Influence of Living Alone or with a Spouse Only on the Short-Term Prognosis in Patients after an Acute Ischemic Stroke


Abstract
1. Introduction
2. Materials and Methods
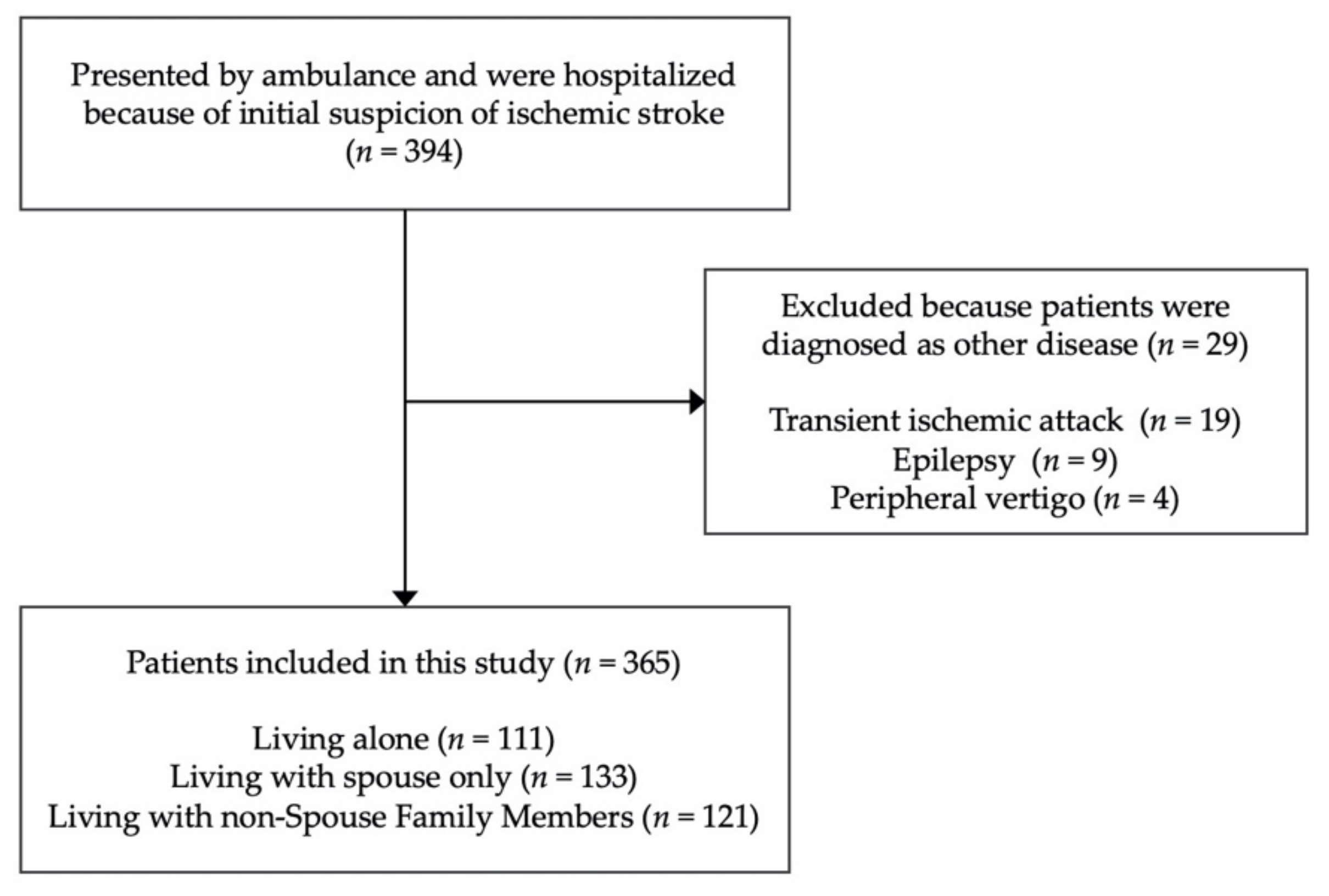
2.1. Design and Overview
2.2. Cohabiting Family Members
2.3. Covariate Assessment
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Differences in the Time from the Stroke Onset to Arriving at the Hospital
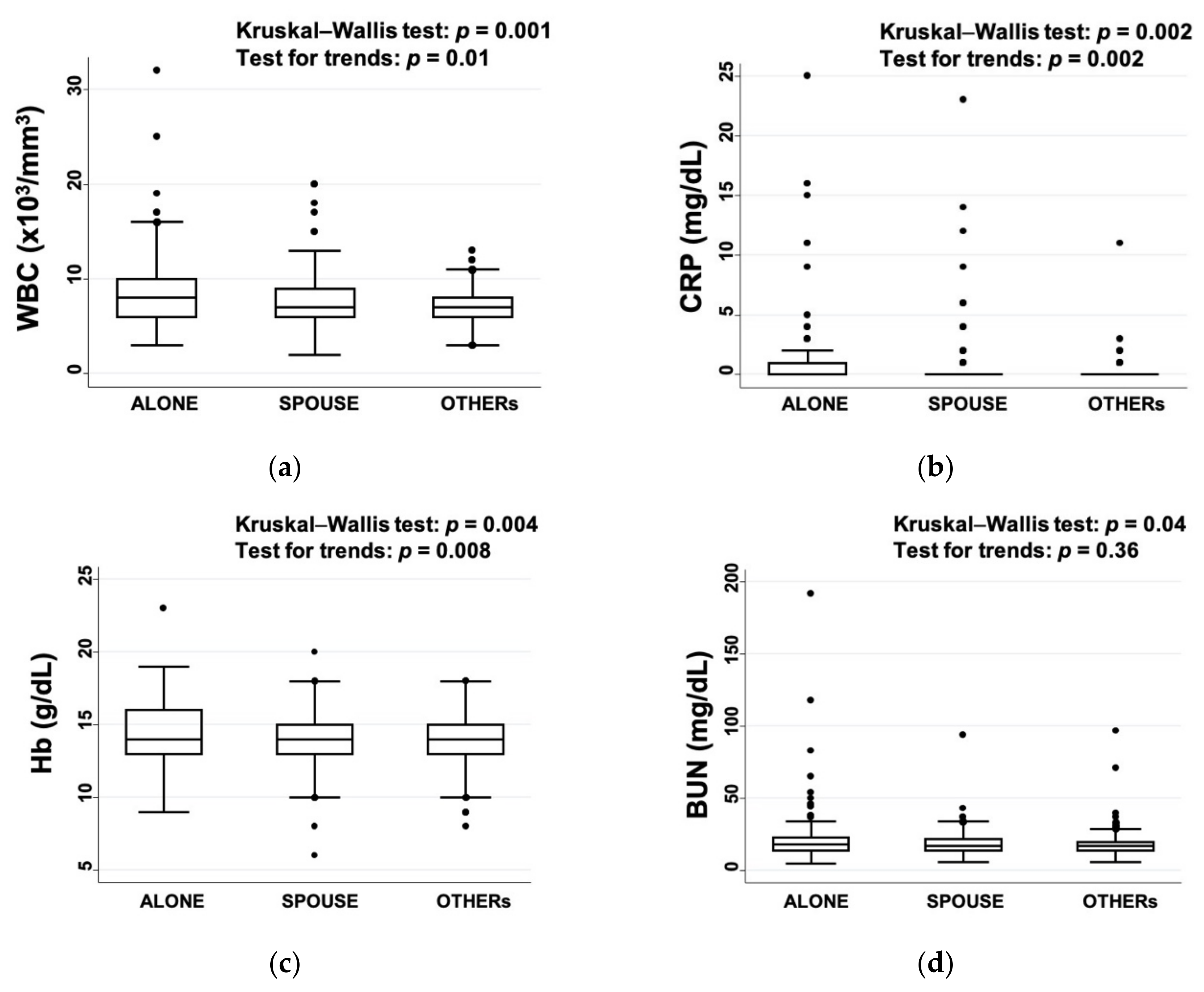
3.3. Differences in the Laboratory Data at Admission
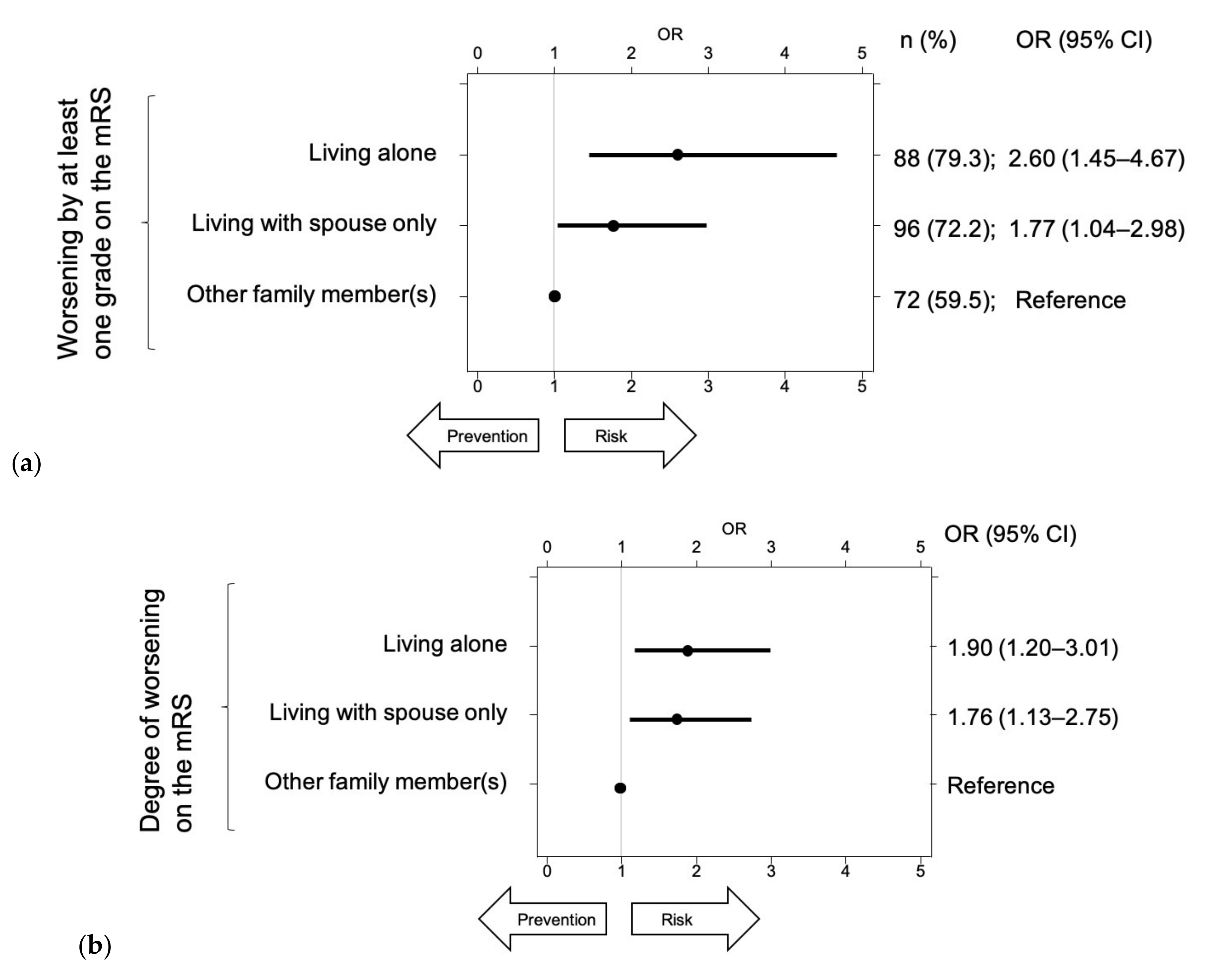
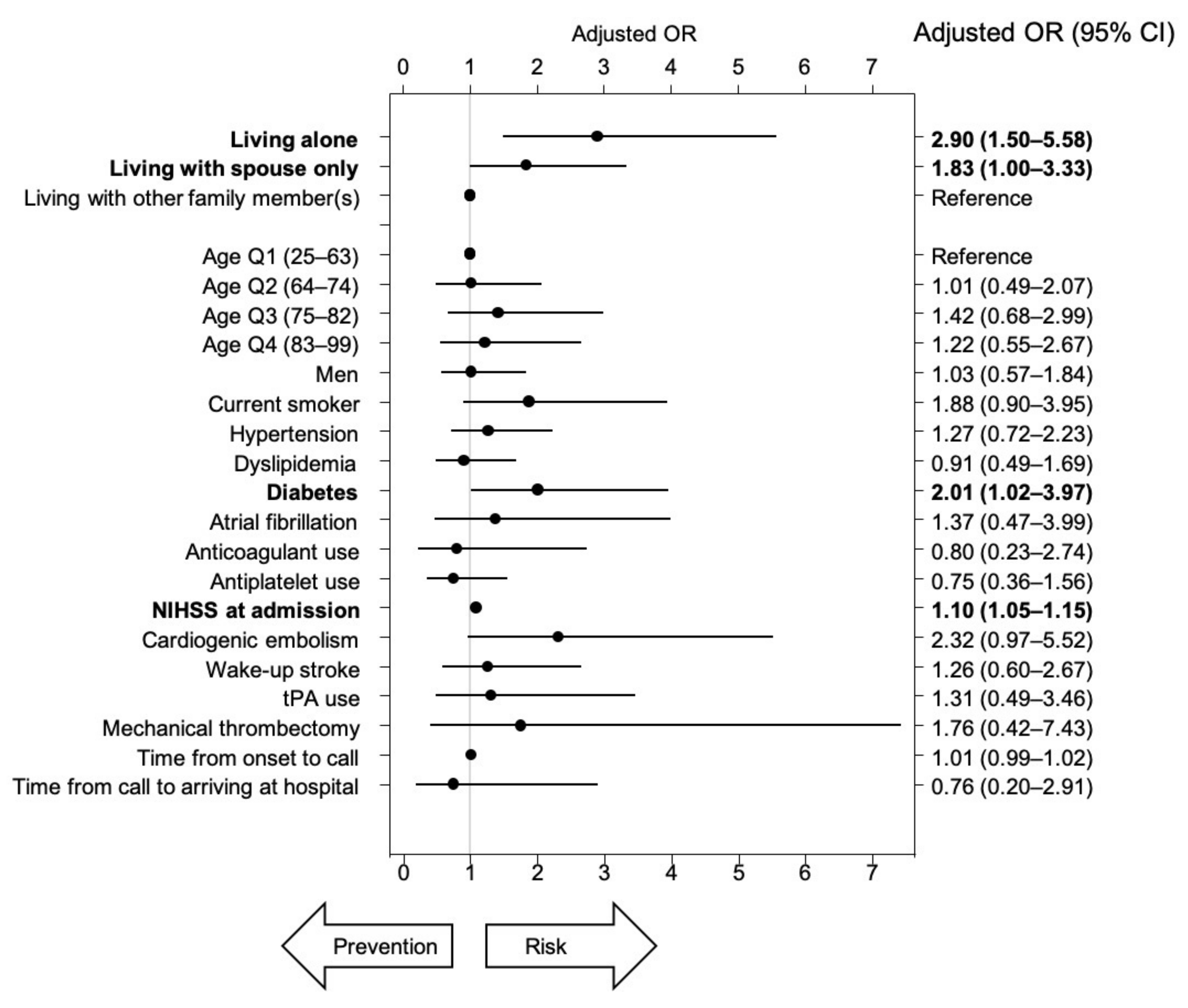
3.4. Risk of Worsening by at Least One Grade on the mRS
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cesaroni, G.; Agabiti, N.; Forastiere, F.; Perucci, C.A. Socioeconomic differences in stroke incidence and prognosis under a universal healthcare system. Stroke 2009, 40, 2812–2819. [Google Scholar] [CrossRef]
- Marshall, I.J.; Wang, Y.; Crichton, S.; McKevitt, C.; Rudd, A.G.; Wolfe, C.D.A. The effects of socioeconomic status on stroke risk and outcomes. Lancet Neurol. 2015, 14, 1206–1218. [Google Scholar] [CrossRef]
