“When I Breastfeed, It Feels as if my Soul Leaves the Body”: Maternal Capabilities for Healthy Child Growth in Rural Southeastern Tanzania


{kind=link}
Abstract
:1. Introduction
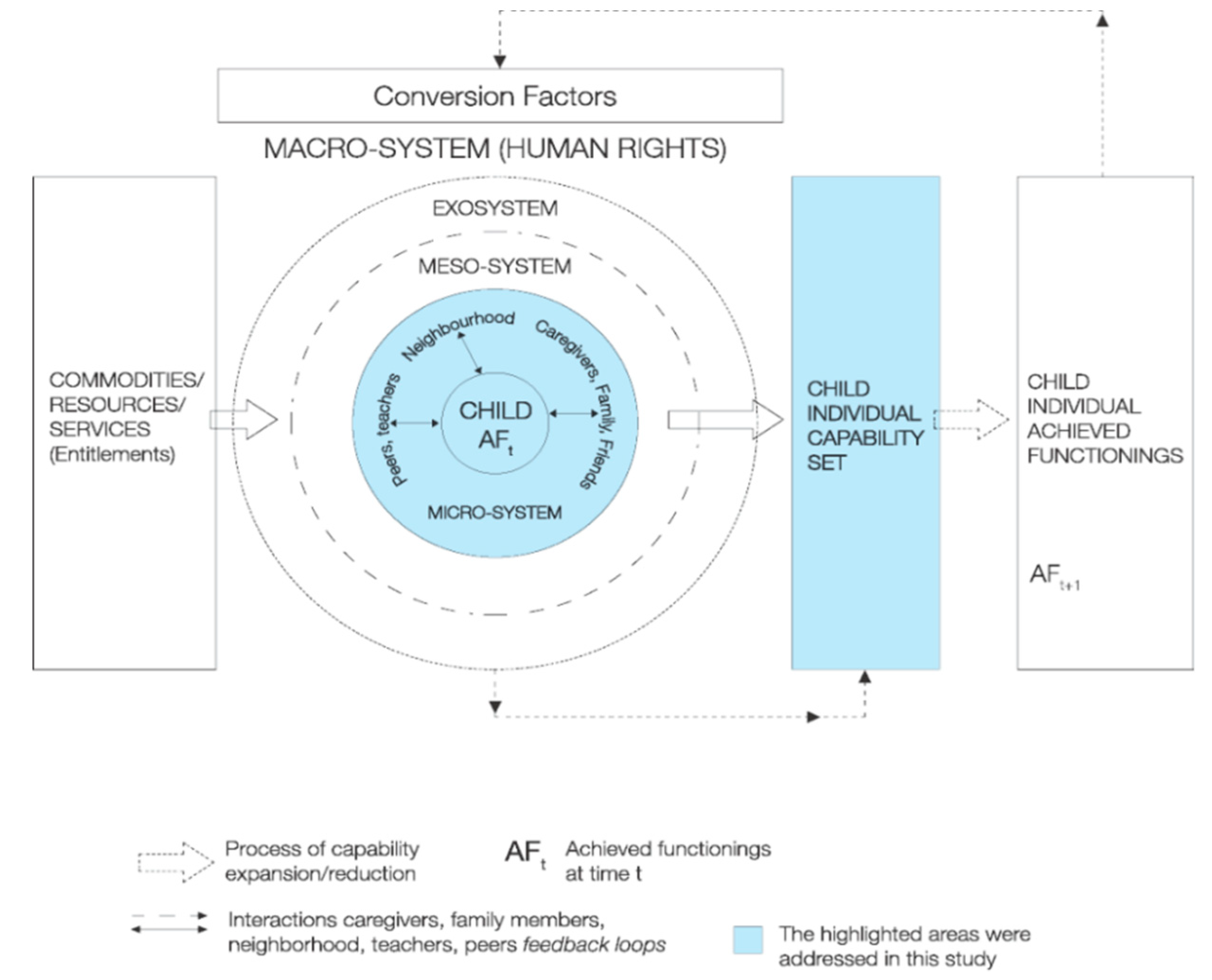
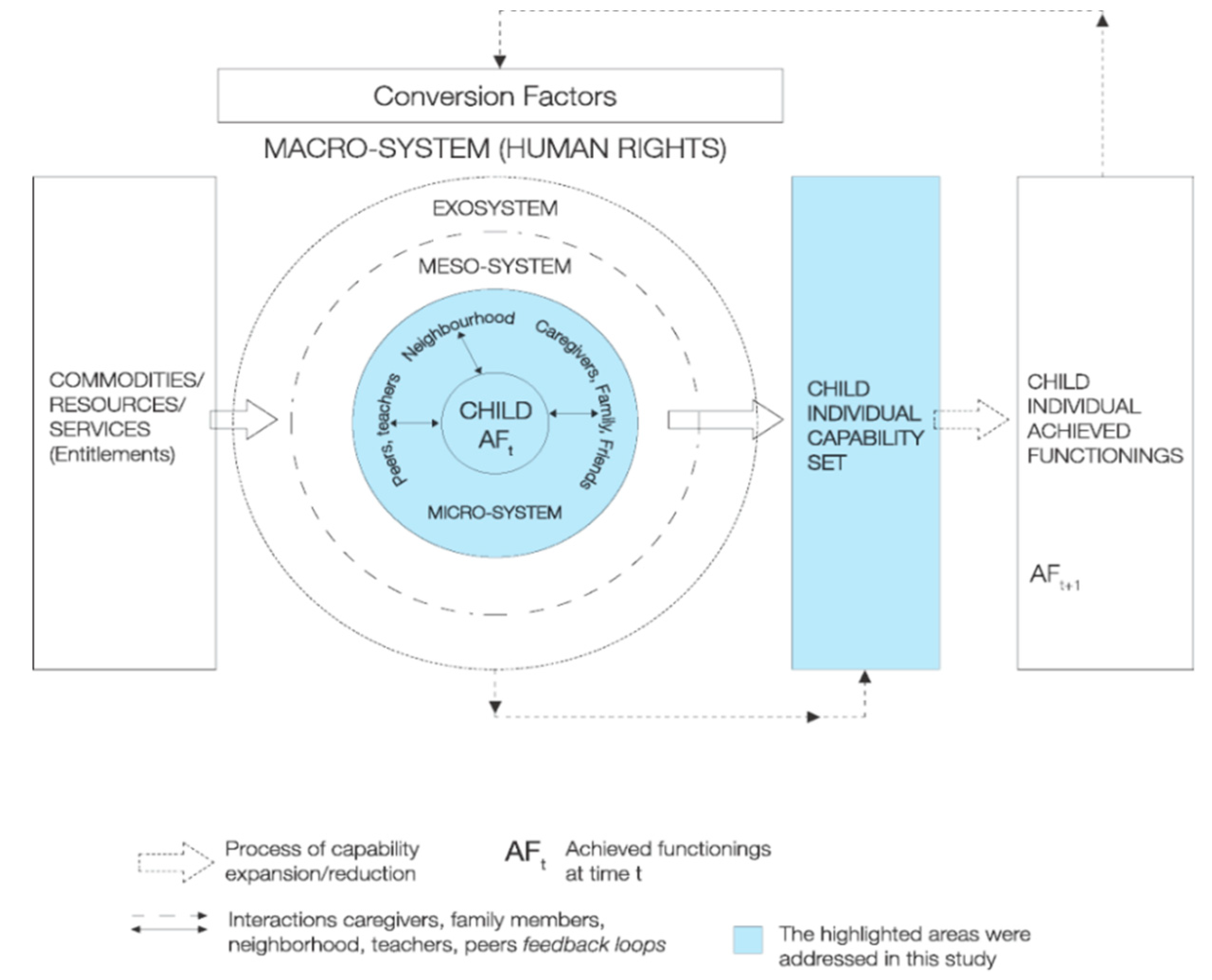
2. Capabilities Approach: A Theoretical Framework
3. Methods
3.1. Study Design
3.2. Study Setting
3.3. Recruitment of Participants
3.4. Data Collection
3.5. Data Analysis
3.6. Positionality
3.7. Ethical Issues
4. Results
5. The Capability to Feed
5.1. Personal Conversion Factors and the Mother’s Capability to Feed
When a mother is pregnant there are particular nutritious foods that she is supposed to use [eat] so that she promotes the health of the baby in her womb. You see, when a mother gives birth, you will find that the baby is in good health. When the baby is born in good health you will hear people say, ‘Someone has given birth to a big baby, the baby is bigger than her mother.’ The baby is big to the extent that when s/he is taken to be weighed you find that it has three or four kilos, you see! That means that a father took a good care of his wife when pregnant. (FGD-#03-Father)
I told him (partner) that the child has been found with UTI and malaria, and that the cost is 3000 shillings. He said, ‘I do not have that 3000 shillings.’ I then decided to report him to the sub-village leader. The leader helped me to make him provide that money. I then paid the lady (nurse). (IDI-#05-Mother)
When returning from the farm work, you are tired, but the household chores await you (majukumu yanakusubiri). You are supposed to fetch water, cook, feed children, wash children, wash clothes, and clean the house. Ideally, a child is supposed to eat three times a day, in the morning, in the afternoon, and in the evening. That is the mother’s good care. But now, I return from farm work at 3 pm, it takes a lot of time to prepare mboga (leafy greens) and cook ugali. Eventually, my children eat late. In most cases, they end up eating twice a day. (IDI-#01-Mother)
