Children with Obesity Experience Different Age-Related Changes in Plantar Pressure Distributions: A Follow-Up Study in China




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. Data Processing
2.4. Statistical Analysis
3. Results
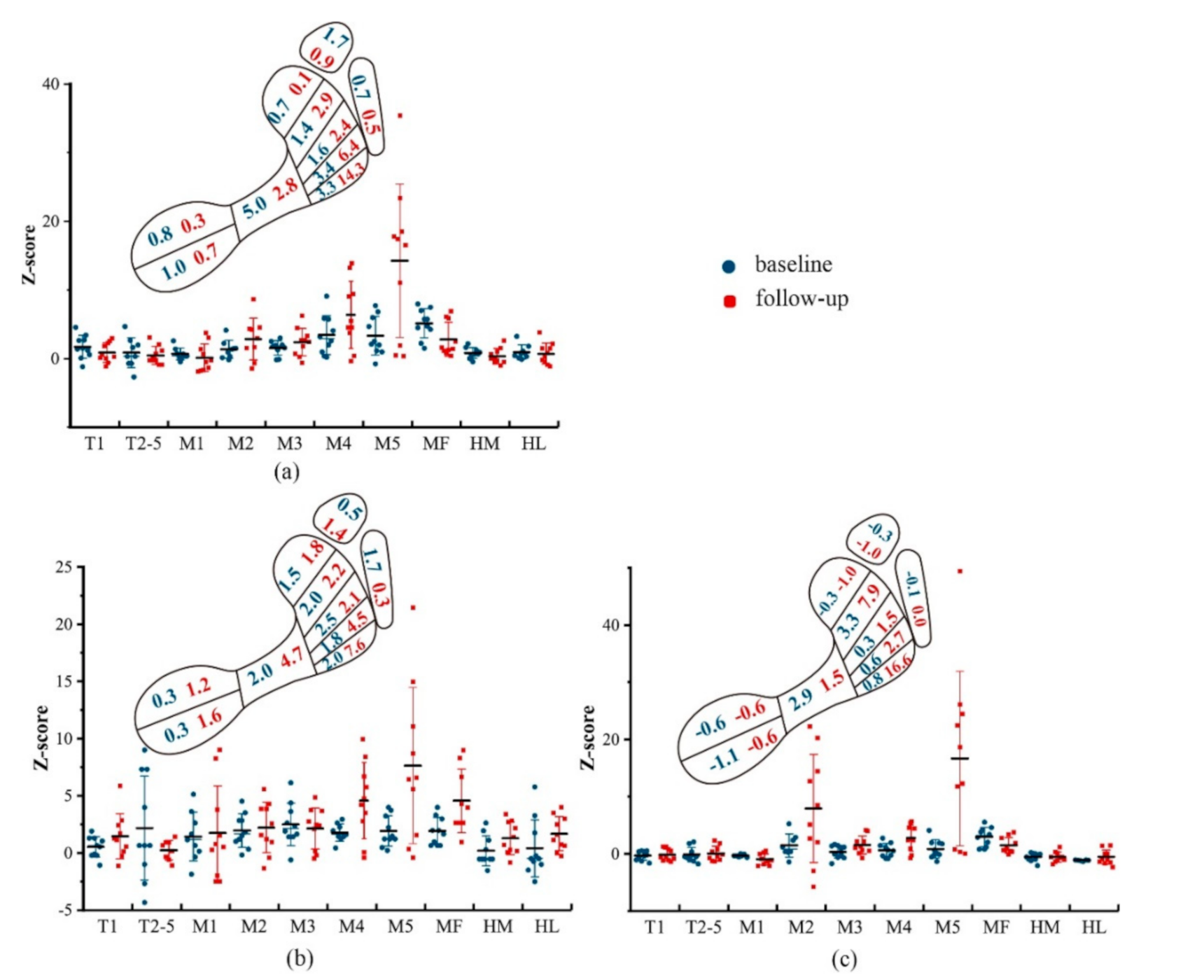
3.1. Age-Related Changes in Plantar Pressure Distributions
3.2. Age-Related Plantar Pressure Deviations in Obese Children
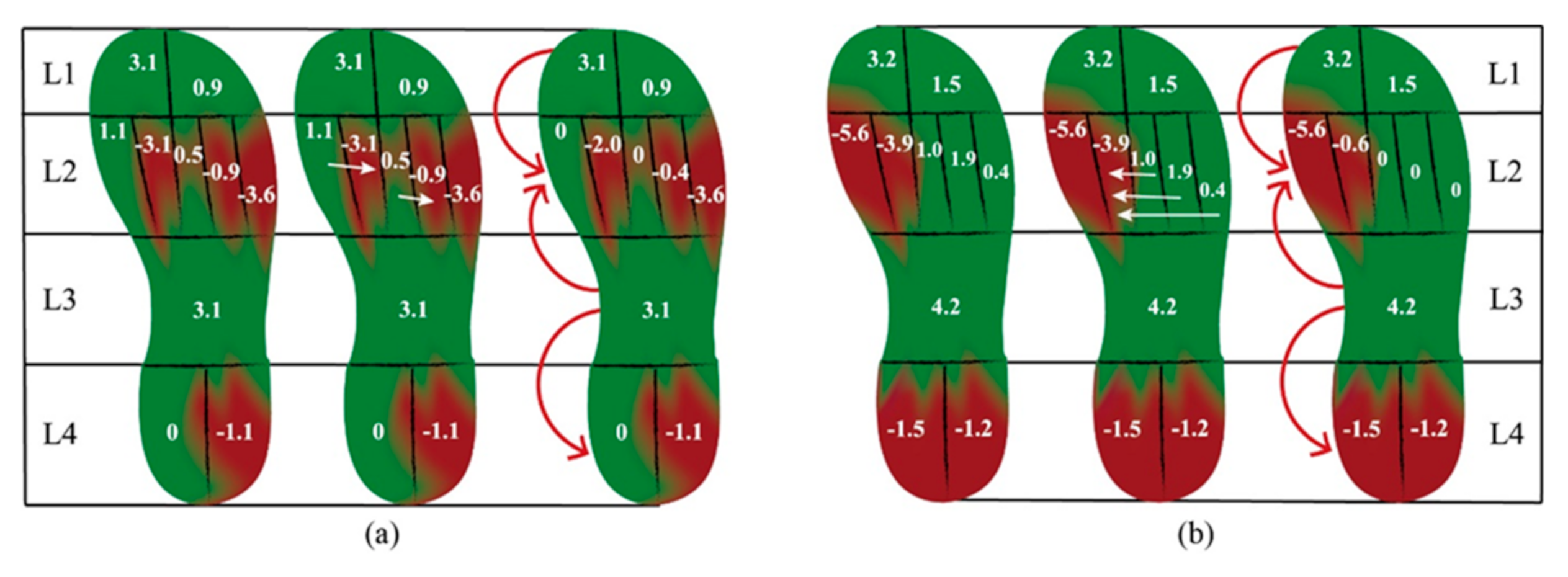
3.3. Age-Related Loading Transferences in Obese Children
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Song-Hua, Y.; Lu, W.; Kuan, Z. Effects of different movement modes on plantar pressure distribution patterns in obese and non-obese chinese children. Gait Posture 2017, 57, 28–34. [Google Scholar] [CrossRef]
- Montes-Alguacil, J.; Paez-Moguer, J.; Jimenez Cebrian, A.M.; Munoz, B.A.; Gijon-Nogueron, G.; Morales-Asencio, J.M. The influence of childhood obesity on spatio-temporal gait parameters. Gait Posture 2019, 71, 69–73. [Google Scholar] [CrossRef]
- da Rocha, E.S.; Bratz, D.T.; Gubert, L.C.; de David, A.; Carpes, F.P. Obese children experience higher plantar pressure and lower foot sensitivity than non-obese. Clin. Biomech. 2014, 29, 822–827. [Google Scholar] [CrossRef]
- Villarrasa-Sapina, I.; Serra-Ano, P.; Pardo-Ibanez, A.; Gonzalez, L.M.; Garcia-Masso, X. Relationship between body composition and vertical ground reaction forces in obese children when walking. Clin. Biomech. 2017, 41, 77–81. [Google Scholar] [CrossRef]
- Gil Madrona, P.; Romero Martinez, S.J.; Saez-Gallego, N.M.; Ordonez Camacho, X.G. Psychomotor limitations of overweight and obese five-year-old children: Influence of body mass indices on motor, perceptual, and social-emotional skills. Int. J. Environ. Res. Public Health 2019, 16, 427. [Google Scholar] [CrossRef]
- Walsh, T.P.; Butterworth, P.A.; Urquhart, D.M.; Cicuttini, F.M.; Landorf, K.B.; Wluka, A.E.; Michael Shanahan, E.; Menz, H.B. Increase in body weight over a two-year period is associated with an increase in midfoot pressure and foot pain. J. Foot Ankle Res. 2017, 10, 31. [Google Scholar] [CrossRef]
