The Impact of Overweight and Obesity on Plantar Pressure in Children and Adolescents: A Systematic Review


 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
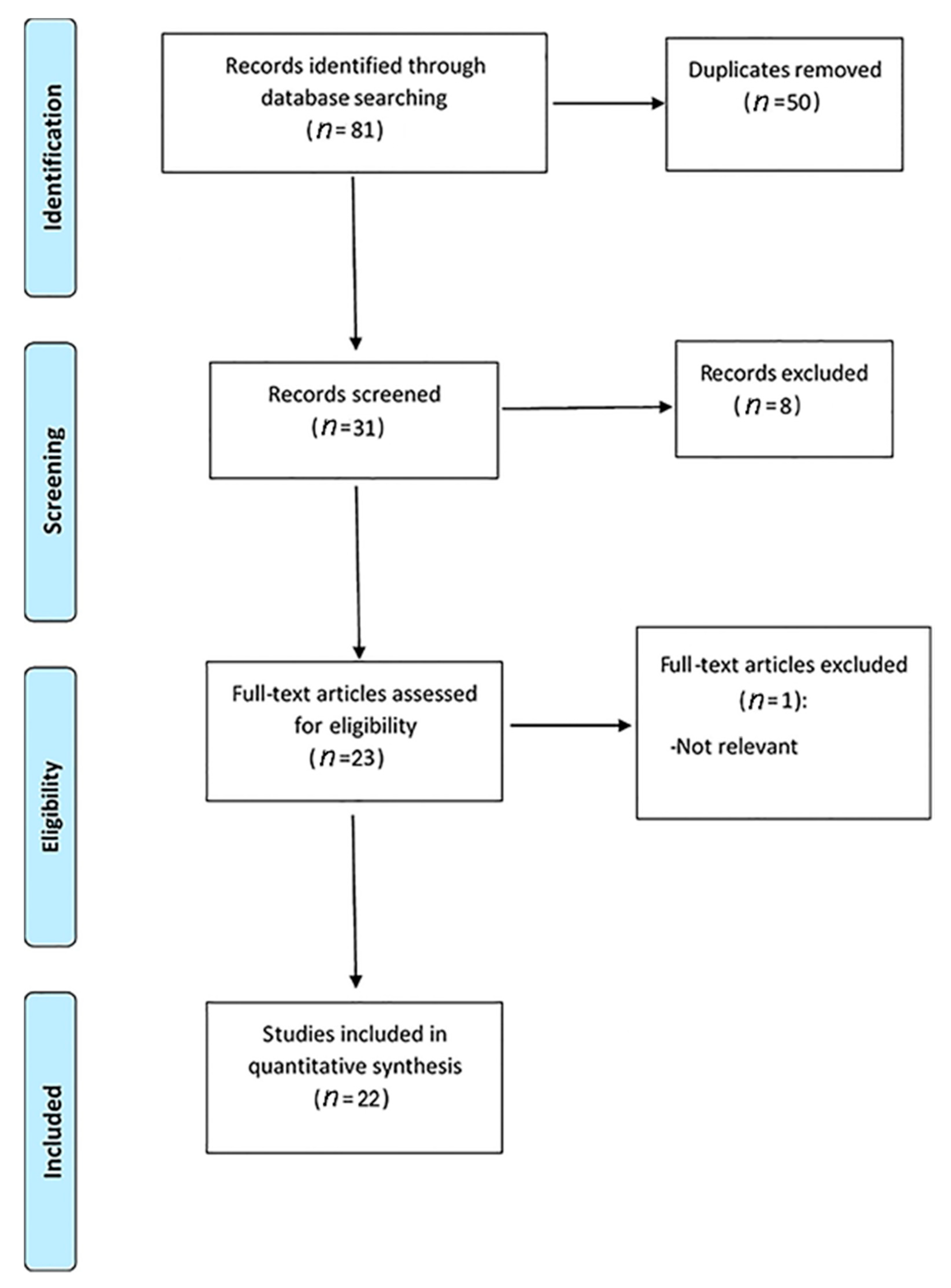
2. Materials and Methods
3. Results
3.1. Plantar Pressure during Walking/Running
3.2. Plantar Pressure during Balance Test
3.3. Static and Dynamic Plantar Assessments
3.4. Temporary Mass Increases Versus Long-Term Mass Increase and Plantar Pressure
3.5. Plantar Pressure and Fat Pad Thickness
3.6. Plantar Pressure and Foot Sensitivity
3.7. Plantar Pressure and Type of the Foot
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Obesity Data and Statistics. Available online: http://www.euro.who.int/en/health-topics/noncommunicable-diseases/obesity/data-and-statistics (accessed on 5 May 2020).
