Exploring the Impact of Augmented Reality in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Exclusion and Inclusion Criteria
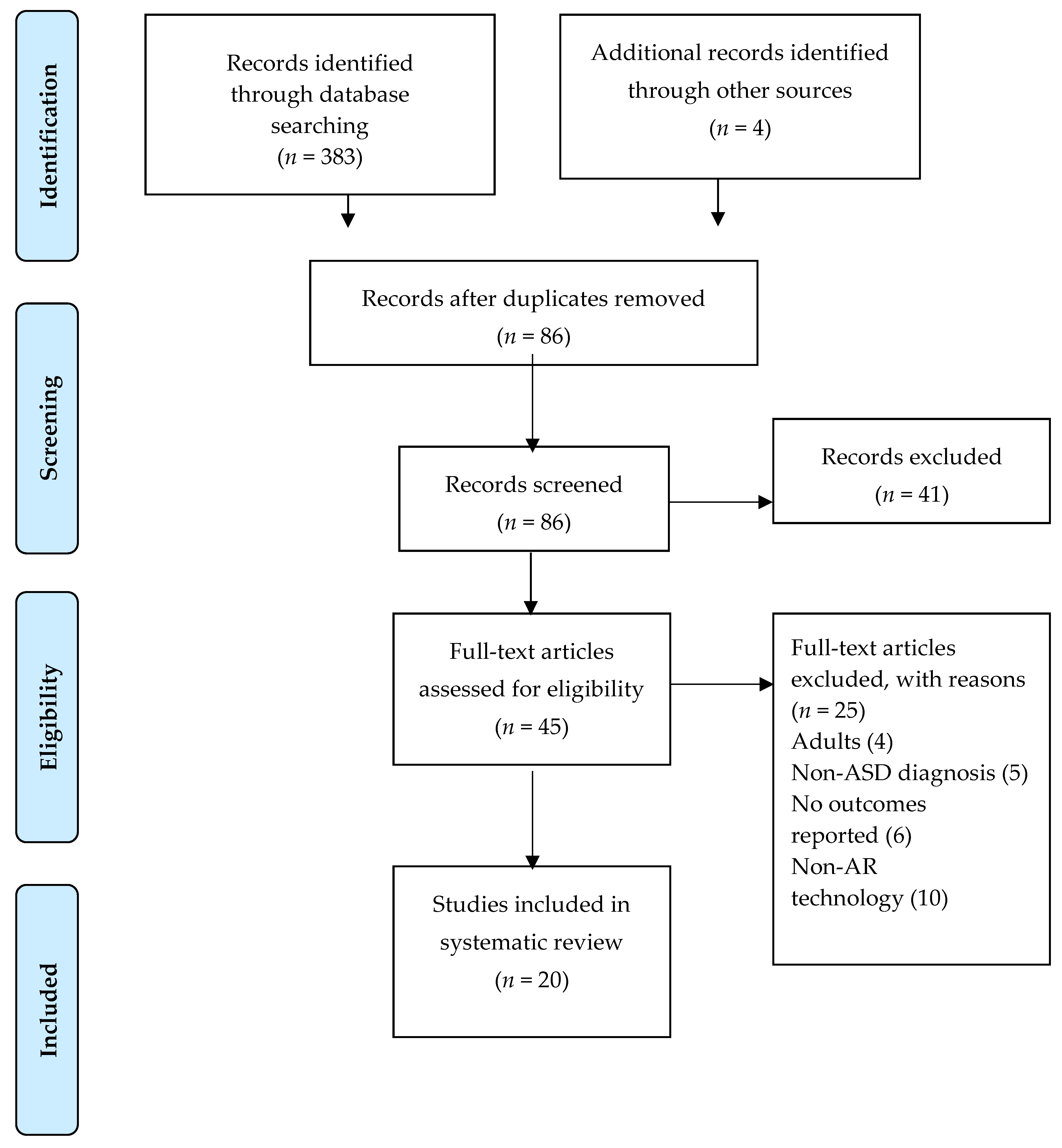
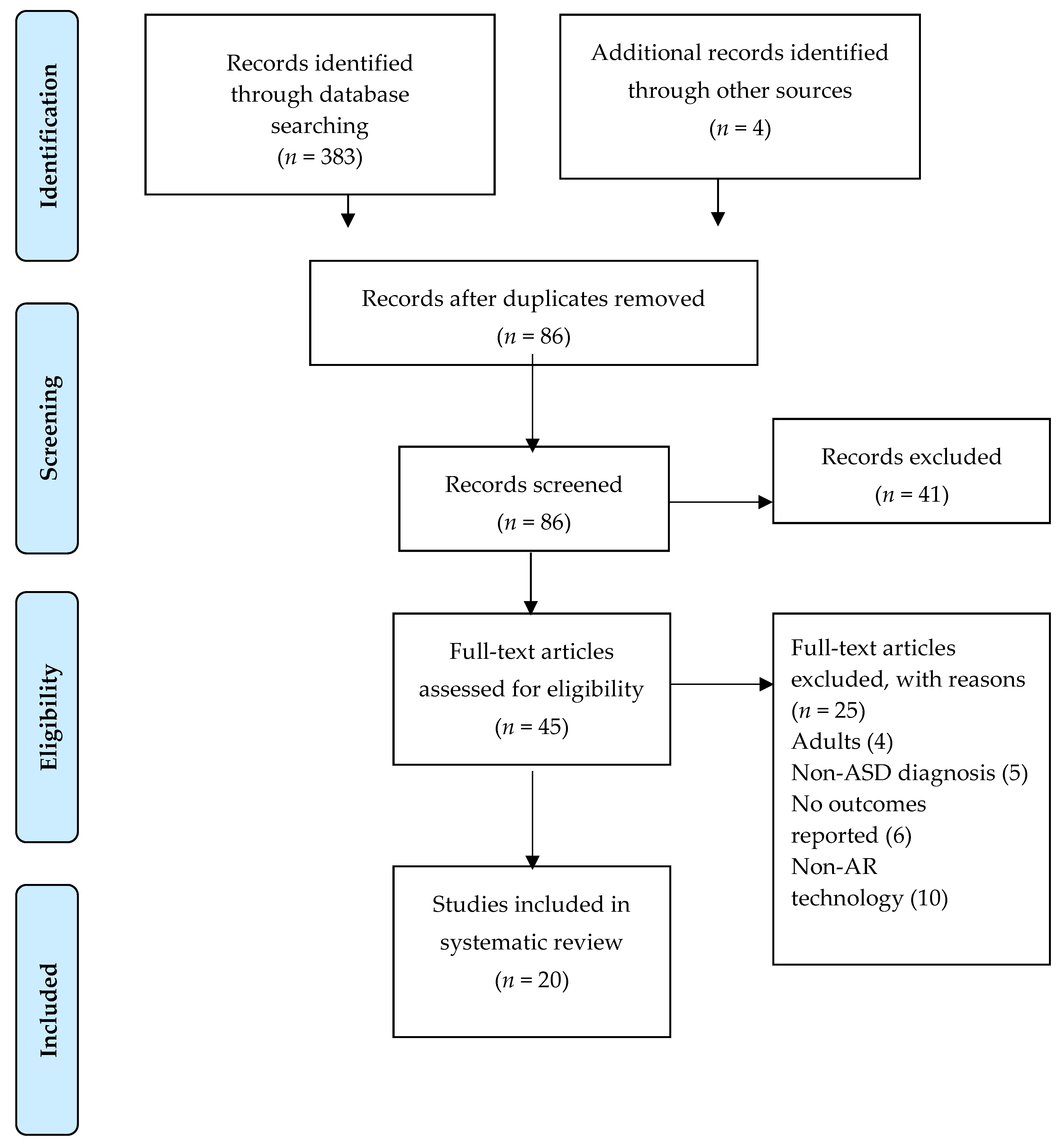
2.3. Screening Process
2.4. Methodological Quality Evaluation
3. Results
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
| Reference | Participants: N, Mean Age (MA) or Range, % Males, and IQ | Study Design | Technology/ Evaluation | Dependent Variables | Main Results |
|---|---|---|---|---|---|
| Cihak et al. [24] | ASD (3), 6–7 years, 100% males, IQ (70–75) | Single subject multiple baseline design | AR picture prompt to trigger a video model clip | Functional life skills (number of steps completed independently for brushing teeth) | AR was an effective tool for teaching chain tasks |
| Bai et al. [25] | ASD (12), MA (6.8 SD 5.5), % males (83%), IQ > 70 | Within-subject experiment with two conditions: AR and non-AR | Set of AR props, video analysis, and parent and participants questionnaire | Elicit pretend play engagement | Significantly higher frequency and duration of pretend play in the AR condition and participants are more engaged |
| Chen et al. [26] | ASD (6), MA (11.5), males (83%), IQ 103.6 (9.3) | Single subject multiple baseline design | AR video modelling and storybook | Understand facial emotions and social expressions | Significant improvement in social/emotional awareness |
| Chen et al. [27] | ASD (3), MA (12.2), males (100%), IQ 101 (9.2) | Single subject multiple baseline design | AR-based self-facial learning system | 6 basic facial expressions | Significant improvement in emotion recognition |
| Escobedo et al. [28] | ASD (12), MA (5.1 SD 0.9), males n.r., IQ low | Single subject design | AR smartphone | Selective and sustained attention | Improvement of both attention skills |
| Antão et al. [29] | ASD (48), MA (11, SD 5), males (89%), IQ > 70 TD (48), MA (11.8, SD 5.2) males (68%) | Group design | AR computer game “MoviLetrando” | Reaction time (RT) | ASD: significant improvement in RT after AR task |
| Liu et al. [30] | ASD (2), 8–9 age, males (100%), IQ > 70 | Single subject design | AR smartglasses and parent questionnaires | Social interaction | Improvement in nonverbal communication, eye contact, and social engagement |
