“Cultural Security Is an On-Going Journey…” Exploring Views from Staff Members on the Quality and Cultural Security of Services for Aboriginal Families in Western Australia

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
- (1)
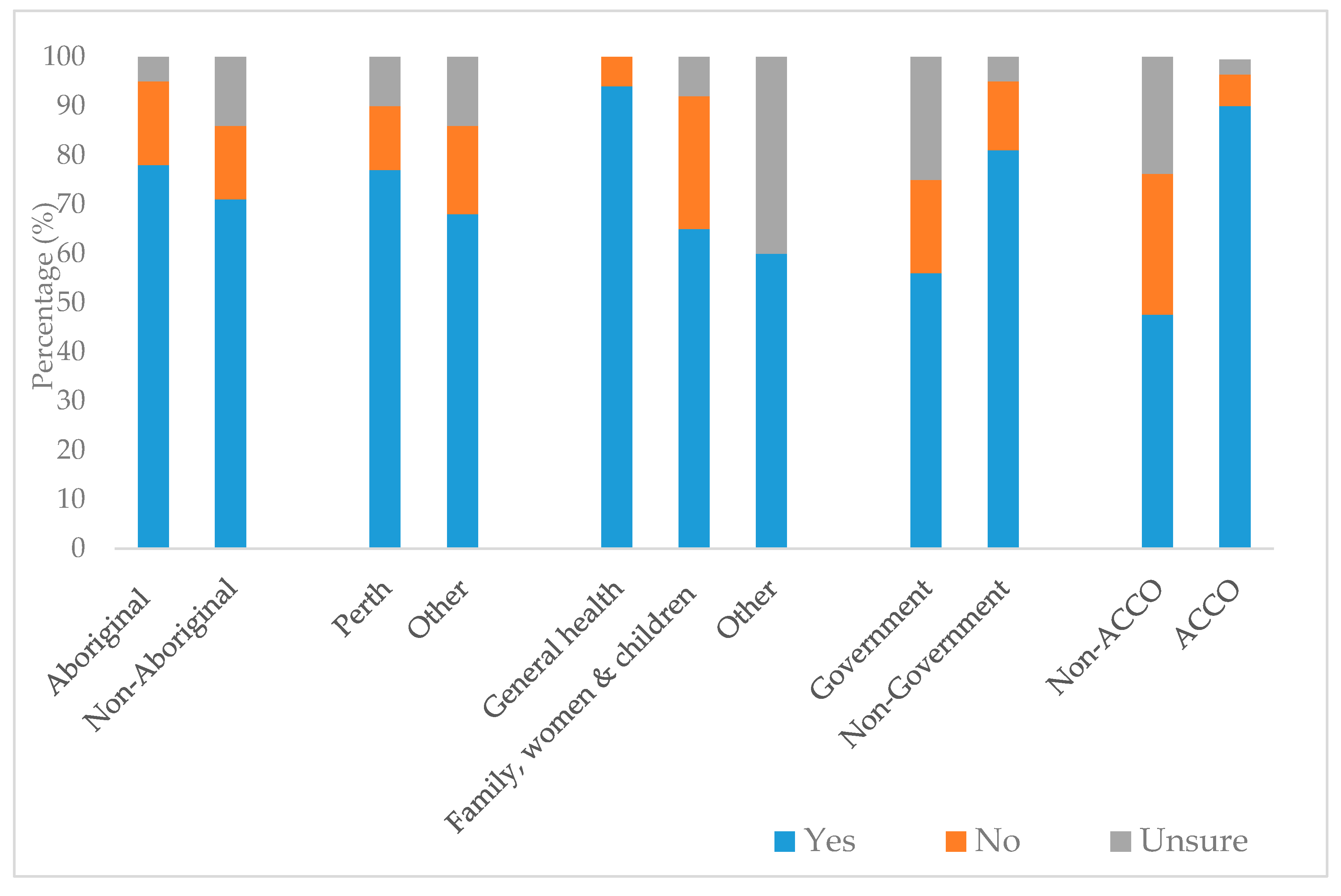
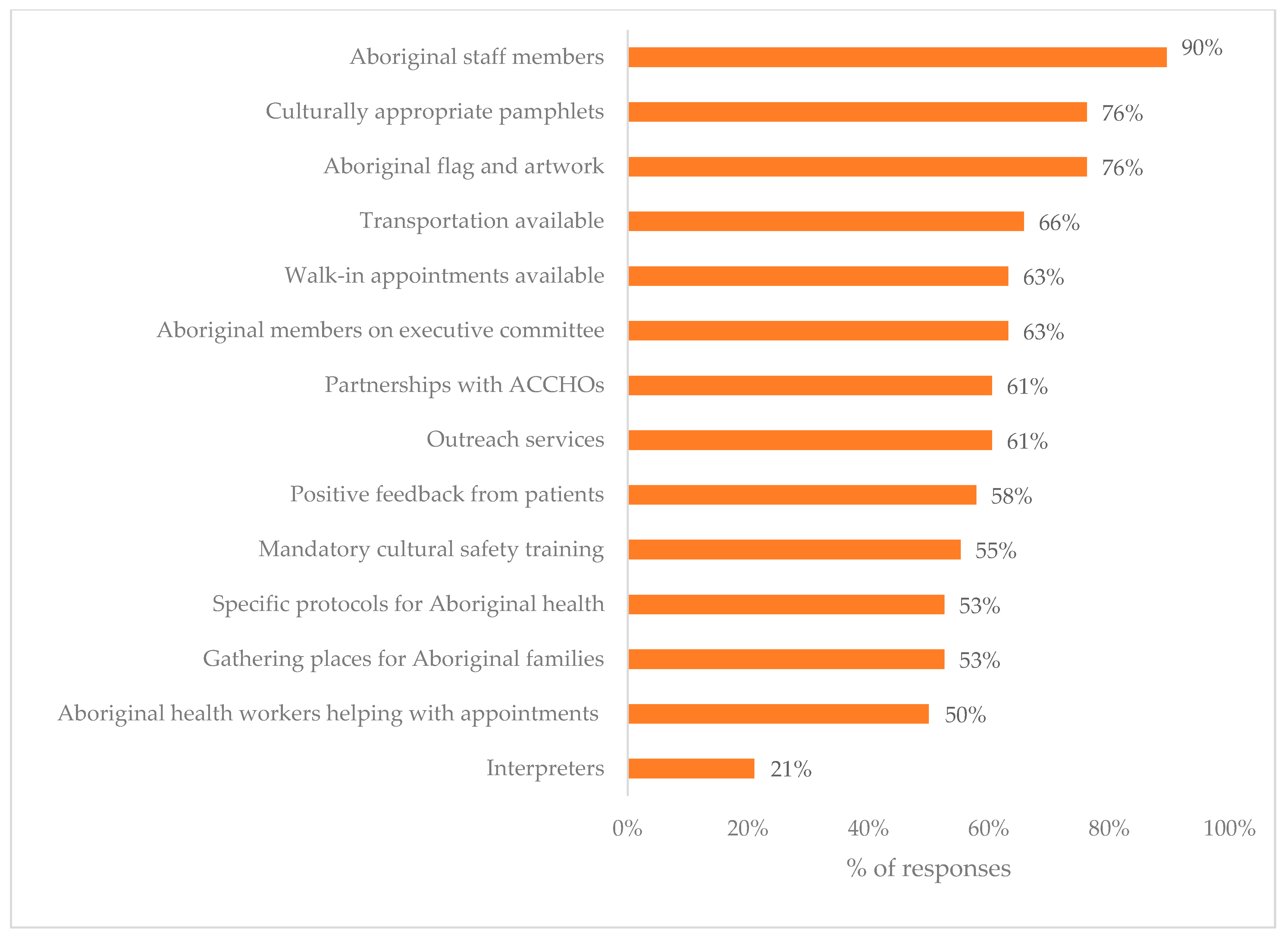
- Do you believe that this service is a culturally secure environment for Aboriginal people? If Yes, please select from the following list the reasons (multiple responses were accepted and 14 options were given to choose from). If No, how can cultural security be improved?
- (2)
- Do you believe the staff employed here have sufficient knowledge on cultural security?
- (3)
- Do you think the Aboriginal patients/clients attending this service believe it to be culturally secure?
- (4)
- Is the local Aboriginal community supportive of this service?
Data Management and Analyses
3. Results
3.1. Respondent Characteristics
3.2. Cultural Security
“Staff have technical knowledge but struggle with the context of practice, for example chasing kiddies/families a few times to attend an appt... Understanding what is normal in Aboriginal communities.”
“Cultural security is an ongoing journey and for non-Aboriginal people we can never have enough knowledge.”