- Rubinstein, M.; Eliakim, A.; Steinberg, N.; Nemet, D.; Ayalon, M.; Zeev, A.; Pantanowitz, M.; Brosh, T. Biomechanical characteristics of overweight and obese children during five different walking and running velocities. Footwear Sci. 2017, 9, 149–159. [Google Scholar] [CrossRef]
- Mesquita, P.R.; Neri, S.G.R.; Lima, R.M.; Carpes, F.P.; de David, A.C. Childhood obesity is associated with altered plantar pressure distribution during running. Gait Posture 2018, 62, 202–205. [Google Scholar] [CrossRef]
- Yan, S.H.; Zhang, K.; Tan, G.Q.; Yang, J.; Liu, Z.C. Effects of obesity on dynamic plantar pressure distribution in chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef]
- Phethean, J.; Nester, C. The influence of body weight, body mass index and gender on plantar pressures: Results of a cross-sectional study of healthy children’s feet. Gait Posture 2012, 36, 287–290. [Google Scholar] [CrossRef]
- Kung, S.M.; Fink, P.W.; Legg, S.J.; Ali, A.; Shultz, S.P. Age-dependent variability in spatiotemporal gait parameters and the walk-to-run transition. Hum. Mov. Sci. 2019, 66, 600–606. [Google Scholar] [CrossRef]
- Demirbuken, I.; Ozgul, B.; Timurtas, E.; Yurdalan, S.U.; Cekin, M.D.; Polat, M.G. Gender and age impact on plantar pressure distribution in early adolescence. Acta Orthop. Traumatol. Turc. 2019, 53, 215–220. [Google Scholar] [CrossRef]
- Zeininger, A.; Schmitt, D.; Jensen, J.L.; Shapiro, L.J. Ontogenetic changes in foot strike pattern and calcaneal loading during walking in young children. Gait Posture 2018, 59, 18–22. [Google Scholar] [CrossRef]
- Muller, S.; Carlsohn, A.; Muller, J.; Baur, H.; Mayer, F. Static and dynamic foot characteristics in children aged 1–13 years: A cross-sectional study. Gait Posture 2012, 35, 389–394. [Google Scholar] [CrossRef]
