Addition of Probiotics to Anti-Obesity Therapy by Percutaneous Electrical Stimulation of Dermatome T6. A Pilot Study

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Methodology
2.1. Subjects of Study
2.2. Percutaneous Electrical Stimulation (PENS)
2.3. Hypocaloric Diet, Exercise, and Probiotics Administration
2.4. Variables
2.4.1. Anthropometric Variables
2.4.2. Analysis of Microbiota
2.5. Statistics
3. Results
3.1. Characterization of the Obese Population with Gut Dysbiosis
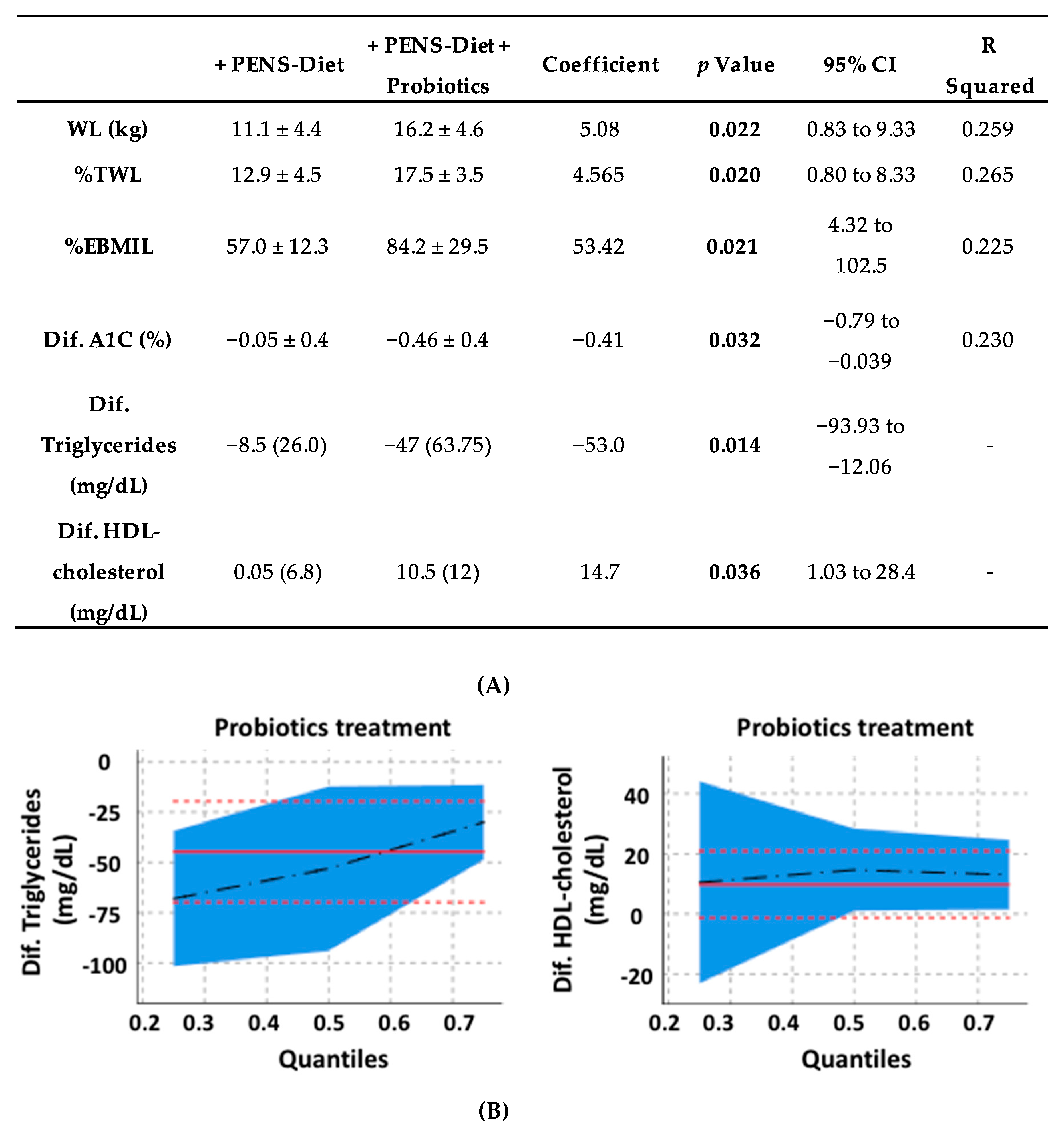
3.2. Reduction of the Body Weight and CV Risk Factors by PENS-Diet +/− Probiotics
3.3. Microbiota Modifications after PENS-Diet +/− Probiotics
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metab. Clin. Exp. 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO consultation; World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- Su, X.; Peng, D. Emerging functions of adipokines in linking the development of obesity and cardiovascular diseases. Mol. Biol. Rep. 2020. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, A.; Silva, H.M.; Moore, K.J.; Schmidt, A.M.; Fisher, E.A. Leukocyte heterogeneity in adipose tissue, including in obesity. Circ. Res. 2020, 126, 1590–1612. [Google Scholar] [CrossRef] [PubMed]
- Kyle, T.K.; Dhurandhar, E.J.; Allison, D.B. Regarding obesity as a disease: Evolving policies and their implications. Endocrinol. Metab. Clin. N. Am. 2016, 45, 511–520. [Google Scholar] [CrossRef]
- Normand, M.P.; Gibson, J.L. Behavioral approaches to weight management for health and wellness. Pediatr. Clin. N. Am. 2020, 67, 537–546. [Google Scholar] [CrossRef]
- Van Der Pal, F.; Van Balken, M.R.; Heesakkers, J.P.F.A.; Debruyne, F.M.; Bemelmans, B.L. Percutaneous tibial nerve stimulation in the treatment of refractory overactive bladder syndrome: Is maintenance treatment necessary? BJU Int. 2006, 97, 547–550. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Llavero, C. Long-term effect of percutaneous electrical neurostimulation of dermatome T6 for Appetite reduction and weight loss in obese patients. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, 212–215. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Llavero, C.; Smith, W. Percutaneous electrical neurostimulation of dermatome T6 for short-term weight loss in overweight and obese patients: Effect on ghrelin levels, glucose, lipid, and hormonal profile. Surg. Laparosc. Endosc. Percutaneous Tech. 2017, 27, 241–247. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Oller, I.; Diez, M.; Zubiaga, L.; Arroyo, A.; Calpena, R. Percutaneous electrical neurostimulation of dermatome T6 for appetite reduction and weight loss in morbidly obese patients. Obes. Surg. 2013, 24, 205–211. [Google Scholar] [CrossRef]
- Schroeder, B.O. Fight them or feed them: How the intestinal mucus layer manages the gut microbiota. Gastroenterol. Rep. (Oxf.) 2019, 7, 3–12. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef]
- Thursby, E.; Juge, N. Introduction to the human gut microbiota. Biochem. J. 2017, 474, 1823–1836. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Ma, L.; Ma, Y.; Zhang, F.; Zhao, C.; Nie, Y. Insights into the role of gut microbiota in obesity: Pathogenesis, mechanisms, and therapeutic perspectives. Protein Cell 2018, 9, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Moschen, A.R.; Kaser, A. Obesity and the Microbiota. Gastroenterology 2009, 136, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Duncan, S.H.; Lobley, G.; Holtrop, G.; Ince, J.; Johnstone, A.M.; Louis, P.; Flint, H. Human colonic microbiota associated with diet, obesity and weight loss. Int. J. Obes. (Lond.) 2008, 32, 1720–1724. [Google Scholar] [CrossRef] [PubMed]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.; Krakoff, J. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am. J. Clin. Nutr. 2011, 94, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Cerdó, T.; García-Santos, J.A.; Bermúdez, M.G.; Campoy, C. The Role of Probiotics and Prebiotics in the Prevention and Treatment of Obesity. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6470608/ (accessed on 14 February 2020).
