Anxiety and Depression Associated with Anal Sexual Practices among HIV-Negative Men Who Have Sex with Men in Western China

 ,
,
Abstract
1. Introduction
2. Materials and Methods
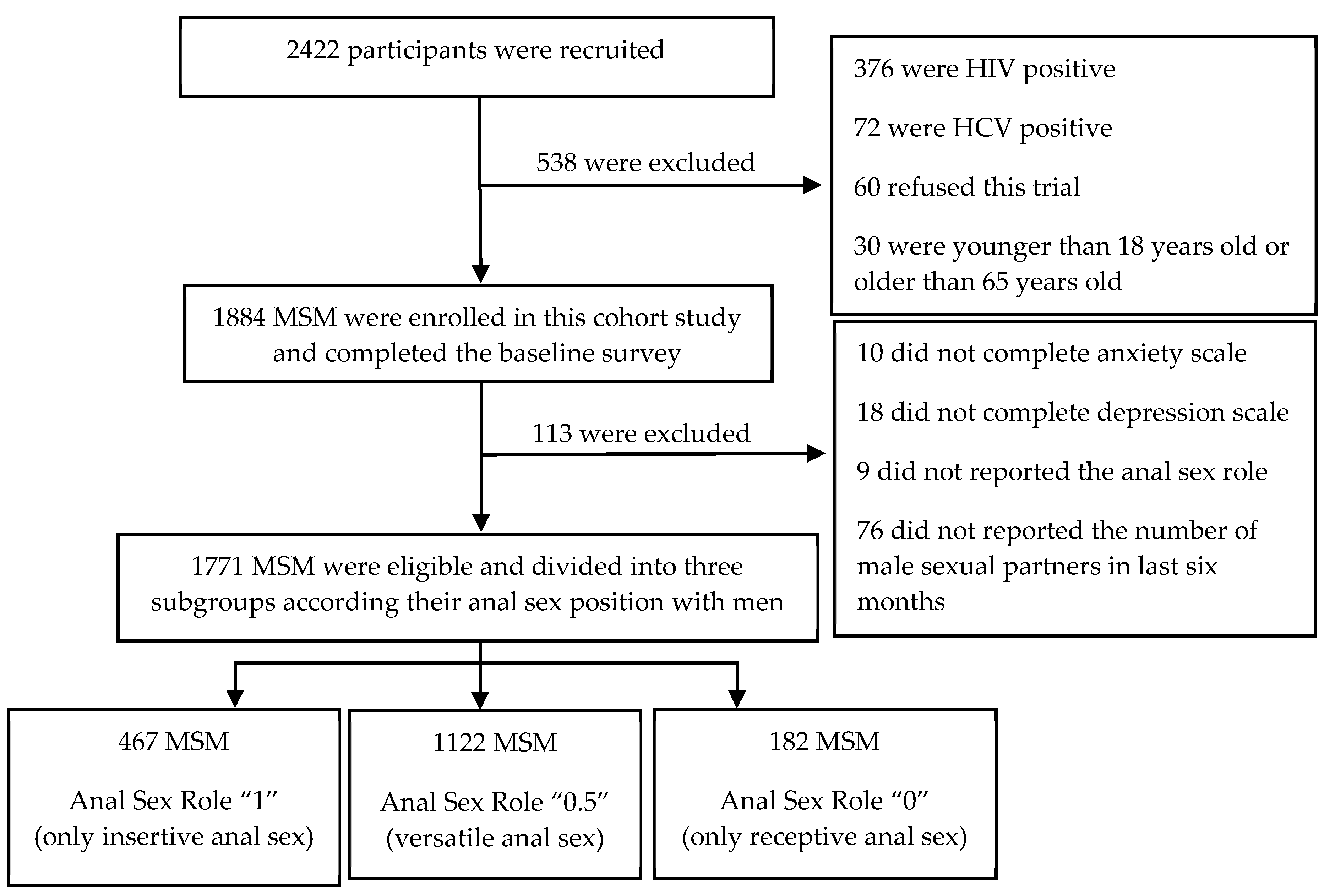
2.1. Study Procedures
2.2. Study Content and Measurements
2.2.1. Assessment of Anxiety
2.2.2. Assessment of Depression
2.2.3. Anal Sex Role Factors
2.2.4. Social Demographic Factors
2.2.5. Behavior-Related Factors
2.2.6. Risk Perception-Related Factors
2.3. Quality Control and Ethics
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. The Prevalence of Anxiety and Depression in Different Anal Sex Roles of MSM
3.3. The Influencing Factors of Anxiety in HIV-Negative MSM
3.4. The Influencing Factors of Depression in HIV-Negative MSM
4. Discussion
4.1. The Prevalence of Anxiety and Depression in HIV-Negative MSM
4.2. Influencing Factors
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chow, E.P.F.; Lau, J.T.F.; Zhuang, X.; Zhang, X.; Wang, Y.; Zhang, L. HIV Prevalence Trends, Risky Behaviours, and Governmental and Community Responses to the Epidemic among Men Who Have Sex with Men in China. BioMed Res. Int. 2014, 2014, 607261. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.E.; Li, D.; Li, P.; Guo, W.; Cui, Y. Population Specific Sentinel Surveillance for HIV Infection, Syphilis and HCV Infection in China, During 2010–2015. Dis. Surveill. 2017, 32, 111–117. (In Chinese) [Google Scholar]
- Wu, Z.; Xu, J.; Liu, E.; Mao, Y.; Xiao, Y.; Sun, X.; Liu, Y.; Jiang, Y.; McGoogan, J.M.; Dou, Z.; et al. HIV and syphilis prevalence among men who have sex with men: A cross-sectional survey of 61 cities in China. Clin. Infect. Dis. 2013, 57, 298–309. [Google Scholar] [CrossRef] [PubMed]
- UNAIDS. The Gap Report 2014: Gay Men and Other Men Who Have Sex with Men. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf (accessed on 16 June 2019).
