Is Adiposity Associated with the Quality of Movement Patterns in the Mid-Adolescent Period?

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
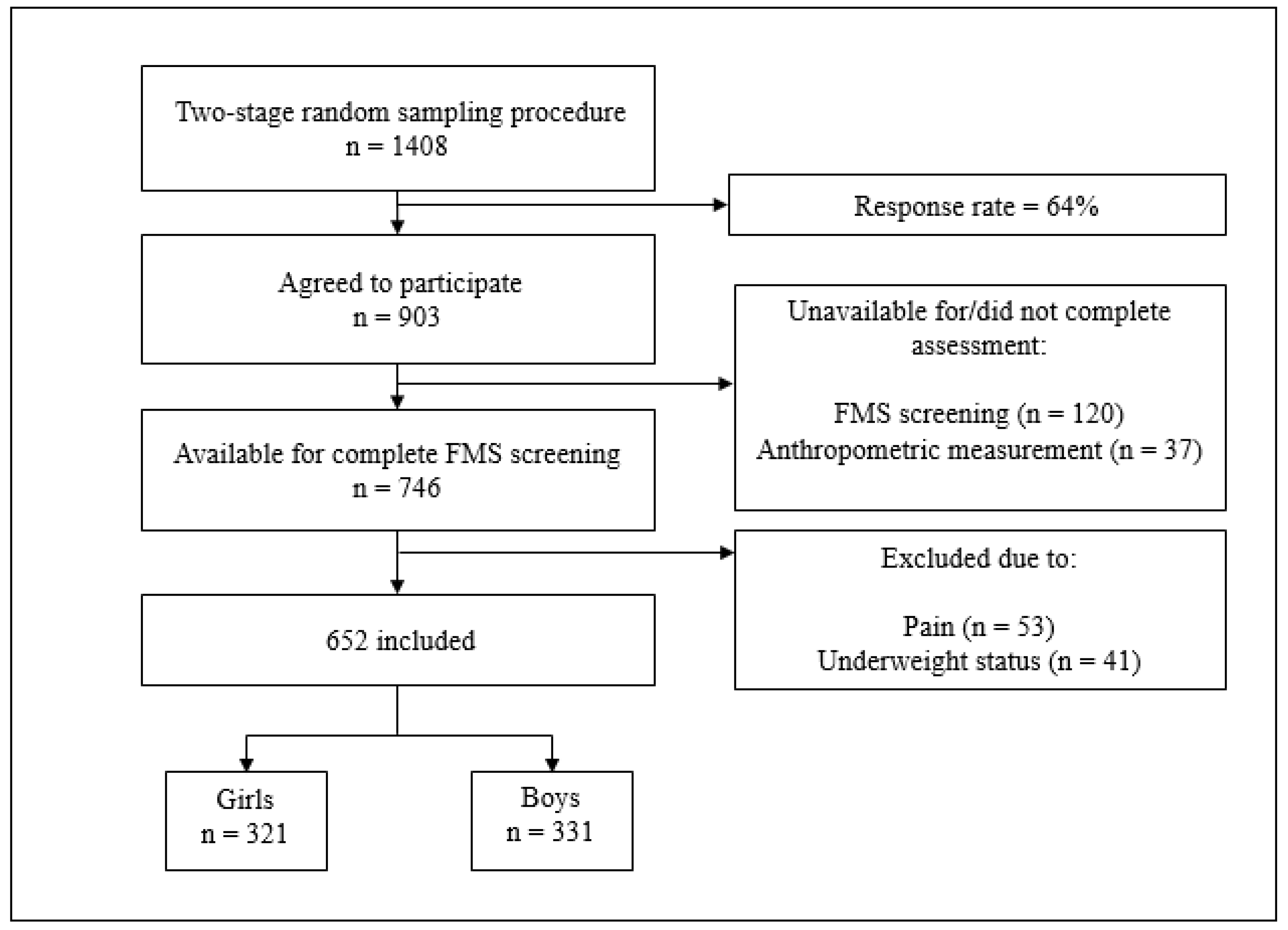
2.1. Participants
2.2. Procedures
2.2.1. Outcomes: Functional Movement Screen Variables
2.2.2. Predictors: Body Mass Index, Sum of Four Skinfolds, Waist and Hip Circumference
2.2.3. Confounders: Moderate-To-Vigorous Physical Activity (MVPA), Socioeconomic Status (SES), and Age
2.3. Data Analysis
3. Results
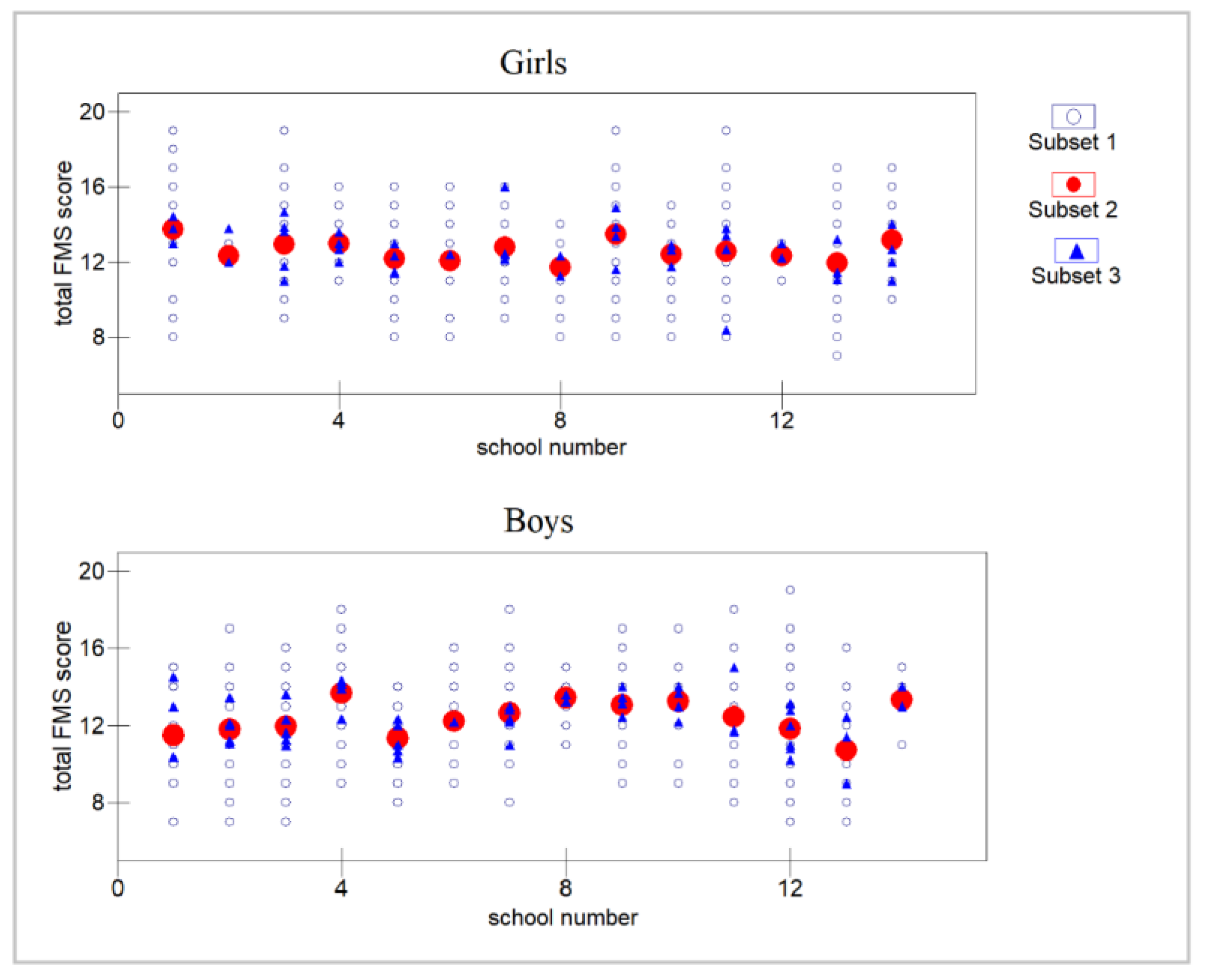
3.1. Descriptive Statistics
3.2. Differences between Children with Normal Weight and Children with Overweight and Obesity in Total FMS Score
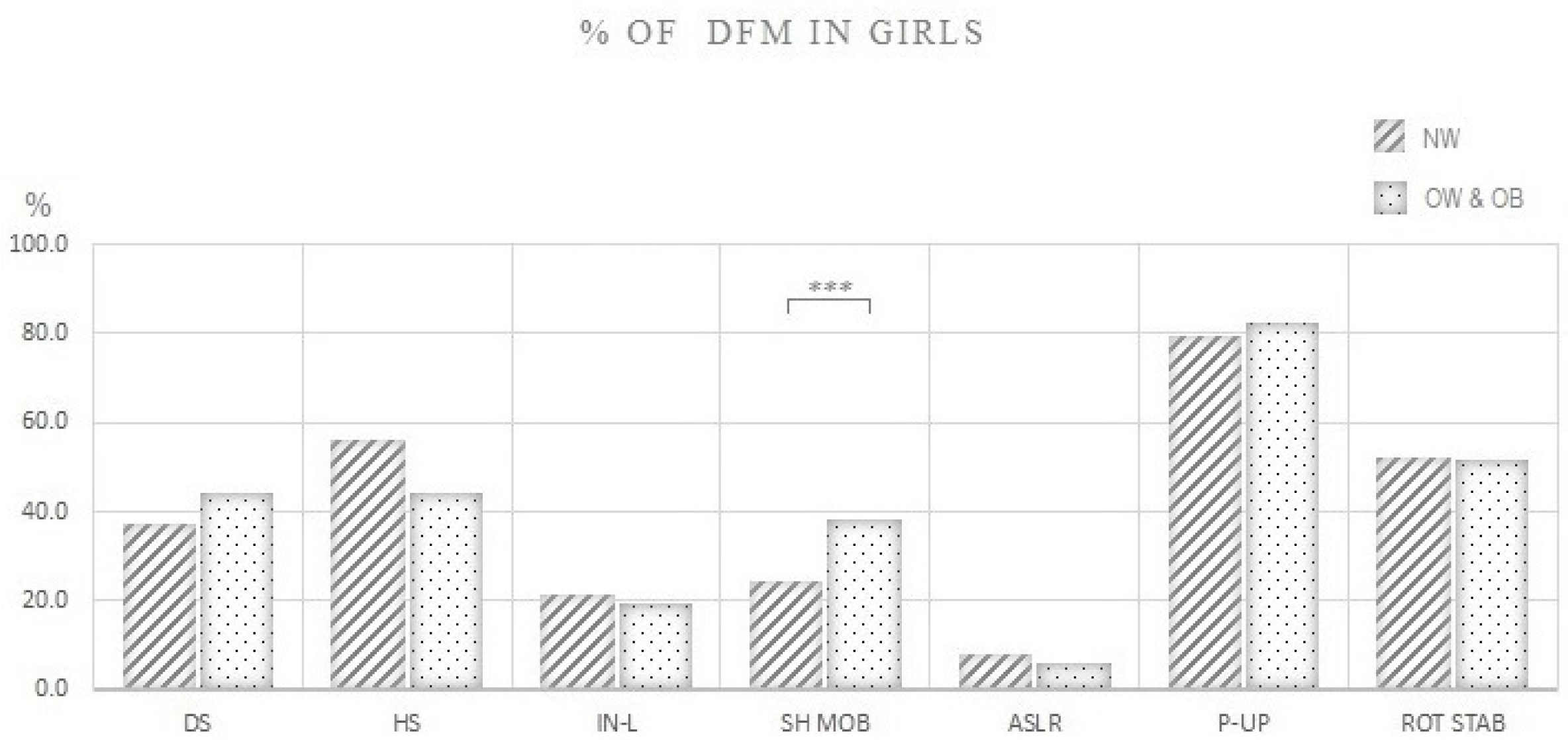
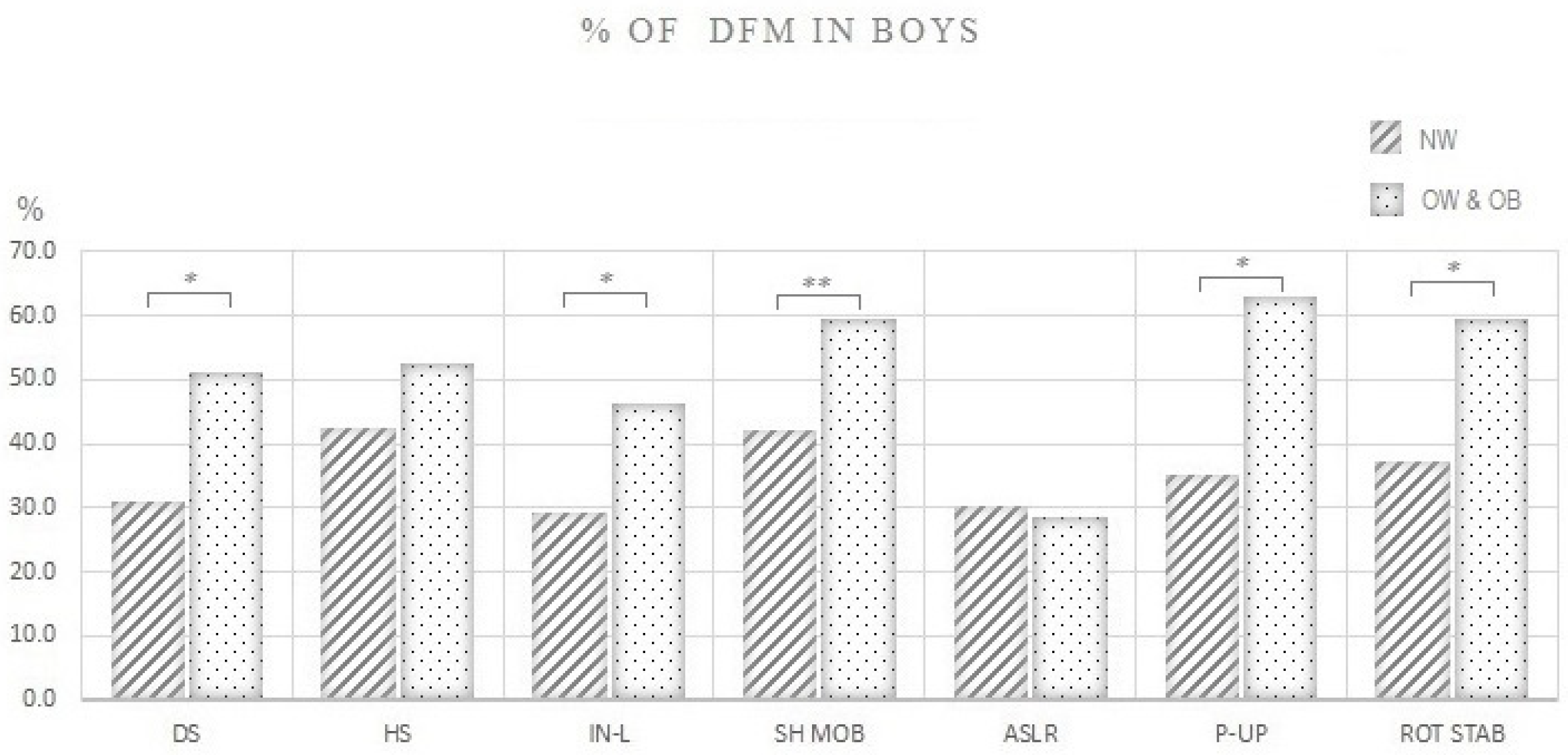
3.3. Differences between Children with Normal Weight and Children with Overweight and Obesity in the Proportion of Individuals That Performed DFM in Each FMS Test
3.4. Relationship between the Variables of Adiposity and Total FMS Score
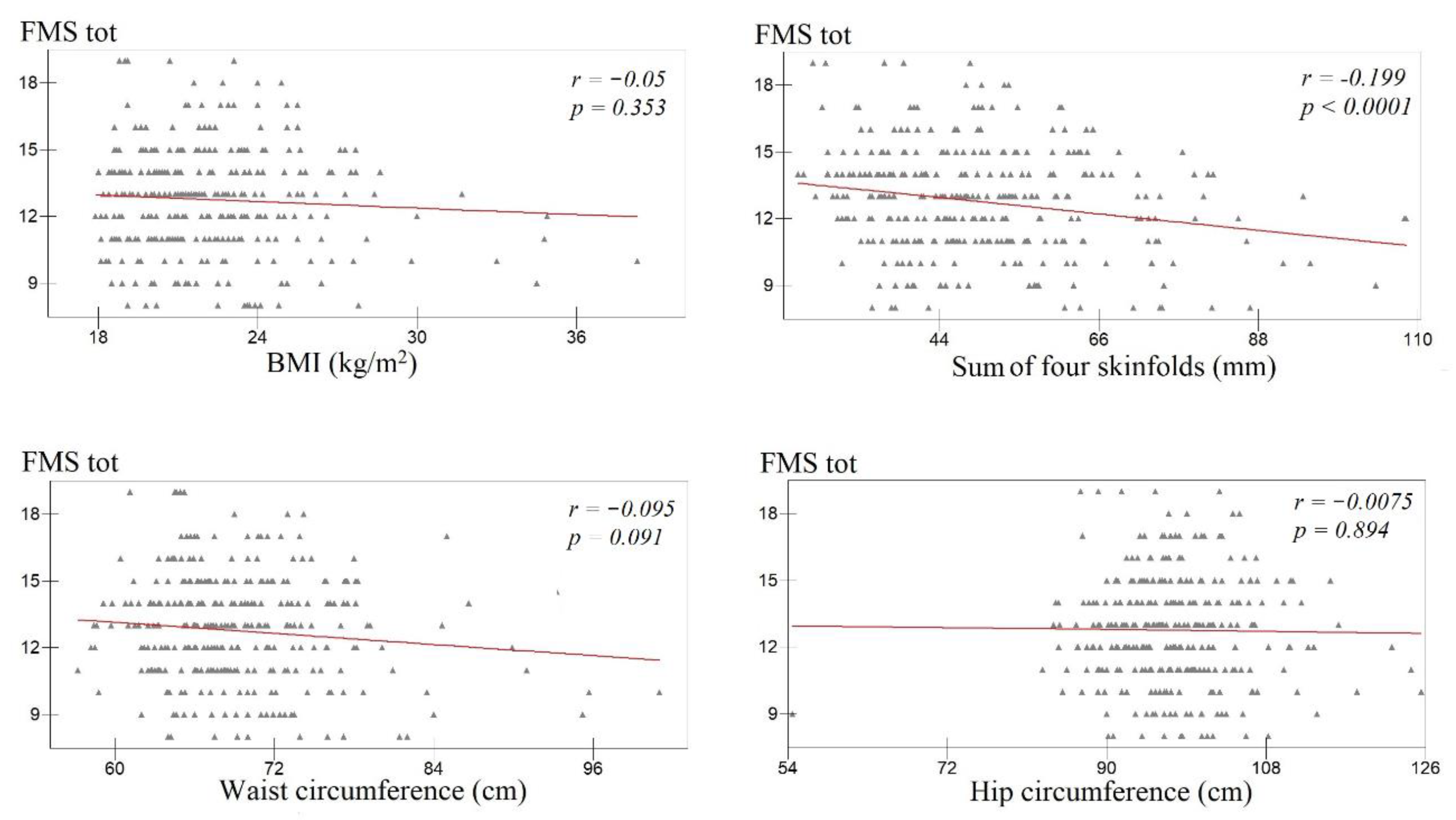
3.4.1. Association between Indicators of Adiposity and Total FMS Score among Girls
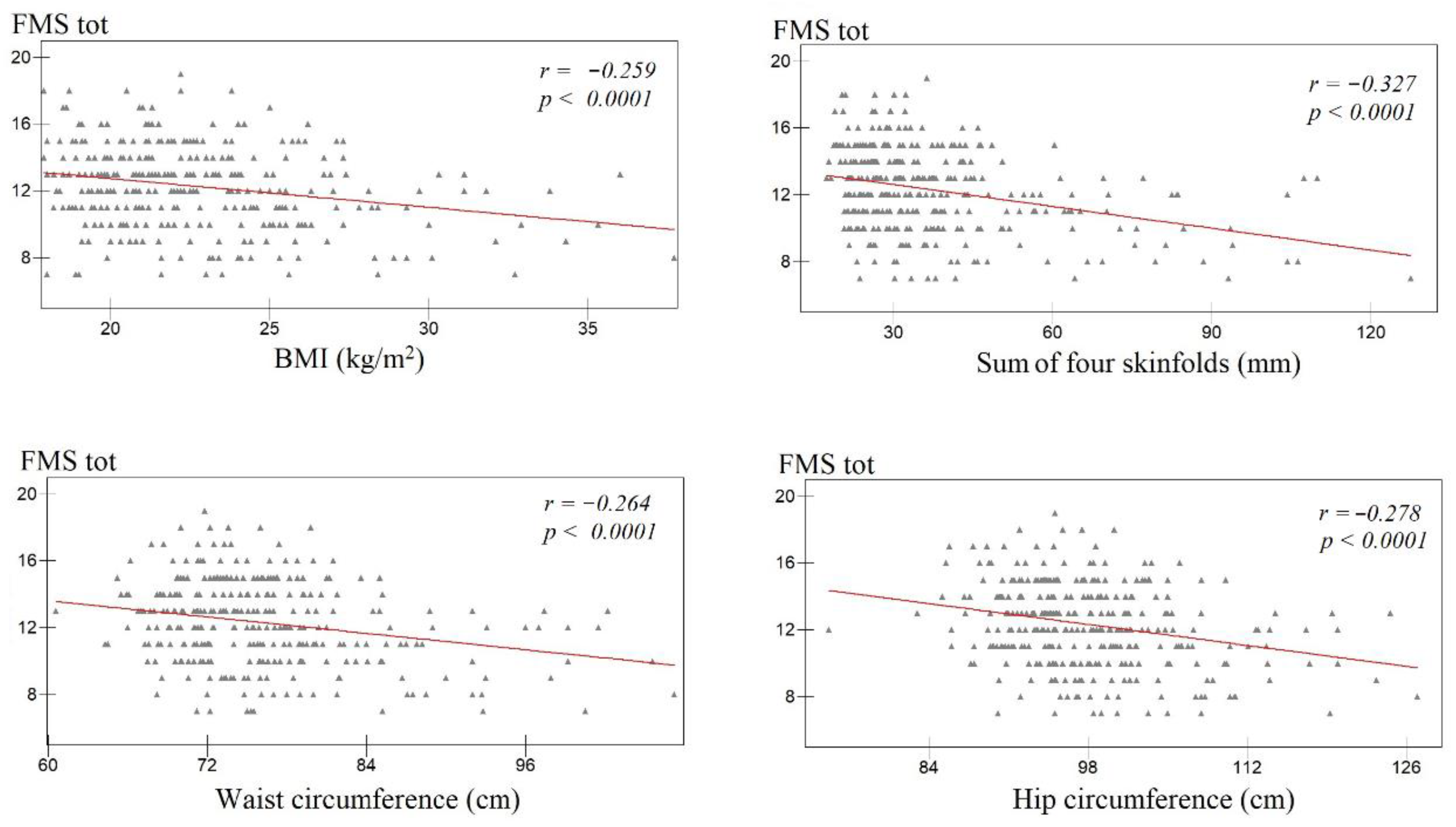
3.4.2. Association between Indicators of Adiposity and Total FMS Score among Boys
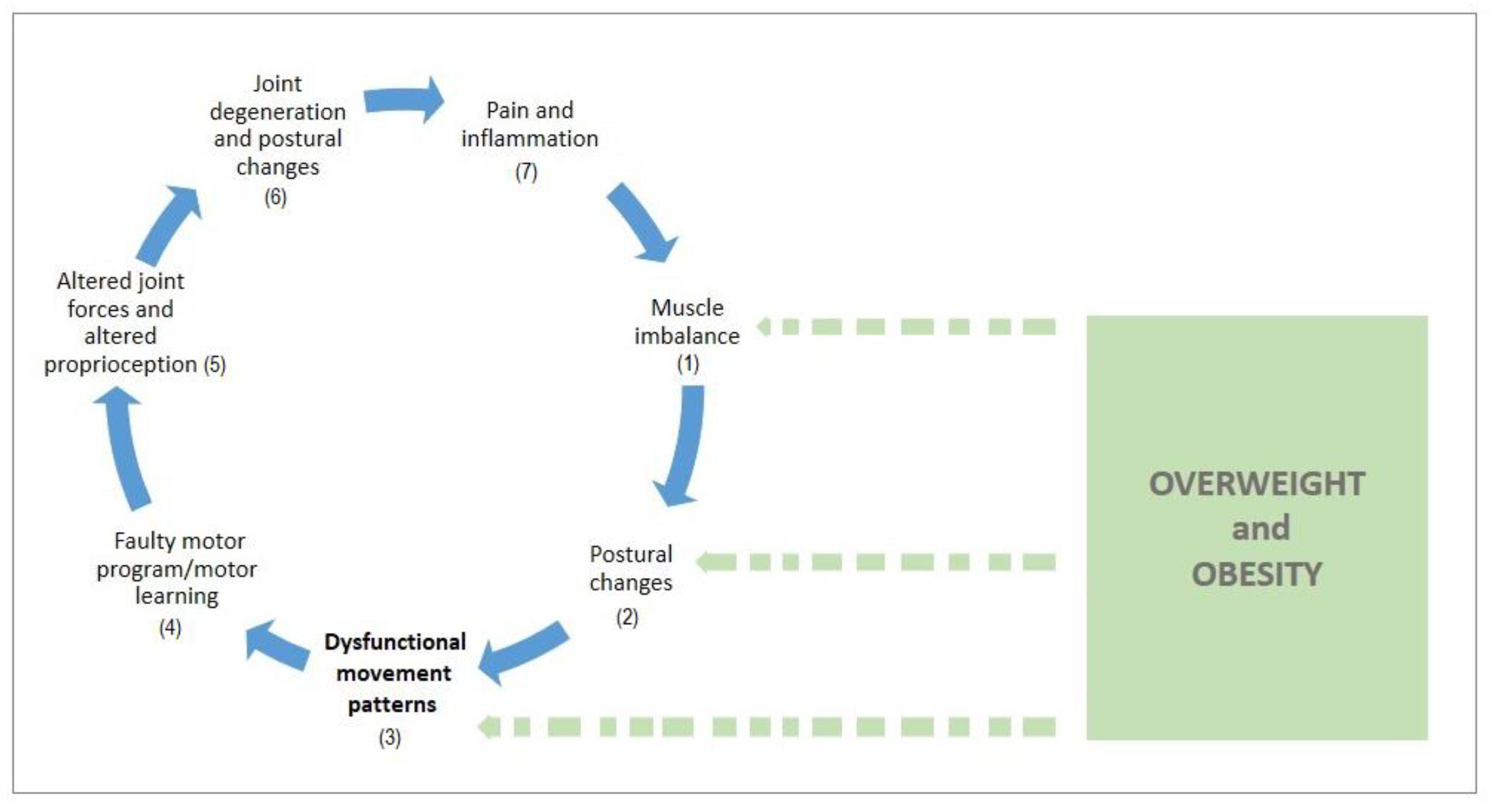
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



References
- Merder-Coşkun, D.; Uzuner, A.; Keniş-Coşkun, Ö.; Çelenlioğlu, A.E.; Akman, M.; Karadağ-Saygi, E. Relationship between obesity and musculoskeletal system findings among children and adolescents. Turk. J. Phys. Med. Rehabil. 2017, 63, 207–214. [Google Scholar] [CrossRef]
- Weihrauch-Blüher, S.; Schwarz, P.; Klusmann, J.H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metabolism 2019, 92, 147–152. [Google Scholar] [CrossRef]
- Krul, M.; Van Der Wouden, J.C.; Schellevis, F.G.; Van Suijlekom-Smit, L.W.A.; Koes, B.W. Musculoskeletal problems in overweight and obese children. Ann. Fam. Med. 2009, 7, 352–356. [Google Scholar] [CrossRef]
- Tsiros, M.D.; Tian, E.J.; Shultz, S.P.; Olds, T.; Hills, A.P.; Duff, J.; Kumar, S. Obesity, the new childhood disability? An umbrella review on the association between adiposity and physical function. Obes. Rev. 2020, 12, 26–36. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; Migueles, J.H.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Vanrenterghem, J.; Ortega, F.B. A systematic review on biomechanical characteristics of walking in children and adolescents with overweight/obesity: Possible implications for the development of musculoskeletal disorders. Obes. Rev. 2019, 20, 1033–1044. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56, S243–S255. [Google Scholar] [CrossRef]