- Mueller, S.; Carlsohn, A.; Mueller, J.; Baur, H.; Mayer, F. Influence of obesity on foot loading characteristics in gait for children aged 1 to 12 years. PLoS ONE 2016, 11, e0149924. [Google Scholar] [CrossRef]
- Bosch, K.; Rosenbaum, D. Gait symmetry improves in childhood-a 4-year follow-up of foot loading data. Gait Posture 2010, 32, 464–468. [Google Scholar] [CrossRef]
- Buldt, A.K.; Forghany, S.; Landorf, K.B.; Levinger, P.; Murley, G.S.; Menz, H.B. Foot posture is associated with plantar pressure during gait: A comparison of normal, planus and cavus feet. Gait Posture 2018, 62, 235–240. [Google Scholar] [CrossRef]
- Hofmann, U.K.; Gotze, M.; Wiesenreiter, K.; Muller, O.; Wunschel, M.; Mittag, F. Transfer of plantar pressure from the medial to the central forefoot in patients with hallux valgus. BMC Musculoskelet. Dis. 2019, 20, 149. [Google Scholar] [CrossRef]
- Group of China Obesity Task Force. Body mass index reference norm for screening overweight and obesity in chinese children and adolescence. Chin. J. Epidemiol. 2004, 25, 97–102. [Google Scholar]
- Meyers-Rice, B.; Sugars, L.; McPoil, T.; Cornwall, M.W. Comparison of three methods for obtaining plantar pressures in nonpathologic subjects. J. Am. Podiatr. Med. Assoc. 1994, 84, 499–504. [Google Scholar] [CrossRef]
- Menz, H.B. Two feet, or one person? Problems associated with statistical analysis of paired data in foot and ankle medicine. Foot 2004, 14, 2–5. [Google Scholar] [CrossRef]
- Cole, T.J.; Faith, M.S.; Pietrobelli, A.; Heo, M. What is the best measure of adiposity change in growing children: Bmi, bmi %, bmi z-score or bmi centile? Eur. J. Clin. Nutr. 2005, 59, 419–425. [Google Scholar] [CrossRef]
- Hu, M.; Zhou, N.; Xu, B.; Chen, W.; Wu, J.; Zhou, J. The mechanism of force transference in feet of children ages two to six. Gait Posture 2017, 54, 15–19. [Google Scholar] [CrossRef] [PubMed]
- A New View of Statistics. Available online: http://www.sportsci.org/resource/stats/ (accessed on 8 July 2020).