- Wang, Z.-B.; Xin, S.-S.; Ding, L.-N.; Ding, W.-Y.; Hou, Y.-L.; Liu, C.-Q.; Zhang, X. The potential role of probiotics in controlling overweight/obesity and associated metabolic parameters in adults: A systematic review and meta-analysis. Evid. Based Complement. Altern. Med. 2019, 2019, 3862971. [Google Scholar] [CrossRef]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef]
- Mabire, L.; Mani, R.; Liu, L.; Mulligan, H.; Baxter, G.D. The influence of age, sex and body mass index on the effectiveness of brisk walking for obesity management in adults: A systematic review and meta-analysis. J. Phys. Act. Health 2017, 14, 389–407. [Google Scholar] [CrossRef]
- Choo, J.M.; Leong, L.E.X.; Rogers, G.B. Sample storage conditions significantly influence faecal microbiome profiles. Sci. Rep. 2015, 5, 16350. [Google Scholar] [CrossRef]
- Ramírez, E.; Picatoste, B.; González-Bris, A.; Oteo, M.; Cruz, F.; Caro-Vadillo, A.; Egido, J.; Tuñón, J.; Morcillo, M. Ángel; Lorenzo, O. Sitagliptin improved glucose assimilation in detriment of fatty-acid utilization in experimental type-II diabetes: Role of GLP-1 isoforms in Glut4 receptor trafficking. Cardiovasc. Diabetol. 2018, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Hamady, M.; Lozupone, C.; Turnbaugh, P.J.; Ramey, R.R.; Bircher, J.S.; Schlegel, M.L.; Tucker, T.A.; Schrenzel, M.D.; Knight, R.; et al. Evolution of mammals and their gut microbes. Science 2008, 320, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.R. The Ribosomal Database Project (RDP-II): Sequences and tools for high-throughput rRNA analysis. Nucleic Acids Res. 2004, 33, D294–D296. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Glycemic targets: Standards of medical care in diabetes. Diabetes Care 2018, 41, S55–S64. [Google Scholar] [CrossRef]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H.; Hoes, A.W.; Jennings, C.S.; Landmesser, U.; Pedersen, T.R.; et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef]
- Brahe, L.K.; Astrup, A.; Larsen, L.H. Can we prevent obesity-related metabolic diseases by dietary modulation of the gut microbiota? Adv. Nutr. 2016, 7, 90–101. [Google Scholar] [CrossRef]
- CDC. Adult Overweight and Obesity. Available online: https://www.cdc.gov/obesity/adult/index.html (accessed on 5 February 2020).
- Flegal, K.M.; Kit, B.K.; Orpana, H.M.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef]
- Abdel-Kadar, M. Percutaneous Electrical Neurostimulation (PENS) of dermatome t6 with an ambulatory self-applied patch vs PENS of dermatome T6 with conventional procedure: Effect on appetite and weight loss in moderately obese patients. Obes. Surg. 2016, 26, 2899–2905. [Google Scholar] [CrossRef]
- Huang, X.; Fan, X.; Ying, J.; Chen, S. Emerging trends and research foci in gastrointestinal microbiome. J. Transl. Med. 2019, 17, 1–11. [Google Scholar] [CrossRef]