- Rosenfeld, S.B.; Schroeder, K.; Watkins-Castillo, S.I. The Economic Burden of Musculoskeletal Disease in Children and Adolescents in the United States. J. Pediatr. Orthop. 2018, 38, e230–e236. [Google Scholar] [CrossRef]
- Kozak, A.; Schedlbauer, G.; Wirth, T.; Euler, U.; Westermann, C.; Nienhaus, A. Association between work-related biomechanical risk factors and the occurrence of carpal tunnel syndrome: An overview of systematic reviews and a meta-analysis of current research. BMC Musculoskelet. Disord. 2015, 16, 231. [Google Scholar] [CrossRef]
- Mahmoud, N.F.; Hassan, K.A.; Abdelmajeed, S.F.; Moustafa, I.M.; Silva, A.G. The Relationship between Forward Head Posture and Neck Pain: A Systematic Review and Meta-Analysis. Curr. Rev. Musculoskelet. Med. 2019, 12, 562–577. [Google Scholar] [CrossRef]
- Aderem, J.; Louw, Q.A. Biomechanical risk factors associated with iliotibial band syndrome in runners: A systematic review Rehabilitation, physical therapy and occupational health. BMC Musculoskelet. Disord. 2015, 16, 356. [Google Scholar] [CrossRef]
- Boling, M.C.; Padua, D.A.; Marshall, S.W.; Guskiewicz, K.; Pyne, S.; Beutler, A. A prospective investigation of biomechanical risk factors for Patellofemoral pain syndrome: The joint undertaking to monitor and prevent acl injury (JUMP-ACL) Cohort. Am. J. Sports Med. 2009, 37, 2108–2116. [Google Scholar] [CrossRef] [PubMed]
- Maciałczyk-Paprocka, K.; Stawińska-Witoszyńska, B.; Kotwicki, T.; Sowińska, A.; Krzyżaniak, A.; Walkowiak, J.; Krzywińska-Wiewiorowska, M. Prevalence of incorrect body posture in children and adolescents with overweight and obesity. Eur. J. Pediatr. 2017, 176, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Brzeziński, M.; Czubek, Z.; Niedzielska, A.; Jankowski, M.; Kobus, T.; Ossowski, Z. Relationship between lower-extremity defects and body mass among polish children: A cross-sectional study. BMC Musculoskelet. Disord. 2019, 20, 84. [Google Scholar] [CrossRef] [PubMed]