- De Onis, M.; Blössner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- De Vita, P.; Hortobágyi, T. Obesity is not associated with increased knee joint torque and power during level walking. J. Biomech. 2003, 36, 1355–1362. [Google Scholar] [CrossRef]
- Hills, A.P.; Parker, A.W. Gait characteristics of obese children. Arch. Phys. Med. Rehabil. 1991, 72, 403–407. [Google Scholar] [CrossRef] [PubMed]
- McGraw, B.; McClenaghan, B.A.; Williams, H.G.; Dickerson, J.; Ward, D.S. Gait and postural stability in obese and nonobese prepubertal boys. Arch. Phys. Med. Rehabil. 2000, 81, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Park, D.-J. Comparison of Foot Structure, Function, Plantar Pressure and Balance Ability According to the Body Mass Index of Young Adults. Osong Public Health Res. Perspect. 2019, 10, 102–107. [Google Scholar] [CrossRef]
- Kathirgamanathan, B.; Silva, P.; Fernandez, J. Implication of obesity on motion, posture and internal stress of the foot: An experimental and finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 47–54. [Google Scholar] [CrossRef]
- Fink, P.W.; D’Hondt, E.; Shultz, S.P.; Lenoir, M.; Hills, A.P. Multifractal analysis differentiates postural sway in obese and nonobese children. Motor Control 2019, 23, 262–271. [Google Scholar] [CrossRef]
- Leidecker, E.; Kellermann, P.; Tiszberger, M.G.; Molics, B.; Bohner-Beke, A.; Nyárády, J.; Kránicz, J. Analysis of plantar pressure patterns among obese population. Orv. Hetil. 2016, 157, 1919–1925. [Google Scholar] [CrossRef][Green Version]
- Telfer, S.; Bigham, J.J. The influence of population characteristics and measurement system on barefoot plantar pressures: A systematic review and meta-regression analysis. Gait Posture 2019, 67, 269–276. [Google Scholar] [CrossRef]
- Buldt, A.K.; Allan, J.J.; Landorf, K.B.; Menz, H.B. The relationship between foot posture and plantar pressure during walking in adults: A systematic review. Gait Posture 2018, 62, 56–67. [Google Scholar] [CrossRef]
- Vieira, T.N.; Mesquita, P.R.; Neri, S.G.R.; de David, A.C. Plantar pressure distribution during running in early childhood. Gait Posture 2018, 65, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Franco, P.S.; Moro, C.F.; Figueiredo, M.M.; Azevedo, R.R.; Ceccon, F.G.; Carpes, F.P. Within and between-days repeatability and variability of plantar pressure measurement during walking in children, adults and older adults. Adv. Rheumatol. 2018, 58, 15. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Kasović, M.; Zvonar, M. Association between the levels of physical activity and plantar pressure in 6-14-year-old children. PeerJ 2020, 8, e8551. [Google Scholar] [CrossRef]
- Walsh, T.P.; Butterworth, P.A.; Urquhart, D.M.; Cicuttini, F.M.; Landorf, K.B.; Wluka, A.E.; Michael Shanahan, E.; Menz, H.B. Increase in body weight over a two-year period is associated with an increase in midfoot pressure and foot pain. J. Foot Ankle Res. 2017, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Neri, S.G.R.; Gadelha, A.B.; Correia, A.L.M.; Pereira, J.C.; de David, A.C.; Lima, R.M. Obesity is Associated With Altered Plantar Pressure Distribution in Older Women. J. Appl. Biomech. 2017, 33, 323–329. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S.A. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12. [Google Scholar]
- da Santos, C.M.C.; de Pimenta, C.A.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Latino-Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; Miranda-Aparicio, D.; Molina-Molina, A.; Plaza-Florido, A.; Migueles, J.H.; Mora-Gonzalez, J.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Rodriquez-Ayllon, M.; Solis-Urra, P.; et al. Effects of Exercise on Plantar Pressure during Walking in Children with Overweight/Obesity. Med. Sci. Sport. Exerc. 2020, 52, 654–662. [Google Scholar] [CrossRef]