- Safren, S.A.; Thomas, B.E.; Mimiaga, M.J.; Chandrasekaran, V.; Menon, S.; Swaminathan, S.; Mayer, K.H. Depressive symptoms and human immunodeficiency virus risk behavior among men who have sex with men in Chennai, India. Psychol. Health Med. 2009, 14, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Bluthenthal, R.N.; Palar, K.; Mendel, P.; Kanouse, D.E.; Corbin, D.E.; Derose, K.P. Attitudes and beliefs related to HIV/AIDS in urban religious congregations: Barriers and opportunities for HIV-related interventions. Soc. Sci. Med. 2012, 74, 1520–1527. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Zhou, X.; Wang, H.; Luo, M.; Pan, X.; Ma, Q.; Chen, L. Psychosocial Factors Associated with Quality of Life in Young Men Who Have Sex with Men Living with HIV/AIDS in Zhejiang, China. Int. J. Environ. Res. Public Health 2019, 16, 2667. [Google Scholar] [CrossRef]
- Salomon, E.A.; Mimiaga, M.J.; Husnik, M.J.; Welles, S.L.; Manseau, M.W.; Montenegro, A.B.; Safren, S.A.; Koblin, B.A.; Chesney, M.A.; Mayer, K.H. Depressive Symptoms, Utilization of Mental Health Care, Substance Use and Sexual Risk among Young Men Who Have Sex with Men in Explore: Implications for Age-Specific Interventions. AIDS Behav. 2009, 13, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McGonagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.-U.; Kendler, K.S. Lifetime and 12-Month Prevalence of DSM-III-R Psychiatric Disorders in the United States. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Mills, T.C.; Paul, J.; Stall, R.; Pollack, L.; Canchola, J.; Chang, Y.J.; Moskowitz, J.T.; Catania, J.A. Distress and Depression in Men Who Have Sex with Men: The Urban Men’s Health Study. Am. J. Psychiatry 2004, 161, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.R.; Zhang, J.; Shi, Q.; Song, Z.; Ding, Z.; Pang, S.; Li, X.; Zhang, Y.; Wang, Z. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001–2005: An epidemiological survey. Lancet 2009, 373, 2041–2053. [Google Scholar] [CrossRef]
- Chou, F.Y.; Armstrong, H.L.; Wang, L.; Bacani, N.; Lachowsky, N.J.; Patterson, T.L.; Walsh, Z.; Olarewaju, G.; Card, K.G.; Roth, E.A.; et al. A longitudinal analysis of cannabis use and mental health symptoms among gay, bisexual, and other men who have sex with men in Vancouver, Canada. J. Affect. Disord. 2019, 247, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Díaz, R.M.; Ayala, G.; Bein, E.; Henne, J.; Marin, B.V. The impact of homophobia, poverty, and racism on the mental health of gay and bisexual Latino men: Findings from 3 US cities. Am. J. Public Health 2001, 91, 927–932. [Google Scholar] [PubMed]
- Gao, X.; Zhang, R.; Li, Y.; Ma, Y.; Chen, Y.; Ma, J.; Li, Z.; Jia, M. Depression and Related Influential Factors among Men Who Have Sex with Men in Kunming. Chin. J. AIDS STD 2018, 24, 170–173. (In Chinese) [Google Scholar]
- Jiang, T.; Pan, X.; Wang, H.; Zhou, X.; Ma, Q. Depressive, Anxiety Symptoms and Related Influential Factors among Man Who Have Sex with Man in Zhejiang. Chin. J. AIDS STD 2016, 22, 357–360. (In Chinese) [Google Scholar]
- Wang, Y.; Li, L.; Zhou, W.; Fan, J.; Zhao, X.; Tang, Y.; He, J.; Liu, J.; Zhou, L.; Zhang, X. Anxiety and Depressive Symptoms and Related Factors in 15–24 Year-Old Young Men Who Have Sex with Men Behavior. Chin. Ment. Health J. 2018, 32, 1017–1024. (In Chinese) [Google Scholar]
- Zeng, X.; Zhong, X.; Peng, B.; Zhang, Y.; Kong, C.; Liu, X.; Huang, A. Prevalence and associated risk characteristics of HIV infection based on anal sexual role among men who have sex with men: A multi-city cross-sectional study in Western China. Int. J. Infect. Dis. 2016, 49, 111–118. [Google Scholar] [CrossRef]
