Risk Factors Associated with Outcomes of Recombinant Tissue Plasminogen Activator Therapy in Patients with Acute Ischemic Stroke

 ,
, 


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
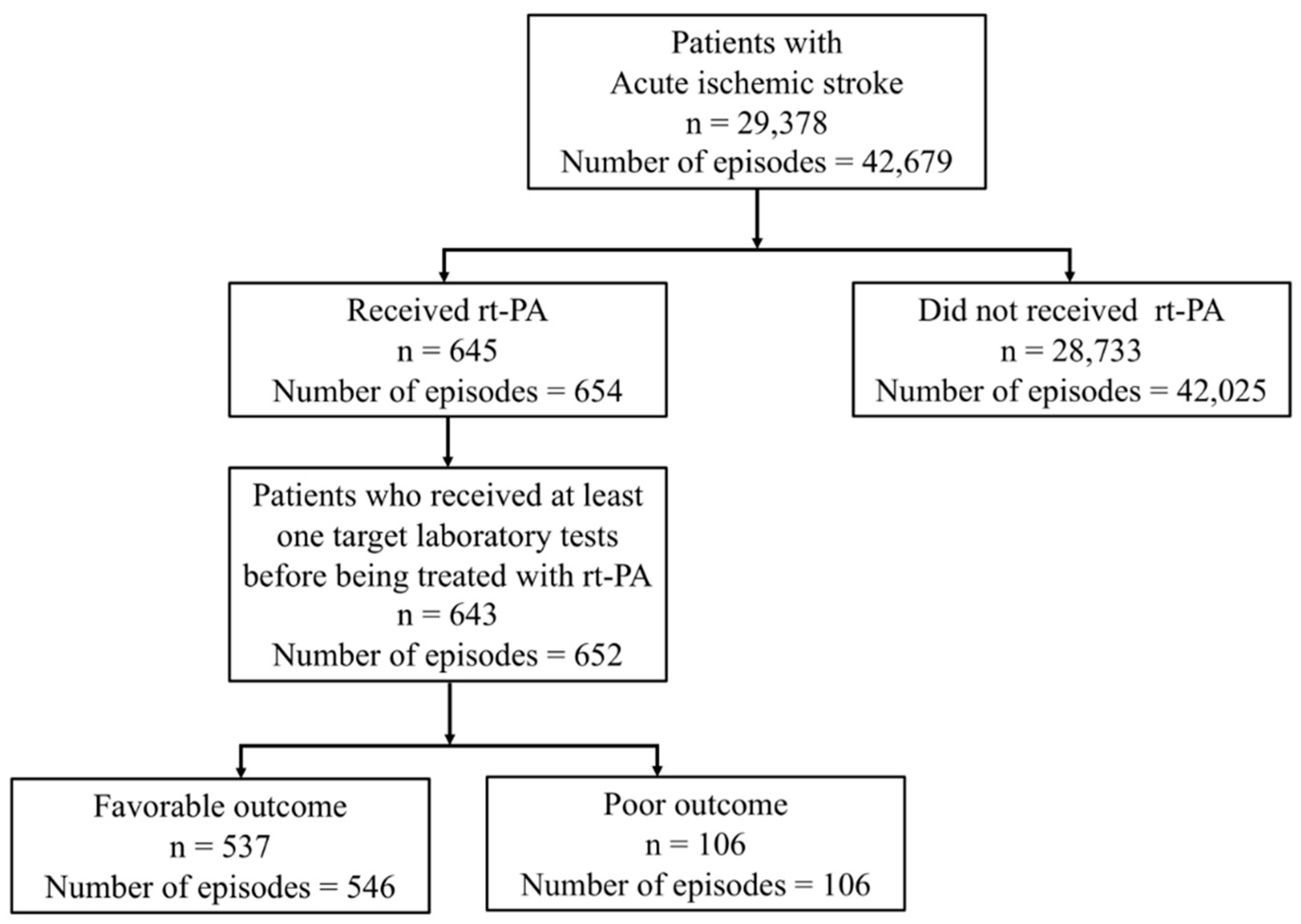
2.2. Case Identification
2.3. Outcome Definition
2.4. Laboratory Assessments
2.5. Medical History Assessment
2.6. Stroke Severity Measurement
2.7. Sensitivity Analyses
2.8. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Medical History Analysis
3.3. Multivariable Analysis
3.4. Sensitivity Analysis: Outcome Definition
3.5. Sensitivity Analysis: Transformed Laboratory Test Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2018 update: A report from the american heart association. Circulation 2018, 137, E67–E492. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.J.; Tang, S.C.; Lee, C.W.; Jeng, J.S.; Liu, H.M. Endovascular thrombectomy for acute ischemic stroke: A single-center experience in Taiwan. J. Formos. Med. Assoc. 2018, 117, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration, Ministry of Health and Welfare. The Key to Stroke Response is FAST. Available online: https://www.hpa.gov.tw/EngPages/Detail.aspx?nodeid=1038&pid=10548 (accessed on 7 January 2020).