- Grigorescu, I.; Dumitrascu, D. Implication of gut microbiota in diabetes mellitus and obesity. Acta Endocrinol. (Buchar.) 2016, 12, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Roselli, M.; Devirgiliis, C.; Zinno, P.; Guantario, B.; Finamore, A.; Rami, R.; Perozzi, G. Impact of supplementation with a food-derived microbial community on obesity-associated inflammation and gut microbiota composition. Genes Nutr. 2017, 12, 25. [Google Scholar] [CrossRef] [PubMed]
- Montandon, S.A.; Jornayvaz, F.R. Effects of antidiabetic drugs on gut microbiota composition. Genes 2017, 8, 250. [Google Scholar] [CrossRef] [PubMed]
- Kovatcheva-Datchary, P.; Nilsson, A.; Akrami, R.; Lee, Y.S.; De Vadder, F.; Arora, T.; Hallén, A.; Martens, E.; Björck, I.; Bäckhed, F. Dietary fiber-induced improvement in glucose metabolism is associated with increased abundance of prevotella. Cell Metab. 2015, 22, 971–982. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.-C.; Lee, M.-C.; Lee, C.-C.; Ng, K.-S.; Hsu, Y.-J.; Tsai, T.-Y.; Young, S.-L.; Lin, J.-S.; Huang, C.-C. Effect of lactobacillus plantarum TWK10 on exercise physiological adaptation, performance, and body composition in healthy humans. Nutrients 2019, 11, 2836. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-M.; Wei, L.; Chiu, Y.-S.; Hsu, Y.-J.; Tsai, T.-Y.; Wang, M.-F.; Huang, C.-C. Lactobacillus plantarum TWK10 supplementation improves exercise performance and increases muscle mass in mice. Nutrients 2016, 8, 205. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Jung, S.-R.; Lee, S.-Y.; Lee, N.-K.; Paik, H.-D.; Lim, S. Lactobacillus plantarum strain Ln4 attenuates diet-induced obesity, insulin resistance, and changes in hepatic mRNA levels associated with glucose and lipid metabolism. Nutrients 2018, 10, 643. [Google Scholar] [CrossRef]
- Crovesy, L.; Ostrowski, M.; Ferreira, D.M.T.P.; Rosado, E.L.; Soares-Mota, M. Effect of Lactobacillus on body weight and body fat in overweight subjects: A systematic review of randomized controlled clinical trials. Int. J. Obes. (Lond.) 2017, 41, 1607–1614. [Google Scholar] [CrossRef]
- Sun, Q.; Zhang, Y.; Li, Z.; Yan, H.; Li, J.; Wan, X. Mechanism analysis of improved glucose homeostasis and cholesterol metabolism in high-fat-induced obese mice treated with La-SJLH001 via transcriptomics and culturomics. Food Funct. 2019, 10, 3556–3566. [Google Scholar] [CrossRef]
- Minami, J.-I.; Iwabuchi, N.; Tanaka, M.; Yamauchi, K.; Xiao, J.-Z.; Abe, F.; Sakane, N. Effects of Bifidobacterium breve B-3 on body fat reductions in pre-obese adults: A randomized, double-blind, placebo-controlled trial. Biosci. Microbiota Food Health 2018, 37, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Kondo, S.; Xiao, J.-Z.; Satoh, T.; Odamaki, T.; Takahashi, S.; Sugahara, H.; Yaeshima, T.; Iwatsuki, K.; Kamei, A.; Abe, K. Antiobesity effects ofBifidobacterium breveStrain B-3 Supplementation in a mouse model with high-fat diet-induced obesity. Biosci. Biotechnol. Biochem. 2010, 74, 1656–1661. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Morita, H.; Hashimoto, H.; Hosoda, M.; Kurisaki, J.-I.; Ouwehand, A.C.; Isolauri, E.; Benno, Y.; Salminen, S. Intestinal Bifidobacterium species induce varying cytokine production. J. Allergy Clin. Immunol. 2002, 109, 1035–1036. [Google Scholar] [CrossRef] [PubMed]