At times, I overstay there [in the field] and return home late. I start cooking, but find that by the time I finish cooking, it is already late evening. They (children) end up eating just a single meal per day, as you cannot return early from the farm. (IDI-#02-Mother)
We usually go to farms early in the morning and return home at 2.00 p.m. At times, we even lack a chance to eat lunch. You only come to get ugali (stiff porridge) in the evening, around 4:00 p.m. That is when you return from the farm, you start cooking, and you finish around 6:00 p.m. That is the only meal you have for the day. While working in the farm, you are starving, but the baby breastfeeds on you the whole day. Thus, both you and the baby starve. When I breastfeed, it feels as if my soul leaves the body. So, you say, aah, it is better to stop breastfeeding her/him so that we can both eat ugali. Or you say, it is better to introduce food to him/her early so that s/he does not heavily breastfeed on you. (KII-#03-TBA)
Working with the babies in the farm is not pleasant at all. The farm environment is for work, not for resting. [...]. You find that a child cries so much, s/he becomes exhausted as most of the time s/he is tied on her/his mother’s back. S/he must be tired. A child needs to relax, play a little bit, and sleep. But in the farms, s/he lacks that. (IDI-#03-Father)
Most of men in our village are patriarchal (wana mfumo dume). They leave the burden [of child care] to mothers. You find that a mother has a lot of activities to do, and is still supposed to look after children. [...] With that situation, instead of preparing food that has nutrients proper for healthy growth of her child, a mother decides to feed her child kiporo (dinner left-overs) so that s/he does not bother her with his/her hunger. That’s why you find that a child becomes malnourished as s/he is not being provided with food suitable for her/his age. (IDI-#07-Father)
