J.; Lamminpää, A.; Husman, P. Work health promotion, job well-being, and sickness absences--a systematic review and meta-analysis. J. Occup. Environ. Med. 2008, 50, 1216–1227. [Google Scholar] [CrossRef]
- Grüne, E.; Popp, J.; Carl, J.; Pfeifer, K. Bewegungsförderungsmaßnahmen in der beruflichen Bildung: Ein systematisches Review [Physical activity interventions in vocational education and training: A systematic review]. In Sport im öffentlichen Raum. Abstractband des 24. dvs-Hochschultags vom 18. bis 20. September 2019 in Berlin; Arampatzis, A., Braun, S., Schmitt, K., Wolfarth, B., Eds.; Feldhaus: Hamburg, Germany, 2019. [Google Scholar]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; de Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F.M. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef]
- Lee, J.A.; Williams, S.M.; Brown, D.D.; Laurson, K.R. Concurrent validation of the Actigraph gt3x+, Polar Active accelerometer, Omron HJ-720 and Yamax Digiwalker SW-701 pedometer step counts in lab-based and free-living settings. J. Sports Sci. 2015, 33, 991–1000. [Google Scholar] [CrossRef]
- Ozemek, C.; Kirschner, M.M.; Wilkerson, B.S.; Byun, W.; Kaminsky, L.A. Intermonitor reliability of the GT3X+ accelerometer at hip, wrist and ankle sites during activities of daily living. Physiol. Meas. 2014, 35, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, R.; Klaperski, S.; Gerber, M.; Seelig, H. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen [Measurement of Physical Activity and Sport Activity With the BSA Questionnaire]. Zeitschrift für Gesundheitspsychologie 2015, 23, 60–76. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Mâsse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Wanner, M.; Martin, B.W.; Meier, F.; Probst-Hensch, N.; Kriemler, S. Effects of filter choice in GT3X accelerometer assessments of free-living activity. Med. Sci. Sports Exerc. 2013, 45, 170–177. [Google Scholar] [CrossRef]
- WHO. Global Recommendations on Physical Activity For Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Tudor-Locke, C.; Craig, C.L.; Brown, W.J.; Clemes, S.A.; de Cocker, K.; Giles-Corti, B.; Hatano, Y.; Inoue, S.; Matsudo, S.M.; Mutrie, N.; et al. How many steps/day are enough? For adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 79. [Google Scholar] [CrossRef]
- Weymar, F.; Braatz, J.; Guertler, D.; van den Berg, N.; Meyer, C.; John, U.; Felix, S.B.; Dörr, M.; Ulbricht, S. Characteristics associated with non-participation in 7-day accelerometry. Prev. Med. Rep. 2015, 2, 413–418. [Google Scholar] [CrossRef][Green Version]
- Baumann, S.; Groß, S.; Voigt, L.; Ullrich, A.; Weymar, F.; Schwaneberg, T.; Dörr, M.; Meyer, C.; John, U.; Ulbricht, S. Pitfalls in accelerometer-based measurement of physical activity: The presence of reactivity in an adult population. Scand. J. Med. Sci. Sports 2018, 28, 1056–1063. [Google Scholar] [CrossRef]
- Trost, S.G.; Zheng, Y.; Wong, W.-K. Machine learning for activity recognition: Hip versus wrist data. Physiol. Meas. 2014, 35, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Swartz, A.M.; Strath, S.J.; Bassett, D.R.; O’Brien, W.L.; King, G.A.; Ainsworth, B.E. Estimation of energy expenditure using CSA accelerometers at hip and wrist sites. Med. Sci. Sports Exerc. 2000, 32, S450–S456. [Google Scholar] [CrossRef] [PubMed]
- Jun, S.Y.; Kim, J.; Choi, H.; Kim, J.S.; Lim, S.H.; Sul, B.; Hong, B.Y. Physical Activity of Workers in a Hospital. Int. J. Environ. Res. Public Health 2019, 16, 532. [Google Scholar] [CrossRef] [PubMed]