- Rich, A.J.; Lachowsky, N.J.; Cui, Z.; Sereda, P.; Lal, A.; Moore, D.M.; Hogg, R.S.; Roth, E.A. Event-Level Analysis of Anal Sex Roles and Sex Drug Use among Gay and Bisexual Men in Vancouver, British Columbia, Canada. Arch. Sex. Behav. 2016, 45, 1443–1451. [Google Scholar] [CrossRef]
- Carballo-Diéguez, A.; Bauermeister, J.A.; Ventuneac, A.; Dolezal, C.; Balan, I.; Remien, R.H. The Use of Rectal Douches among HIV-Uninfected and Infected Men Who Have Unprotected Receptive Anal Intercourse: Implications for Rectal Microbicides. AIDS Behav. 2008, 12, 860–866. [Google Scholar] [CrossRef]
- Ucciferri, C.; Tamburro, M.; Falasca, K.; Sammarco, M.L.; Ripabelli, G.; Vecchiet, J. Prevalence of Anal, Oral, Penile and Urethral Human Papillomavirus in HIV Infected and HIV Uninfected Men Who Have Sex with Men. J. Med. Virol. 2018, 90, 358–366. [Google Scholar] [CrossRef]
- Hart, T.L.; Coon, D.W.; Kowalkowski, M.A.; Zhang, K.; Hersom, J.I.; Goltz, H.H.; Wittmann, D.A.; Latini, D.M. Changes in sexual roles and quality of life for gay men after prostate cancer: Challenges for sexual health providers. J. Sex. Med. 2014, 11, 2308–2317. [Google Scholar] [CrossRef]
- Johns, M.M.; Pingel, E.; Eisenberg, A.; Santana, M.L.; Bauermeister, J. Butch tops and femme bottoms? Sexual positioning, sexual decision making, and gender roles among young gay men. Am. J. Men’s Health 2012, 6, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Wei, C.; Raymond, H.F. Preference for and Maintenance of Anal Sex Roles among Men Who Have Sex with Men: Sociodemographic and Behavioral Correlates. Arch. Sex. Behav. 2011, 40, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Nugraheni, P.; Tobing, H.; Kusumadewi, I.; Siste, K.; Putri, N. Is it important to assess mental health problem in MSM? Asian J. Psychiatry 2018, 101584. [Google Scholar] [CrossRef] [PubMed]
- Bostwick, W.B.; Boyd, C.J.; Hughes, T.L.; McCabe, S.E. Dimensions of Sexual Orientation and the Prevalence of Mood and Anxiety Disorders in the United States. Am. J. Public Health 2010, 100, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.D.; Lõhmus, L.; Valk, A.; Mangine, C.; Rüütel, K. Outcomes associated with anxiety and depression among men who have sex with men in Estonia. J. Affect. Disord. 2015, 183, 205–209. [Google Scholar] [CrossRef]
- Fendrich, M.; Avci, O.; Johnson, T.P.; Mackesy-Amiti, M.E. Depression, Substance Use and Hiv Risk in a Probability Sample of Men Who Have Sex with Men. Addict. Behav. 2013, 38, 1715–1718. [Google Scholar] [CrossRef]
- Hanrahan, N.P.; Wu, E.; Kelly, D.; Aiken, L.H.; Blank, M.B. Randomized Clinical Trial of the Effectiveness of a Home-Based Advanced Practice Psychiatric Nurse Intervention: Outcomes for Individuals with Serious Mental Illness and HIV. Nurs. Res. Pract. 2011, 2011, 840248. [Google Scholar] [CrossRef]
- Pappin, M.; Wouters, E.; Booysen, F.L. Anxiety and depression amongst patients enrolled in a public sector antiretroviral treatment programme in South Africa: A cross-sectional study. BMC Public Health 2012, 12, 244. [Google Scholar] [CrossRef]
- Chen, F.; Ding, F.; Lin, X.; Wang, X.; He, H.; Huang, W.; Dong, Y.; Yang, Q.; Zhang, H. Prevalence Rates of Depression and Anxiety in HIV-Infected Men Who Have Sex with Men. Chin. Ment. Health J. 2015, 29, 251–257. (In Chinese) [Google Scholar]