I have best friends (maswahiba) with whom my child is comfortable. They like to stay with my child. One of the neighbors, who is with my son as we speak… I used to leave my child at her place, go to the farm and return late in the evening, say at 3 pm. I even do not leave behind any food for him (child), because what they will eat, my child also eats. She (friend) is so helpful. (IDI-#03-Mother)
5.2. Socio-Cultural Conversion Factors and Mother’s Capability to Feed
When a woman becomes pregnant prematurely, she can’t continue to breastfeed while knowing that she has a baby in her womb. She has to stop breastfeeding, short of that, the baby will contract excessive diarrhea, which will weaken her and make her growth falter. […] It is important to immediately stop breastfeeding completely when you notice that you are pregnant, even if the baby is three or five months old. (KII-#02-TBA)
People in our community have come to know over the years that when an infant cries much, it means that s/he is born with hunger. Thus, when a baby reaches three weeks, one month or two months, you find that s/he [caregiver] starts feeding her/him some ‘uji’ (porridge). (KII-#01-CHW)
Other children are denied breastfeeding by the evil spirits. When a mother has an evil spirit in her body, the child is being threatened by that evil spirit that you have. So, when a child is scared s/he avoids coming closer to you. […] when that happens, a mother decides to give the baby porridge or cow’s milk. (FGD-#03-Mother)
5.3. Capability to Control and make Decisions on Farm Produce and Income
In our context, men control farm income. Thus, a woman decides to cultivate her own farm, and her man cultivates his own farm. When you harvest, you have your own income, and the man will have his own income (IDI-#04-Mother).
