Upper Lip Horizontal Line: Characteristics of a Dynamic Facial Line

 and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. ULHL—Prevalence by Gender
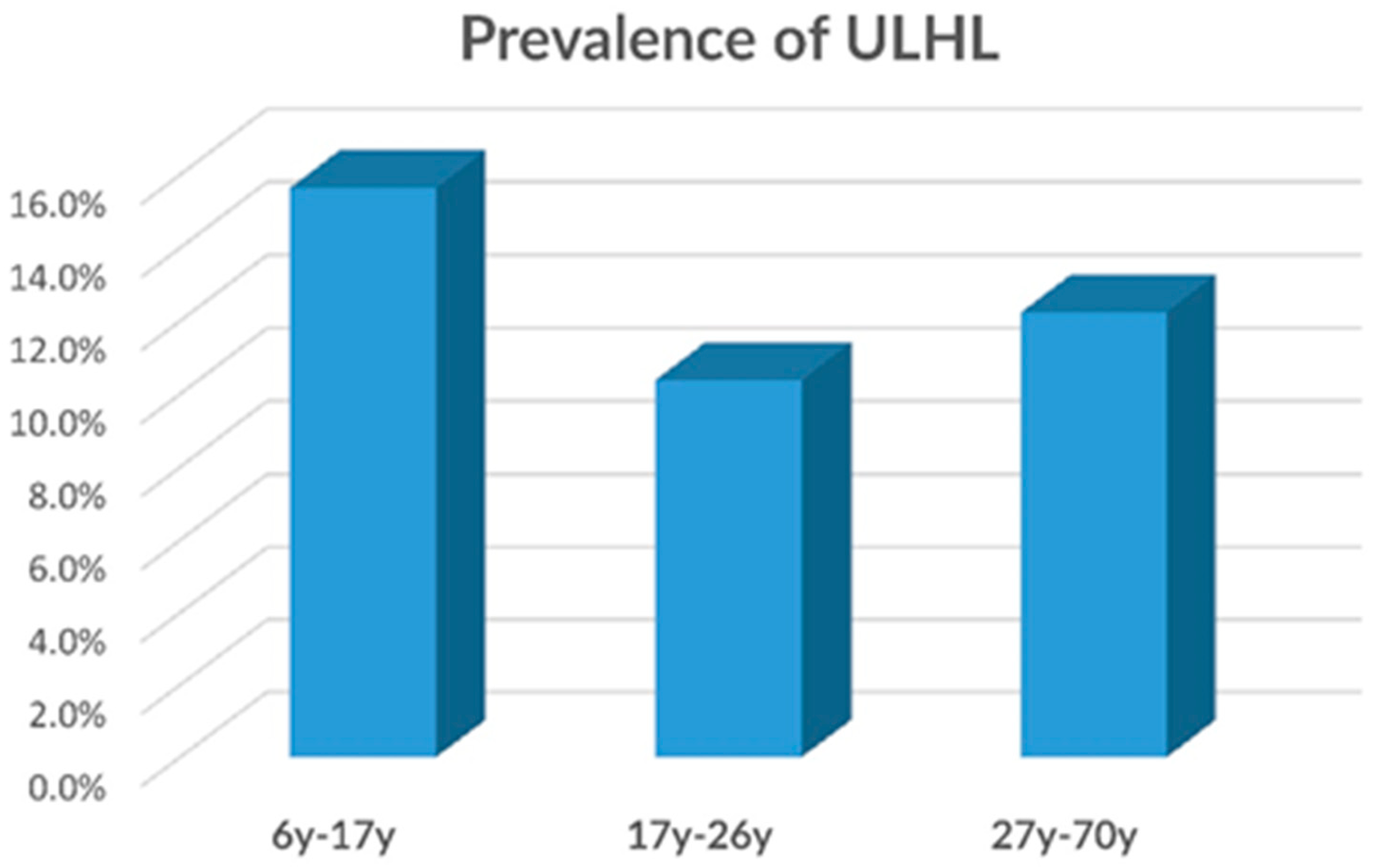
3.2. ULHL—Prevalence by Age
3.3. ULHL—Prevalence by Malocclusions
3.4. ULHL—Prevalence by Gummy Smile
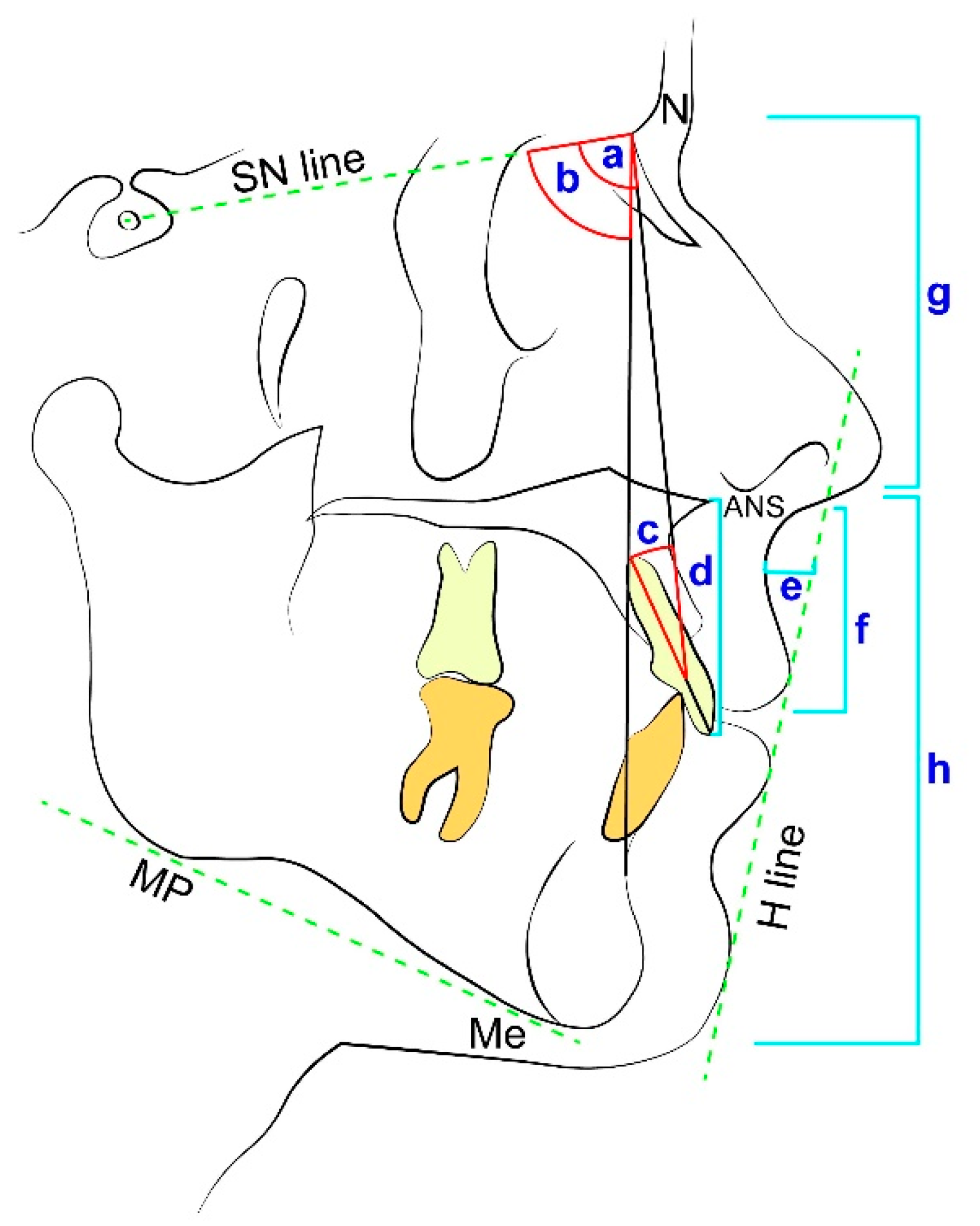
3.5. ULHL—Cephalometric Measurements
3.6. ULHL—Linear Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| Sella | Midpoint of sella turcica |
| A point | Most concave point of anterior maxilla |
| B point | Most concave point on mandibular symphysis |
| Menton | Lowest point on mandibular symphysis |
| Nasion | Most anterior point on frontonasal suture |
| ANS | The anterior nasal spine |
| SNA (°) | Sella-Nasion-A point angle |
| SNB (°) | Sella-Nasion-B point angle |
| U1 to NA (°) | Upper incisors–Nasion-A point angle |
| SN to MP (°) | Sella- Nasion to mandibular plane angle |
| N-ANS/N-Me | Nasion-Anterior nasal spine/Nasion-Menton |
| ANS-Me/N-Me | Anterior nasal spine-Menton/Naion-Menton |
| Mandibular plane (MP) | The plane connecting Gonion to Gnathion at the inferior border of the mandible |
| H line | Drawn tangent to the soft tissue chin and the upper lip |
References
- Naini, F.B.B.; Moss, J.P.P.; Gill, D.S.S. The enigma of facial beauty: Esthetics, proportions, deformity, and controversy. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Auger, T.A.; Turley, P.K. The female soft tissue profile as presented in fashion magazines during the 1900s: A photographic analysis. Int. J. Adult Orthod. Orthognath. Surg. 1999, 14, 7–18. [Google Scholar]
- Alkek, D.S.; GEM, S. Lip augmentation with silicone. J. Dermatol. Surg. Oncol. 1991, 17, 747–748. [Google Scholar] [CrossRef] [PubMed]
- Austin, H.W.; Weston, G.W. Rejuvenation of the aging mouth. Clin. Plast. Surg. 1992, 19, 511–524. [Google Scholar] [CrossRef]
- Ulloa, M.G. The sensuous lip. Aesthetic Plast. Surg. 1992, 16, 231–236. [Google Scholar] [CrossRef]
- Ho, L.C.Y. Augmentation cheiloplasty. Br. J. Plast. Surg. 1994, 47, 257–262. [Google Scholar] [CrossRef]
- Alfen, N.V.; Gilhuis, H.J.; Keijzers, J.P.; Pillen, S.; Van Dijk, J.P. Quantitative facial muscle ultrasound: Feasibility and reproducibility. Muscle Nerve 2013, 48, 375–380. [Google Scholar] [CrossRef]