| Lee et al. [31] | ASD (3), MA (8.8) 67% males, IQ (93.3, SD 4.6) | Single subject multiple baseline design | AR CM training system and social story test | Social interaction | AR CM training system improved social relationships |
| Lee et al. [32] | ASD (3), MA (8.1) 67% males, IQ (102.3, SD 0.6) | Single subject multiple baseline design | KST System with AR technology and social story test | Social interaction | AR-KST System intervention improved significantly autism social interaction |
| Magrini et al. [33] | ASD (10), 5–7 years, males (100%), IQ low | Within-subject experiment with two conditions: AR (5 subjects) and non-AR (5 subjects) | AR system with multisensory experience | Fine Motor skills | Significant motor improvement in AR condition |
| Lorenzo et al. [34] | ASD (11), MA (4, SD 1.2), males (91%), IQ low | Within-subject experiment with two conditions: AR and non-AR | AR smartphone and questionnaires | Social interaction | Nonsignificant improvement between groups |
| Farr et al. [35] | ASD (12), MA (11.2), males (% 42%), IQ n.r. | Within-subject experiment with two conditions: AR and non-AR | AR Knight’s Castle (AKC) play | Social interaction | AR condition showed more social behavior interaction than non-AR |
| Sahin et al. [36] | ASD (8), MA (11.7 SD 3.3), males (88%), IQ > 70 | Single subject design | AR smartglasses and questionnaires | Social interaction | Positive social experience after AR |
| Nazaruddin et al. [37] | ASD (4), 6–7 years, 50% males, IQ > 70 | Single subject design | Augmented reality book and teacher questionnaire | Attention skills | AR book was able to increase focus and recognition of objects |
| Keshav et al. [38] | ASD (1), 13 years old, 100% males, IQ > 70 | Single subject design | Empowered BrainAR Smartglasses and Social Responsiveness Scale-2 (SRS-2) | Social interaction and social communication skills | Improvement in SRS-2 social communication, motivation, and restricted and repetitive behavior subscales; improvements in verbal and nonverbal skills |