You work in the farm from the first month of pregnancy till when you are almost due. In the ninth month if you feel that you are so tired, you may rest for one month, and then give birth. When you give birth, you continue working. […] If you refuse to go to the farm, when he harvests, he will not involve you with the products. He could even decide to sell all the crops in the farm. You will just hear that your partner has sold the crops and has married another wife. Women are now conscious! She goes to work in the farm even when she has a little infant. This way, men hardly find a good reason to misappropriate the crops. (KII-#03-Traditional birth attendant)
5.4. Capability to Assure Access to and Utilization of Medical Care
Usually, when a child is sick, a mother is the first person who will notice. She will then inform you (a father) that this little one is sick. Even if a child cannot speak, the mother has the capacity to recognize an ill condition in her child. By being close to a child, she can just tell if something is wrong in his/her (baby’s) health” (FGD-FOU-#03)
Men in our context do not take children to the clinic. They feel shy (laughs). He will be laughed at by his colleagues. They will ask him, ‘Why do you take the child to the clinic? Are you controlled by your wife? (umetawaliwa na mkeo?).’ That is what most of them (men) fear. (IDI-#01-Mother)
Many men lack confidence. People talk about being charmed by a wife. That’s why one may ask himself, ‘Should I take the child to the (CGM) clinic? No way, this is my wife’s role.’ So, he leaves it up to his wife. (IDI-#05-father)
The lack of a dispensary (health facility) in this village is a big challenge towards our efforts to ensure that our children get better health care. We are greatly affected. Geographically, our area is troublesome during rainy season. We also lack good roads which could enable someone to rush someone to the nearby hospital in times of health emergencies. If we could have a dispensary in our village, it would be much better. […] So, if a child falls sick, and if you are not careful, you may be surprised that the child dies at home. (IDI-#04-Father).
You find that the child is ill and needs immediate treatment, but the father is not around or he tells you that he does not have money. What will you do? You must use your brain. If you have a friend, you go and ask her for a help or a loan so as you take your child to the hospital, with the agreement of refunding her later. (IDI-#04-Mother)
One day my son was feverish, I could not sleep. I was alone as his father does not sleep here. When the morning came, I informed his father about the child’s condition. He told me to go to the drug shop for medication. I decided to take the child to the hospital for diagnosis. I only had 1000 shillings, while the diagnosis costs 3000 shillings. So I asked the nurse to help me (give medication on loan), she trusted me and told me to bring the remaining 2000 shillings later. When I returned home, I told him (partner) that the child has been diagnosed with UTI and malaria, and that the cost is 3000 shillings. He said, ‘I do not have that 3000 shillings’. I then decided to report him to the sub-village leader. The leader helped me to make him provide that money. I then paid the lady (nurse). (IDI-#05-Mother)
6. Discussion
6.1. Being Able to Feed
6.2. Being Able to Control and Make Decisions on Farm Produce and Income
6.3. Being Able to Ensure Access to Medical Care
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Children’s Fund. Breastfeeding: A Mother’s Gift, for Every Child; United Nations Children’s Fund: New York, NY, USA, 2018. [Google Scholar]