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Murray, V.; Berge, E.; DelZoppo, G.; Sandercock, P.; Lindley, R.L.; Cohen, G. Recombinant tissue plasminogen activator for acute ischaemic stroke: An updated systematic review and meta-analysis. Lancet 2012, 379, 2364–2372. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: A guideline for healthcare professionals from the American heart association/American stroke. Stroke 2019, 50, 344–418. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; vonKummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.-H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: The European cooperative acute stroke study (ECASS). JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthi, R.R.V.; Feigin, V.L.; Forouzanfar, M.H.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.M.; Truelsen, T.; et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010. Lancet Glob. Health 2013, 1, e259–e281. [Google Scholar] [CrossRef]
- Lapchak, P.A. Critical early thrombolytic and endovascular reperfusion therapy for acute ischemic stroke victims: A call for adjunct neuroprotection. Transl. Stroke Res. 2015, 6, 345–354. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T.; et al. Thrombolysis with Alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Chen, Y.W.; Sung, S.F.; Chen, C.H.; Tang, S.C.; Tsai, L.K.; Lin, H.J.; Huang, H.Y.; Po, H.L.; Sun, Y.; Chen, P.L.; et al. Intravenous thrombolysis administration 3–4.5 h after acute ischemic stroke: A retrospective, multicenter study. Front. Neurol. 2019, 10, 1–9. [Google Scholar] [CrossRef]
- Betts, K.A.; Hurley, D.; Song, J.; Sajeev, G.; Guo, J.; Du, E.X.; Paschoalin, M.; Wu, E.Q. Real-world outcomes of acute ischemic stroke treatment with intravenous recombinant tissue plasminogen activator. J. Stroke Cerebrovasc. Dis. 2017, 26, 1996–2003. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Willey, J.Z.; Cucchiara, B.; Goldstein, J.N.; Gonzales, N.R.; Khatri, P.; Kim, L.J.; Mayer, S.A.; Sheth, K.N.; Schwamm, L.H. Treatment and outcome of hemorrhagic transformation after intravenous alteplase in acute ischemic stroke a scientific statement for healthcare professionals from the American heart association/American stroke association. Stroke 2017, 48, e343–e361. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Pan, Y.; Zhao, X.; Liu, L.; Li, H.; Liao, X.; Wang, C.; Wang, Y.; Wang, Y. Intravenous thrombolysis in Chinese patients with different subtype of mild stroke: Thrombolysis in patients with mild stroke. Sci. Rep. 2017, 7, 2299. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, F.I.; Lien, L.M.; Chen, S.T.; Bai, C.H.; Sun, M.C.M.H.; Tseng, H.P.; Chen, Y.W.; Chen, C.H.; Jeng, J.S.; Tsai, S.Y.; et al. Get with the guidelines-stroke performance indicators: Surveillance of stroke care in the Taiwan stroke registry: Get with the guidelines-stroke in Taiwan. Circulation 2010, 122, 1116–1123. [Google Scholar] [CrossRef]