- Cani, P.D.; Possemiers, S.; Van De Wiele, T.; Guiot, Y.; Everard, A.; Rottier, O.; Geurts, L.; Naslain, D.; Neyrinck, A.M.; Lambert, D.M.; et al. Changes in gut microbiota control inflammation in obese mice through a mechanism involving GLP-2-driven improvement of gut permeability. Gut 2009, 58, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Bubnov, R.V.; Babenko, L.; Lazarenko, L.; Mokrozub, V.V.; Demchenko, O.A.; Nechypurenko, O.V.; Spivak, M.Y. Comparative study of probiotic effects of Lactobacillus and Bifidobacteria strains on cholesterol levels, liver morphology and the gut microbiota in obese mice. EPMA J. 2017, 8, 357–376. [Google Scholar] [CrossRef]
- Nagpal, R.; Wang, S.; Woods, L.C.S.; Seshie, O.; Chung, S.T.; Shively, C.A.; Register, T.C.; Craft, S.; McClain, D.A.; Yadav, H. Comparative Microbiome signatures and short-chain fatty acids in mouse, rat, non-human primate, and human feces. Front. Microbiol. 2018, 9, 2897. [Google Scholar] [CrossRef]
- Lin, H.V.; Frassetto, A.; Kowalik, E.J.; Nawrocki, A.R.; Lu, M.M.; Kosinski, J.R.; Hubert, J.A.; Szeto, D.; Yao, X.; Forrest, G.; et al. Butyrate and propionate protect against diet-induced obesity and regulate gut hormones via free fatty acid receptor 3-independent mechanisms. PLoS ONE 2012, 7, e35240. [Google Scholar] [CrossRef]
- Geerlings, S.Y.; Kostopoulos, I.; De Vos, W.M.; Belzer, C. Akkermansia muciniphila in the human gastrointestinal tract: When, where, and how? Microorganisms 2018, 6, 75. [Google Scholar] [CrossRef]
- Everard, A.; Belzer, C.; Geurts, L.; Ouwerkerk, J.P.; Druart, C.; Bindels, L.B.; Guiot, Y.; Derrien, M.; Muccioli, G.G.; Delzenne, N.M.; et al. Cross-talk between Akkermansia muciniphila and intestinal epithelium controls diet-induced obesity. Proc. Natl. Acad. Sci. USA 2013, 110, 9066–9071. [Google Scholar] [CrossRef]
- Shin, N.-R.; Lee, J.-C.; Lee, H.-Y.; Kim, M.-S.; Whon, T.W.; Lee, M.-S.; Bae, J.-W. An increase in theAkkermansiaspp. population induced by metformin treatment improves glucose homeostasis in diet-induced obese mice. Gut 2013, 63, 727–735. [Google Scholar] [CrossRef]
- Li, J.; Lin, S.; Vanhoutte, P.M.; Woo, C.W.; Xu, A. Akkermansia muciniphila protects against atherosclerosis by preventing metabolic endotoxemia-induced inflammation in Apoe-/- Mice. Circulation 2016, 133, 2434–2446. [Google Scholar] [CrossRef]
- Clifton, L.; Birks, J.S.; Clifton, D. Comparing different ways of calculating sample size for two independent means: A worked example. Contemp. Clin. Trials Commun. 2018, 13, 100309. [Google Scholar] [CrossRef] [PubMed]