3.3. Quality and Effectiveness of the Service
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gwynne, K.; Jeffries, T., Jr.; Lincoln, M.; Jeffries, T. Improving the efficacy of healthcare services for Aboriginal Australians. Aust. Health Rev. 2019, 43, 314. [Google Scholar] [CrossRef] [PubMed]
- McCormack, P.; Mohammed, F.; O’Brien, A. Learning to Work with the Community: The Development of the Wujal Wujal Guidelines for Supporting People Who are at Risk. Aborig. Isl. Health Work J. 2001, 25, 19–25. [Google Scholar]
- Coffin, J. Rising to the Challenge in Aboriginal Health by Creating Cultural Security. Aborig. Isl. Health Work J. 2007, 31, 22–24. [Google Scholar]
- Curtis, E.; Jones, R.; Tipene-Leach, D.; Walker, C.; Loring, B.; Paine, S.-J.; Reid, P. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int. J. Equity Health 2019, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Ramsden, I. Cultural Safety and Nursing Education in Aotearoa and Te Waipounamu; Victoria University: Wellington, New Zealand, 2002. [Google Scholar]
- Williamson, M.; Harrison, L. Providing culturally appropriate care: A literature review. Int. J. Nurs. Stud. 2010, 47, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Downing, R.; Kowal, E.; Paradies, Y. Indigenous cultural training for health workers in Australia. Int. J. Qual. Health Care 2011, 23, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Panaretto, K.; Lee, H.M.; En, M.R.M.; Larkins, S.L.; Manessis, V.; Buettner, P.G.; Watson, D. Impact of a collaborative shared antenatal care program for urban Indigenous women: A prospective cohort study. Med. J. Aust. 2005, 182, 514–519. [Google Scholar] [CrossRef]
- Panaretto, K.; Mitchell, M.R.; Anderson, L.; Larkins, S.L.; Manessis, V.; Buettner, P.G.; Watson, D. Sustainable antenatal care services in an urban Indigenous community: The Townsville experience. Med. J. Aust. 2007, 187, 18–22. [Google Scholar] [CrossRef]
- Reibel, T.; Walker, R. Antenatal services for Aboriginal women: The relevance of cultural competence. Qual. Prim. Care 2010, 18, 65–74. [Google Scholar]
- Kelaher, M.; Ferdinand, A.; Paradies, Y. Experiencing racism in health care: The mental health impacts for Victorian Aboriginal communities. Med. J. Aust. 2014, 201, 44–47. [Google Scholar] [CrossRef]
- Jongen, C.; McCalman, J.; Bainbridge, R. Health workforce cultural competency interventions: A systematic scoping review. BMC Health Serv. Res. 2018, 18, 232. [Google Scholar] [CrossRef] [PubMed]
- McCalman, J.; Jongen, C.; Bainbridge, R. Organisational systems’ approaches to improving cultural competence in healthcare: A systematic scoping review of the literature. Int. J. Equity Health. 2017, 16, 78. [Google Scholar] [CrossRef] [PubMed]
- McNamara, B.; Gubhaju, L.; Jorm, L.; Preen, D.; Jones, J.; Joshy, G.; Shepherd, C.; McAullay, D.; Eades, S. Exploring factors impacting early childhood health among Aboriginal and Torres Strait Islander families and communities: Protocol for a population-based cohort study using data linkage (the ‘Defying the Odds’ study). BMJ Open 2018, 8, e021236. [Google Scholar] [CrossRef] [PubMed]
- McAullay, D. Primary Health Care and Maternal, Infant and Child Health of Western Australia. Ph.D. Thesis, Australian National University, Canberra, Australia, 2010. [Google Scholar]
- Kildea, S.; Stapleton, H.; Murphy, R.; Low, N.B.; Gibbons, K. The Murri clinic: A comparative retrospective study of an antenatal clinic developed for Aboriginal and Torres Strait Islander women. BMC Pregnancy Childbirth 2012, 12, 159. [Google Scholar] [CrossRef]
- Gomersall, J.S.; Gibson, O.; Dwyer, J.; O’Donnell, K.; Stephenson, M.; Carter, D.; Canuto, K.; Munn, Z.; Aromataris, E.; Brown, A. What Indigenous Australian clients value about primary health care: A systematic review of qualitative evidence. Aust. N. Zeal. J. Public Health 2017, 41, 417–423. [Google Scholar] [CrossRef]