- Sung, S.F.; Tseng, M.C. Code stroke: A mismatch between number of activation and number of thrombolysis. J. Formos. Med. Assoc. 2014, 113, 442–446. [Google Scholar] [CrossRef][Green Version]
- Cheng, T.J.; Peng, G.S.; Jhao, W.S.; Lee, J.T.; Wang, T.H. Nationwide “hospital emergent capability accreditation by level-stroke” improves stroke treatment in Taiwan. J. Stroke 2017, 19, 205–212. [Google Scholar] [CrossRef]
- Lyden, P. Why don’t more patients receive intravenous rt-PA for acute stroke? Expert Rev. Neurother. 2015, 15, 571–574. [Google Scholar] [CrossRef][Green Version]
- Willeit, J.; Geley, T.; Schöch, J.; Rinner, H.; Tür, A.; Kreuzer, H.; Thiemann, N.; Knoflach, M.; Toell, T.; Pechlaner, R.; et al. Thrombolysis and clinical outcome in patients with stroke after implementation of the Tyrol stroke pathway: A retrospective observational study. Lancet Neurol. 2015, 14, 48–56. [Google Scholar] [CrossRef]
- Fang, M.C.; Cutler, D.M.; Rosen, A.B. Trends in thrombolytic use for ischemic stroke in the United States. J. Hosp. Med. 2010, 5, 406–409. [Google Scholar] [CrossRef]
- Chapman, S.N.; Mehndiratta, P.; Johansen, M.C.; McMurry, T.L.; Johnston, K.C.; Southerland, A.M. Current perspectives on the use of intravenous recombinant tissue plasminogen activator (tPA) for treatment of acute ischemic stroke. Vasc. Health Risk Manag. 2014, 10, 75–87. [Google Scholar] [CrossRef]
- Liu, M.; Pan, Y.; Zhou, L.; Wang, Y. Predictors of post-thrombolysis symptomatic intracranial hemorrhage in Chinese patients with acute ischemic stroke. PLoS ONE 2017, 12, e0184646. [Google Scholar] [CrossRef] [PubMed]
- Yeo, L.L.L.; Luen, T.H.; Sharma, V.; Chan, B.; Lin, J.R.; Liow, C.W.; Lee, J.D.; Peng, T.I.; Chien, S.C.; Lee, T.H. Derivation and validation of a scoring system for intravenous tissue plasminogen activator use in Asian patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 1695–1703. [Google Scholar] [CrossRef]
- Fleming, T.; Blum, B.; Averkamp, B.; Sullivan, J.; Nathaniel, T. Effect of antihypertensive medications on thrombolysis therapy and outcomes in acute ischemic stroke patients. J. Clin. Hypertens. 2019, 21, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Gumbinger, C.; Reuter, B.; Stock, C.; Sauer, T.; Wiethölter, H.; Bruder, I.; Rode, S.; Kern, R.; Ringleb, P.; Hennerici, M.G.; et al. Time to treatment with recombinant tissue plasminogen activator and outcome of stroke in clinical practice: Retrospective analysis of hospital quality assurance data with comparison with results from randomised clinical trials. BMJ 2014, 348, g3429. [Google Scholar] [CrossRef]
- Lee, T.H.; Chang, C.H.; Chang, Y.J.; Chang, K.C.; Chung, J.; Liu, S.J.; Liou, C.W.; Chen, S.C.; Lee, J.D.; Peng, T.Y.; et al. Establishment of electronic chart-based stroke registry system in a Medical System in Taiwan. J. Formos. Med. Assoc. 2011, 110, 543–547. [Google Scholar] [CrossRef][Green Version]