- You, D.; Hug, L.; Ejdemyr, S.; Idele, P.; Hogan, D.; Mathers, C.; Gerland, P.; Rou, J.; Alkema, L.; United Nations Inter-agency Group for Child Mortality Estimation (UN IGME). Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: A systematic analysis by the un Inter-Agency Group for Child Mortality Estimation. Lancet 2015. [Google Scholar] [CrossRef]
- Unicef/WHO/The World Bank. Levels and Trends in Child Malnutrition—Unicef WHO The World Bank Joint Child Malnutrition Estimates, Key Findings pf the 2019 Edition; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar] [CrossRef]
- MoHCDGEC. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16; MoHCDGEC, MoH, NBS, OCGS, and ICF: Dar es Salaam, Tanzania; Rockville, MD, USA, 2016. [Google Scholar] [CrossRef]
- Bégin, F.; Elder, L.; Griffiths, M.; Holschneider, S.; Piwoz, E.; Ruel-Bergeron, J.; Shekar, M. Promoting child growth and development in the sustainable development goals era: Is it time for new thinking? J. Nutr. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haisma, H.; Yousefzadeh, S.; Boele Van Hensbroek, P. Towards a capability approach to child growth: A theoretical framework. Matern. Child Nutr. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefzadeh, S.; Biggeri, M.; Arciprete, C.; Haisma, H. A Capability Approach to Child Growth. Child Indic. Res. 2019. [Google Scholar] [CrossRef] [Green Version]
- Mangasaryan, N.; Arabi, M.; Schultink, W. Revisiting the concept of growth monitoring and its possible role in community-based nutrition programs. Food Nutr. Bull. 2011. [Google Scholar] [CrossRef] [PubMed]
- Nabarro, D.; Chinnock, P. Growth monitoring-inappropriate promotion of an appropriate technology. Soc. Sci. Med. 1988. [Google Scholar] [CrossRef]
- Hall, D. Health for all Children: Report of the Third Joint Working Party on Child Health Surveillance; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Ashworth, A.; Shrimpton, R.; Jamil, K. Growth monitoring and promotion: Review of evidence of impact. Matern. Child Nutr. 2008. [Google Scholar] [CrossRef] [Green Version]
- Afnan-Holmes, H.; Magoma, M.; John, T.; Levira, F.; Msemo, G.; Armstrong, C.E.; Martínez-Álvarez, M.; Kerber, K.; Kihinga, C.; Makuwani, A.; et al. Tanzania’s Countdown to 2015: An analysis of two decades of progress and gaps for reproductive, maternal, newborn, and child health, to inform priorities for post-2015. Lancet Glob. Health 2015. [Google Scholar] [CrossRef] [Green Version]
- James, A.; Prout, A. Constructing and Reconstructing Childhood: Contemporary Issues in the Sociological Study of Childhood; Classic Edition; Routledge: London, UK; New York, NY, USA, 2015. [Google Scholar] [CrossRef]
- Hadley, C. Is polygyny a risk factor for poor growth performance among Tanzanian agropastoralists? Am. J. Phys. Anthropol. 2005. [Google Scholar] [CrossRef]
- Howard, M. Socio-economic causes and cultural explanations of childhood malnutrition among the Chagga of Tanzania. Soc. Sci. Med. 1994. [Google Scholar] [CrossRef]
- Nordang, S.; Shoo, T.; Holmboe-Ottesen, G.; Kinabo, J.; Wandel, M. Women’s work in farming, child feeding practices and nutritional status among under-five children in rural Rukwa, Tanzania. Br. J. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sellen, D.W. Polygyny and child growth in a traditional pastoral society: The case of the Datoga of Tanzania. Hum. Nat. 1999. [Google Scholar] [CrossRef] [PubMed]
- Shilugu, L.L.; Sunguya, B.F. Stunting in the Context of Plenty: Unprecedented Magnitudes among Children of Peasant’s Households in Bukombe, Tanzania. Front. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sen, A. Capability and well-being. In The Quality of Life; Sen, A.K., Nussbaum, M., Eds.; Clarendon Press: Oxford, UK, 1993. [Google Scholar]