- Steeves, J.A.; Tudor-Locke, C.; Murphy, R.A.; King, G.A.; Fitzhugh, E.C.; Bassett, D.R.; van Domelen, D.; Schuna, J.M.; Harris, T.B. Daily physical activity by occupational classification in us adults: NHANES 2005–2006. J. Phys. Act. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, A.; Nauerth, A.; Pfefferle, P.I. Gesundheitszustand und Gesundheitsverhalten von Auszubildenden im ersten Lehrjahr—Erste Ergebnisse einer Befragung in Bielefelder Berufskollegs [Health Status and Health Behaviour of Apprentices in the First Year of Apprenticeship—First Results of a Survey in Vocational Training Schools in Bielefeld]. Gesundheitswesen 2008, 70, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Wirth, T.; Kozak, A.; Schedlbauer, G.; Nienhaus, A. Health behaviour, health status and occupational prospects of apprentice nurses and kindergarten teachers in Germany: A cross-sectional study. J. Occup. Med. Toxicol. 2016, 11, 26. [Google Scholar] [CrossRef] [PubMed]
- Deissinger, T. Dual System. In International Encyclopedia of Education, 3rd ed.; Peterson, P., Baker, E., McGraw, B., Eds.; Elsevier: Oxford, UK, 2010; pp. 448–454. ISBN 978-008044894-7. [Google Scholar]
- Daub, U.; Budaker, B.; Schneider, U. Assistive technologies for workers in the automotive industry. In 15. Internationales Stuttgarter Symposium; Bargende, M., Reuss, H.-C., Wiedemann, J., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2015; pp. 101–110. ISBN 978-3-658-08843-9. [Google Scholar]
- Vandergrift, J.L.; Gold, J.E.; Hanlon, A.; Punnett, L. Physical and psychosocial ergonomic risk factors for low back pain in automobile manufacturing workers. Occup. Environ. Med. 2012, 69, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, A.; Bruno, S.; L’Abbate, N. A review of low back pain and musculoskeletal disorders among Italian nursing personnel. Ind. Health 2007, 45, 637–644. [Google Scholar] [CrossRef]
- Hall, C.; Heck, J.E.; Sandler, D.P.; Ritz, B.; Chen, H.; Krause, N. Occupational and leisure-time physical activity differentially predict 6-year incidence of stroke and transient ischemic attack in women. Scand. J. Work Environ. Health 2019, 45, 267–279. [Google Scholar] [CrossRef]
- Hallman, D.M.; Jørgensen, M.B.; Holtermann, A. On the health paradox of occupational and leisure-time physical activity using objective measurements: Effects on autonomic imbalance. PLoS ONE 2017, 12, e0177042. [Google Scholar] [CrossRef]
- Hu, G.-C.; Chien, K.-L.; Hsieh, S.-F.; Chen, C.-Y.; Tsai, W.-H.; Su, T.-C. Occupational versus leisure-time physical activity in reducing cardiovascular risks and mortality among ethnic Chinese adults in Taiwan. Asia Pac. J. Public Health 2014, 26, 604–613. [Google Scholar] [CrossRef]
- Kulmala, J.; Ngandu, T.; Pajala, S.; Lehtisalo, J.; Levälahti, E.; Antikainen, R.; Laatikainen, T.; Oksa, H.; Peltonen, M.; Rauramaa, R.; et al. Leisure-time and occupational physical activity in early and late adulthood in relation to later life physical functioning. J. Phys. Act. Health 2016, 13, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Holtermann, A.; Krause, N.; van der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2018, 52, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Sudeck, G.; Pfeifer, K. Physical activity-related health competence as an integrative objective in exercise therapy and health sports – conception and validation of a short questionnaire. German J. Exerc. Sport Res. 2016, 46, 74–87. [Google Scholar] [CrossRef]