- Szymańska-Kotwica, B.; Cholewińska, G.; Cielniak, I.; Firlag-Burkacka, E.; Łojek, E.; Horban, A.; Bornstein, R. Prevalence of depression and anxiety symptoms in HIV-positive men who have sex with men treated with effective cART. J. Psychosom. Res. 2018, 109, 138. [Google Scholar] [CrossRef]
- Tran, B.X.; Ho, R.C.M.; Ho, C.S.H.; Latkin, C.A.; Phan, H.T.; Ha, G.H.; Vu, G.T.; Ying, J.; Zhang, M.W.B. Depression among Patients with HIV/AIDS: Research Development and Effective Interventions (GAPRESEARCH). Int. J. Environ. Res. Public Health 2019, 16, 1772. [Google Scholar] [CrossRef]
- Clark, J.; Salvatierra, J.; Segura, E.R.; Salazar, X.; Konda, K.; Perez-Brumer, A.; Hall, E.; Klausner, J.; Caceres, C.; Coates, T. Moderno love: Sexual role-based identities and HIV/STI prevention among men who have sex with men in Lima, Peru. AIDS Behav. 2013, 17, 1313–1328. [Google Scholar] [CrossRef] [PubMed]
- Zung, W.W. A Rating Instrument for Anxiety Disorders. Psychosomatics 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Koblin, B.; Chesney, M.; Coates, T. Effects of a behavioural intervention to reduce acquisition of HIV infection among men who have sex with men: The EXPLORE randomised controlled study. Lancet 2004, 364, 41–50. [Google Scholar] [CrossRef]
- Ying, M.; Zhang, Y.; Song, G. Research on Epidemic Model of Emergency Events Risk Perception in Food Industry. Sci. Res. Manag. 2013, 34, 123–130. (In Chinese) [Google Scholar]
- Bradley, H.; Tsui, A.; Hindin, M.; Kidanu, A.; Gillespie, D. Developing scales to measure perceived HIV risk and vulnerability among Ethiopian women testing for HIV. AIDS Care 2011, 23, 1043–1052. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.; Zhang, J.; Chu, Z.; Hu, Q.; Geng, W.; Jiang, Y.; Wang, N.; Xu, J. Association between Psychological Disorders, Depression and the Cd4 Level of HIV Negative MSM in Shenyang. Chin. J. AIDS STD 2018, 24, 1115–1118. (In Chinese) [Google Scholar]
- Hylton, E.; Wirtz, A.L.; Zelaya, C.E.; Latkin, C.; Peryshkina, A.; Mogilnyi, V.; Dzhigun, P.; Kostetskaya, I.; Galai, N.; Beyrer, C. Sexual Identity, Stigma, and Depression: The Role of the “Anti-gay Propaganda Law” in Mental Health among Men Who Have Sex with Men in Moscow, Russia. J. Hered. 2017, 94, 319–329. [Google Scholar] [CrossRef]
- Stoloff, K.; Joska, J.A.; Feast, D.; De Swardt, G.; Hugo, J.; Struthers, H.; McIntyre, J.; Rebe, K. A Description of Common Mental Disorders in Men Who Have Sex with Men (MSM) Referred for Assessment and Intervention at an MSM Clinic in Cape Town, South Africa. AIDS Behav. 2013, 17 (Suppl. 1), S77–S81. [Google Scholar] [CrossRef]
- De Santis, J.P.; Colin, J.M.; Vasquez, E.P.; McCain, G.C. The Relationship of Depressive Symptoms, Self-Esteem, and Sexual Behaviors in a Predominantly Hispanic Sample of Men Who Have Sex with Men. Am. J. Men’s Health 2008, 2, 314–321. [Google Scholar] [CrossRef]
- Chen, C.; Wang, M.; Wang, T.; Li, L.; Lai, X.; Sun, Y.; Chen, J. Analysis of the Sex Roles in the Relationship with the HIV/Syphilis Infection and the Related Behaviors among Men Who Have Sex with Men in Zhongshan City. J. Public Health Prev. Med. 2016, 27, 53–56. (In Chinese) [Google Scholar]
- Jorm, A.F.; Korten, A.E.; Rodgers, B.; Jacomb, P.A.; Christensen, H. Sexual orientation and mental health: Results from a community survey of young and middle—Aged adults. Br. J. Psychiatry 2002, 180, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Secor, A.M.; Wahome, E.; Micheni, M.; Rao, D.; Simoni, J.M.; Sanders, E.J.; Graham, S.M. Depression, substance abuse and stigma among men who have sex with men in coastal Kenya. AIDS 2015, 29, S251–S259. [Google Scholar] [CrossRef] [PubMed]