- Munro, A.; Allan, J.; Shakeshaft, A.; Breen, C.L. “I just feel comfortable out here, there’s something about the place”: Staff and client perceptions of a remote Australian Aboriginal drug and alcohol rehabilitation service. Subst. Abus. Treat. Prev. Policy 2017, 12, 49. [Google Scholar] [CrossRef]
- Wilson, A. Addressing Uncomfortable Issues: Reflexivity as a Tool for Culturally Safe Practice in Aboriginal and Torres Strait Islander Health. Aust. J. Indig. Educ. 2014, 43, 218–230. [Google Scholar] [CrossRef]
- Barclay, L.M.; Kruske, S.; Bar-Zeev, S.; Steenkamp, M.; Josif, C.; Narjic, C.W.; Wardaguga, M.; Belton, S.; Gao, Y.; Dunbar, T.; et al. Improving Aboriginal maternal and infant health services in the ‘Top End’ of Australia; synthesis of the findings of a health services research program aimed at engaging stakeholders, developing research capacity and embedding change. BMC Health Serv. Res. 2014, 14, 241. [Google Scholar] [CrossRef]
- Gador-Whyte, A.P.; Wakerman, J.; Campbell, D.; Lenthall, S.; Struber, J.; Hope, A.; Watson, C. Cost of best-practice primary care management of chronic disease in a remote Aboriginal community. Med. J. Aust. 2014, 200, 663–666. [Google Scholar] [CrossRef][Green Version]
- Rheault, H.; Coyer, F.; Jones, L.; Bonner, A. Health literacy in Indigenous people with chronic disease living in remote Australia. BMC Health Serv. Res. 2019, 19, 523. [Google Scholar]
- AIHW. Australia’s Health 2014; AIHW: Canberra, Australia, 2014. [Google Scholar]
- Haggerty, J.; Roberge, D.; Lévesque, J.-F.; Gauthier, J.; Loignon, C. An exploration of rural–urban differences in healthcare-seeking trajectories: Implications for measures of accessibility. Health Place 2014, 28, 92–98. [Google Scholar] [CrossRef] [PubMed]
- AIHW. Cultural Safety in Health Care: Monitoring Framework; AIHW: Canberra, Australia, 2019. [Google Scholar]



{kind=link}
{kind=link}
| Participating Services (N = 21) % (n) | Services That Did Not Participate (N = 18) % (n) | |
|---|---|---|
| Location | ||
| Perth | 52 (11) | 83 (15) |
| Goldfields/Esperance/Kalgoorlie | 29 (6) | 6 (1) |
| Great Southern | 14 (3) | 6 (1) |
| South West | 5 (1) | 6 (1) |
| Gov/Non-Gov | ||
| Government agency | 29 (6) | 28 (5) |
| Non-Government agency | 71 (15) | 72 (13) |
| Aboriginal community-controlled organisation (ACCO) | ||
| Yes | 57 (12) | 67 (12) |
| No | 43 (9) | 33 (6) |
| Main type of services provided | ||
| General health service (GP) | 24 (5) | 11 (<3) |
| Women’s, Maternal, Child health | 10 (<3) | 22 (4) |
| Family support | 38 (8) | 22 (4) |
| Alcohol/Drug | 14 (3) | 22 (4) |
| Mental health | 10 (<3) | 22 (4) |
| Legal | 5 (<3) | 0 (0) |
| % (n) | |
|---|---|
| Aboriginal and/or Torres Strait Islander | |
| Yes | 32 (19) |
| No | 68 (41) |
| Age bracket | |
| 18–24 years | 3 (<;3) |
| 25–34 years | 14 (8) |
| 35–44 years | 27 (16) |
| 45 years or over | 54 (32) |
| Highest educational qualifications | |
| Secondary—Year 12 | 15 (9) |
| Diploma—TAFE | 20 (12) |
| Undergraduate/Bachelor’s degree | 25 (15) |
| Post-graduate degree/diploma | 38 (23) |
| Aboriginal Community Controlled Organisation | |
| Yes | 53 (31) |
| No | 43 (25) |
| Staff start date at service | |
| 1999 or earlier | 15 (9) |
| 2000–2004 | 7 (4) |
| 2005–2009 | 15 (9) |
| 2010 onwards | 63 (38) |
| Position within organisation | |
| Medical professional * | 27 (16) |
| Project coordinator/project officer | 27 (16) |
| Support worker/Caregiver # | 18 (11) |
| Executive officer, Manager | 13 (8) |
| Counsellor/Mental health worker ^ | 7 (4) |
| Admin officer | 3 (<3) |
| Overall | Service Type | Location | Government | Aboriginal Community Controlled | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| General (n = 16) | Women, Maternal & Child (n = 26) | Other (n = 10) | Perth (n = 30) | Other (n = 23) | No (n = 37) | Yes (n = 16) | No (n = 22) | Yes (n = 31) | ||