- Araújo, F.A.; Martins, A.; Alegrete, N.; Howe, L.D.; Lucas, R. A shared biomechanical environment for bone and posture development in children. Spine J. 2017, 17, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Lonner, B.S.; Toombs, C.S.; Husain, Q.M.; Sponseller, P.; Shufflebarger, H.; Shah, S.A.; Samdani, A.F.; Betz, R.R.; Cahill, P.J.; Yaszay, B.; et al. Body Mass Index in Adolescent Spinal Deformity: Comparison of Scheuermann’s Kyphosis, Adolescent Idiopathic Scoliosis, and Normal Controls. Spine Deform. 2015, 3, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Jankowicz-Szymańska, A.; Bibro, M.; Wodka, K.; Smola, E. Does excessive body weight change the shape of the spine in children? Child. Obes. 2019, 15, 346–352. [Google Scholar] [CrossRef]
- Catan, L.; Amaricai, E.; Onofrei, R.R.; Popoiu, C.M.; Iacob, E.R.; Stanciulescu, C.M.; Cerbu, S.; Horhat, D.I.; Suciu, O. The impact of overweight and obesity on plantar pressure in children and adolescents: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6600. [Google Scholar] [CrossRef]
- Pill, S.; Harvey, S. A Narrative Review of Children’s Movement Competence Research 1997–2017. Phys. Cult. Sport. Stud. Res. 2019, 81, 47–74. [Google Scholar] [CrossRef]
- Duncan, M.J.; Stanley, M.; Leddington Wright, S. The association between functional movement and overweight and obesity in British primary school children. Sport. Med. Arthrosc. Rehabil. Ther. Technol. 2013, 5, 11. [Google Scholar] [CrossRef]
- Duncan, M.J.; Stanley, M. Functional movement is negatively associated with weight status and positively associated with physical activity in British primary school children. J. Obes. 2012, 2012, 697563. [Google Scholar] [CrossRef]
- Ahnert, J.; Schneider, W.; Bös, K. Developmental changes and individual stability of motor abilities from the preschool period to young adulthood. In Human Development from Early Childhood to Early Adulthood: Evidence from the Munich Longitudinal Study on the Genesis of Individual Competencies (LOGIC), 1st ed.; Schneider, W., Bullock, M., Eds.; Psychology Press: New York, NY, USA, 2009; pp. 54–57. [Google Scholar]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Bernardes Marques, V.; Menezes Medeiros, T.; de Souza Stigger, F.; Yuzo Nakamura, F.; Manfredini Baroni, B. The funcional Movement Screen (FMSTM) in elite young soccer players between 14 and 20 years: Composite score, individual-test scores and asymmetries. Int. J. Sports Phys. Ther. 2017, 12, 977–985. [Google Scholar] [CrossRef]