- Mesquita, P.R.; Neri, S.G.R.; Lima, R.M.; Carpes, F.P.; de David, A.C. Childhood obesity is associated with altered plantar pressure distribution during running. Gait Posture 2018, 62, 202–205. [Google Scholar] [CrossRef]
- Steinberg, N.; Rubinstein, M.; Nemet, D.; Ayalon, M.; Zeev, A.; Pantanowitz, M.; Brosh, T.; Eliakim, A. Effects of a Program for Improving Biomechanical Characteristics During Walking and Running in Children Who Are Obese. Pediatr. Phys. Ther. 2017, 29, 330–340. [Google Scholar] [CrossRef]
- Song-Hua, Y.; Lu, W.; Kuan, Z. Effects of different movement modes on plantar pressure distribution patterns in obese and non-obese Chinese children. Gait Posture 2017, 57, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Zhang, K.; Tan, G.; Yang, J.; Liu, Z. Effects of obesity on dynamic plantar pressure distribution in Chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.; Carlsohn, A.; Mueller, J.; Baur, H.; Mayer, F. Influence of Obesity on Foot Loading Characteristics in Gait for Children Aged 1 to 12 Years. PLoS ONE 2016, 11, e0149924. [Google Scholar] [CrossRef]
- Riddiford-Harland, D.L.; Steele, J.R.; Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Baur, L.A. Does participation in a physical activity program impact upon the feet of overweight and obese children? J. Sci. Med. Sport 2016, 19, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Riddiford-Harland, D.L.; Steele, J.R.; Cliff, D.P.; Okely, A.D.; Morgan, P.J.; Jones, R.A.; Baur, L.A. Lower activity levels are related to higher plantar pressures in overweight children. Med. Sci. Sports Exerc. 2015, 47, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Cousins, S.D.; Morrison, S.C.; Drechsler, W.I. Foot loading patterns in normal weight, overweight and obese children aged 7 to 11 years. J. Foot Ankle Res. 2013, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Mickle, K.J.; Steele, J.R.; Munro, B.J. Does excess mass affect plantar pressure in young children? Int. J. Pediatr. Obes. 2006, 1, 183–188. [Google Scholar] [CrossRef]
- Dowling, A.M.; Steele, J.R.; Baur, L.A. Does obesity influence foot structure and plantar pressure patterns in prepubescent children? Int. J. Obes. 2001, 25, 845–852. [Google Scholar] [CrossRef]
- Pau, M.; Galli, M.; Crivellini, M.; Albertini, G. Relationship between Obesity and Plantar Pressure Distribution in Youths with Down Syndrome. Am. J. Phys. Med. Rehabil. 2013, 92, 889–897. [Google Scholar] [CrossRef]
- Dowling, A.M.; Steele, J.R.; Baur, L.A. What are the effects of obesity in children on plantar pressure distributions? Int. J. Obes. 2004, 28, 1514–1519. [Google Scholar] [CrossRef] [PubMed]
- Filippin, N.T.; Bacarin, T.d.A.; Lobo da Costa, P.H. Comparison of Static Footprints and Pedobarography in Obese and Non-obese Children. Foot Ankle Int. 2008, 29, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Leban, B.; Corona, F.; Gioi, S.; Nussbaum, M.A. School-based screening of plantar pressures during level walking with a backpack among overweight and obese schoolchildren. Ergonomics 2016, 59, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Pau, M.; Leban, B.; Pau, M. Alterations in the Plantar Pressure Patterns of Overweight and Obese Schoolchildren Due to Backpack Carriage. J. Am. Podiatr. Med. Assoc. 2013, 103, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Riddiford-Harland, D.L.; Steele, J.R.; Baur, L.A. Are the feet of obese children fat or flat? Revisiting the debate. Int. J. Obes. 2011, 35, 115–120. [Google Scholar] [CrossRef]
- Riddiford-Harland, D.L.; Steele, J.R.; Baur, L. Medial midfoot fat pad thickness and plantar pressures: Are these related in children? Int. J. Pediatr. Obes. 2011, 6, 261–266. [Google Scholar] [CrossRef]
- Mickle, K.J.; Steele, J.R.; Munro, B.J. The Feet of Overweight and Obese Young Children: Are They Flat or Fat? Obesity 2006, 14, 1949–1953. [Google Scholar] [CrossRef]