- Goldstein, L.B. Accuracy of ICD-9-CM coding for the identification of patients with acute ischemic stroke: Effect of modifier codes. Stroke 1998, 29, 1602–1604. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, B.; Wu, L.; Guan, X.; Luo, Y.; Jiang, C.; Gupta, S.; Huang, Z.; Everett, G. Safety of intravenous thrombolysis for acute ischemic stroke in patients with thrombocytopenia. Cerebrovasc. Dis. 2019, 06606, 1–8. [Google Scholar] [CrossRef]
- Holroyd-Leduc, J.M.; Kapral, M.K.; Austin, P.C.; Tu, J.V. Sex differences and similarities in the management and outcome of stroke patients. Stroke 2000, 31, 1833–1837. [Google Scholar] [CrossRef]
- Nasr, D.M.; Biller, J.; Rabinstein, A.A. Use and in-hospital outcomes of recombinant tissue plasminogen activator in pediatric arterial ischemic stroke patients. Pediatr. Neurol. 2014, 51, 624–631. [Google Scholar] [CrossRef]
- Wada, T.; Yasunaga, H.; Inokuchi, R.; Horiguchi, H.; Fushimi, K.; Matsubara, T.; Nakajima, S.; Yahagi, N. Effects of edaravone on early outcomes in acute ischemic stroke patients treated with recombinant tissue plasminogen activator. J. Neurol. Sci. 2014, 345, 106–111. [Google Scholar] [CrossRef]
- Lee, H.C.; Chang, K.C.; Lan, C.F.; Hong, C.T.; Huang, Y.C.; Chang, M.L. Factors Associated with Prolonged Hospital Stay for Acute Stroke in Taiwan. Acta Neurol. Taiwan. 2008, 17, 17–25. [Google Scholar] [PubMed]
- Tseng, Y.J.; Cami, A.; Goldmann, D.A.; DeMaria, A.; Mandl, K.D. Incidence and patterns of extended-course antibiotic therapy in patients evaluated for Lyme disease. Clin. Infect. Dis. 2015, 61, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity Measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Tseng, Y.J.; Chiu, H.J. Tool of Electric Medical Record for grouping with ICD-9 and ICD-10 codes by ccs, comorbidities and phecodes, and calculating condition era emr. Available online: https://github.com/DHLab-CGU/emr/ (accessed on 7 January 2020).
- Sung, S.F.; Hsieh, C.Y.; Lin, H.J.; Chen, Y.W.; Chen, C.H.; Kao Yang, Y.H.; Hu, Y.H. Validity of a stroke severity index for administrative claims data research: A retrospective cohort study. BMC Health Serv. Res. 2016, 16, 509. [Google Scholar] [CrossRef]
- Sung, S.F.; Hsieh, C.Y.; Kao Yang, Y.H.; Lin, H.J.; Chen, C.H.; Chen, Y.W.; Hu, Y.H. Developing a stroke severity index based on administrative data was feasible using data mining techniques. J. Clin. Epidemiol. 2015, 68, 1292–1300. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Chen, C.H.; Chen, Y.C.; Kao Yang, Y.H. National survey of thrombolytic therapy for acute ischemic stroke in Taiwan 2003–2010. J. Stroke Cerebrovasc. Dis. 2013, 22, e620–e627. [Google Scholar] [CrossRef]
- Liu, S.Y.; Cao, W.F.; Wu, L.F.; Xiang, Z.B.; Liu, S.M.; Liu, H.Y.; Pan, Y.; Nie, F.; Wu, X.M.; Xie, X.F. Effect of glycated hemoglobin index and mean arterial pressure on acute ischemic stroke prognosis after intravenous thrombolysis with recombinant tissue plasminogen activator. Medicine 2018, 97, e13216. [Google Scholar] [CrossRef]