| Objectives being met | 75 | 63 | 78 | 90 | 77 | 74 | 78 | 69 | 73 | 77 |
| Quality requires a great deal of improvements | 47 | 63 | 33 | 60 | 40 | 57 | 54 | 31 | 23 | 65 |
| Service is having a positive impact | 85 | 75 | 85 | 100 | 80 | 91 | 84 | 88 | 86 | 84 |
| People attending are generally happy and satisfied | 77 | 63 | 78 | 100 | 67 | 91 | 81 | 69 | 77 | 77 |
| I would recommend this service to my family and friends | 83 | 94 | 70 | 100 | 77 | 91 | 87 | 75 | 73 | 90 |
| People find it easy to get an appointment | 75 | 87 | 59 | 100 | 66 | 87 | 83 | 56 | 55 | 90 |
| Overall | Service Type | Location | Government | Aboriginal Community Controlled | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| General (n = 16) | Women, Maternal & Child (n = 26) | Other (n = 10) | Perth (n = 30) | Other (n = 23) | No (n = 37) | Yes (n = 16) | No (n = 22) | Yes (n = 31) | ||
| Staff Characteristics | ||||||||||
| Adequately trained | 65 | 75 | 69 | 40 | 67 | 64 | 69 | 56 | 71 | 61 |
| Good leaders | 62 | 56 | 69 | 50 | 63 | 59 | 61 | 63 | 71 | 55 |
| Happy and motivated | 46 | 44 | 58 | 20 | 47 | 45 | 50 | 38 | 48 | 45 |
| Number of long-term staff | 73 | 88 | 73 | 50 | 73 | 73 | 75 | 69 | 71 | 74 |
| Feel burnt out and overwhelmed | 33 | 38 | 31 | 30 | 37 | 27 | 31 | 38 | 29 | 36 |
| Sufficient staff and resources | ||||||||||
| Medical staff | 23 | 44 | 12 | 20 | 13 | 36 | 22 | 25 | 14 | 29 |
| Allied health staff | 21 | 38 | 12 | 20 | 17 | 27 | 22 | 19 | 19 | 23 |
| Admin staff | 58 | 63 | 50 | 70 | 47 | 73 | 58 | 56 | 52 | 61 |
| Aboriginal staff | 33 | 38 | 31 | 30 | 33 | 32 | 33 | 31 | 19 | 42 |
| Funding to improve care | 46 | 63 | 50 | 10 | 57 | 32 | 53 | 31 | 29 | 58 |
| Funding for equipment & consumables | 33 | 45 | 24 | 38 | 20 | 50 | 35 | 30 | 47 | 24 |
| Space to treat patients | 27 | 44 | 19 | 20 | 23 | 32 | 22 | 38 | 19 | 32 |
| Patient characteristics | ||||||||||
| Attend scheduled appointments | 12 | 13 | 12 | 10 | 13 | 9 | 14 | 6 | 10 | 13 |
| Have knowledge/skills to follow treatment plans | 17 | 13 | 27 | 0 | 30 | 0 | 14 | 25 | 24 | 13 |
| Have sufficient money for appointments/buy medicine | 8 | 13 | 4 | 10 | 10 | 5 | 3 | 19 | 10 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gubhaju, L.; Williams, R.; Jones, J.; Hamer, D.; Shepherd, C.; McAullay, D.; Eades, S.J.; McNamara, B. “Cultural Security Is an On-Going Journey…” Exploring Views from Staff Members on the Quality and Cultural Security of Services for Aboriginal Families in Western Australia. Int. J. Environ. Res. Public Health 2020, 17, 8480. https://doi.org/10.3390/ijerph17228480
Gubhaju L, Williams R, Jones J, Hamer D, Shepherd C, McAullay D, Eades SJ, McNamara B. “Cultural Security Is an On-Going Journey…” Exploring Views from Staff Members on the Quality and Cultural Security of Services for Aboriginal Families in Western Australia. International Journal of Environmental Research and Public Health. 2020; 17(22):8480. https://doi.org/10.3390/ijerph17228480
Chicago/Turabian StyleGubhaju, Lina, Robyn Williams, Jocelyn Jones, David Hamer, Carrington Shepherd, Dan McAullay, Sandra J. Eades, and Bridgette McNamara. 2020. "“Cultural Security Is an On-Going Journey…” Exploring Views from Staff Members on the Quality and Cultural Security of Services for Aboriginal Families in Western Australia" International Journal of Environmental Research and Public Health 17, no. 22: 8480. https://doi.org/10.3390/ijerph17228480
APA StyleGubhaju, L., Williams, R., Jones, J., Hamer, D., Shepherd, C., McAullay, D., Eades, S. J., & McNamara, B. (2020). “Cultural Security Is an On-Going Journey…” Exploring Views from Staff Members on the Quality and Cultural Security of Services for Aboriginal Families in Western Australia. International Journal of Environmental Research and Public Health, 17(22), 8480. https://doi.org/10.3390/ijerph17228480