- Kraus, K.; Schütz, E.; Taylor, W.R.; Doyscher, R. Efficacy of the functional movement screen: A review. J. Strength. Cond. Res. 2014, 28, 3571–3584. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.; Rodrigues, L.P.; Clemente, F.M.; Cancela, J.M.; Bezerra, P. Association between motor competence and functional movement screen scores. PeerJ 2019, 7, e7270. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function–Part 1. N. Am. J. Sport. Phys. Ther. 2006, 1, 62–72. [Google Scholar]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function–Part 2. N. Am. J. Sport. Phys. Ther. 2006, 1, 132–139. [Google Scholar]
- Cook, G. Movement: Functional Movement Systems: Screening, Asseessmnet and Corrective Strategies, 1st ed.; Lottus Pub: Aptos, CA, USA, 2011; pp. 31–32. [Google Scholar]
- Kiesel, K.B.; Butler, R.J.; Plisky, P.J. Prediction of Injury by Limited and Asymmetrical Fundamental Movement Patterns in American Football Players. J. Sport Rehabil. 2014, 23, 88–94. [Google Scholar] [CrossRef]
- Shojaedin, S.S.; Letafatkar, A.; Hadadnezhad, M.; Dehkhoda, M.R. Relationship between functional movement screening score and history of injury and identifying the predictive value of the FMS for injury. Int. J. Inj. Contr. Saf. Promot. 2014, 21, 355–360. [Google Scholar] [CrossRef]
- Bonazza, N.A.; Smuin, D.; Onks, C.A.; Silvis, M.L.; Dhawan, A. Reliability, Validity, and Injury Predictive Value of the Functional Movement Screen. Am. J. Sports Med. 2017, 45, 725–732. [Google Scholar] [CrossRef]
- Garrison, M.; Westrick, R.; Johnson, M.R.; Benenson, J. Association between the functional movement screen and injury development in college athletes. Int. J. Sports Phys. Ther. 2015, 10, 21–28. [Google Scholar]
- Molina-Garcia, P.; Plaza-Florido, A.; Mora-Gonzalez, J.; Torres-Lopez, L.V.; Vanrenterghem, J.; Ortega, F.B. Role of physical fitness and functional movement in the body posture of children with overweight/obesity. Gait Posture 2020, 80, 331–338. [Google Scholar] [CrossRef]
- García-Pinillos, F.; Roche-Seruendo, L.E.; Delgado-Floody, P.; Mayorga, D.J.; Latorre-Román, P.Á. Original is there any relationship between functional movement and weight status. Nutr. Hosp. 2018, 35, 805–810. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; De Bourdeaudhuij, I.; Lenoir, M. Childhood obesity affects fine motor skill performance under different postural constraints. Neurosci. Lett. 2008, 440, 72–75. [Google Scholar] [CrossRef]