- Martinelli, P.; Gabellini, A.S.; Gulli, M.R.; Lugaresi, E. Different clinical features of essential tremor: A 200-patient study. Acta Neurol. Scand. 1987, 75, 106–111. [Google Scholar] [CrossRef]
- Tessitore, A.; Magna, L.A.; Paschoal, J.R. Angular measurement for determining muscle tonus in facial paralysis. Pro-Fono Rev. Atualizacao Cient. 2010, 22, 119–124. [Google Scholar] [CrossRef][Green Version]
- Iblher, N.; Stark, G.B.; Penna, V. The aging perioral region—Do we really know what is happening. J. Nutr. Health Aging 2012, 16, 581–585. [Google Scholar] [CrossRef]
- Paes, E.C.; Teepen, H.J.; Koop, W.A.; Kon, M. Perioral wrinkles: Histologic differences between men and women. Aesthetic Surg. J. 2009, 29, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Beer, G.M.; Manestar, M. Prevalence of transverse upper labial crease. Eur. J. Plast. Surg. 2017, 40, 401–406. [Google Scholar] [CrossRef]
- Rohrich, R.J.; Huynh, B.; Muzaffar, A.R.; Adams, W.P., Jr.; Robinson, J.B., Jr. Importance of the depressor septi nasi muscle in rhinoplasty: Anatomic study and clinical application. Plast. Reconstr. Surg. 2000, 105, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Hwang, W.S.; Hur, M.S.; Hu, K.S.; Song, W.C.; Koh, K.S.; Baik, H.S.; Kim, S.T.; Kim, H.J.; Lee, K.J. Surface anatomy of the lip elevator muscles for the treatment of gummy smile using botulinum toxin. Angle Orthod. 2009, 79, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Homicz, M.R.; Watson, D. Review of injectable materials for soft tissue augmentation. Facial Plast. Surg. 2004, 20, 21–29. [Google Scholar] [CrossRef]
- Ishida, L.H.; Ishida, L.C.; Ishida, J.; Grynglas, J.; Alonso, N.; Ferreira, M.C. Myotomy of the Levator Labii Superioris muscle and lip repositioning: A combined approach for the correction of gummy smile. Plast. Reconstr. Surg. 2010, 126, 1014–1019. [Google Scholar] [CrossRef]
- Tonnard, P.L.; Verpaele, A.M.; Ramaut, L.E.; Blondeel, P.N. Aging of the upper lip: Part II. evidence-based rejuvenation of the upper lip—A review of 500 consecutive cases. Plast. Reconstr. Surg. 2019, 143, 1333–1342. [Google Scholar] [CrossRef]