- da Rocha, E.S.; Bratz, D.T.K.; Gubert, L.C.; de David, A.; Carpes, F.P. Obese children experience higher plantar pressure and lower foot sensitivity than non-obese. Clin. Biomech. 2014, 29, 822–827. [Google Scholar] [CrossRef]
- Cimolin, V.; Capodaglio, P.; Cau, N.; Galli, M.; Pau, M.; Patrizi, A.; Tringali, G.; Sartorio, A. Foot-type analysis and plantar pressure differences between obese and nonobese adolescents during upright standing. Int. J. Rehabil. Res. 2016, 39, 87–91. [Google Scholar] [CrossRef]
- Cavanagh, P.R.; Rodgers, M.M. The arch index: A useful measure from footprints. J. Biomech. 1987, 20, 547–551. [Google Scholar] [CrossRef]
- Stolzman, S.; Irby, M.B.; Callahan, A.B.; Skelton, J.A. Pes planus and paediatric obesity: A systematic review of the literature. Clin. Obes. 2015, 5, 52–59. [Google Scholar] [CrossRef]
- Teasdale, N.; Hue, O.; Marcotte, J.; Berrigan, F.; Simoneau, M.; Doré, J.; Marceau, P.; Marceau, S.; Tremblay, A. Reducing weight increases postural stability in obese and morbid obese men. Int. J. Obes. 2007, 31, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Moga, M.; Preda, G.; Marceanu, L.; Miclaus, R.; Bagiu, N. Lifestyle factors related to bone mineral density in postmenopausal women. J. Environ. Prot. Ecol. 2008, 1, 67–69. [Google Scholar]


{kind=link}
| Authors/Country/Year and Month of Publication | Number of Participants | Group Comparison | Plantar Pressure System | Method for Determining Plantar Pressure | Plantar Pressure Variables | Significant Findings (Group Comparisons) |
|---|---|---|---|---|---|---|
| Fink et al./USA/2019 April [8] | 22 children with O/NW | Group one: 11 children with O (height 1.59 ± 0.09 m, weight 64.3 ± 13.8 kg) Group two: 11 children with NW (height 1.51 ± 0.16 m, weight 43.2 ± 13.9 kg) | Plantar pressure distribution system (EMED-SF; Novel GmbH, Munich, Germany) | Static balance tests (Two 30 s static balance tests: eyes open followed by eyes closed) | Displacement of centre of pressure (COP); Euclidean distance | Group one: ↑ Persistence for small oscillations ↓ Proprioceptive ability |
| Molina-Garcia et al./Spain/2020 March [19] | 70 children with O/OW | Group one: 39 children (performed 13-week exercise programme BMI 25.59 (25.2 to 25.99)) Group two: 31 children (had a usual lifestyle) BMI 25.44 (25.1 to 25.79) | Pressure platform FreeMed® Pro (Sensormedica, Rome, Italy) with 450,000 pressure sensors | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution and loading while walking) | Contact area (CA); maximal force (MF); force–time integral (FTI) 11 anatomical regions (lateral and medial rearfoot, lateral and medial midfoot; 1st, 2nd, 3rd, 4th and 5th metatarsal; hallux; 2nd to 5th toes) | Group one: ↑ MF, specifically under the lateral and medial forefoot Group two: ↑ CA ↑ FTI forefoot |
| Mesquita et al./Brazil/2018 May [20] | 42 children with O/OW/NW | Group one: 9 children with O (BMI = 22.90 ± 0.7 kg/m2) Group two: 14 children with OW (BMI = 19.21 ± 0.42 kg/m2) Group three: 19 children with NW (BMI = 15.23 ± 0.22 kg/m2) | Pressure platform Emed AT-4 (Novel GmbH, Munchen, GE; 50 Hz; 4 sensors/cm2; 415 × 255 mm) | Dynamic plantar pressure measurement (Barefoot—During running 5–10 min with a self-selected speed); | Maximum force; normalised maximum force; contact area; peak pressure under each anatomic region (6 anatomical regions: whole foot, rearfoot, midfoot, forefoot, hallux and lesser toes) | Group one: - Generated more forces, except for the hallux - BMI was positively correlated with PP for whole, midfoot and forefoot - ↑ CA under all foot areas |