- Pfeifer, K.; Sudeck, G.; Geidl, W.; Tallner, A. Bewegungsförderung und Sport in der Neurologie – Kompetenzorientierung und Nachhaltigkeit [Physical activity enhancement and sports in neurology –competence orientation and sustainability]. Neurol. Rehabil. 2013, 19, 7–19. [Google Scholar]
- Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Sudeck, G. Physical activity-related health competence, physical activity, and physical fitness: analysis of control competence for the self-directed exercise of adolescents. Int. J. Environ. Res. Public Health 2020, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Rongen, A.; Robroek, S.J.W.; van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Cadiz, D.M.; Brady, G.; Rineer, J.R.; Truxillo, D.M.; Wang, M. A review and synthesis of the work ability literature. Work Aging Retire. 2019, 5, 114–138. [Google Scholar] [CrossRef]
- Ilmarinen, J. From work ability research to implementation. Int. J. Environ. Res. Public Health 2019, 16, 2882. [Google Scholar] [CrossRef]
- Ford, M.T.; Cerasoli, C.P.; Higgins, J.A.; Decesare, A.L. Relationships between psychological, physical, and behavioural health and work performance: A review and meta-analysis. Work Stress 2011, 25, 185–204. [Google Scholar] [CrossRef]
- Jansson, I.; Björklund, A.; Perseius, K.-I.; Gunnarsson, A.B. The concept of ‘work ability’ from the view point of employers. Work J. Prev. Assesment Rehabil. 2015, 52, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Vänni, K.; Virtanen, P.; Luukkaala, T.; Nygård, C.-H. Relationship between perceived work ability and productivity loss. Int. J. Occup. Saf. Ergon. 2012, 18, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Reeuwijk, K.G.; Robroek, S.J.W.; Niessen, M.A.J.; Kraaijenhagen, R.A.; Vergouwe, Y.; Burdorf, A. The prognostic value of the work ability index for sickness absence among office workers. PLoS ONE 2015, 10, e0126969. [Google Scholar] [CrossRef]
- Alavinia, S.M.; de Boer, A.G.E.M.; van Duivenbooden, J.C.; Frings-Dresen, M.H.W.; Burdorf, A. Determinants of work ability and its predictive value for disability. Occup. Med. 2009, 59, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Faragher, E.B.; Cass, M.; Cooper, C.L. The relationship between job satisfaction and health: A meta-analysis. Occup. Environ. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.; Bjaalid, G.; Mikkelsen, A. Work climate and the mediating role of workplace bullying related to job performance, job satisfaction, and work ability: A study among hospital nurses. J. Adv. Nurs. 2017, 73, 2709–2719. [Google Scholar] [CrossRef]
- Camerino, D.; Conway, P.M.; van der Heijden, B.I.J.M.; Estryn-Béhar, M.; Costa, G.; Hasselhorn, H.-M. Age-dependent relationships between work ability, thinking of quitting the job, and actual leaving among Italian nurses: A longitudinal study. Int. J. Nurs. Stud. 2008, 45, 1645–1659. [Google Scholar] [CrossRef]
- Sjogren-Ronkä, T.; Ojanen, M.T.; Leskinen, E.K.; Mustalampi, S.T.; Mälkiä, E.A. Physical and psychosocial prerequisites of functioning in relation to work ability and general subjective well-being among office workers. Scand. J. Work Environ. Health 2002, 28, 184–190. [Google Scholar] [CrossRef]
- Sörensen, L.E.; Pekkonen, M.M.; Männikkö, K.H.; Louhevaara, V.A.; Smolander, J.; Alén, M.J. Associations between work ability, health-related quality of life, physical activity and fitness among middle-aged men. Appl. Ergon. 2008, 39, 786–791. [Google Scholar] [CrossRef]
- Ilmarinen, J. Work ability—a comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef]