- Kramer, S.C.; Schmidt, A.J.; Berg, R.C.; Furegato, M.; Hospers, H.; Folch, C.; Marcus, U.; Network, E. Factors associated with unprotected anal sex with multiple non-steady partners in the past 12 months: Results from the European Men-Who-Have-Sex-with-Men Internet Survey (EMIS 2010). BMC Public Health 2016, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Li, L.; Qi, J.; Chen, M. Status of Anxiety and Depression and Related Influence Factors among Men Who Have Sex with Man in Shenzhen. Chin. J. AIDS STD 2017, 23, 630–633. (In Chinese) [Google Scholar]
- Chen, C.; Wang, M.; Wang, T.; Li, L.; Lai, X.; Sun, Y.; Chen, J. Impact of the Sexual Roles in the Relationship with the HIV Infection and the Related Behaviors among Men Who Have Sex with Men, Zhongshan City. Mod. Prev. Med. 2016, 43, 99–102. (In Chinese) [Google Scholar]
- Zhang, J.; Li, Q.; Han, D.; Wang, X.; Wu, C.; He, Q.; Liu, S.; Nuan, R. The Sexual Role Status and Its Relationship with Condom Use and HIV-Testing in Men Who Have Sex with Men. Chin. J. Dis. Control Prev. 2013, 17, 400–403. (In Chinese) [Google Scholar]
- Alvy, L.M.; McKirnan, D.J.; Mansergh, G.; Koblin, B.; Colfax, G.N.; Flores, S.A.; Hudson, S.; Project MIX Study Group. Depression is Associated with Sexual Risk among Men Who Have Sex with Men, but is Mediated by Cognitive Escape and Self-Efficacy. AIDS Behav. 2011, 15, 1171–1179. [Google Scholar] [CrossRef]
- Gilman, S.E.; Cochran, S.D.; Mays, V.M.; Hughes, M.; Ostrow, D.; Kessler, R.C. Risk of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Survey. Am. J. Public Health 2001, 91, 933–939. [Google Scholar]
- Tao, J.; Qian, H.-Z.; Kipp, A.M.; Ruan, Y.; Shepherd, B.E.; Amico, K.R.; Shao, Y.; Lu, H.; Vermund, S.H. Effects of depression and anxiety on antiretroviral therapy adherence among newly diagnosed HIV-infected Chinese MSM. AIDS 2017, 31, 401–406. [Google Scholar]


{kind=link}
| Characteristics | Total n (%) | Anxiety | p Value | Depression | p Value | ||
|---|---|---|---|---|---|---|---|
| NO n (%) | YES n (%) | NO n (%) | YES n (%) | ||||
| N | 1771 (100.00) | 1310 (73.97) | 461 (26.03) | 1101 (62.17) | 670 (37.83) | ||
| Anal sex role factors | |||||||
| The role of MSM in anal sex with male sexual partners | |||||||
| Anal sex role “1” | 467 (26.37) | 363 (77.73) | 104 (22.27) | 0.0415 | 314 (67.24) | 153 (32.76) | 0.0047 |
| Anal sex role “0.5” | 1122 (63.35) | 822 (73.26) | 300 (26.74) | 689 (61.41) | 433 (38.59) | ||
| Anal sex role “0” | 182 (10.28) | 125 (68.68) | 57 (31.32) | 98 (53.85) | 84 (46.15) | ||
| Social demographic factors | |||||||
| Age | |||||||
| 18–24 | 557 (31.45) | 400 (71.81) | 157 (28.19) | 0.1633 | 321 (57.63) | 236 (42.37) | 0.0285 |
| 25–30 | 532 (30.04) | 389 (73.12) | 143 (26.88) | 342 (64.29) | 190 (35.71) | ||
| ≥31 | 682 (38.51) | 521 (76.39) | 161 (23.61) | 438 (64.22) | 244 (35.78) | ||
| Area # | |||||||
| Urban | 1267 (71.74) | 971 (76.64) | 296 (23.26) | <0.0001 | 829 (65.43) | 438 (34.57) | <0.0001 |
| Rural | 499 (28.26) | 337 (67.54) | 162 (32.46) | 271 (54.31) | 228 (45.69) | ||
| Ethnic groups # | |||||||
| Han nationality | 1638 (92.54) | 1201 (73.32) | 437 (26.68) | 0.0324 | 1009 (61.60) | 629 (38.40) | 0.0944 |
| Other ethnic minorities | 132 (7.46) | 108 (81.82) | 24 (18.18) | 91 (68.94) | 41 (31.06) | ||
| Educational level # | |||||||
| Junior high or below | 215 (12.15) | 128 (59.53) | 87 (40.47) | <0.0001 | 108 (50.23) | 107 (49.77) | <0.0001 |
| Senior high | 468 (26.46) | 330 (70.51) | 138 (29.49) | 275 (58.76) | 193 (41.24) | ||
