Generic Health Literacy Measurements for Adults: A Scoping Review

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
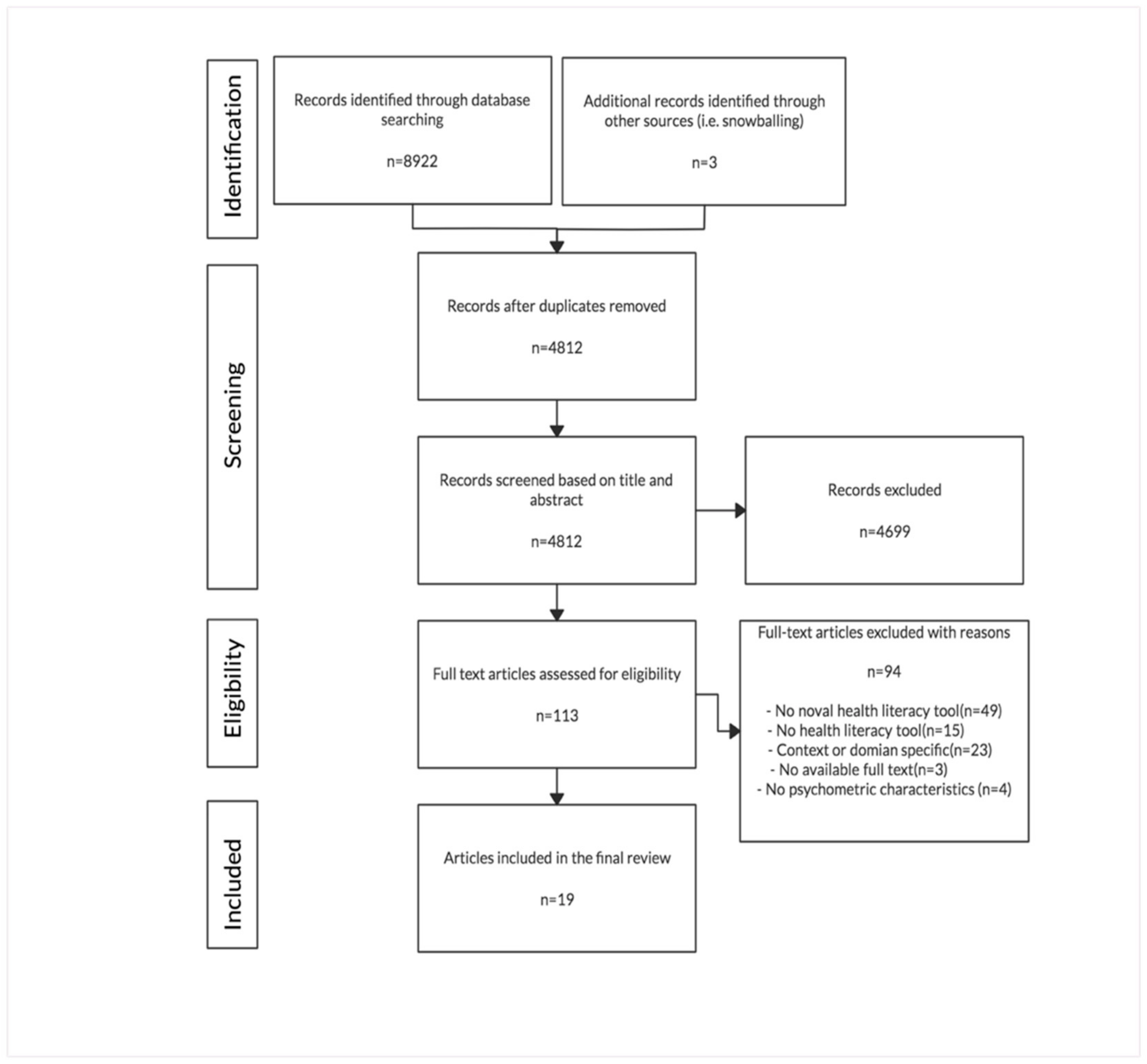
2.3. Study Selection
2.4. Data Charting and Collation
3. Results
3.1. Instrument Characteristics
3.2. Underlying Definition and Models
3.2.1. Measurements Summarized under Nutbeam’s Conceptual Model
3.2.2. Measurements Summarized under the Sørensen’s Integrated Model
3.2.3. Measurements Summarized under the Other Models
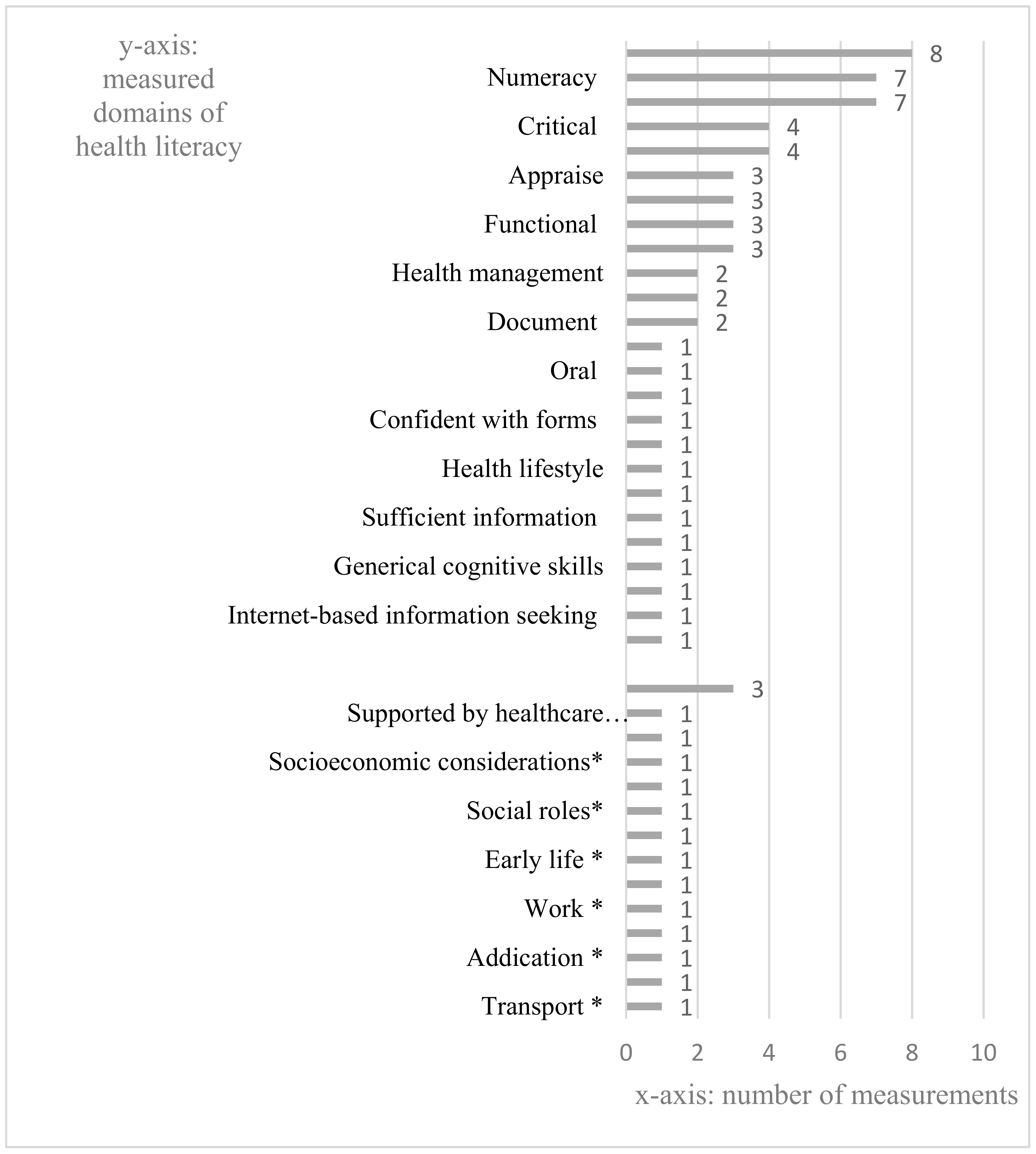
3.3. Measured Domains of Health Literacy
3.4. Adopted Approaches of Instruments
4. Discussion
4.1. Importance of Social Determinants of Health to Health Literacy
4.2. Theoretical Foundation of Social Determinants of Health Literacy
4.3. Role of Social Determinants on the Constructs of Health Literacy
4.4. Representative Social Determinants of Health Literacy
4.5. Adopted Approaches
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Nutbeam, D. Health promotion glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- American Medical Association. Health literacy: Report of the council on scientific affairs. JAMA 1999, 281, 552–557. [Google Scholar] [CrossRef]