- Gushue, D.L.; Houck, J.; Lerner, A.L. Effects of Childhood Obesity on Three-Dimensional Knee Joint Biomechanics during Walking. J. Pediatr. Orthop. 2005, 25, 763–768. [Google Scholar] [CrossRef]
- Widhalm, H.K.; Seemann, R.; Hamboeck, M.; Mittlboeck, M.; Neuhold, A.; Friedrich, K.; Hajdu, S.; Widhalm, K. Osteoarthritis in morbidly obese children and adolescents, an age-matched controlled study. Knee Surg. Sport. Traumatol. Arthrosc. 2016, 24, 644–652. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Quatman-Yates, C.C.; Quatman, C.E.; Meszaros, A.J.; Paterno, M.V.; Hewett, T.E. A systematic review of sensorimotor function during adolescence: A developmental stage of increased motor awkwardness? Br. J. Sports Med. 2012, 46, 649–655. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; Migueles, J.H.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Molina-Molina, A.; Garcia-Delgado, G.; D’Hondt, E.; et al. Fatness and fitness in relation to functional movement quality in overweight and obese children. J. Sports Sci. 2019, 37, 878–885. [Google Scholar] [CrossRef]
- Nicolozakes, C.P.; Schneider, D.K.; Rower, B.; Borchers, J.; Hewett, T.E. Influence of Body Composition on Functional Movement ScreenTM Scores in Collegiate Football Players. J. Sport Rehabil. 2017, 27, 431–437. [Google Scholar] [CrossRef]
- Mitchell, U.H.; Johnson, A.W.; Adamson, B. Relationship between functional movement screen scores, core strength, posture, and body mass index in school children in moldova. J. Strength Cond. Res. 2015, 29, 1172–1179. [Google Scholar] [CrossRef]
- Štefan, L.; Sorić, M.; Devrnja, A.; Podnar, H.; Mišigoj-Duraković, M. Is school type associated with objectively measured physical activity in 15-year-olds? Int. J. Environ. Res. Public Health 2017, 14, 1417. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. Br. Med. J. 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Smith, C.A.; Chimera, N.J.; Wright, N.J.; Warren, M. Interrater and intrarater reliability of the functional movement screen. J. Strength Cond. Res. 2013, 27, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.; Jull, G.; Wright, A. The effect of musculoskeletal pain on motor activity and control. J. Pain 2001, 2, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar] [PubMed]
- WHO Expert Committee on Physical Status. Physical Status: The Use and Interpretation of Anthropometry: Report of a WHO Expert Committee; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 1995; pp. 263–306. [Google Scholar]