- Kim, D.H.; Lee, D.S.; Nah, H.W.; Cha, J.K. Clinical and radiological factors associated with unfavorable outcome after intravenous thrombolysis in patients with mild ischemic stroke. BMC Neurol. 2018, 18, 30. [Google Scholar] [CrossRef]
- Tang, H.; Zhang, S.; Yan, S.; Liebeskind, D.S.; Sun, J.; Ding, X.; Zhang, M.; Lou, M. Unfavorable neurological outcome in diabetic patients with acute ischemic stroke is associated with incomplete recanalization after intravenous thrombolysis. J. Neurointerventional Surg. 2016, 8, 342–346. [Google Scholar] [CrossRef]
- Al-hussain, F.; Hussain, M.S.; Molina, C.; Uchino, K.; Shuaib, A.; Demchuk, A.M.; Alexandrov, A.V.; Saqqur, M. Does the sex of acute stroke patients influence the effectiveness of rt-PA? BMC Neurol. 2014, 14, 60. [Google Scholar] [CrossRef] [PubMed]
- Jovanović, D.R.; Beslać-Bumbaširević, L.; Budimkić, M.; Pekmezović, T.; Živković, M.; Kostić, V.S. Do women benefit more from systemic thrombolysis in acute ischemic stroke? A Serbian experience with thrombolysis in ischemic stroke (SETIS) study. Clin. Neurol. Neurosurg. 2009, 111, 729–732. [Google Scholar] [CrossRef] [PubMed]
- Meseguer, E.; Mazighi, M.; Labreuche, J.; Arnaiz, C.; Cabrejo, L.; Slaoui, T.; Guidoux, C.; Olivot, J.M.; Abboud, H.; Lapergue, B.; et al. Outcomes of intravenous recombinant tissue plasminogen activator therapy according to gender: A clinical registry study and systematic review. Stroke 2009, 40, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- Buijs, J.E.; Uyttenboogaart, M.; Brouns, R.; DeKeyser, J.; Kamphuisen, P.W.; Luijckx, G.J. The effect of age and sex on clinical outcome after intravenous recombinant tissue plasminogen activator treatment in patients with acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2016, 25, 312–316. [Google Scholar] [CrossRef]
- Kent, D.M.; Price, L.L.; Ringleb, P.; Hill, M.D.; Selker, H.P. Sex-based differences in response to recombinant tissue plasminogen activator in acute ischemic stroke: A pooled analysis of randomized clinical trials. Stroke 2005, 36, 62–65. [Google Scholar] [CrossRef]
- Kapral, M.K.; Fang, J.; Hill, M.D.; Silver, F.; Richards, J.; Jaigobin, C.; Cheung, A.M. Sex differences in stroke care and outcomes: Results from the registry of the Canadian stroke Network. Stroke 2005, 36, 809–814. [Google Scholar] [CrossRef]
- Gargano, J.W.; Wehner, S.; Reeves, M. Sex differences in acute stroke care in a statewide stroke registry. Stroke 2008, 39, 24–29. [Google Scholar] [CrossRef]
- Förster, A.; Gass, A.; Kern, R.; Wolf, M.E.; Ottomeyer, C.; Zohsel, K.; Hennerici, M.; Szabo, K. Gender differences in acute ischemic stroke etiology, stroke patterns and response to thrombolysis. Stroke 2009, 40, 2428–2432. [Google Scholar] [CrossRef]
- Lorenzano, S.; Ahmed, N.; Falcou, A.; Mikulik, R.; Tatlisumak, T.; Roffe, C.; Wahlgren, N.; Toni, D. Does sex influence the response to intravenous thrombolysis in ischemic stroke? Answers from safe implementation of treatments in stroke-international stroke thrombolysis register. Stroke 2013, 44, 3401–3406. [Google Scholar] [CrossRef]