- Kindig, D.A.; Panzer, A.M.; Nielsen-Bohlman, L. Health Literacy: A Prescription to End Confusion; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Scott, T.L.; Gazmararian, J.A.; Williams, M.V.; Baker, D.W. Health literacy and preventive health care use among medicare enrollees in a managed care organization. Med. Care 2002, 40, 395–404. [Google Scholar] [CrossRef]
- Baker, D.W.; Parker, R.M.; Williams, M.V.; Clark, W.S. Health literacy and the risk of hospital admission. J. Gen. Intern. Med. 1998, 13, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.W.; Gazmararian, J.A.; Williams, M.V.; Scott, T.; Parker, R.M.; Green, D.; Ren, J.; Peel, J. Functional health literacy and the risk of hospital admission among Medicare managed care enrollees. Am. J. Public Health 2002, 92, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Mäenpää, T.; Suominen, T.; Asikainen, P.; Maass, M.; Rostila, I. The outcomes of regional healthcare information systems in health care: A review of the research literature. Int. J. Med. Inform. 2009, 78, 757–771. [Google Scholar] [CrossRef]
- Sun, X.; Shi, Y.; Zeng, Q.; Wang, Y.; Du, W.; Wei, N.; Xie, R.; Chang, C. Determinants of health literacy and health behavior regarding infectious respiratory diseases: A pathway model. BMC Public Health 2013, 13, 261. [Google Scholar] [CrossRef]
- Batterham, R.W.; Hawkins, M.; Collins, P.; Buchbinder, R.; Osborne, R.H. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health 2016, 132, 3–12. [Google Scholar] [CrossRef]
- U.S. Department of Education. The Health Literacy of America’s Adults Results From the 2003 National Assessment of Adult Literacy; U.S. Department of Education: Washington, DC, USA, 2006.
- Murray, T.; Hagey, J.; Willms, D.; Shillington, R.; Desjardins, R. Health Literacy in Canada: A Healthy Understanding; UCLA: Los Angeles, CA, USA, 2008. [Google Scholar]
- Statistics, A.B.O. Health Literacy, Australia. 2006. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Latestproducts/4233.0Main%20Features22006 (accessed on 5 May 2020).