- Wong, S.L.; Leatherdale, S.T.; Manske, S. Reliability and validity of a school-based physical activity questionnaire. Med. Sci. Sports Exerc. 2006, 38, 1593–1600. [Google Scholar] [CrossRef]
- Rasbash, J.; Steele, F.; Browne, W.J.; Goldstein, H. A User’s Guide to MLwiN; Centre for Multilevel Modelling, University of Bristol: Bristol, UK, 2019; Available online: http://www.bristol.ac.uk/cmm/ (accessed on 5 September 2020).
- Abraham, A.; Sannasi, R.; Nair, R. Normative values for the functional movement screenTM in adolescent school aged children. Int. J. Sports Phys. Ther. 2015, 10, 29–36. [Google Scholar]
- Lester, D.; McGrane, B.; Belton, S.; Duncan, M.J.; Chambers, F.C.; O’Brien, W. The Age-Related Association of Movement in Irish Adolescent Youth. Sports 2017, 5, 77. [Google Scholar] [CrossRef]
- Charlton, C.; Rasbash, J.; Browne, W.J.; Healy, M.; Cameron, B. MLwiN Version 3.04; Centre for Multilevel Modelling, University of Bristol: Bristol, UK, 2019. [Google Scholar]
- Skelly, A.; Dettori, J.; Brodt, E. Assessing bias: The importance of considering confounding. Evid. Based Spine Care J. 2012, 3, 9–12. [Google Scholar] [CrossRef]
- Bardenett, S.M.; Micca, J.J.; DeNoyelles, J.T.; Miller, S.D.; Jenk, D.T.; Brooks, G.S. Functional Movement Screen Normative Values and Validity in High School Athletes: Can the FmsTM Be Used as a Predictor of Injury? Int. J. Sports Phys. Ther. 2015, 10, 303–308. [Google Scholar]
- Portas, M.D.; Parkin, G.; Roberts, J.; Batterham, A.M. Maturational effect on Functional Movement ScreenTM score in adolescent soccer players. J. Sci. Med. Sport 2016, 19, 854–858. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.E.; Neumann, M.L.; Huxel Bliven, K.C. Functional movement screen differences between male and female secondary school athletes. J. Strength Cond. Res. 2015, 29, 1098–1106. [Google Scholar] [CrossRef] [PubMed]
- Dolphens, M.; Cagnie, B.; Vleeming, A.; Vanderstraeten, G.; Danneels, L. Gender differences in sagittal standing alignment before pubertal peak growth: The importance of subclassification and implications for spinopelvic loading. J. Anat. 2013, 223, 629–640. [Google Scholar] [CrossRef]
- Gijon-Nogueron, G.; Montes-Alguacil, J.; Martinez-Nova, A.; Alfageme-Garcia, P.; Cervera-Marin, J.A.; Morales-Asencio, J.M. Overweight, obesity and foot posture in children: A cross-sectional study. J. Paediatr. Child Health 2017, 53, 33–37. [Google Scholar] [CrossRef]