- Kasovic, M.; Stefan, L.; Zvonar, M. Foot characteristics during walking in 6–14-year-old children. Sci. Rep. 2020, 10, 9501. [Google Scholar] [CrossRef]
- Cousins, S.D.; Morrison, S.C.; Drechsler, W.I. Foot loading patterns in normal weight, overweight and obese children aged 7 to 11 years. J. Foot Ankle Res. 2013, 6, 36. [Google Scholar] [CrossRef]
- Szczepanowska-Wolowiec, B.; Sztandera, P.; Kotela, I.; Zak, M. Body weight-dependent foot loads, assessed in terms of bmi and adiposity, in school-aged children: A cross sectional study. Sci. Rep. 2020, 10, 12360. [Google Scholar] [CrossRef]
- Mahaffey, R.; Morrison, S.C.; Bassett, P.; Drechsler, W.I.; Cramp, M.C. Biomechanical characteristics of lower limb gait waveforms: Associations with body fat in children. Gait Posture 2018, 61, 220–225. [Google Scholar] [CrossRef]
- Summa, S.; De Peppo, F.; Petrarca, M.; Caccamo, R.; Carbonetti, R.; Castelli, E.; Ottavio Adorisio, D. Gait changes after weight loss on adolescent with severe obesity after sleeve gastrectomy. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2019, 15, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Bosch, K.; Gerss, J.; Rosenbaum, D. Development of healthy children’s feet-Nine-year results of a longitudinal investigation of plantar loading patterns. Gait Posture 2010, 32, 564–571. [Google Scholar] [CrossRef]
- Butterworth, P.A.; Urquhart, D.M.; Landorf, K.B.; Wluka, A.E.; Cicuttini, F.M.; Menz, H.B. Foot posture, range of motion and plantar pressure characteristics in obese and non-obese individuals. Gait Posture 2015, 41, 465–469. [Google Scholar] [CrossRef]
- Taillie, L.S.; Wang, D.; Popkin, B.M. Snacking is longitudinally associated with declines in body mass index z scores for overweight children, but increases for underweight children. J. Nutr. 2016, 146, 1268–1275. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, M.; Gabriel, R.; Aranha, J.; Neves e Castro, M.; Sousa, M.; Moreira, M. Influence of obesity and sarcopenic obesity on plantar pressure of postmenopausal women. Clin. Biomech. 2010, 25, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wen, X.X.; Huang, L.Y.; Shang, L.; Cheng, X.X.; Yan, Y.B.; Lei, W. Normal foot loading parameters and repeatability of the footscan(r) platform system. J. Foot Ankle Res. 2017, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wen, X.X.; Huang, L.Y.; Shang, L.; Yang, Z.; Yan, Y.B.; Lei, W. Reliability of the footscan(r) platform system in healthy subjects: A comparison of without top-layer and with top-layer protocols. BioMed. Res. Int. 2017, 2017, 2708712. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline | Follow-Up | p | Mean Difference | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Obese Group | |||||