- Takashima, N.; Arima, H.; Kita, Y.; Fujii, T.; Miyamatsu, N.; Komori, M.; Sugimoto, Y.; Nagata, S.; Miura, K.; Nozaki, K. Two-year survival after first-ever stroke in a general population of 1.4 million Japanese: Shiga stroke registry. Circ. J. 2018, 82, 2549–2556. [Google Scholar] [CrossRef]
- Kato, Y.; Hayashi, T.; Tanahashi, N.; Kobayashi, S. Cardioembolic stroke is the most serious problem in the aging society: Japan standard stroke registry study. J. Stroke Cerebrovasc. Dis. 2015, 24, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Japan Ministry of Health Labour and Welfare. 2018 Annual Health, Labour and Welfare Report 2018. Available online: https://www.mhlw.go.jp/english/wp/wp-hw12/index.html (accessed on 25 October 2020).
- Japan Cabinet Office. 2020 Annual Report on the Aging Society. Available online: https://www8.cao.go.jp/kourei/english/annualreport/index-wh.html (accessed on 25 October 2020).
- Van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.A.; Van Gijn, J. Interobserver Agreement for the Assessment of Handicap in Stroke Patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Cuzick, J. A wilcoxon-type test for trend. Stat. Med. 1985, 4, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Redfors, P.; Isaksén, D.; Lappas, G.; Blomstrand, C.; Rosengren, A.; Jood, K.; Jern, C. Living alone predicts mortality in patients with ischemic stroke before 70 years of age: A long-term prospective follow-up study. BMC Neurol. 2016, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Börü, U.T.; Oztürk, E.; Taşdemir, M.; Sur, H. Living alone following first-ever stroke: A prospective study in Turkey identifying the risk factors and evaluating their effects. N. Z. Med. J. 2007, 120, U2559. [Google Scholar] [PubMed]
- Reeves, M.J.; Prager, M.; Fang, J.; Stamplecoski, M.; Kapral, M.K. Impact of living alone on the care and outcomes of patients with acute stroke. Stroke 2014, 45, 3083–3085. [Google Scholar] [CrossRef] [PubMed]
- Dhand, A.; Luke, D.; Lang, C.; Tsiaklides, M.; Feske, S.; Lee, J.-M. Social networks and risk of delayed hospital arrival after acute stroke. Nat. Commun. 2019, 10, 1206. [Google Scholar] [CrossRef] [PubMed]