- Ying-Hua, L. Introduction of 2012 Chinese residents health literacy monitoring program. Chin. J. Health Educ. 2014, 6, 563–565. [Google Scholar]
- Altin, S.V.; Finke, I.; Kautz-Freimuth, S.; Stock, S. The evolution of health literacy assessment tools: A systematic review. BMC Public Health 2014, 14, 1207. [Google Scholar] [CrossRef]
- Liu, H.; Shen, Y.; Zhang, F.; Sharma, M.; Lai, W.; Zhao, Y.; Tao, G.; Yuan, J.; Zhao, Y. Assessment tools for health literacy among the general population: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 1711. [Google Scholar] [CrossRef] [PubMed]
- Haun, J.N.; Valerio, M.A.; McCormack, L.A.; Sørensen, K.; Paasche-Orlow, M.K. Health literacy measurement: An inventory and descriptive summary of 51 instruments. J. Health Commun. 2014, 19, 302–333. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef]
- Bröder, J.; Kickbusch, I.; Levin-Zamir, D.; McElhinney, E.; Nutbeam, D.; Okan, O.; Osborne, R.; Pelikan, J.; Rootman, I. IUHPE position statement on health literacy: A practical vision for a health literate world. Glob. Health Promot. 2018, 25, 79–88. [Google Scholar] [CrossRef]
- Pleasant, A.; McKinney, J.; Rikard, R.V. Health literacy measurement: A proposed research agenda. J. Health Commun. 2011, 16, 11–21. [Google Scholar] [CrossRef]
- Marmot, M.; Wilkinson, R. Social Determinants of Health; OUP Oxford: Oxford, UK, 2005. [Google Scholar]
- Garcia-Codina, O.; Juvinyà-Canal, D.; Amil-Bujan, P.; Bertran-Noguer, C.; González-Mestre, M.A.; Masachs-Fatjo, E.; Santaeugènia, S.J.; Magrinyà-Rull, P.; Saltó-Cerezuela, E. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health 2019, 19, 1122. [Google Scholar] [CrossRef]
- Rowlands, G.; Shaw, A.; Jaswal, S.; Smith, S.; Harpham, T. Health literacy and the social determinants of health: A qualitative model from adult learners. Health Promot. Int. 2017, 32, 130–138. [Google Scholar] [CrossRef]
- Pleasant, A.; McKinney, J. Coming to consensus on health literacy measurement: An online discussion and consensus-gauging process. Nurs. Outlook 2011, 59, 95–106. [Google Scholar] [CrossRef]
- Pleasant, A.; Maish, C.; O’Leary, C.; Carmona, R. Measuring health literacy in adults: An overview and discussion of current tools. In International Handbook of Health Literacy; Policy Press: Bristol, UK, 2019. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Murphy, P.W.; Davis, T.C.; Long, S.W.; Jackson, R.H.; Decker, B.C. Rapid estimate of adult literacy in medicine (REALM): A quick reading test for patients. J. Read. 1993, 37, 124–130. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Haynes, S.N.; Richard, D.; Kubany, E.S. Content validity in psychological assessment: A functional approach to concepts and methods. Psychol. Assess. 1995, 7, 238. [Google Scholar] [CrossRef]
- Hauser, R.M.; Edley, C.F.; Koenig, J.A.; Elliott, S.W. Measuring Literacy: Performance Levels for Adults; ERIC; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The health literacy skills framework. J. Health Commun. 2012, 17, 30–54. [Google Scholar] [CrossRef]
- Parker, R.M.; Baker, D.W.; Williams, M.V.; Nurss, J.R. The test of functional health literacy in adults: A new instrument for measuring patients’ literacy skills. J. Gen. Intern. Med. 1995, 10, 537–541. [Google Scholar] [CrossRef]
- Chew, L.D.; Bradley, K.; Boyko, E.J. Brief questions to identify patients with inadequate health literacy. Health 2004, 11, 12. [Google Scholar]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef]
- Pleasant, A.; Kuruvilla, S. A tale of two health literacies: Public health and clinical approaches to health literacy. Health Promot. Int. 2008, 23, 152–159. [Google Scholar] [CrossRef]
- McCormack, L.; Bann, C.; Squiers, L.; Berkman, N.D.; Squire, C.; Schillinger, D.; Ohene-Frempong, J.; Hibbard, J. Measuring health literacy: A pilot study of a new skills-based instrument. J. Health Commun. 2010, 15 (Suppl. 2), 51–71. [Google Scholar] [CrossRef]