- Chakraborty, B.; Yousefzadeh, S.; Darak, S.; Haisma, H. “We struggle with the earth everyday”: Parents’ perspectives on the capabilities for healthy child growth in haor region of Bangladesh. BMC Public Health 2020. [Google Scholar] [CrossRef] [Green Version]
- Sen, A. Famines as Failures of Exchange Entitlements. Econ. Polit. Wkly. 1976, 11, 1273–1280. [Google Scholar]
- Robeyns, I. Sen’s capability approach and gender inequality: Selecting relevant capabilities. Fem. Econ. 2003. [Google Scholar] [CrossRef]
- Carlough, M.; McCall, M. Skilled birth attendance: What does it mean and how can it be measured? A clinical skills assessment of maternal and child health workers in Nepal. Int. J. Gynecol. Obstet. 2005, 89, 200–208. [Google Scholar] [CrossRef]
- Mchome, Z.; Bailey, A.; Darak, S.; Haisma, H. “A child may be tall but stunted.” Meanings attached to childhood height in Tanzania. Matern. Child Nutr. 2019, 15. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Hennink, M.; Hutter, I.; Bailey, A. Qualitative Research Methods; SAGE: Los Angeles, CA, USA, 2011. [Google Scholar]
- Mchome, Z.; Bailey, A.; Kessy, F.; Darak, S.; Haisma, H. Postpartum sex taboos and child growth in Tanzania: Implications for child care. Matern. Child Nutr. 2020. [Google Scholar] [CrossRef]
- Abubakar, A.; Holding, P.; Mwangome, M.; Maitland, K. Maternal perceptions of factors contributing to severe under-nutrition among children in a rural African setting. Rural Remote Health 2011, 11, 1423. [Google Scholar]
- Nankumbi, J.; Muliira, J.K. Barriers to infant and child-feeding practices: A qualitative study of primary caregivers in rural Uganda. J. Health Popul. Nutr. 2015. [Google Scholar] [CrossRef]
- Affleck, W.; Pelto, G. Caregivers’ responses to an intervention to improve young child feeding behaviors in rural Bangladesh: A mixed method study of the facilitators and barriers to change. Soc. Sci. Med. 2012. [Google Scholar] [CrossRef]
- Ahishakiye, J.; Bouwman, L.; Brouwer, I.D.; Matsiko, E.; Armar-Klemesu, M.; Koelen, M. Challenges and responses to infant and young child feeding in rural Rwanda: A qualitative study. J. Health Popul. Nutr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Dearden, K.A.; Quan, L.N.; Do, M.; Marsh, D.R.; Pachón, H.; Schroeder, D.G.; Lang, T.T. Work outside the home is the primary barrier to exclusive breastfeeding in rural Viet Nam: Insights from mothers who exclusively breastfed and worked. Food Nutr. Bull. 2002, 23, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Wandel, M.; Holmboe-Ottesen, G. Women’s Work in Agriculture and Child Nutrition in Tanzania. J. Trop. Pediatr. 1992, 38, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.L. These are not our priorities: Maasai women, human rights, and the problem of culture. In Gender and Culture at the Limit of Rights; University of Pennsylvania Press: Philadelphia, PA, USA, 2011. [Google Scholar]
- Howard, M.T.; Millard, A.V. Hunger and Shame: Child Malnutrition and Poverty on Mount Kilimanjaro; Routledge: London, UK, 1997. [Google Scholar]
- Mabilia, M. The cultural context of childhood diarrhoea among Gogo infants. Anthropol. Med. 2000. [Google Scholar] [CrossRef]
- Harris-Davis, E.; Haughton, B. Model for Multicultural Nutrition Counseling Competencies. J. Am. Diet. Assoc. 2000, 100, 1178–1185. [Google Scholar] [CrossRef]
- Curry, K.R. Multicultural competence in dietetics and nutrition. J. Am. Diet. Assoc. 2000. [Google Scholar] [CrossRef]
- Hahn, R.A.; Inhorn, M.C. (Eds.) Anthropology in Public Health: Bridging Differences in Culture and Society; Oxford University Press: New York, NY, USA, 2009. [Google Scholar]