- Houde, S.C.; Gautam, R.; Kai, I. Long-term care insurance in Japan: Implications for U.S. long-term care policy. J. Gerontol. Nurs. 2007, 33, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Vangilder, R.L.; Davidov, D.M.; Stinehart, K.R.; Huber, J.D.; Turner, R.C.; Wilson, K.S.; Haney, E.; Davis, S.M.; Chantler, P.D.; Theeke, L.; et al. C-reactive protein and long-term ischemic stroke prognosis. J. Clin. Neurosci. 2014, 21, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Nelson-Coffey, S.K.; Fritz, M.M.; Lyubomirsky, S.; Cole, S.W. Kindness in the blood: A randomized controlled trial of the gene regulatory impact of prosocial behavior. Psychoneuroendocrinology 2017, 81, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Kim, B.J.; Kim, J.S.; Yang, M.H.; Jang, M.S.; Kim, N.; Han, M.K.; Lee, J.S.; Lee, J.; Kim, S.Y.; et al. Impact of both ends of the hemoglobin range on clinical outcomes in acute ischemic stroke. Stroke 2013, 44, 3220–3222. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Living Alone | Living with Spouse Only | Living with Non-Spouse Family Members | p-Value |
|---|---|---|---|---|---|
| n = 365 | n = 111 | n = 133 | n = 121 | ||