- Wang, J.; Thombs, B.D.; Schmid, M.R. The Swiss Health Literacy Survey: Development and psychometric properties of a multidimensional instrument to assess competencies for health. Health Expect. 2014, 17, 396–417. [Google Scholar] [CrossRef] [PubMed]
- Chinn, D.; McCarthy, C. All Aspects of Health Literacy Scale (AAHLS): Developing a tool to measure functional, communicative and critical health literacy in primary healthcare settings. Patient Educ. Couns. 2013, 90, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.E.; Buchbinder, R.; Briggs, A.M.; Elsworth, G.R.; Busija, L.; Batterham, R.; Osborne, R.H. The health literacy management scale (HeLMS): A measure of an individual’s capacity to seek, understand and use health information within the healthcare setting. Patient Educ. Couns. 2013, 91, 228–235. [Google Scholar] [CrossRef]
- Osborne, R.H.; Batterham, R.W.; Elsworth, G.R.; Hawkins, M.; Buchbinder, R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658. [Google Scholar] [CrossRef]
- Sorensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H.; et al. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.J.; Lee, T.W.; Paasche-Orlow, M.K.; Kim, G.S.; Won, H.K. Development and evaluation of the Korean Health Literacy Instrument. J. Health Commun. 2014, 19 (Suppl. 2), 254–266. [Google Scholar] [CrossRef]
- Nakagami, K.; Revelle, W.; Waite, K.; Wilson, E.A.H.; Condon, D.M.; Bojarski, E.; Park, D.C.; Baker, D.W.; Wolf, M.S. Development and validation of a new instrument for testing functional health literacy in Japanese adults. Nurs. Health Sci. 2014, 16, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.M.; Revelle, W.; Waite, K.; Wilson, E.A.H.; Condon, D.M.; Bojarski, E.; Park, D.C.; Baker, D.W.; Wolf, M.S. Development and validation of the comprehensive health activities scale: A new approach to health literacy measurement. J. Health Commun. 2015, 20, 157–164. [Google Scholar] [CrossRef]
- Matsumoto, M.; Nakayama, K. Development of the health literacy on social determinants of health questionnaire in Japanese adults. BMC Public Health 2017, 17, 30. [Google Scholar] [CrossRef]
- Lee, T.W.; Kang, S.J.; Lee, H.J.; Hyun, S.I. Testing health literacy skills in older Korean adults. Patient Educ. Couns. 2009, 75, 302–307. [Google Scholar] [CrossRef]
- Tsai, T.I.; Lee, S.Y.; Tsai, Y.W.; Kuo, K.N. Methodology and validation of health literacy scale development in Taiwan. J. Health Commun. 2011, 16, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.H.; Chen, L.K.; Peng, L.N.; Chi, M.J. Development and validation of the health literacy assessment tool for older people in Taiwan: Potential impacts of cultural differences. Arch. Gerontol. Geriatr. 2015, 61, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Haghdoost, A.A.; Rakhshani, F.; Aarabi, M.; Montazeri, A.; Tavousi, M.; Solimanian, A.; Sarbandi, F.; Namdar, H.; Iranpour, A. Iranian health literacy questionnaire (IHLQ): An instrument for measuring health literacy in Iran. Iran. Red Crescent Med. J. 2015, 17. [Google Scholar] [CrossRef]
- Intarakamhang, U.; Kwanchuen, Y. The development and application of the ABCDE-health literacy scale for Thais. Asian Biomed. 2016, 10, 587–594. [Google Scholar]
- Ratzan, S.; Parker, R.; Selden, C.; Zorn, M. National Library of Medicine Current Bibliographies in Medicine: Health literacy; National Institutes of Health, US Department of Health and Human Services: Bethesda, MD, USA, 2000.
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef]
- WHO. Social Determinants of Health: The Solid Facts; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Pinheiro, P. Future avenues for health literacy: Learning from literacy and literacy learning. In International Handbook of Health Literacy; Policy Press: Bristol, UK, 2019. [Google Scholar]
- Bitzer, E.M.; Nicole, E. Proposal for an Expanded Definition of Health Literacy. 2019. Available online: https://dngk.de/gesundheitskompetenz/definition-health-literacy-august-2019/ (accessed on 5 May 2020).