- Hetzel, C.; Baumann, R.; Bilhuber, H.; Mozdzanowski, M. Ermittlung der Arbeitsfähigkeit anhand eines reduzierten Work Ability Index (WAI-r) [Determination of work ability by a Work Ability Index short form (WAI-r)]. ASU Arb. Soz. Umw. 2014, 49, 368–374. [Google Scholar]
- Morfeld, M.; Kirchberger, I.; Bullinger, M. SF-36 Fragebogen zum Gesundheitszustand—DeutscheVersion des Short Form-36 Health Survey, [German version of the Short Form-36 Health Survey]; Hogrefe: Göttingen, Germany, 2011. [Google Scholar]
- Carl, J.; Geidl, W.; Sudeck, G.; Schultz, K.; Pfeifer, K. Competencies for a healthy physically active lifestyle —Validation of an integrative model. ResearchSquare [preprint from 2020-01-14]. 2020. [Google Scholar] [CrossRef]
- Carl, J.; Semrau, J.; Pfeifer, K. Physical Activity-Related Health Competence: Using the PArC-AVE Study for an Extended Model Validation. In Abstract Book of the 23rd Annual Congress of the Eurpean College of Sport Sciences, Dublin, Ireland, 4–7 July 2018; Murphy, M., Boreham, C., De Vito, G., Tsolakidis, E., Eds.; SporTools: Cologne, Germany, 2018. [Google Scholar]
- Backhaus, K.; Erichson, B.; Weiber, R. Fortgeschrittene Multivariate Analysemethoden—Eine anwendungsorientierte Einführung [Advanced multivariate methods of analysis—An application-oriented introduction], 3, revised and actualized; Gabler: Berlin, Germany, 2015; ISBN 3662460866. [Google Scholar]
- El Fassi, M.; Bocquet, V.; Majery, N.; Lair, M.L.; Couffignal, S.; Mairiaux, P. Work ability assessment in a worker population: Comparison and determinants of work ability index and work ability score. BMC Public Health 2013, 13, 305–314. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Correction for multiple testing: Is there a resolution? Chest 2011, 140, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical power analysis for the behavioral sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Rosseel, Y. Package lavaan. Available online: https://cran.r-project.org/web/packages/lavaan/lavaan.pdf (accessed on 12 August 2019).
- Warburton, D.E.R.; Bredin, S.S.D. Reflections on physical activity and health: what should we recommend? Can. J. Cardiol. 2016, 32, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Taunton, J.; Bredin, S.S.D.; Isserow, S.H. The risk-benefit paradox of exercise. BC Med J. 2016, 58, 210–218. [Google Scholar]
- Tamminen-Peter, L.; Östring, E.; Sormunen, E. Improving ergonomics competences in the social and health care sector in Finland. In Health and Social Care Systems of the Future: Demographic Changes, Digital Age and Human Factors; Cotrim, T.P., Serranheira, F., Suosa, P., Hignett, S., Albolino, S., Tartaglia, R., Eds.; Springer: Cham, Switzerland, 2019; pp. 90–98. [Google Scholar]
- Ashford, S.; Edmunds, J.; French, D.P. What is the best way to change self-efficacy to promote lifestyle and recreational physical activity? A systematic review with meta-analysis. Br. J. Health Psychol. 2010, 15, 265–288. [Google Scholar] [CrossRef] [PubMed]
- Friese, M.; Hofmann, W.; Wiers, R.W. On taming horses and strengthening riders: Recent developments in research on interventions to improve self-control in health behaviors. Self Identity 2011, 10, 336–351. [Google Scholar] [CrossRef]
- European Centre for the Development of Vocational Training. Insights into skill shortaged and skill mismatch: Learning from Cedefop’s European skills and jobs survey. Available online: https://www.cedefop.europa.eu/files/3075_en.pdf (accessed on 7 December 2019).