| Age, median (IQR) 1 | 74 (63–82) | 73 (64–84) | 74 (63–81) | 76 (61–83) | 0.786 |
| Male, n (%) 2 | 238 (65.2) | 69 (62.2) | 104 (78.2) | 65 (53.7) | <0.001 |
| mRS score before onset, n (%) 1 | 0.044 | ||||
| 0 | 307 (84.1) | 92 (82.9) | 120 (90.2) | 95 (78.5) | |
| 1 | 14 (3.8) | 4 (3.6) | 6 (4.5) | 4 (3.3) | |
| 2 | 13 (3.6) | 7 (6.3) | 3 (2.3) | 3 (2.5) | |
| 3 | 9 (2.5) | 3 (2.7) | 2 (1.5) | 4 (3.3) | |
| 4 | 13 (3.6) | 3 (2.7) | 1 (0.7) | 9 (7.4) | |
| 5 | 9 (2.5) | 9 (2.5) | 1 (0.7) | 6 (5.0) | |
| Hypertension (%) 2 | 207 (56.7) | 60 (54.1) | 84 (63.2) | 63 (52.1) | 0.162 |
| Diabetes (%) 2 | 81 (22.2) | 24 (21.6) | 30 (22.6) | 27 (22.3) | 0.984 |
| Atrial fibrillation (%) 2 | 57 (15.6) | 23 (20.7) | 16 (12.0) | 18 (14.9) | 0.170 |
| Current smoking (%) 2 | 62 (17.0) | 24 (21.6) | 22 (16.5) | 16 (13.2) | 0.232 |
| Creatinine (μmol/L), median (IQR) 1 | 69 (58–87) | 69 (58–90) | 70 (59–88) | 68 (55–83) | 0.559 |