- Sentell, T.; Pitt, R.; Buchthal, O.V. Health literacy in a social context: Review of quantitative evidence. HLRP Health Lit. Res. Pract. 2017, 1, e41–e70. [Google Scholar] [CrossRef] [PubMed]
- Okan, O.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 166. [Google Scholar] [CrossRef] [PubMed]
- Pleasant, A. Advancing health literacy measurement: A pathway to better health and health system performance. J. Health Commun. 2014, 19, 1481–1496. [Google Scholar] [CrossRef]
- McCormack, L.; Haun, J.; Sørensen, K.; Valerio, M. Recommendations for advancing health literacy measurement. J. Health Commun. 2013, 18 (Suppl. 1), 9–14. [Google Scholar] [CrossRef]
- Healy, T. The measurement of social capital at international level. In Social Capital: The Challenge of International Measurement; OECD: Paris, France, 2002; Available online: http://www.oecd.org/dataoecd/1/60/2380281.pdf (accessed on 5 May 2020).
- Lee, D.; Jeong, K.-Y.; Chae, S. Measuring social capital in East Asia and other world regions: Index of social capital for 72 countries. Glob. Econ. Rev. 2011, 40, 385–407. [Google Scholar] [CrossRef]
- Abel, T.; Hofmann, K.; Ackermann, S.; Bucher, S.; Sakarya, S. Health literacy among young adults: A short survey tool for public health and health promotion research. Health Promot. Int. 2015, 30, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Guttersrud, Ø.; Dalane, J.Ø.; Pettersen, S. Improving measurement in nutrition literacy research using Rasch modelling: Examining construct validity of stage-specific ‘critical nutrition literacy’scales. Public Health Nutr. 2014, 17, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Health Literacy Tool Shed. Available online: https://healthliteracy.bu.edu/ (accessed on 5 May 2020).
- Easton, P.; Entwistle, V.; Williams, B. How the stigma of low literacy can impair patient-professional spoken interactions and affect health: Insights from a qualitative investigation. BMC Health Serv. Res. 2013, 13, 319. [Google Scholar] [CrossRef] [PubMed]
- Guzys, D.; Kenny, A.; Dickson-Swift, V.; Threlkeld, G. A critical review of population health literacy assessment. BMC Public Health 2015, 15, 215. [Google Scholar] [CrossRef]
- Sucharew, H.; Macaluso, M. Methods for research evidence synthesis: The scoping review approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Scale Names | Year Nation | Research Questions | Theoretical Basis | Validated Sample | Domains, Items (#) | Domains | Administration Mode and Time |
|---|---|---|---|---|---|---|---|
| The Test of Functional Health Literacy in Adults [34] (TOFHLA; Parker, R.M., Baker, D.W., et al.) | 1995 US | To develop a valid and reliable instrument to measure the functional health literacy for patients. | Not mentioned | 200 participants (18+ years) | 2, 67 | (1) Prose (reading comprehension); (2) Numeracy (competencies to apply arithmetic operations and use numerical information). | Performance-based 22 min |
| Brief Health Literacy Screener [35] (BHLS; Chew, L.D., Bradley, K.A., et al.) | 2004 US | To develop a screening tool for identifying patients with inadequate or marginal health literacy. | Not mentioned | 332 participants (18+ years) | 3, 3 | (1) Help read; (2) Confident with forms; (3) Problems learning (about medical condition because of difficulty understanding written information). | Self-reported 1 min |
| The Newest Vital Sign [36] (NVS; Weiss. B.D., Mays, M.Z., et al.) | 2005 US | To develop a quick and accurate screening tool for the individuals’ with inadequate literacy. | Not mentioned | 500 participants (18+ years) | 2, 6 | (1) Prose; (2) Numeracy. | Performance-based 3 min |
| The Public Health Literacy Knowledge [37] Scale(PHLKS; Pleasant, A., Kuruvilla, S.) | 2008 US | To develop a valid and reliable public health literacy knowledge sale at the population level. | Essential facts for life messages | 829 participants (Average age = 37 years) | 1, 17 | (1) Health knowledge. | Performance-based Not mentioned |