| Nili Steinberg et al./Israel/2017 October [21] | 30 children with O | Group one: 10 children (Dietary Intervention during the 6-month) (BMI 25.74 ± 3.07 kg/m2) Group two: 10 children (a similar programme as group one, with additional specific exercises, in a twice-weekly training session for 1 h each) (BMI 24.25 ± 1.79 kg/m2) Group three: 10 children (with no intervention programme) (BMI 25.13 ± 4.76 kg/m2) | A portable insole system (Novell Pedar, Munich, Germany) | Dynamic plantar pressure measurement (3 different velocities of walking and 2 different velocities of running x group × pre-/postintervention) 6 areas: heel, inner medial, lateral medial, inner forefoot, lateral forefoot, and toes | Contact area; length of contact; length of contact percentile; peak pressure; Maximum force; foot pressure–time integral and Foot force–time integral | Group one: ↓ CA in walking, ↑ PP, ↑ MaxF Group two: ↓ CA, ↓ PP, ↓ MaxF, Group three: ↑ CA, ↓ PP in walking and ↑ PP in running, ↓ MaxF in walking |
| Song-Hua et al./China/2017 September [22] | 40 children with O/NW | Group one: 20 children with O (BMI 28.13 ± 3.40 kg/m2) Group two: 20 children with NW (BMI 17.44 ± 1.57 kg/m2) | Plantar pressure mat (RSscan International, Belgium) | Dynamic plantar pressure measurement (Barefoot—During three movements: natural comfortable walking used in everyday activities, slow running, such as jogging and fast running; 50 m race) | Plantar pressure (at 10 anatomic regions); subphases of stance phase; peak pressure; arch index and angle of the foot axis | Group one has the most significant values while jogging: ↑ PP in most of the plantar regions ↑ AI |
| Song-Hua et al./China/2013 January [23] | 100 prepubescent children with O/NW | Group one: 50 children with O (BMI of 23.68 ± 3.00 kg/m2) Group two: 50 children with NW (BMI of 17.08 ± 1.25 kg/m2) | The system of foot scan plantar pressure (RSscan International, Olen, Belgium), with a plate of 0.578 m/0.418 m, 4096 resistive sensors and a resolution of 4 sensors/cm2 | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution and loading while walking) | Subphases during foot–ground contact duration; peak pressures; time to peak pressures and pressure rate in 10 plantar regions; foot arch index; relative regional impulses (RIR) under three plantar regions; foot balance and foot axis angle | Group one: ↑ Midstance duration ↓ Propulsion duration ↑ AI for the left foot, and the left and right foot axis angle ↑ PP under the 4th and 5th metatarsal heads, and midfoot ↓ Stability while walking - Have a flat foot model |
| Mueller et al./Germany/2016 February [24] | 7575 Children with O/OW/NW | Group one: 371 children with O (BMI 23.1 ± 3.3 kg/m2) Group two: 746 children with OW (BMI 19.7 ± 1.9 kg/m2) Group three: 6458 children with NW (BMI 16.4 ± 1.5 kg/m2) | Pressure platform (Emed X1, Novel GmbH, Munich, Germany), mounted in the walkway | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution and loading while walking) | Contact area; arch index (AI); force–time integral; peak pressure 5 anatomical regions: toes, forefoot, medial midfoot, lateral midfoot and hindfoot | Group one and two: ↑ CA ↑ AI ↑ Peak pressure midfoot and forefoot ↑ Force–time integral of the force–time Group one compared to group three: the midfoot loading was 1.48 higher in the 1-year group and 3.49 higher in the 10-year group |
| Riddiford-Harland et al./Australia/2016 January [25] | 34 children with O | Group one: 24 children (performed a 10-week physical activity programme) Group two: 10 children (10 children did not practice any physical activity) (BMI z-score for all: 2.63 ± 0.61) | AT-4 Emed system (Novel GmbH, Munich, Germany) and ActiGraph | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution while walking) | Mean peak pressure footprints; peak pressure; pressure–time integral 10 anatomical regions | Group one and two: ↓ BMI (z-score) ↑ Foot length; ↑ Foot height; ↑ PTI—lateral midfoot and forefoot - No differences in plantar pressure parameters between the two groups |