| College or graduate or above | 1086 (61.39) | 850 (78.27) | 236 (21.73) | 716 (65.93) | 370 (34.07) | ||
| Employment status # | |||||||
| On the job | 1358 (76.81) | 1016 (74.82) | 342 (25.18) | 0.0150 | 861 (63.40) | 497 (36.60) | 0.1219 |
| Students at school | 243 (13.74) | 184 (75.72) | 59 (24.28) | 144 (59.26) | 99 (40.74) | ||
| Retired or unemployed | 167 (9.45) | 108 (64.67) | 59 (35.33) | 94 (56.29) | 73 (43.71) | ||
| Marital status | |||||||
| Unmarried | 1314 (74.20) | 986 (75.04) | 328 (24.96) | 0.0706 | 834 (63.47) | 480 (36.53) | 0.1257 |
| Married | 307 (17.33) | 211 (68.73) | 96 (31.27) | 176 (57.33) | 131 (42.67) | ||
| Divorce or widowhood | 150 (8.47) | 113 (75.33) | 37 (24.67) | 91 (60.67) | 59 (39.33) | ||
| Personal monthly income # | |||||||
| ≤3000 | 927 (52.94) | 658 (70.98) | 269 (29.02) | 0.0014 | 522 (56.31) | 405 (43.69) | <0.0001 |
| 3001–5000 | 602 (34.38) | 454 (75.42) | 148 (24.58) | 398 (66.11) | 204 (33.89) | ||
| ≥5001 | 222 (12.68) | 183 (82.43) | 39 (17.57) | 168 (75.68) | 54 (24.32) | ||
| Behavior-related factors | |||||||
| Regular male sexual partners in the last six months # | |||||||
| 0 | 293 (16.80) | 217 (74.06) | 76 (25.94) | 0.2290 | 179 (61.09) | 114 (38.91) | 0.3778 |
| 1 | 1188 (68.12) | 892 (75.08) | 296 (24.92) | 755 (63.55) | 433 (36.45) | ||
| ≥2 | 263 (15.08) | 184 (69.96) | 79 (30.04) | 156 (59.32) | 107 (40.68) | ||
| Casual male sexual partners in the last six months # | |||||||
| 0 | 705 (40.68) | 541 (76.74) | 164 (23.26) | 0.0373 | 466 (66.10) | 239 (33.90) | 0.0072 |
| ≥1 | 1028 (59.32) | 743 (72.28) | 285 (27.72) | 614 (59.73) | 414 (40.27) | ||
| Female sexual partners in the last six months # | |||||||
| 0 | 1462 (84.17) | 1113 (76.13) | 349 (23.87) | <0.0001 | 944 (64.57) | 518 (35.43) | <0.0001 |
| ≥1 | 275 (15.83) | 172 (62.55) | 103 (37.45) | 137 (49.82) | 138 (50.18) | ||
| Frequency of seeking partners on the Internet in the last 6 months # | |||||||
| Often | 117 (6.62) | 69 (58.97) | 48 (41.03) | 0.0006 | 55 (47.01) | 62 (52.99) | 0.0008 |
| Sometimes or occasionally | 986 (55.80) | 743 (75.35) | 243 (24.65) | 612 (62.07) | 374 (37.93) | ||
| Never | 664 (37.58) | 495 (74.55) | 169 (25.45) | 434 (65.36) | 230 (34.64) | ||
| Whether a commercial sexual service in the past 6 months # | |||||||
| Yes | 100 (5.66) | 63 (63.00) | 37 (37.00) | 0.0095 | 54 (54.00) | 46 (46.00) | 0.0810 |
| No | 1668 (94.34) | 1246 (74.70) | 422 (25.30) | 1046 (62.71) | 622 (37.29) | ||
| Diagnosed with an sexually transmitted diseases (STD) in the past six months # | |||||||
| Yes | 142 (8.03) | 87 (61.27) | 55 (38.73) | 0.0003 | 70 (49.30) | 72 (50.70) | 0.0009 |
| No | 1626 (91.97) | 1221 (75.09) | 405 (24.91) | 1030 (63.25) | 596 (36.65) | ||
| Frequency of alcohol use in the last month # | |||||||
| Daily | 72 (4.07) | 45 (62.50) | 27 (37.50) | 0.0464 | 30 (41.67) | 42 (58.33) | 0.0009 |
| Occasionally | 1152 (65.12) | 866 (75.17) | 286 (24.83) | 733 (63.63) | 419 (36.37) | ||
| Never | 545 (30.81) | 397 (72.84) | 148 (27.16) | 336 (61.65) | 209 (38.35) | ||
| Whether a use of illicit drugs in the past six months # | |||||||
| No | 1695 (96.91) | 1261 (74.40) | 434 (25.60) | 0.1136 | 1058 (62.42) | 637 (37.58) | 0.8452 |
| Yes | 54 (3.09) | 35 (64.81) | 19 (35.19) | 33 (61.11) | 21 (38.89) | ||
| Risk perception-related factors | |||||||
| Perceived severity of AIDS # | |||||||
| Very serious | 1107 (62.54) | 832 (75.16) | 275 (24.84) | 0.3072 * | 679 (61.34) | 428 (38.66) | 0.5051 * |