- Blimkie, C.J.R.; Sale, D.G.; Bar-Or, O. Voluntary strength, evoked twitch contractile properties and motor unit activation of knee extensors in obese and non-obese adolescent males. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 61, 313–318. [Google Scholar] [CrossRef]
- Duncan, M.J.; Bryant, E.; Stodden, D. Low fundamental movement skill proficiency is associated with high BMI and body fatness in girls but not boys aged 6–11 years old. J. Sports Sci. 2017, 35, 2135–2141. [Google Scholar] [CrossRef]
- D’Hondt, E.; Deforche, B.; De Bourdeaudhuij, I.; Lenoir, M. Relationship between motor skill and body mass index in 5- to 10-year-old children. Adapt. Phys. Act. Q. 2009, 26, 21–37. [Google Scholar] [CrossRef]
- Lopes, V.P.; Stodden, D.F.; Bianchi, M.M.; Maia, J.A.R.; Rodrigues, L.P. Correlation between BMI and motor coordination in children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Chen, X.; Dai, B. Exploratory factor analysis of the functional movement screen in elite athletes. J. Sports Sci. 2015, 33, 1166–1172. [Google Scholar] [CrossRef]
- Kazman, J.B.; Galecki, J.M.; Lisman, P.; Deuster, P.A.; O’Connor, F.G. Factor structure of the functional movement screen in marine officer candidates. J. Strength Cond. Res. 2014, 28, 672–678. [Google Scholar] [CrossRef]
- Wright, M.D.; Chesterton, P. Functional Movement Screen TM total score does not present a gestalt measure of movement quality in youth athletes. J. Sports Sci. 2019, 37, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Page, P.; Frank, C.C.; Lardner, R. Assessment and Treatment of Muscle Imbalance: The Janda Approach, 1st ed.; Human Kinetics: Champaign, IL, USA, 2010; pp. 44–46. [Google Scholar]
- Teyhen, D.S.; Shaffer, S.W.; Lorenson, C.L.; Halfpap, J.P.; Donofry, D.F.; Walker, M.J.; Dugan, J.L.; Childs, J.D. The Functional Movement Screen: A Reliability Study. J. Orthop. Sport. Phys. Ther. 2012, 42, 530–540. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Height and body-mass index trajectories of school-aged children and adolescents from 1985 to 2019 in 200 countries and territories: A pooled analysis of 2181 population-based studies with 65 million participants. Lancet 2020, 396, 1511–1524. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Characteristics | Girls (n = 321) | Boys (n = 331) |