- Nayyar, P.; Kumar, P.; Nayyar, P.V.; Singh, A. Botox: Broadening the horizon of dentistry. J. Clin. Diagn. Res. 2014, 8, ZE25. [Google Scholar]
- Hochman, M.N.; Chu, S.J.; Tarnow, D.P. Maxillary anterior papilla display during smiling: A clinical study of the interdental smile line. Int. J. Periodontics Restor. Dent. 2012, 32, 375. [Google Scholar]
- Monaco, A.; Streni, O.; Chiara Marci, M.; Marzo, G.; Gatto, R.; Giannoni, M. Gummy smile: Clinical parameters useful for diagnosis and therapeutical approach. J. Clin. Pediatr. Dent. 2005, 29, 19–25. [Google Scholar] [CrossRef]
- McLeod, C.; Fields, H.W.; Hechter, F.; Wiltshire, W.; Rody, W., Jr.; Christensen, J. Esthetics and smile characteristics evaluated by laypersons: A comparison of Canadian and US data. Angle Orthod. 2011, 81, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Orce-Romero, A.; Iglesias-Linares, A.; Cantillo-Galindo, M.; Yañez-Vico, R.M.; Mendoza-Mendoza, A.; Solano-Reina, E. Do the smiles of the world’s most influential individuals have common parameters? J. Oral Rehabil. 2013, 40, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Darwin, C. The Expression of Emotions in Animals and Man; Murray: London, UK, 1872; p. 11. [Google Scholar]
- Moskowitz, M.E.; Nayyar, A. Determinants of dental esthetics: A rational for smile analysis and treatment. Compend. Contin. Educ. Dent. 1995, 16, 1164–1166. [Google Scholar] [PubMed]
- Hungerford, E.; Beatty, M.W.; Marx, D.B.; Simetich, B.; Wee, A.G. Coverage error of commercial skin pigments as compared to human facial skin tones. J. Dent. 2013, 41, 986–991. [Google Scholar] [CrossRef]
- Williams, D.M.; Bentley, R.; Cobourne, M.T.; Gibilaro, A.; Good, S.; Huppa, C.; Matthews, N.S.; O’Higgins, L.; Patel, S.; Newton, J.T. The impact of idealised facial images on satisfaction with facial appearance: Comparing ‘ideal’and ‘average’faces. J. Dent. 2008, 36, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Naert, I.E. Patient evaluation and treatment planning. J. Dent. 1997, 25, S5–S11. [Google Scholar] [CrossRef]
- Masarei, A.G.; Sell, D.; Habel, A.; Mars, M.; Sommerlad, B.C.; Wade, A. The nature of feeding in infants with unrepaired cleft lip and/or palate compared with healthy noncleft infants. Cleft Palate-Craniofac. J. 2007, 44, 321–328. [Google Scholar] [CrossRef]