| Riddiford-Harland et al./Australia/2015 February [26] | 73 children with O/OW | One group: 73 children with O/OW (BMI z-score = 2.7 ± 0.7) | AT-4 Emed (25 Hz, 4 sensors/cm2; Novel GmbH, Munich, Germany) and ActiGraph 7164 accelerometer (ActiGraph, Pensacola, FL) | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution while walking) | Mean peak pressure footprints; peak pressure; 10 anatomical regions | PP generated beneath the forefoot during walking were inversely correlated with time spent in different intensity levels of physical activity |
| Cousins et al./UK/2013 August [27] | 100 children with O/OW/NW | Group one: 22 children with O (BMI = 24.16 ± 3.14 kg/m2) Group two: 22 children with OW (BMI = 19.17 ± 1.28 kg/m2) Group three: 56 children with NW (BMI = 15.63 ± 2.04 kg/m2) | MatScan® 3150 5 m platform (TekScan, USA) Portable ultrasound (SonoSite ® 180 PLUS system, Washington, USA) with a linear transducer (10–5 MHz, maximum depth of 7 cm) | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution while walking) | Peak pressure; peak force; normalised peak force; pressure–time integral; force–time integral. (At six regions of the plantar foot—lateral heel, medial heel, midfoot, 1st metatarsophalangeal joint, 2nd–5th metatarsophalangeal joint and hallux) | Group one and two: Under the midfoot and 2nd–5th metatarsal regions: ↑ PP, ↑ PTI, ↑ FTI |
| Mickle et al./Australia/2006 [28] | 34 children with O/NW | Group one: 17 children with O (BMI 18.59 ± 1.3 kg/m2) Group two: 17 children with NW (BMI 15.79 ± 0.7 kg/m2) | The pressure platform AT-4 (25 Hz; Novel GmbH, Munich, Germany) | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution while walking) | Peak pressure; maximum force; maximum contact area; Pressure–time integral and force–time integral. (heel, midfoot, forefoot, hallux and toes 2–5) | Group one: ↑ PP, ↑ CA of the whole foot, heel, midfoot and forefoot ↑ PTI and ↑ FTI in the midfoot region, |
| Dowling et al./Australia/2001 January [29] | 26 children with O/NW | Group one: 13 children with O (BMI 25.5 ± 2.9 kg/m2) Group two: 13 children with NW (BMI 16.9 ± 1.2 kg/m2) | One podograph and mini-Emed1 system (Novel GmbH, Munich, Germany) | Static and dynamic plantar pressure measurement Barefoot | Fingerprint angle and Chippaux–Smirak index; peak static and dynamic force; peak static and dynamic area; peak static and dynamic pressure. (For the whole foot). Dynamic rearfoot and forefoot force. 2 anatomic regions | Group one: ↓ footprint angle ↑ Chippaux–Smirak index ↑ Peak dynamic forefoot pressures ↑ Peak forces ↑ Peak contact area ↑ Forefoot contact area |
| Pau et al./Italy/2013 October [30] | 118 children and adolescents (with Down syndrome) with O/OW/NW | Group one: 59 children and adolescents with O/OW (BMI 26.7 ± 3.9: male, 28.3 ± 3.9: female kg/m2) Group two: 59 children and adolescents with NW (BMI 19.6 ± 4.0: male, 18.0 ± 2.1: female kg/m2) | A pressure-sensitive carpet (Tekscan Inc, South Boston, MA) consisting of 2016 detection elements embedded in a 42 × 48 matrix | Static plantar pressure measurement Barefoot | Contact area (total, rearfoot, midfoot, forefoot); arch index; peak plantar pressures (rearfoot midfoot, forefoot) 3 anatomic regions | Group one: ↑ CA (girls only)) ↑ PP (midfoot +26%, and forefoot +32%, for the males; midfoot +33%, and forefoot +37%, for the females) Group one and two: flat foot is the prevalent arch type |
| Dowling et al./Australia/2004 November [31] | 20 children with O/NW | Group one: 10 children with O (BMI 25.8 ± 3.8 kg/m2) Group two: 10 children with NW (BMI 16.8 ± 2.0 kg/m2) | Pressure platform AT-4 Emed (Novel GmbH, Munich, Germany) with 4 sensors per cm2 | Static and dynamic plantar pressure measurement Barefoot | Peak force; peak area; peak pressure; (for the total foot); force–time integral; pressure–time integral 10 anatomical regions | Group one: ↑ PF, ↑ PA, ↑ PP especially midfoot, ↑ contact area ↑ Forces over all areas of their feet, except the toes ↑ Values of plantar pressure, midfoot and 2nd head metatarsal ↑ PTI in lateral midfoot, forefoot - Flatten the midfoot |