- Aubel, J.; Touré, I.; Diagne, M. Senegalese grandmothers promote improved maternal and child nutrition practices: The guardians of tradition are not averse to change. Soc. Sci. Med. 2004. [Google Scholar] [CrossRef]
- Aubel, J. The role and influence of grandmothers on child nutrition: Culturally designated advisors and caregivers. Matern. Child Nutr. 2012. [Google Scholar] [CrossRef]
- Mukuria, A.G.; Martin, S.L.; Egondi, T.; Bingham, A.; Thuita, F.M. Role of social support in improving infant feeding practices in Western Kenya: A quasi-experimental study. Glob. Health Sci. Pract. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassley, J.; Eschiti, V. Grandmother breastfeeding support: What do mothers need and want? Birth 2008. [Google Scholar] [CrossRef] [PubMed]
- Engle, P.L.; Pelto, G.H. Responsive Feeding: Implications for Policy and Program Implementation. J. Nutr. 2011, 141, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Kulwa, K.B.M.; Kinabo, J.L.D.; Modest, B. Constraints on good child-care practices and nutritional status in urban Dar-es-Salaam, Tanzania. Food Nutr. Bull. 2006. [Google Scholar] [CrossRef] [PubMed]
- Onyango, A.; Tucker, K.; Eisemon, T. Household headship and child nutrition: A case study in Western Kenya. Soc. Sci. Med. 1994. [Google Scholar] [CrossRef]
- Pfeiffer, J.; Gloyd, S.; Li, L.R. Intrahousehold resource allocation and child growth in Mozambique: An ethnographic case-control study. Soc. Sci. Med. 2001. [Google Scholar] [CrossRef]
- Richards, E.; Theobald, S.; George, A.; Kim, J.C.; Rudert, C.; Jehan, K.; Tolhurst, R. Going beyond the surface: Gendered intra-household bargaining as a social determinant of child health and nutrition in low and middle income countries. Soc. Sci. Med. 2013. [Google Scholar] [CrossRef]
- Kariuki, J.; Njuki, J.; Mburu, S.; Waithanji, E. Women, livestock ownership and food security. In Women, Livestock Ownership and Markets: Bridging the Gender Gap in Eastern and Southern Africa; Routledge: London, UK, 2013. [Google Scholar]
- Schroeder, R.A. “Gone to Their Second Husbands”: Marital Metaphors and Conjugal Contracts in The Gambia’s Female Garden Sector. Can. J. Afr. Stud. Rev. Can. Études Afr. 1996. [Google Scholar] [CrossRef]
- Su, M.; Ouyang, Y.Q. Father’s role in breastfeeding promotion: Lessons from a quasi-experimental trial in China. Breastfeed. Med. 2016. [Google Scholar] [CrossRef]
- Rosane Odeh Susin, L.; Regina Justo Giugliani, E. Inclusion of fathers in an intervention to promote breastfeeding: Impact on breastfeeding rates. J. Hum. Lact. 2008, 24, 386–392. [Google Scholar] [CrossRef]
- Ruiz, M. Risks of Self-Medication Practices. Curr. Drug Saf. 2010. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mchome, Z.; Yousefzadeh, S.; Bailey, A.; Haisma, H. “When I Breastfeed, It Feels as if my Soul Leaves the Body”: Maternal Capabilities for Healthy Child Growth in Rural Southeastern Tanzania. Int. J. Environ. Res. Public Health 2020, 17, 6215. https://doi.org/10.3390/ijerph17176215
Mchome Z, Yousefzadeh S, Bailey A, Haisma H. “When I Breastfeed, It Feels as if my Soul Leaves the Body”: Maternal Capabilities for Healthy Child Growth in Rural Southeastern Tanzania. International Journal of Environmental Research and Public Health. 2020; 17(17):6215. https://doi.org/10.3390/ijerph17176215
Chicago/Turabian StyleMchome, Zaina, Sepideh Yousefzadeh, Ajay Bailey, and Hinke Haisma. 2020. "“When I Breastfeed, It Feels as if my Soul Leaves the Body”: Maternal Capabilities for Healthy Child Growth in Rural Southeastern Tanzania" International Journal of Environmental Research and Public Health 17, no. 17: 6215. https://doi.org/10.3390/ijerph17176215