| Korean Health Literacy Scale [48] (KHLS; Lee, T.W., Kang, S.J., et al.) | 2009 KR | To develop a valid and reliable screening test for limited health literacy for older Korean adults. | Not mentioned. | 411 community dwelling (60+ years) | 3, 24 | (1) Prose; (2) Numeracy; (3) Health knowledge. | Performance-based 15–20 min |
| Health Literacy Skills Instrument [38] (HLSI; McCormack, L., Bann, C., et al.) | 2010 US | To develop a comprehensive and skill-based instrument to measure an individual’s health literacy. | Ratzan and Parker’s definition of health literacy. | 889 participants (18+ years) | 5, 25 | (1) Prose; (2) Document; (3) Numeracy; (4) Oral (listening or audiovisual); (5) Internet-based information seeking. | Performance-based (computer-based) 45 min |
| Mandarin Health Literacy Scale [49] (MHLS; Tsai, T., Lee, S.Y.D, et al.) | 2010 China (Taiwan) | To develop a culturally suitable screening test for people who speak Mandarin Chinese. | IOM’s definition of health literacy. | 448 individuals (18+ years) | 3, 50 | (1) Prose; (2) Document; (3) Numeracy. | Performance-based Not mentioned |
| Swiss Health Literacy Survey [39] (HLS-CH; Wang, J., Thombs, B.D., et al.) | 2012 (CH) | To identify specific capabilities for health in definitions of health literacy and patient-centered concepts among the general population. | Developed a broad, inclusive framework by focusing on the level of shared core competencies of five patient-centered topics. | 1250 respondents (15+ years) | 5, 73 | (1) Information and knowledge; (2) General cognitive skills (literacy, numeracy and self-expression, interpersonal, problem-solving, critical decision-making); (3) Social roles (address social determinants of health, and consumer competencies); (4) Health management; (5) Health lifestyle. | Self-reported (telephone interview and face-to-face interview) 30 min |
| All Aspects of Health Literacy Scale [40] (AAHLS; Chinn, D., MaCarthy, C.) | 2013 UK | To develop a tool to measure functional, communicative, and critical health literacy in primary healthcare setting. | Nutbeam’s definition and conceptual model. | 146 participants (15–82 years) | 3, 14 | (1) Functional; (2) Interactive; (3) Critical. | Self-reported 7 min |
| Health Literacy Management Scale [41] (HeLMS; Jordan, J.E., Buchbinder, R. et al.) | 2013 AUS | To develop a tool to assess health literacy constructs crucial to patients when accessing, understanding, and using health information within the health systems. | Developed a conceptual framework of health literacy from the perspective of patients. | 350 participants (40+ years) | 8, 29 | (1) Attitudes; (2) Understand; (3) Social support; (4) Socioeconomic considerations; (5) Assess; (6) Interactive; (7) Being proactive(take proactive steps to source and understand health information to better address a health issue); (8) Apply. | Self-reported No time limit |
| Health Literacy Questionnaire [42] (HLQ; Osborne, R.H., Batterham, R.W., et al.) | 2013 AUS | To develop an instrument to measure health literacy needs and challenges across individuals, organizations. | Developed a comprehensive model covered the full range of health literacy capabilities in a real-world setting from the perspective of general population, practitioners, and policy makers. | 405 participants (18+ years) | 9, 44 | (1) Supported by healthcare providers; (2) Sufficient information; (3) Health management; (4) Social support; (5) Appraise; (6) Interactive; (7) Navigation; (8) Access; (9) Understand. | Self-reported No time limit |
| European Health Literacy Survey Questionnaire [43] (HLS-EU-Q; Sørensen, K., Broucke, S.V., et al.) | 2013 EU | To develop a valid and reliable tool to measure the comprehensive construct of health literacy in different populations. | Sørensen’s definition and conceptual model of health literacy. | 99 participants (15–81 years) | 4, 47 | (1) Access; (2) Understand; (3) Appraise; (4) Apply. | Self-reported 20–30 min |