| Taisa Filippin et al./Brazil/2008 November [32] | 20 children with O/NW | Group one: 10 children with O (BMI = 28.4 ± 2.7 kg/m2) Group two: 10 children with NW (BMI = 15.8 ± 1.9 kg/m2) | Digital planimeter (Placom -CST) and Pedar system (Novel GmbH, Munich, Germany) | Static and Dynamic plantar pressure measurement (Barefoot—The static and dynamic distribution of the plantar pressure while walking on a 10 m walkway) | Arch index; static contact area (SCA); dynamic contact area (DCA); dynamic peak pressure (DPP); dynamic maximum mean pressure (DMMP). | Group two: correlations between the static and dynamic plantar pressure parameters ↓ Arch index: obese Dynamic midfoot area was greater than the static one for both |
| Pau et al./Italy/2016 May [33] | 130 children with O/OW/NW | Group one: 65 children with O/OW (BMI 21.4 ± 2.3 kg/m2) Group two: 65 children with NW (BMI 16.7 ± 1.6 kg/m2) | A 4 m walkway with an embedded plantar pressure platform (FDM-S, Zebris Medical GmbH, Germany) was used; the platform had 2560 capacitive sensitive elements in a 64 x40 matrix, with an acquisition frequency of 100 Hz | Dynamic plantar pressure measurement (Barefoot—Plantar pressure distribution while walking with and without wearing the schoolbag) | Contact areas; arch index; Peak and mean plantar pressures (3 anatomic regions: forefoot, midfoot and rearfoot) | Group two: ↑ Mean midfoot pressure Group one: ↑ Larger contact area—all regions ↑ Dynamic arch index ↑ Mean, peak pressure midfoot and forefoot With schoolbag—↑ mean peak in forefoot and midfoot |
| Pau et al./Italy/2013 July–August [34] | 140 children with O/OW/NW | Group one: 70 children with O/OW (BMI 21.6 ± 1.9: boys, 21.3 ± 2.7: girls kg/m2) Group two: 70 children with NW (BMI 16.3 ± 1.4: boys, 16.7 ± 1.7: girls kg/m2) | Footscan 0.5 system (RSscan International, Olen, Belgium) | Static plantar pressure measurement (Barefoot—Static plantar pressure distribution with and without wearing the schoolbag) | Contact area (total, rearfoot, midfoot, forefoot); arch index; peak plantar pressures (rearfoot midfoot, forefoot) 3 anatomic regions | Group one: ↑ CA ↑ PP (in the rearfoot and midfoot by 17% and 37% in boys and 38% and 27% in girls with no significant increase in forefoot) ↑ arch index |
| Riddiford-Harland et al./Australia/2011 January [35] | 150 children with O/NW | Group one: 75 children with O (BMI 25.2 ± 3.6 kg/m2) Group two: 75 children with NW (BMI 15.9 ± 1.4 kg/m2) | Portable ultrasound (SonoSite ® 180 PLUS system, Washington, USA) with a linear transducer (10–5 MHz, maximum depth of 7 cm) | Ultrasonography of the midfoot Barefoot | The midfoot fat pad thickness in both non-weight-bearing and weight-bearing positions; Height of internal arch | Group one: ↑ Midfoot fat pad thickness ↓ Medial longitudinal arch height |
| Riddiford-Harland et al./Australia/2011 August [36] | 252 children with O/OW | One group: 252 children with O/OW (BMI 19.1 ± 4.3 kg/m2) | Portable ultrasound (SonoSite ® 180 PLUS system, Washington, USA) with a linear transducer (10–5 MHz, maximum depth of 7 cm) and the pressure platform ® Emed ® AT-4 system (Novel GmbH, Munich, Germany). | Ultrasonography of the midfoot and dynamic plantar pressure Barefoot | The midfoot fat pad thickness in both non-weight-bearing and weight-bearing positions; Contact area; Force; Peak plantar pressure. (For the 10 anatomic foot regions) | - Medial midfoot plantar fat pad thickness and medial midfoot plantar pressure were correlated with BMI - Medial midfoot plantar pressure low correlated with midfoot plantar fat pad thickness during non-weight-bearing and weight-bearing |