| Serious | 522 (29.49) | 379 (72.61) | 143 (27.39) | 334 (63.98) | 188 (36.02) | ||
| General | 123 (6.95) | 87 (70.73) | 36 (29.27) | 77 (62.60) | 46 (37.40) | ||
| Not serious | 10 (0.56) | 7 (70.00) | 3 (30.00) | 7 (70.00) | 3 (30.00) | ||
| Not serious at all | 8 (0.45) | 4 (50.00) | 4 (50.00) | 3 (37.50) | 5 (62.50) | ||
| Perceived prevalence of HIV among MSM in your city # | |||||||
| Very high | 375 (21.23) | 258 (68.80) | 117 (31.20) | 0.0691 | 219 (58.40) | 156 (41.60) | 0.2287 |
| High | 774 (43.83) | 595 (76.87) | 179 (23.13) | 502 (64.86) | 272 (35.14) | ||
| General | 420 (23.78) | 308 (73.33) | 112 (26.67) | 253 (60.24) | 167 (39.76) | ||
| Low | 126 (7.13) | 93 (73.81) | 33 (26.19) | 81 (64.29) | 45 (35.71) | ||
| Very low | 71 (4.02) | 52 (73.24) | 19 (26.76) | 43 (60.56) | 28 (39.44) | ||
| Perceived threat of HIV to yourself and your family # | |||||||
| Very large | 973 (55.03) | 707 (72.66) | 266 (27.34) | 0.0994 | 587 (60.33) | 386 (39.67) | 0.0147 |
| Relatively large and moderate | 639 (36.14) | 474 (74.18) | 165 (25.82) | 400 (62.60) | 239 (37.40) | ||
| Very small | 156 (8.82) | 126 (80.77) | 30 (19.23) | 113 (72.44) | 43 (27.56) | ||
| Frequency of condom use when having anal sex with men # | |||||||
| Always | 956 (56.84) | 725 (75.84) | 231 (24.16) | 0.0051 | 616 (64.44) | 340 (35.56) | 0.0050 |
| Occasionally | 562 (33.41) | 423 (75.27) | 139 (24.73) | 356 (63.35) | 206 (36.65) | ||
| Never | 164 (9.75) | 105 (64.02) | 59 (35.98) | 84 (51.22) | 80 (48.78) | ||
| HIV voluntary counseling # | |||||||
| Yes | 1074 (60.88) | 820 (76.35) | 254 (23.65) | 0.0046 | 719 (66.95) | 355 (33.05) | <0.0001 |
| No | 690 (39.12) | 485 (70.29) | 205 (29.71) | 377 (54.64) | 313 (45.36) | ||
| HIV voluntary testing # | |||||||
| Yes | 1362 (77.17) | 1021 (74.96) | 341 (25.04) | 0.1586 | 870 (63.88) | 492 (36.12) | 0.0133 |
| No | 403 (22.83) | 288 (71.46) | 115 (28.54) | 230 (57.07) | 173 (42.93) | ||
| Mental Health Problems | Anal Sex Role “1” (n = 467) | Anal Sex Role “0.5” (n = 1122) | Anal Sex Role “0” (n = 182) | F/χ2 | p |
|---|---|---|---|---|---|
| Score/N (%) | Score/N (%) | Score/N (%) | |||
| Anxiety | |||||
| Mean ± SD | 42.09 ± 10.20 | 42.94 ± 10.75 | 44.25 ± 11.55 | 2.80 | 0.0611 a |
| Median | 42.00 | 42.00 | 42.00 | ||
| Yes (≥50) | 104 (22.27) | 300 (26.74) | 57 (31.32) | 6.3652 | 0.0415 b |
| No (<50) | 363 (77.73) | 822 (73.26) | 125 (68.68) | ||
| Depression | |||||
| Mean ± SD | 12.78 ± 8.93 | 14.02 ± 9.62 | 16.31 ± 11.71 | 8.83 | 0.0002 a |
| Median | 12.00 | 12.00 | 13.50 | ||
| Yes (≥16) | 153 (32.76) | 433 (38.59) | 84 (46.15) | 10.7378 | 0.0047 b |
| No (<16) | 314 (67.24) | 689 (61.41) | 98 (53.85) |
| Independent Variables | B | S.E. | Wald | p Value | OR | 95%CI for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Anal sex role | |||||||
| “1” | (reference) | ||||||
| “0.5” | 0.2900 | 0.1374 | 4.4534 | 0.0348 | 1.336 | 1.021 | 1.750 |
| “0” | 0.5783 | 0.2073 | 7.7802 | 0.0053 | 1.783 | 1.188 | 2.677 |
| Educational level | |||||||
| College or graduate or above | (reference) | ||||||
| Senior high | 0.3117 | 0.1322 | 5.5604 | 0.0184 | 1.366 | 1.054 | 1.770 |
| Junior high or below | 0.8225 | 0.1664 | 24.4415 | <0.0001 | 2.276 | 1.643 | 3.154 |
| Female sexual partners in the last six months | |||||||
| 0 | (reference) | ||||||
| ≥1 | 0.5404 | 0.1478 | 13.3661 | 0.0003 | 1.717 | 1.285 | 2.293 |
| Frequency of seeking partners on the Internet in the last 6 months | |||||||
| Never | (reference) | ||||||
| Sometimes or occasionally | −0.0636 | 0.1221 | 0.2715 | 0.6023 | 0.938 | 0.739 | 1.192 |