- Labiche, L.A.; Chan, W.; Saldin, K.R.; Morgenstern, L.B. Sex and acute stroke presentation. Ann. Emerg. Med. 2002, 40, 453–460. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Eijkemans, M.J.C.; Habbema, J.D.F. Stepwise Selection in small data sets. J. Clin. Epidemiol. 1999, 52, 935–942. [Google Scholar] [CrossRef]
- Harrell, F.E. Regression Modeling Strategies; Springer Series in Statistics; Springer: New York, NY, USA, 2001; ISBN 978-1-4419-2918-1. [Google Scholar]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for defining comorbidities in icd-9-cm and icd-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Menendez, M.E.; Neuhaus, V.; VanDijk, C.N.; Ring, D. The Elixhauser comorbidity method outperforms the Charlson index in predicting inpatient death after orthopaedic surgery. Clin. Orthop. Relat. Res. 2014, 472, 2878–2886. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.H.; Lin, H.J.; Chen, Y.W.; Tseng, M.C.; Hsieh, H.C.; Chen, C.H.; Sung, S.F. Safety and effectiveness of intravenous thrombolysis for acute ischemic stroke outside the coverage of national health insurance in Taiwan. Acta Neurol. Taiwan 2017, 26, 3–12. [Google Scholar]
- Nogueira, R.C.; Bor-Seng-Shu, E.; Saeed, N.P.; Teixeira, M.J.; Panerai, R.B.; Robinson, T.G. Meta-analysis of vascular imaging features to predict outcome following intravenous rtPA for acute ischemic stroke. Front. Neurol. 2016, 7, 77. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Characteristics | Favorable Outcome (n = 546) | Poor Outcome (n = 106) | p Value |
|---|---|---|---|
| Sex (%) | 0.013 * | ||
| Male | 356 (65.2) | 55 (51.9) | |
| Female | 190 (34.8) | 51 (48.1) | |
| Age (median [IQR a, Q1–Q3 b]) | 66.00 [18, 56.00–74.00] | 71.00 [18.75, 59.25–78.00] | 0.001 * |
| SSI c (median [IQR, Q1–Q3]) | 9.65 [3.51, 8.28–11.79] | 15.21 [11.34, 10.20–21.54] | <0.001 *** |
| Stroke severity (%) | <0.001 *** | ||
| Mild | 99 (18.1) | 14 (13.2) | |
| Moderate | 313 (57.3) | 20 (18.9) | |
| Severe | 134 (24.5) | 72 (67.9) |
| Laboratory Tests | Favorable Outcome (n = 546) | Poor Outcome (n = 106) | p Value |
|---|---|---|---|
| Creatinine (median [IQR a, Q1–Q3 b]) | 0.94 [0.36, 0.78–1.14] | 0.95 [0.44, 0.79–1.23] | 0.472 |
| Hemoglobin (median [IQR, Q1–Q3]) | 14.20 [2.3, 13.00–15.30] | 13.70 [2.6, 12.30–14.90] | 0.015 * |
| Hematocrit (median [IQR, Q1–Q3]) | 41.70 [5.8, 38.70–44.50] | 41.10 [6.2, 37.30–43.50] | 0.053 |
| MCH (mean corpuscular hemoglobin) (median [IQR, Q1–Q3]) | 30.50 [2.4, 29.30–31.70] | 30.60 [2.4, 29.30–31.70] | 0.826 |
| MCHC (mean corpuscular hemoglobin concentration) (median [IQR, Q1–Q3]) | 33.90 [1.5, 33.20–34.70] | 33.60 [1.8, 32.80–34.60] | 0.024 * |
| MCV (mean corpuscular volume) (median [IQR, Q1–Q3]) | 89.60 [6, 86.50–92.50] | 90.20 [6.2, 86.90–93.10] | 0.259 |
| Sodium (median [IQR, Q1–Q3]) | 139.00 [3.85, 137.15–141.00] | 138.90 [3, 137.00–140.00] | 0.116 |
| Platelets (median [IQR, Q1–Q3]) | 206.00 [72, 170.00–242.00] | 186.00 [64, 159.00–223.00] | 0.007 ** |