| Albumin (g/dL), median (IQR) 1 | 4 (4–4) | 4 (4–4) | 4 (4–4) | 4 (4–4) | 0.214 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, Y.; Hifumi, T.; Urashima, M. Influence of Living Alone or with a Spouse Only on the Short-Term Prognosis in Patients after an Acute Ischemic Stroke. Int. J. Environ. Res. Public Health 2020, 17, 8223. https://doi.org/10.3390/ijerph17218223
Ishikawa Y, Hifumi T, Urashima M. Influence of Living Alone or with a Spouse Only on the Short-Term Prognosis in Patients after an Acute Ischemic Stroke. International Journal of Environmental Research and Public Health. 2020; 17(21):8223. https://doi.org/10.3390/ijerph17218223
Chicago/Turabian StyleIshikawa, Yohei, Toru Hifumi, and Mitsuyoshi Urashima. 2020. "Influence of Living Alone or with a Spouse Only on the Short-Term Prognosis in Patients after an Acute Ischemic Stroke" International Journal of Environmental Research and Public Health 17, no. 21: 8223. https://doi.org/10.3390/ijerph17218223
APA StyleIshikawa, Y., Hifumi, T., & Urashima, M. (2020). Influence of Living Alone or with a Spouse Only on the Short-Term Prognosis in Patients after an Acute Ischemic Stroke. International Journal of Environmental Research and Public Health, 17(21), 8223. https://doi.org/10.3390/ijerph17218223