- Noiray, A.; Cathiard, M.A.; Ménard, L.; Abry, C. Test of the movement expansion model: Anticipatory vowel lip protrusion and constriction in French and English speakers. J. Acoust. Soc. Am. 2011, 129, 340–349. [Google Scholar] [CrossRef]
- Ortega, A.d.O.L.; Marques-Dias, M.J.; dos Santos, M.T.B.R.; Castro, T.; Gallottini, M. Oral motor assessment in individuals with Moebius syndrome. J. Oral Pathol. Med. 2014, 43, 157–161. [Google Scholar] [CrossRef]
- Löfqvist, A. Lip kinematics in long and short stop and fricative consonants. J. Acoust. Soc. Am. 2005, 117, 858–878. [Google Scholar] [CrossRef]
- Phillips, C.; Tulloch, C.; Dann, C. Rating of facial attractiveness. Community Dent. Oral Epidemiol. 1992, 20, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Soh, J.; Chew, M.T.; Wong, H.B. An Asian community’s perspective on facial profile attractiveness. Community Dent. Oral Epidemiol. 2007, 35, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Ahluwalia, R.; Verma, D.; Grewal, S.B.; Goel, R.; Kumar, P.S. Perioral age-related changes in smile dynamics along the vertical plane: A videographic cross-sectional study. Angle Orthod. 2013, 83, 468–475. [Google Scholar] [CrossRef]
- Vig, R.G.; Brundo, G.C. The kinetics of anterior tooth display. J. Prosthet. Dent. 1978, 39, 502–504. [Google Scholar] [CrossRef]
- Kent-Braun, J.A.; Callahan, D.M.; Fay, J.L.; Foulis, S.A.; Buonaccorsi, J.P. Muscle weakness, fatigue, and torque variability: Effects of age and mobility status. Muscle Nerve 2014, 49, 209–217. [Google Scholar] [CrossRef]
- Zabojova, J.; Thrikutam, N.; Tolley, P.; Perez, J.; Rozen, S.M.; Rodriguez-Lorenzo, A. Relational anatomy of the mimetic muscles and its implications on free functional muscle inset in facial reanimation. Ann. Plast. Surg. 2018, 81, 203–207. [Google Scholar] [CrossRef]
- Sandulescu, T.; Spilker, L.; Rauscher, D.; Naumova, E.A.; Arnold, W.H. Morphological analysis and three-dimensional reconstruction of the SMAS surrounding the nasolabial fold. Ann. Anat. Anat. Anz. 2018, 217, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Sandulescu, T.; Franzmann, M.; Jast, J.; Blaurock-Sandulescu, T.; Spilker, L.; Klein, C.; Naumova, E.A.; Arnold, W.H. Facial fold and crease development: A new morphological approach and classification. Clin. Anat. 2019, 32, 573–584. [Google Scholar] [CrossRef]