| Korean Health Literacy Instrument [44] (KHLI; Kang, S.J., Lee, T.W., et al.) | 2014 KR | To develop and validate an instrument measuring the ability to understand and use health-related information and make informed health decisions in Korean adults. | Nutbeam’s definition and conceptual model. | 315 participants (40–64 years) | 3, 18 | (1) Functional; (2) Interactive; (3) Critical. | Self-reported 25 min |
| Japanese Functional Health Literacy Test [45] (JFHLT; Nakagami, K., Yamauchi. T., et al.) | 2014 Japan | To develop a reliable and valid tool of functional health literacy in a Japanese clinical setting. | Function health literacy. | 535 Japanese outpatients (22+ years) | 2, 16 | (1) Prose; (2) Numeracy. | Performance-based 10–15 min |
| Comprehensive Health Activities Scale [46] (CHAS; Curtis, L.M., Revelle, W., et al.) | 2015 US | To develop a comprehensive tasks-based health literacy measurement. | Developed a conceptual framework covered nine scenarios. depicting health-related tasks that patients often experience. | 826 participants (55–74 years) | 2, 45 | (1) Prose; (2) Numeracy. | Performance-based 60 min |
| Taiwanese Health Literacy Assessment Tool [50] (THLAT; Chung, M.H., Chen, L.K., et al.) | 2015 China (Taiwan) | To evaluate health literacy among urban elderly in Taiwan. | Nutbeam’s definition and conceptual model | 1082 elderly (60+ years) | 2, 10 | (1) Interactive; (2) Critical. | Self-reported 3–5 min |
| Iranian Health Literacy Questionnaire [51] (IHLQ; Haghdoost, A.A., Rakhshani, F., et al.) | 2015 Iran | To develop a valid and reliable instrument to measure and monitor community health literacy in Iran. | Develop a framework to measure health literacy in exposure to disease and health promotion approach adjusted for the Iranian culture. | 1080 participants (18–60 years) | 7, 36 | (1) Prose; (2) Individual empowerment (household medical equipment use); (3) Interactive; (4) Access; (5) Appraise; (6) Social empowerment; (7) Health knowledge. | Self-reported No time limit |
| ABCDE Health literacy scale [52] (ABCDE-HLS; Intarakamhang, U., Y. Kwanchuen) | 2016 Thai | To develop an instrument to measure health literacy based on the concept of ABCDE (alcohol, baccy, coping, diet, and exercise) behavior for risk reduction | Nutbeam’s conceptual model. | 4401 people (15+ years) | 3, 64 | (1) Functional; (2) Interactive; (3) Critical. | Self-reported No time limit |
| Health Literacy on Social Determinants of Health Questionnaire [47] (HL-SDHQ; M. Matsumoto, K. Nakayama) | 2017 Japan | To develop a tool measuring health literacy from the perspective of social determinants of health. | Sorensen’s definition of health literacy for the domain of health promotion; the solid fact developed by CSDH. | 831 adults (18+ years) | 10, 33 | (1) Social gradient; (2) Early life (the health impact of early development and education lasts a lifetime); (3) Social exclusion; (4) Work; (5) Unemployment; (6) Social support; (7) Social capital; (8) Addiction (9) Food; (10) Transport. | Self-reported No time limit |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, C.Y.; Xu, R.H.; Mo, P.K.-H.; Dong, D.; Wong, E.L.-Y. Generic Health Literacy Measurements for Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 7768. https://doi.org/10.3390/ijerph17217768
Tian CY, Xu RH, Mo PK-H, Dong D, Wong EL-Y. Generic Health Literacy Measurements for Adults: A Scoping Review. International Journal of Environmental Research and Public Health. 2020; 17(21):7768. https://doi.org/10.3390/ijerph17217768
Chicago/Turabian StyleTian, Cindy Yue, Richard Huan Xu, Phoenix Kit-Han Mo, Dong Dong, and Eliza Lai-Yi Wong. 2020. "Generic Health Literacy Measurements for Adults: A Scoping Review" International Journal of Environmental Research and Public Health 17, no. 21: 7768. https://doi.org/10.3390/ijerph17217768
APA StyleTian, C. Y., Xu, R. H., Mo, P. K.-H., Dong, D., & Wong, E. L.-Y. (2020). Generic Health Literacy Measurements for Adults: A Scoping Review. International Journal of Environmental Research and Public Health, 17(21), 7768. https://doi.org/10.3390/ijerph17217768