| RBCs (red blood cells) (median [IQR, Q1–Q3]) | 4.69 [0.67, 4.36–5.03] | 4.69 [0.85, 4.15–5.00] | 0.116 |
| RDW (red cell distribution width) (median [IQR, Q1–Q3]) | 13.60 [3.6, 12.90–16.50] | 13.60 [2.5, 12.80–15.30] | 0.608 |
| WBCs (white blood cells) (median [IQR, Q1–Q3]) | 7.90 [3.5, 6.40–9.90] | 7.50 [3, 6.50–9.50] | 0.639 |
| ALT (alanine aminotransferase) (median [IQR, Q1–Q3]) | 23.00 [15, 17.00–32.00] | 22.50 [17, 16.00–33.00] | 0.694 |
| Glucose (median [IQR, Q1–Q3]) | 128.00 [47, 110.00–157.00] | 144.00 [56, 124.00–180.00] | <0.001 *** |
| Potassium (median [IQR, Q1–Q3]) | 3.70 [0.5, 3.44–3.94] | 3.70 [0.42, 3.57–3.99] | 0.139 |
| Medical Histories (%) | Favorable Outcome (n = 546) | Poor Outcome (n = 106) | p-Value |
|---|---|---|---|
| Deficiency anemias | 11 (2.0) | 6 (5.7) | 0.068 |
| Congestive heart failure | 42 (7.7) | 7 (6.6) | 0.851 |
| Diabetes without chronic complications | 85 (15.6) | 16 (15.1) | 1 |
| Hypertension, uncomplicated | 187 (34.2) | 33 (31.1) | 0.611 |
| Hypertension, complicated | 21 (3.8) | 6 (5.7) | 0.554 |
| Liver disease | 28 (5.1) | 8 (7.5) | 0.444 |
| Chronic pulmonary disease | 45 (8.2) | 12 (11.3) | 0.401 |
| Solid tumor without metastasis | 29 (5.3) | 8 (7.5) | 0.496 |
| Valvular disease | 34 (6.2) | 8 (7.5) | 0.771 |
| Selected Variable | Coefficient |
|---|---|
| Anemia | 0.752 |
| Sex: Male | −0.178 |
| SSI a | 0.887 |
| MCHC | −0.042 |
| Platelet Count | −0.142 |
| Glucose | 0.200 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, Y.-J.; Hu, R.-F.; Lee, S.-T.; Lin, Y.-L.; Hsu, C.-L.; Lin, S.-W.; Liou, C.-W.; Lee, J.-D.; Peng, T.-I.; Lee, T.-H. Risk Factors Associated with Outcomes of Recombinant Tissue Plasminogen Activator Therapy in Patients with Acute Ischemic Stroke. Int. J. Environ. Res. Public Health 2020, 17, 618. https://doi.org/10.3390/ijerph17020618
Tseng Y-J, Hu R-F, Lee S-T, Lin Y-L, Hsu C-L, Lin S-W, Liou C-W, Lee J-D, Peng T-I, Lee T-H. Risk Factors Associated with Outcomes of Recombinant Tissue Plasminogen Activator Therapy in Patients with Acute Ischemic Stroke. International Journal of Environmental Research and Public Health. 2020; 17(2):618. https://doi.org/10.3390/ijerph17020618
Chicago/Turabian StyleTseng, Yi-Ju, Ru-Fang Hu, Shin-Tyng Lee, Yu-Li Lin, Chien-Lung Hsu, Shih-Wei Lin, Chia-Wei Liou, Jiann-Der Lee, Tsung-I Peng, and Tsong-Hai Lee. 2020. "Risk Factors Associated with Outcomes of Recombinant Tissue Plasminogen Activator Therapy in Patients with Acute Ischemic Stroke" International Journal of Environmental Research and Public Health 17, no. 2: 618. https://doi.org/10.3390/ijerph17020618
APA StyleTseng, Y.-J., Hu, R.-F., Lee, S.-T., Lin, Y.-L., Hsu, C.-L., Lin, S.-W., Liou, C.-W., Lee, J.-D., Peng, T.-I., & Lee, T.-H. (2020). Risk Factors Associated with Outcomes of Recombinant Tissue Plasminogen Activator Therapy in Patients with Acute Ischemic Stroke. International Journal of Environmental Research and Public Health, 17(2), 618. https://doi.org/10.3390/ijerph17020618