- Bruland, D.; Voß, M.; Schulenkorf, T.; Latteck, Ä.-D. Mit Schwung und Energie durch den Tag. Partizipative Forschung zur Förderung der bewegungsbezogenen Gesundheitskompetenz bei Menschen mit Lernschwierigkeiten [With enthusiasm and energy through the day. Participatory research to promote physical-activity-related health literacy in people with intellectual disabilities]. Prävention Gesundh. 2019, 10, 1048. [Google Scholar] [CrossRef]
- Haible, S.; Volk, C.; Demetriou, Y.; Höner, O.; Thiel, A.; Trautwein, U.; Sudeck, G. Promotion of physical activity-related health competence in physical education: Study protocol for the GEKOS cluster randomized controlled trial. BMC Public Health 2019, 19, 396. [Google Scholar] [CrossRef]
- Geidl, W.; Semrau, J.; Streber, R.; Lehbert, N.; Wingart, S.; Tallner, A.; Wittmann, M.; Wagner, R.; Schultz, K.; Pfeifer, K. Effects of a brief, pedometer-based behavioral intervention for individuals with COPD during inpatient pulmonary rehabilitation on 6-week and 6-month objectively measured physical activity: Study protocol for a randomized controlled trial. Trials 2017, 18, 396. [Google Scholar] [CrossRef] [PubMed]
- Popp, J.; Carl, J.; Grüne, E.; Semrau, J.; Gelius, P.; Pfeifer, K. Physical activity promotion in German vocational education: Does capacity building work? Health Promot. Int. 2020. (In press)


| Parameter |
Activity counts [cpm] [18] | MET Values |
Apprentices of nursing care (n = 28) |
Apprentices of Automotive Mechatronics (n = 27) |
Group Comparison | Group Comparison, Adjusted for Wearing Time |
|---|---|---|---|---|---|---|
|
Sedentary Behavior (minutes /day) | 0–99 | <1.50 | 349.01 ± 54.81 | 397.86 ± 52.53 | F(1, 53) = 11.4, p < 0.001 **, d = 0.91 | F(1, 52) = 1.17, p = 0.284 |
|
Light PA (minutes/day) | 100–1951 | 1.50–2.99 | 232.53 ± 37.09 | 276.13 ± 37.89 | F(1, 53) = 18.6, p < 0.001 **, d = 1.16 | F(1, 52) = 1.10, p = 0.300 |
|
Moderate PA (minutes/week) | 1952–5724 | 3.00–5.99 | 415.64 ± 135.19 | 528.43 ± 168.16 | F(1, 53) = 7.54, p < 0.001 **, d = 0.74 | F(1, 52) = 0.027, p = 0.869 |
| Vigorous PA (minutes/week) | ≥5725 | ≥6.00 | 15.75 ± 17.32 | 30.83 ± 42.13 | F(1, 53) = 3.05, p = 0.087 | F(1, 52) = 0.798, p = 0.376 |
| Number of Steps (per day) | - | - | 16,822 ± 2,353 | 21,215 ± 3,704 | F(1, 53) = 27.8, p < 0.001 **, d = 1.42 | F(1, 52) = 2.12, p = 0.152 |
|
Wearing Time (minutes/day) | - | - | 643.16 ± 47.80 | 753.88 ± 79.42 | F(1, 53) = 39.6, p < 0.001 **, d = 1.70 | - |
| Variable | Description |
|---|---|
| Sample Size | n = 745 |
| Profession | Automotive Mechatronics (66.6%), Nursing Care (33.4%) |
| Gender | Male (59.1%), Female (40.9%) |
| Age | 19.06 ± 3.38 Years [Range 15–48] |
| Level of Education | Hauptschule/Middle School (22.3%), Realschule/Junior High School (57.3%), Fachhochschule/Senior High School (4.5%), Abitur/University Entrance Qualification (13.8%), Other Qualification (2.1%) |
| Body Mass Index [kg/m²] | 23.10 ± 3.87 [Range 14.7–43.3] |
| Progress within the Apprenticeship Program | First Year (54.4%), Second Year (23.0%), Third Year (18.1%), Supplementary Year (4.5%) |
| Volume of Sport Activity (BSA) [minutes/week] | 218.33 ± 256.50 |