| Number (n) | 10 | 10 | |||
| Age (years) | 8 | 11 | |||
| Height (cm) | 136.3 ± 4 | 160.1 ± 5.8 | 0 | 23.8 | −28.5 to −19.1 |
| Body mass (kg) | 43.4 ± 5.4 | 70.3 ± 6 | 0 | 26.9 | −32.3 to −21.5 |
| BMI (kg/m2) | 23.3 ± 2.2 | 27.5 ± 2.2 | 0 | 4.14 | −6.2 to −2.1 |
| Control Group | |||||
| Number (n) | 11 | 11 | |||
| Age (years) | 8 | 11 | |||
| Height (cm) | 126.9 ± 4.7 | 149.7 ± 5.8 | 0 | 22.82 | −27.5 to 18.1 |
| Body mass (kg) | 25.7 ± 3.7 | 39.1 ± 6.9 | 0 | 13.37 | −18.4 to −8.5 |
| BMI (kg/m2) | 15.9 ± 1.3 | 17.3 ± 2.2 | 0.081 | 1.44 | −3.1 to 0.2 |
| Follow-Up vs. Baseline in Obese Group | Follow-Up vs. Baseline in Control Group | |||||
|---|---|---|---|---|---|---|
| Follow-Up | Baseline | MD (95% CI), ES | Follow-Up | Baseline | MD (95% CI), ES | |
| PP (kPa) | ||||||
| T1 | 126.7 (48.3) a | 57.4 (20.3) | 69.3 (34.5 to 104.1), 1.87 | 96.7 (33.7) b | 37.4 (11.8) | 59.3 (34.3 to 84.4), 2.40 |
| T2–5 | 54.7 (24.6) a | 13.5 (6.5) | 41.1 (23.3 to 59.1), 2.42 | 45.6 (19.2) b | 10.9 (3.2) | 34.7 (21 to 48.3), 2.40 |
| M1 | 88.3 (36.2) a | 41.2 (10.6) | 47.1 (20.6 to 73.5), 1.81 | 85.8 (17.7) b | 33.3 (12.1) | 52.5 (38.7 to 66.2), 3.49 |
| M2 | 214.6 (91.2) a | 91.1 (22.2) | 123.5 (52.6 to 194.4), 1.86 | 129.3 (30.5) b | 67.8 (16.6) | 61.5 (39.4 to 83.7), 2.55 |
| M3 | 230.1 (98.8) a | 102.7 (17) | 127.4 (56.3 to 198.5), 1.84 | 112.6 (49) b | 77.6 (15.6) | 35 (2.6 to 67.3), 0.96 |
| M4 | 264.7 (137.2) a | 94.2 (28.4) | 170.5 (71.4 to 269.5), 1.72 | 85.7 (28.2) b | 60.4 (9.9) | 25.3 (6.5 to 44.1), 1.20 |
| M5 | 351.2 (223.4) a | 49.4 (19.6) | 301.8 (141.7 to 461.8), 1.90 | 66.1 (19.8) b | 25.6 (6.9) | 40.6 (27.4 to 53.8), 2.73 |
| MF | 68.6 (29.8) a | 37.5 (8.5) | 31.1 (9.4 to 52.8), 1.42 | 35.1 (12.4) b | 16.7(4.4) | 18.4 (9.7 to 27.1), 2.01 |
| HM | 191 (71.5) a | 84.9 (12.1) | 106.1 (54.7 to 157.6), 2.07 | 169.7 (63.6) b | 71.5 (15.8) | 98.2 (57 to 139.4), 2.12 |
| HL | 176.6 (63.2) a | 78.7 (11.3) | 97.8 (52.3 to 143.4), 2.21 | 147.4 (41.4) b | 67.9 (11.3) | 7.9 (51.1 to 107.8), 2.62 |
| PTI (kPa·s) | ||||||
| T1 | 28.3 (13.7) a | 17.9 (7.3) | 10.4 (0.9 to 20.7), 0.95 | 18 (7.4) | 13.6 (7.9) | 4.4 (−2.7 to 11.6) |
| T2–5 | 8.5 (3.6) a | 2.9 (2.7) | 4.6(1.5 to 7.7), 1.43 | 7.4 (4.4) b | 2.6 (0.6) | 4.8 (1.8 to 7.7), 1.61 |
| M1 | 30 (16.5) a | 14.6 (4.1) | 15.4 (3.4 to 27.3), 1.31 | 22.9 (4.4) b | 11.7 (1.7) | 11.2 (8 to 14.4), 3.29 |
| M2 | 60 (24.2) a | 34.6 (8.8) | 25.4 (8.3 to 42.5), 1.39 | 35.7 (11.1) b | 22.9 (5.8) | 12.8 (4.4 to 21.1), 1.40 |
| M3 | 61.7 (25.3) a | 38.3 (7.3) | 23.5 (5 to 41.8), 1.26 | 31.8 (14.1) | 28.4 (3.5) | 3.4 (−6.8 to 13.5) |
| M4 | 75.8 (36.5) a | 32 (4.4) | 43.8 (17.6 to 70), 1.73 | 25.6 (11.4) | 21.3 (5.8) | 4.2 (−4.2 to 12.7) |