| Vahabzadeh et al. [39] | ASD (4), MA (7.5), male (100%), IQ > 70 | Single subject design | Empowered brain, AR-computerized smartglasses, and Aberrant Behavioral Checklist (ABC) | Socioemotional and behavioral effects | Improvement in irritability, hyperactivity, and social withdrawal in a sample of students with ASD |
| Chung et al. [40] | ASD (3), 6–12 years old, males (100%), IQ > 70 non-ASD siblings (3), 6–12 years old, males (100%), IQ > 70 | Single subject design | AR video games sessions | Social communication and joint positive affect | AR condition showed more joint positive affect and increased reciprocal communication |
| Soares et al. [41] | ASD (4), 8–12 years old, males (75%), IQ n.r. (low) | Single subject design | AR-based cardboard head-mounted display | Social interaction and facial processing | Better facial processing after use of AR cardboard display and EF implications |
| Escobedo et al. [42] | ASD (3), MA (10.1, SD 0.9), IQ > 70, non-ASD (11), 8–11 years old, IQ > 70 | Group design | Mobile augmented reality application and selfreports | Social interaction | AR mobile application increased the number social interactions in ASD group |
| Nag et al. [43] | ASD (16), MA (12.1, SD 3.3), IQ (102.7, SD 19.5) non-ASD (17) MA (11.5, SD 2.4), IQ (108.9, SD 9.5), males n.r. | Group design | AR smartglasses task | Emotion recognition | AR task contributed to differentiating and classifying gaze and emotion recognition patterns between ASD and non-ASD groups |
3.3. Main Outcomes
3.4. Methodological Quality Evaluation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Baio, J. Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators. Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years: Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2010. MMWR Surveill Summ. 2014, 63, 1–21. [Google Scholar] [CrossRef]
- Christensen, D.L.; Maenner, M.J.; Bilder, D.; Charles, J.; Constantino, J.; Daniels, J.; Fitzgerald, R.; Kurzius-Spencer, M.; Ching Lee, L.; Pettygrove, S.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 4 Years—Early Autism and Developmental Disabilities Monitoring Network, Seven Sites, United States, 2010, 2012, and 2014. MMWR Surveill Summ. 2019, 68, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Blumberg, S.J.; Bramlett, M.D.; Kogan, M.D.; Schieve, L.A.; Jones, J.R.; Lu, M.C. Changes in Prevalence of Parent-Reported Autism Spectrum Disorder in School-Aged US Children: 2007 to 2011–2012; (No. 65); US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2013.