- Peck, S.; Peck, L. Selected aspects of the art and science of facial esthetics. Semin. Orthod. 1995, 1, 105–126. [Google Scholar] [CrossRef]
- Sharma, P.K.; Sharma, P. Dental smile esthetics: The assessment and creation of the ideal smile. Semin. Orthod. 2012, 18, 193–201. [Google Scholar] [CrossRef]
- Tjan, A.H.; Miller, G.D. Some esthetic factors in a smile. J. Prosthet. Dent. 1984, 51, 24–28. [Google Scholar] [CrossRef]
- Miron, H.; Calderon, S.; Allon, D. Upper lip changes and gingival exposure on smiling: Vertical dimension analysis. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 87–93. [Google Scholar] [CrossRef] [PubMed]
Sample Availability: The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. |




{kind=link}
{kind=link}
{kind=link}
| Individuals Presenting with ULHL | ||||||
|---|---|---|---|---|---|---|
| All Group | Prevalence | Age | ||||
| N | N | % | Mean | Std | ||
| First stage group | Males | 235 | 15 | 6.4 | 17.12 | 8.149 |
| Females | 408 | 74 | 18.1 | 19.39 | 9.580 | |
| Total | 643 | 89 | 14.0 | 18.60 | 9.190 | |
| Second stage group | Males | 34 | 9 | 26.5 | 14.93 | 4.764 |
| Females | 63 | 41 | 65.1 | 17.63 | 8.678 | |
| Total | 97 | 50 | 51.5 | 16.68 | 7.623 | |
| Malocclusion | Total | |||||
|---|---|---|---|---|---|---|
| Cl I | Cl II/1 | Cl II/2 | Cl III | |||
| ULHL | N | 48 | 31 | 4 | 7 | 90 |
| % | 53.3% | 34.4% | 4.4% | 7.8% | 100.0% | |
| no-ULHL | N | 224 | 234 | 36 | 59 | 553 |
| % | 40.5% | 42.3% | 6.5% | 10.7% | 100.0% | |
| Gummy Smile | Non-Gummy Smile | Total | ||
|---|---|---|---|---|
| ULHL | N | 25 | 65 | 90 |
| % | 27.8% | 72.2% | 100.0% | |
| no-ULHL | N | 84 | 469 | 553 |
| % | 15.2% | 84.8% | 100.0% | |
| Total | N | 109 | 534 | 643 |
| % | 17.0% | 83.0% | 100.0% | |
| Cephalometric Measurement | ULHL | No ULHL | p Value | 95% Confidence Interval of the Difference | |||
|---|---|---|---|---|---|---|---|
| MEAN | STD | MEAN | STD | Lower | Upper | ||