- Giner-Bernal, L.; Ruiz-Tovar, J.; Violeta, J.; Mercader, M.; Miralles, J.; Calpena, R.; Arroyo, A. Plasma ghrelin levels after percutaneous electrical nerve stimulation of dermatome T6 for the treatment of obesity. Endocrinol. Diabetes Nutr. 2020, 67, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Sobaler, A.M.L.; Aparicio, A.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Serra-Majem, L.; Varela-Moreiras, G.; Ortega, R.M. Overweight and general and abdominal obesity in a representative sample of Spanish adults: Findings from the ANIBES study. BioMed Res. Int. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Population (n = 20) | PENS-Diet (n = 10) | PENS-Diet + Probiotics (n = 10) | T(df)/U Value | p Value | |
|---|---|---|---|---|---|
| Age (years) | 44.7 ± 8.2 | 45.2 ± 8.9 | 44.3 ± 7.8 | 0.24 | 0.813 |
| Females/Males | 14/6 | 7/3 | 7/3 | - | >0.999 |
| Body weight (kg) | 87.8 ± 8.4 | 84.6 ± 5.1 | 91.1 ± 10.1 | −1.82 (18) | 0.085 |
| BMI (kg/m2) | 32.2 (5.3) | 32.2 (2.76) | 33.0 (6.82) | 48.0 | 0.912 |
| Systolic blood pressure (mmHg) | 137.5 (20.0) | 140.0 (20.0) | 130.0 (22.5) | 41.5 | 0.529 |
| Diastolic blood pressure (mmHg) | 80.0 (8.75) | 80.0 (6.25) | 80.0 (10.0) | 46.0 | 0.796 |
| Fasting glucose (mg/dL) | 95.5 (24.5) | 96.5 (29.7) | 95.5 (20.2) | 48.0 | 0.912 |
| A1C (%) | 5.5 ± 0.7 | 5.4 ± 0.7 | 5.6 ± 0.7 | −0.61 (18) | 0.544 |
| Triglycerides (mg/dL) | 148.5 (60.7) | 156.0 (96.2) | 147.0 (42.5) | 49.5 | >0.999 |
| Total cholesterol (mg/dL) | 199.9 ± 44.0 | 204.9 ± 52.4 | 195.0 ± 35.9 | 0.49 (18) | 0.628 |
| LDL-cholesterol (mg/dL) | 102.0 (57.0) | 114.6 (79.0) | 107.0 (44.2) | 48.0 | 0.912 |
| HDL-cholesterol (mg/dL) | 45.0 (55.1) | 47.7 (22.7) | 44.5 (15.0) | 38.0 | 0.393 |
| Total Population (log NGC/g) | PENS-Diet (n = 10) | PENS-Diet + Probiotics (n = 10) | T(df)/U Value | p Value | Reference Range (log NGC/g) | |
|---|---|---|---|---|---|---|
| Firmicutes phylum | 8.3 ± 0.86 | 8.2 ± 0.94 | 8.4 ± 0.81 | −0.49 (18) | 0.630 | 8.5–11.0 |
| Lactobacillus spp | 4.9 ± 1.13 | 4.8 ± 1.47 | 5.0 ± 0.7 | −0.5 (18) | 0.619 | 4.5–7.0 |
| Faecalibacterium sp | 6.2 ± 1.09 | 6.0 ± 1.25 | 6.5 ± 0.89 | −1.04 (18) | 0.308 | 7.0–9.0 |
| Roseburia spp | 6.7 (1.08) | 6.6 (1.75) | 6.9 (0.85) | 33.5 | 0.218 | 6.5–8.5 |
| Bacillus sp | 1.9 ± 0.82 | 2.0 ± 1.0 | 1.9 ± 0.67 | 0.27 (18) | 0.979 | 0–4.0 |
| Staphylococcus spp | 3.0 ± 0.62 | 3.1 ± 0.64 | 2.9 ± 0.62 | 0.67 (18) | 0.509 | 2.5–5.0 |
| Veillonella spp | 4.5 ± 0.86 | 4.4 ± 1.06 | 4.6 ± 0.63 | −0.61 (18) | 0.547 | 4.5–7.0 |
| Clostridium (Cocc) | 8.2 (1.05) | 7.9 (1.7) | 8.4 (0.9) | 28.5 | 0.105 | 7.0–9.0 |
| Clostridium (Perf) | 3.8 ± 1.19 | 3.7 ± 1.51 | 3.9 ± 0.83 | −0.23 (18) | 0.814 | 0–5.0 |
| Enterococcus spp | 5.9 (1.20) | 5.6 (1.67) | 6.2 (1.05) | 28.5 | 0.105 | 6.0–8.5 |