| Mickle et al./Australia/2006 November [37] | 38 preschool children with O/OW/NW | Group one: 19 children with O/OW (BMI 18.6 ± 1.2 kg/m2) Group two: 19 children with NW (BMI 15.7 ± 0.7 kg/m2) | Portable ultrasound system SonoSite 180 PLUS (SonoSite, Bothell, WA) with a large linear band of 38 mm, matrix transducer of 10–5 MHz, maximum depth of 7 cm). Pedograph (Suavepie, Capital Federal, Argentina) | Ultrasonography of the midfoot Barefoot | Arch index; plantar arch height; midfoot fat pad thickness in non-weight-bearing positions | Group one: ↓ Plantar arch height ↑ Arch index Group one and two: - No significant between-group differences in the thickness of the midfoot plantar fat pad |
| Da Rocha et al./Brazil/2014 August [38] | 40 children with O/NW | Group one: 20 children with O (BMI 20.67 ± 1.78 kg/m2) Group two: 20 children with NW (BMI 16.27 ± 1.61 kg/m2) | Pressure aestheometry (Semmes–Weinstein Monofilaments, San Jose, USA) and the plantar pressure portable system (Matscan, Tekscan Inc., Boston, USA), with a sampling frequency of 100 Hz | Foot sensitivity and static plantar pressure measurement (During unipedal and bipedal stance, eyes opened and barefoot) | Sensitivity scores (Semmes–Weinstein pressure aesthesiometry); plantar pressure (whole foot, rearfoot, midfoot, forefoot) 3 anatomic regions | Group one: ↓ Foot sensitivity at whole foot and midfoot ↑ Plantar pressure for whole foot and all foot regions ↑ Pressure on rearfoot |
| Cimolin et al./Italy/2016 March [39] | 18 adolescents with O/NW | Group one: 10 adolescents with O (BMI 35.45 ± 4.73 kg/m2) Group two: 8 adolescents with NW (BMI 18.67 ± 2.46 kg/m2) | The footwear system Pedar-X (Novel GmbH, Munich, Germany) in-shoe system | Static plantar pressure measurement In-shoe system—everyday sneakers corresponding to the individual’s size 8 anatomical regions (medial and lateral rearfoot, medial and lateral midfoot, hallux, medial central and lateral forefoot) | Peak pressure; peak force; contact area. Arch index (at medial and lateral rearfoot, midfoot; medial, central and lateral forefoot and hallux) | Group one: ↑ CA (on the forefoot and midfoot) - 70% had flat foot, 20% cavus foot and 10% normal foot type ↑ PP, ↑ PF for all the regions, with the exception of medial rearfoot area (similar between the two groups) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catan, L.; Amaricai, E.; Onofrei, R.R.; Popoiu, C.M.; Iacob, E.R.; Stanciulescu, C.M.; Cerbu, S.; Horhat, D.I.; Suciu, O. The Impact of Overweight and Obesity on Plantar Pressure in Children and Adolescents: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6600. https://doi.org/10.3390/ijerph17186600
Catan L, Amaricai E, Onofrei RR, Popoiu CM, Iacob ER, Stanciulescu CM, Cerbu S, Horhat DI, Suciu O. The Impact of Overweight and Obesity on Plantar Pressure in Children and Adolescents: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(18):6600. https://doi.org/10.3390/ijerph17186600
Chicago/Turabian StyleCatan, Liliana, Elena Amaricai, Roxana Ramona Onofrei, Calin Marius Popoiu, Emil Radu Iacob, Corina Maria Stanciulescu, Simona Cerbu, Delia Ioana Horhat, and Oana Suciu. 2020. "The Impact of Overweight and Obesity on Plantar Pressure in Children and Adolescents: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 18: 6600. https://doi.org/10.3390/ijerph17186600
APA StyleCatan, L., Amaricai, E., Onofrei, R. R., Popoiu, C. M., Iacob, E. R., Stanciulescu, C. M., Cerbu, S., Horhat, D. I., & Suciu, O. (2020). The Impact of Overweight and Obesity on Plantar Pressure in Children and Adolescents: A Systematic Review. International Journal of Environmental Research and Public Health, 17(18), 6600. https://doi.org/10.3390/ijerph17186600