|---|---|---|
| Age mean (SD) | 16.6 (0.4) | 16.7 (0.4) |
| OW & OB within each group n (%) | 52 (16.2) | 84 (25.4) |
| BMI (kg/m2) mean (SD) | 22.1 (3.0) | 22.6 (3.4) |
| Sum of four skinfolds (mm) mean (SD) | 49.9 (14.8) | 37.1 (17.8) |
| Waist circumference (cm) mean (SD) | 69.3 (6.2) | 76.2 (7.3) |
| Hip circumference (cm) mean (SD) | 97.5 (7.2) | 98.1 (7.3) |
| MVPA (min/day) median (IQR) | 85.7 (73.5) | 117.9 (86.3) |
| SES median (IQR) | 3 (1) | 2 (1) |
| Sex/Weight Status Group | NW | OW & OB | Within Sex Group Difference | Interaction |
|---|---|---|---|---|
| Girls | 12.8 | 12.6 | p = 1.00 | p = 1.00 1 |
| Boys | 12.6 | 11.1 | p < 0.0001 | p < 0.001 2 |
| within weight status group difference | p = 1.00 | p < 0.0001 |
| Response | Total FMS Score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | BMI | Sum of Four Skinfolds | Waist Circumference | Hip Circumference | ||||||||
| Parameter | β | S.E. | p | β | S.E. | p | β | S.E. | p | β | S.E. | p |
| Girls | −0.05 | 0.04 | 0.23 | −0.03 | 0.01 | 0.0001 | −0.04 | 0.02 | 0.06 | −0.01 | 0.02 | 0.70 |
| Boys | −0.18 | 0.04 | 0.0001 | −0.04 | 0.01 | 0.0001 | −0.08 | 0.02 | 0.0001 | −0.09 | 0.02 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karuc, J.; Marković, G.; Mišigoj-Duraković, M.; Duncan, M.J.; Sorić, M. Is Adiposity Associated with the Quality of Movement Patterns in the Mid-Adolescent Period? Int. J. Environ. Res. Public Health 2020, 17, 9230. https://doi.org/10.3390/ijerph17249230
Karuc J, Marković G, Mišigoj-Duraković M, Duncan MJ, Sorić M. Is Adiposity Associated with the Quality of Movement Patterns in the Mid-Adolescent Period? International Journal of Environmental Research and Public Health. 2020; 17(24):9230. https://doi.org/10.3390/ijerph17249230
Chicago/Turabian StyleKaruc, Josip, Goran Marković, Marjeta Mišigoj-Duraković, Michael J. Duncan, and Maroje Sorić. 2020. "Is Adiposity Associated with the Quality of Movement Patterns in the Mid-Adolescent Period?" International Journal of Environmental Research and Public Health 17, no. 24: 9230. https://doi.org/10.3390/ijerph17249230
APA StyleKaruc, J., Marković, G., Mišigoj-Duraković, M., Duncan, M. J., & Sorić, M. (2020). Is Adiposity Associated with the Quality of Movement Patterns in the Mid-Adolescent Period? International Journal of Environmental Research and Public Health, 17(24), 9230. https://doi.org/10.3390/ijerph17249230