| Bacteroidetes phylum | 7.5 (1.63) | 8.1 (1.87) | 7.5 (1.0) | 40.0 | 0.481 | 8.0–11.0 |
| Prevotella spp | 6.7 (3.7) | 5.1 (4.1) | 7.3 (4.5) | 47.5 | 0.853 | 5.0–8.5 |
| Bacteroides spp | 7.1 ± 1.26 | 7.4 ± 1.16 | 6.7 ± 1.33 | 1.18 (18) | 0.252 | 7.5–9.0 |
| Firmicutes/Bacteroidetes | 0.5 ± 0.4 | 0.5 ± 0.4 | 0.46 ± 0.3 | 0.37 (18) | 0.714 | 0.1–0.3 |
| Proteobacteria phylum | 5.7 (1.89) | 6.0 (1.37) | 5.0 (1.29) | 39.0 | 0.436 | 3.0–7.0 |
| Escherichia coli | 4.5 ± 1,81 | 4.5 ± 1.79 | 4.6 ± 1.92 | −0.18 (18) | 0.859 | 4.5–7.0 |
| Pseudomonas spp | 1.0 (1.45) | 1.0 (1.42) | 1.0 (1.5) | 45.5 | 0.739 | 0–4.0 |
| Campylobacter spp | 1.0 (<0.001) | 1.0 (<0.001) | 1.0 (0.73) | 45.0 | 0.739 | 0–3.5 |
| Helicobacter spp | 2.4 (2.1) | 1.9 (2.2) | 2.4 (1.95) | 48.0 | 0.912 | 0–3.5 |
| Fusobacteria phylum | 2.79 ± 1.24 | 2.42 ± 1.26 | 3.16 ± 1.15) | −1.36 (18) | 0.188 | 0–4.5 |
| Fusobacterium nucleatum | 2.79 ± 1.24 | 2.42 ± 1.26 | 3.16 ± 1.15) | −1.36 (18) | 0.188 | 0–4.5 |
| Actinobacteria phylum | 4.41 ± 2.28 | 4.34 ± 2.78 | 4.48 ± 1.79 | −0.14 (18) | 0.891 | 6.5–9.0 |
| Bifidobacterium spp | 3.85 ± 1.96 | 3.8 ± 2.4 | 3.9 ± 1.6 | −0.11 (18) | 0.913 | 5.5–7.5 |
| Verrucomicrobia phylum | 2.6 (3.65) | 1.8 (2.3) | 3.7 (3.47) | 30.0 | 0.143 | 5.5–9.0 |
| Akkermansia muciniphila | 2.4 (3.33) | 1.7 (2.1) | 3.4 (3.2) | 29.0 | 0.123 | 5.0–8.5 |
| Baseline | + PENS-Diet | T(df)/W Value | p Value | |
| Body weight (kg) | 84.6 ± 5.1 | 73.5 ± 3.7 | 7.91 (9) | <0.001 |
| BMI (kg/m2) | 32.2 (2.76) | 28.0 (1.6) | 0.00 | 0.005 |
| Systolic blood pressure (mmHg) | 140.0 (20.0) | 120.0 (2.5) | 0.00 | 0.018 |
| Diastolic blood pressure (mmHg) | 80.0 (6.25) | 70.0 (20.0) | 7.5 | 0.038 |
| Fasting glucose (mg/dL) | 96.5 (29.7) | 88.5 (25.0) | 0.00 | 0.005 |
| A1C (%) | 5.4 ± 0.7 | 5.3 ± 0.5 | 0.36 (9) | 0.723 |
| Triglycerides (mg/dL) | 156.0 (96.2) | 138.5 (80.9) | 0.00 | 0.005 |
| Total cholesterol (mg/dL) | 204.9 ± 52.4 | 195.9 ± 46.5 | 1.75 (9) | 0.004 |
| LDL-cholesterol (mg/dL) | 114.6 (79.0) | 132.5 (78.25) | 21.0 | 0.507 |
| HDL-cholesterol (mg/dL) | 47.7 (22.7) | 51.5 (24.9) | 5.0 | 0.798 |
| Baseline | +PENS-Diet + probiotics | T(df)/W value | p value | |
| Body weight (kg) | 91.1 ± 10.1 | 74.9 ± 6.7 | 11.09 (9) | <0.001 |
| BMI (kg/m2) | 33.0 (6.82) | 26.3 (4.3) | 0.00 | 0.005 |
| Systolic blood pressure (mmHg) | 130.0 (22.5) | 120.0 (12.5) | 0.00 | 0.011 |
| Diastolic blood pressure (mmHg) | 80.0 (10.0) | 80.0 (15.0) | 0.00 | 0.041 |
| Fasting glucose (mg/dL) | 95.5 (20.2) | 84.0 (11.5) | 6.00 | 0.028 |
| A1C (%) | 5.6 ± 0.7 | 5.1 ± 0.4 | 3.63 (9) | 0.012 |
| Triglycerides (mg/dL) | 147.0 (42.5) | 85.5 (38.7) | 0.0 | 0.005 |
| Total cholesterol (mg/dL) | 195.0 ± 35.9 | 176.5 ± 47.2 | 1.75 (9) | 0.113 |
| LDL-cholesterol (mg/dL) | 107.0 (44.2) | 100.0 (46.2) | 13.0 | 0.139 |
| HDL-cholesterol (mg/dL) | 44.5 (15.0) | 57.0 (20.0) | 10 | 0.074 |
| +PENS-Diet | +PENS-Diet + Probiotics | T(df)/U-Value | p Value | |