| Volume of Overall PA (BSA) [minutes/week] | 451.41 ± 397.08 |
| Work Ability (WAI-r) Index | 30.14 ± 3.76 [Range 8–36] |
| Work Ability (WAI-r) Classification | Excellent (29.7%), Good (52.0%), Moderate (16.5%), Bad (1.8%) |
| The Model and included variables | Outcome Work Ability | Outcome Psychophysical Health | |||||
|---|---|---|---|---|---|---|---|
| Model | Independent Variable | b | z | p | b | z | p |
| M1a | Volume of PA | 0.031 | 0.748 | 0.455 | 0.017 | 0.423 | 0.672 |
| MSD | 0.334 | 4.82 | <0.001 ** | 0.139 | 3.31 | 0.001 ** | |
| M1b | Volume of PA | 0.016 | 0.379 | 0.705 | −0.014 | −0.342 | 0.733 |
| MED | 0.264 | 5.36 | <0.001 ** | 0.232 | 5.18 | <0.001 ** | |
| M1c | Volume of PA | 0.080 | 1.89 | 0.059 | 0.042 | 1.02 | 0.308 |
| MBD | 0.188 | 3.43 | 0.001 ** | 0.201 | 4.24 | <0.001 ** | |
| M1d | Volume of PA | 0.042 | 0.986 | 0.324 | 0.000 | 0.011 | 0.991 |
| Control of Physical Load | 0.180 | 3.72 | <0.001 ** | 0.189 | 4.05 | <0.001 ** | |
| M1e | Volume of PA | 0.032 | 0.756 | 0.450 | −0.004 | −0.100 | 0.921 |
| Affect Regulation | 0.192 | 4.29 | <0.001 ** | 0.170 | 4.02 | <0.001 ** | |
| M1f | Volume of PA | 0.016 | 0.397 | 0.691 | −0.017 | −0.414 | 0.679 |
| Self-Control | 0.257 | 5.78 | <0.001 ** | 0.238 | 5.70 | <0.001 ** | |
| M1g | Volume of PA | −0.006 | −0.146 | 0.884 | −0.036 | −0.869 | 0.385 |
| Emotional Attitude | 0.312 | 7.81 | <0.001 ** | 0.280 | 6.30 | <0.001 ** | |
| M1h | Volume of PA | 0.041 | 0.984 | 0.325 | 0.012 | 0.282 | 0.778 |
| Self-Efficacy | 0.194 | 4.39 | <0.001 ** | 0.150 | 3.20 | 0.001 ** | |
| Outcome Work Ability | Outcome Psychophysical Health | ||||||
|---|---|---|---|---|---|---|---|
| Model | Independent Variable | b | z | p | b | z | p |
| M2a | Volume of PA | 0.000 | −0.006 | 0.995 | −0.018 | −0.450 | 0.653 |
| Movement Competence | 0.452 | 6.87 | <0.001 ** | 0.347 | 6.78 | <0.001 ** | |
| M2b | Volume of PA | 0.024 | 0.564 | 0.573 | −0.015 | −0.351 | 0.725 |
| Control Competence | 0.241 | 4.42 | <0.001 ** | 0.232 | 4.47 | <0.001 ** | |
| M2c | Volume of PA | −0.022 | −0.528 | 0.597 | −0.048 | −1.13 | 0.257 |
| Self-Regulation Competence | 0.373 | 7.27 | <0.001 ** | 0.328 | 6.36 | <0.001 ** | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carl, J.; Grüne, E.; Popp, J.; Pfeifer, K. Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume. Int. J. Environ. Res. Public Health 2020, 17, 793. https://doi.org/10.3390/ijerph17030793
Carl J, Grüne E, Popp J, Pfeifer K. Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume. International Journal of Environmental Research and Public Health. 2020; 17(3):793. https://doi.org/10.3390/ijerph17030793
Chicago/Turabian StyleCarl, Johannes, Eva Grüne, Johanna Popp, and Klaus Pfeifer. 2020. "Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume" International Journal of Environmental Research and Public Health 17, no. 3: 793. https://doi.org/10.3390/ijerph17030793
APA StyleCarl, J., Grüne, E., Popp, J., & Pfeifer, K. (2020). Physical Activity Promotion for Apprentices in Nursing Care and Automotive Mechatronics–Competence Counts More than Volume. International Journal of Environmental Research and Public Health, 17(3), 793. https://doi.org/10.3390/ijerph17030793