| SNA (°) | 81.84 | 4.11 | 81.26 | 4.18 | NS | −1.09 | 2.26 |
| SNB (°) | 78.14 | 3.51 | 78.65 | 3.69 | NS | −1.96 | 0.94 |
| U1 to NA (°) | 26.86 | 7.40 | 25.37 | 9.52 | NS | −1.94 | 4.91 |
| SN to MP (°) | 33.95 | 5.61 | 33.51 | 7.01 | NS | −2.11 | 2.99 |
| N-ANS/N-Me (%) | 44.62 | 3.08 | 42.40 | 3.15 | 0.001 | 0.96 | 3.47 |
| ANS-Me/N-Me (%) | 55.36 | 3.08 | 57.64 | 3.12 | >0.001 | −3.53 | −1.03 |
| Incisor-maxilla height (mm) | 26.00 | 3.97 | 27.98 | 3.26 | 0.009 | −3.45 | −0.51 |
| Upper lip height (mm) | 19.42 | 2.45 | 23.06 | 3.05 | >0.001 | −4.76 | −2.53 |
| Sulcus depth (mm) | 6.54 | 2.21 | 5.40 | 1.93 | 0.008 | 0.30 | 1.97 |
| Model | 95% Confidence Interval for B | ||
|---|---|---|---|
| Beta | Lower | Upper | |
| Upper lip height (mm) | 0.535 | 0.057 | 0.107 |
| Sulcus depth (mm) | −0.394 | −0.128 | −0.057 |
| Gender | −0.213 | −0.393 | −0.054 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vardimon, A.D.; Shpack, N.; Wasserstein, A.; Skyllouriotou, M.; Strauss, M.; Geron, S.; Sadan, N.; Levartovsky, S.; Sarig, R. Upper Lip Horizontal Line: Characteristics of a Dynamic Facial Line. Int. J. Environ. Res. Public Health 2020, 17, 6672. https://doi.org/10.3390/ijerph17186672
Vardimon AD, Shpack N, Wasserstein A, Skyllouriotou M, Strauss M, Geron S, Sadan N, Levartovsky S, Sarig R. Upper Lip Horizontal Line: Characteristics of a Dynamic Facial Line. International Journal of Environmental Research and Public Health. 2020; 17(18):6672. https://doi.org/10.3390/ijerph17186672
Chicago/Turabian StyleVardimon, Alexander D, Nir Shpack, Atalia Wasserstein, Marilena Skyllouriotou, Morris Strauss, Silvia Geron, Noa Sadan, Shifra Levartovsky, and Rachel Sarig. 2020. "Upper Lip Horizontal Line: Characteristics of a Dynamic Facial Line" International Journal of Environmental Research and Public Health 17, no. 18: 6672. https://doi.org/10.3390/ijerph17186672
APA StyleVardimon, A. D., Shpack, N., Wasserstein, A., Skyllouriotou, M., Strauss, M., Geron, S., Sadan, N., Levartovsky, S., & Sarig, R. (2020). Upper Lip Horizontal Line: Characteristics of a Dynamic Facial Line. International Journal of Environmental Research and Public Health, 17(18), 6672. https://doi.org/10.3390/ijerph17186672