|---|---|---|---|---|
| WL (kg) | 11.1 ± 4.4 | 16.2 ± 4.6 | 2.51 (18) | 0.022 |
| %TWL | 12.9 ± 4.5 | 17.5 ± 3.5 | −2.54 (18) | 0.020 |
| %EBMIL | 57.0 ± 12.3 | 84.2 ± 29.5 | −2.28 (18) | 0.021 |
| Dif. Systolic blood pressure (mmHg) | −12.5 (22.5) | −10.0 (12.5) | 43.0 | 0.631 |
| Dif. Diastolic blood pressure (mmHg) | −10.0 (10.0) | −2.5 (10.0) | 24.0 | 0.052 |
| Dif. Fasting glucose (mg/dL) | −7.0 (11.0) | −13.0 (16.5) | 31.0 | 0.165 |
| Dif. A1C (%) | −0.05± 0.4 | −0.46± 0.4 | 2.32 (18) | 0.032 |
| Dif. Triglycerides (mg/dL) | −8.5 (26.0) | −47.0 (63.75) | 11.0 | 0.002 |
| Dif. Total cholesterol (mg/dL) | −9.0 ± 7.4 | −18.5 ± 33.3 | 0.87 (18) | 0.391 |
| Dif. LDL-cholesterol (mg/dL) | 0.5 (42.75) | −18.0 (25.5) | 26.0 | 0.075 |
| Dif. HDL-cholesterol (mg/dL) | 0.05 (6.8) | 10.5 (12) | 14.00 | 0.005 |
| Baseline | + PENS-Diet | p Value | Baseline | +PENS-Diet + Probiotics | p Value | T *(df)/U * | p * | |
|---|---|---|---|---|---|---|---|---|
| Prevotella spp | 5.10 (4.1) | 5.25 (2.9) | >0.999 | 7.30 (4.5) | 7.40 (2.5) | 0.05 | 20.5 | 0.023 |
| Bifidobacterium spp | 3.80 ± 2.4 | 3.90 ± 2.1 | 0.911 | 3.90 ± 1.6 | 5.90 ± 0.9 | 0.005 | −2.27 (18) | 0.036 |
| Akkermansia muciniphila | 1.70 (2.1) | 1.50 (2.6) | 0.151 | 3.40 (3.2) | 4.80 (1.7) | 0.033 | 13.5 | 0.004 |
| Firmicutes/Bacteroidetes | 0.50 ± 0.4 | 0.40 ± 0.3 | 0.480 | 0.46 ± 0.3 | 0.10 ± 0.5 | 0.019 | 2.17 (18) | 0.043 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzo, O.; Crespo-Yanguas, M.; Hang, T.; Lumpuy-Castillo, J.; Hernández, A.M.; Llavero, C.; García-Alonso, M.; Ruiz-Tovar, J. Addition of Probiotics to Anti-Obesity Therapy by Percutaneous Electrical Stimulation of Dermatome T6. A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 7239. https://doi.org/10.3390/ijerph17197239
Lorenzo O, Crespo-Yanguas M, Hang T, Lumpuy-Castillo J, Hernández AM, Llavero C, García-Alonso M, Ruiz-Tovar J. Addition of Probiotics to Anti-Obesity Therapy by Percutaneous Electrical Stimulation of Dermatome T6. A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(19):7239. https://doi.org/10.3390/ijerph17197239
Chicago/Turabian StyleLorenzo, Oscar, Marta Crespo-Yanguas, Tianyu Hang, Jairo Lumpuy-Castillo, Artur M. Hernández, Carolina Llavero, MLuisa García-Alonso, and Jaime Ruiz-Tovar. 2020. "Addition of Probiotics to Anti-Obesity Therapy by Percutaneous Electrical Stimulation of Dermatome T6. A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 19: 7239. https://doi.org/10.3390/ijerph17197239
APA StyleLorenzo, O., Crespo-Yanguas, M., Hang, T., Lumpuy-Castillo, J., Hernández, A. M., Llavero, C., García-Alonso, M., & Ruiz-Tovar, J. (2020). Addition of Probiotics to Anti-Obesity Therapy by Percutaneous Electrical Stimulation of Dermatome T6. A Pilot Study. International Journal of Environmental Research and Public Health, 17(19), 7239. https://doi.org/10.3390/ijerph17197239