| M5 | 78.3 (54.6) a | 15.6 (5.2) | 62.7 (23.6 to 101.8), 1.62 | 17.4 (8.1) b | 8 (3.6) | 9.4 (3.7 to 15.1), 1.50 |
| MF | 20.7 (8.5) a | 11.7 (3.6) | 9 (2.3 to 15.7), 1.36 | 7.1 (3) | 6 (3.2) | 1.1 (−1.7 to 3.8) |
| HM | 44 (12.8) a | 23.5 (7.8) | 20.5 (10.6 to 30.5), 1.94 | 32.6 (9.3) b | 22.2 (5.6) | 10.4 (3.5 to 17.3), 1.36 |
| HL | 42.4 (12) a | 22.4 (10.2) | 20 (9.6 to 30), 1.81 | 29.1 (8.5) b | 20.9 (4.2) | 8.2 (2.2 to 14.1), 1.22 |
| SMaxF (%) | ||||||
| T1 | 17 (7.5) | 18.6 (6.7) | −1.6 (−8.3 to 5.1) | 18.4 (7.3) | 21.3 (8.3) | −2.8 (−10 to 4.3) |
| T2–5 | 7.4 (5.2) | 7.2 (4.3) | 0.2 (−4.2 to 4.7) | 7.2 (4.1) | 7.6 (3.4) | −0.4 (−3.9 to 3.1) |
| M1 | 20.2 (9.1) | 15.8 (1.7) | 4.5 (−2.1 to 11) | 29.8 (9.6) b | 18 (7.4) | 11.8 (4.2 to 19.4), 1.74 |
| M2 | 40.2 (19.8) a | 20.1 (4.3) | 20.1 (5.7 to 34.5), 1.48 | 23.6 (2.1) b | 17.2 (0.9) | 6.5 (4.5 to 8.6), 3.73 |
| M3 | 28.8 (12.4) | 21.1 (4.7) | 7.6 (−1.2 to 16.4) | 16.8 (7.8) | 19.8 (4.1) | −3 (−8.6 to 2.5) |
| M4 | 26.4 (12.1) | 17.9 (4.2) | 8.5 (−0.5 to 17.4) | 11.9 (5.3) | 15.7 (3.5) | −3.8 (−7.8 to 0.2) |
| M5 | 29 (21.4) a | 10.6 (4.8) | 18.4 (2.9 to 33.8), 1.19 | 5.7 (1.4) | 8.1 (3) | −2.4 (−4.7 to 0) |
| MF | 28.8 (13.3) | 33.6 (9.3) | −4.7 (−15.5 to 6) | 14.6 (9.6) | 17.2 (5.6) | −2.5 (−9.8 to 4.8) |
| HM | 39.6 (14.6) | 31.6 (5.2) | 8 (−2.8 to 18.7) | 49 (16.4) b | 35.7 (7.2) | 13.3 (1.7 to 24.9), 1.05 |
| HL | 34.1 (13) a | 24 (0.6) | 10.1 (0.9 to 19.4), 1.28 | 39.9 (10.1) b | 30 (5.3) | 9.9 (2.6 to 17.3), 1.23 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Zheng, D.; Yan, S.; Liu, M.; Yang, L. Children with Obesity Experience Different Age-Related Changes in Plantar Pressure Distributions: A Follow-Up Study in China. Int. J. Environ. Res. Public Health 2020, 17, 6602. https://doi.org/10.3390/ijerph17186602
Zhao Y, Zheng D, Yan S, Liu M, Yang L. Children with Obesity Experience Different Age-Related Changes in Plantar Pressure Distributions: A Follow-Up Study in China. International Journal of Environmental Research and Public Health. 2020; 17(18):6602. https://doi.org/10.3390/ijerph17186602
Chicago/Turabian StyleZhao, Yihong, Debin Zheng, Shiyang Yan, Mengyuan Liu, and Luming Yang. 2020. "Children with Obesity Experience Different Age-Related Changes in Plantar Pressure Distributions: A Follow-Up Study in China" International Journal of Environmental Research and Public Health 17, no. 18: 6602. https://doi.org/10.3390/ijerph17186602
APA StyleZhao, Y., Zheng, D., Yan, S., Liu, M., & Yang, L. (2020). Children with Obesity Experience Different Age-Related Changes in Plantar Pressure Distributions: A Follow-Up Study in China. International Journal of Environmental Research and Public Health, 17(18), 6602. https://doi.org/10.3390/ijerph17186602