| Often | 0.5836 | 0.2207 | 6.9947 | 0.0082 | 1.793 | 1.163 | 2.763 |
| Diagnosed with STD in the past six months | |||||||
| No | (reference) | ||||||
| Yes | 0.5953 | 0.1933 | 9.4873 | 0.0021 | 1.813 | 1.242 | 2.649 |
| HIV voluntary counseling | |||||||
| No | (reference) | ||||||
| Yes | −0.2628 | 0.1159 | 5.1445 | 0.0233 | 0.769 | 0.613 | 0.965 |
| Independent Variables | B | S.E. | Wald | p Value | OR | 95%CI for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Anal sex role | |||||||
| “1” | (reference) | ||||||
| “0.5” | 0.2693 | 0.1278 | 4.4395 | 0.0351 | 1.309 | 1.019 | 1.682 |
| “0” | 0.5787 | 0.1971 | 8.6243 | 0.0033 | 1.784 | 1.212 | 2.625 |
| Area | |||||||
| Rural | (reference) | ||||||
| Urban | −0.4127 | 0.1182 | 12.1885 | 0.0005 | 0.662 | 0.525 | 0.834 |
| Casual sexual partners in the last six months | |||||||
| 0 | (reference) | ||||||
| ≥1 | 0.2772 | 0.1202 | 5.3133 | 0.0212 | 1.319 | 1.042 | 1.670 |
| Female sexual partners in the last six months | |||||||
| 0 | (reference) | ||||||
| ≥1 | 0.5432 | 0.1467 | 13.7131 | 0.0002 | 1.721 | 1.291 | 2.295 |
| Diagnosed with STD in the past six months | |||||||
| No | (reference) | ||||||
| Yes | 0.5144 | 0.1941 | 7.0253 | 0.0080 | 1.673 | 1.143 | 2.447 |
| Frequency of seeking partners on the Internet in the last 6 months | |||||||
| Never | (reference) | ||||||
| Sometimes or occasionally | 0.0124 | 0.1233 | 0.0101 | 0.9198 | 1.012 | 0.795 | 1.289 |
| Often | 0.6664 | 0.2287 | 8.4909 | 0.0036 | 1.947 | 1.244 | 3.048 |
| Frequency of alcohol use in the last month | |||||||
| Never | (reference) | ||||||
| Occasionally | −0.1704 | 0.1177 | 2.0954 | 0.1477 | 0.843 | 0.670 | 1.062 |
| Daily | 0.8594 | 0.2725 | 9.9499 | 0.0016 | 2.362 | 1.385 | 4.029 |
| Frequency of condom use when having anal sex with men | |||||||
| Never | (reference) | ||||||
| Occasionally | −0.5143 | 0.1966 | 6.8456 | 0.0089 | 0.598 | 0.407 | 0.879 |
| Always | −0.4524 | 0.1871 | 5.8425 | 0.0156 | 0.636 | 0.441 | 0.918 |
| HIV voluntary counseling | |||||||
| No | (reference) | ||||||
| Yes | −0.5317 | 0.1104 | 23.1937 | <0.0001 | 0.588 | 0.473 | 0.730 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Zhong, X.; Lu, Z.; Peng, B.; Zhang, Y.; Liang, H.; Dai, J.; Zhang, J.; Huang, A. Anxiety and Depression Associated with Anal Sexual Practices among HIV-Negative Men Who Have Sex with Men in Western China. Int. J. Environ. Res. Public Health 2020, 17, 464. https://doi.org/10.3390/ijerph17020464
Liu J, Zhong X, Lu Z, Peng B, Zhang Y, Liang H, Dai J, Zhang J, Huang A. Anxiety and Depression Associated with Anal Sexual Practices among HIV-Negative Men Who Have Sex with Men in Western China. International Journal of Environmental Research and Public Health. 2020; 17(2):464. https://doi.org/10.3390/ijerph17020464
Chicago/Turabian StyleLiu, Jiaxiu, Xiaoni Zhong, Zhuo Lu, Bin Peng, Yan Zhang, Hao Liang, Jianghong Dai, Juying Zhang, and Ailong Huang. 2020. "Anxiety and Depression Associated with Anal Sexual Practices among HIV-Negative Men Who Have Sex with Men in Western China" International Journal of Environmental Research and Public Health 17, no. 2: 464. https://doi.org/10.3390/ijerph17020464
APA StyleLiu, J., Zhong, X., Lu, Z., Peng, B., Zhang, Y., Liang, H., Dai, J., Zhang, J., & Huang, A. (2020). Anxiety and Depression Associated with Anal Sexual Practices among HIV-Negative Men Who Have Sex with Men in Western China. International Journal of Environmental Research and Public Health, 17(2), 464. https://doi.org/10.3390/ijerph17020464