- Hatta, K.; Hosozawa, M.; Tanaka, K.; Shimizu, T. Exploring Traits of Autism and Their Impact on Functional Disability in Children with Somatic Symptom Disorder. J. Autism Dev. Disord. 2019, 49, 729–737. [Google Scholar] [CrossRef]
- Leontine, W.; de Nijs, P.F.; Duvekot, J.; Greaves-Lord, K.; Hillegers, M.H.; Brouwer, W.B.; Hakkaart-van Roijen, L. Children with an autism spectrum disorder and their caregivers: Capturing health-related and care-related quality of life. J. Autism Dev. Disord. 2020, 50, 263–277. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.; Iadarola, S. Evidence base update for autism spectrum disorder. J. Clin. Child. Adolesc Psychol. 2015, 44, 897–922. [Google Scholar] [CrossRef] [Green Version]
- Grynszpan, O.; Weiss, P.L.; Perez-Diaz, F.; Gal, E. Innovative technology-based interventions for autism spectrum disorders: A meta-analysis. Autism 2014, 18, 346–361. [Google Scholar] [CrossRef]
- Hugues, O.; Fuchs, P.; Nannipieri, O. New augmented reality taxonomy: Technologies and features of augmented environment. In Hand-Book of Augmented Reality; Furht, B., Ed.; Springer: New York, NY, USA, 2011; pp. 47–63. [Google Scholar]
- Craig, A.B. Understanding Augmented Reality: Concepts and Applications; Morgan Kaufmann: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Lim, K.C.; Selamat, A.; Alias, R.A.; Krejcar, O.; Fujita, H. Usability Measures in Mobile-Based Augmented Reality Learning Applications: A Systematic Review. Appl. Sci. 2019, 9, 2718. [Google Scholar] [CrossRef] [Green Version]
- El-Seoud, M.; Halabi, O.; Geroimenko, V. Assisting Individuals with Autism and Cognitive Disorders: An Augmented Reality based Framework. Int. J. Online Biomed. Eng. 2019, 15, 28–39. [Google Scholar] [CrossRef]
- Quintero, J.; Baldiris Navarro, S.M.; Rubira, R.; Cerón, J.; Velez, G. Augmented Reality in Educational Inclusion. A Systematic Review on the Last Decade. Front. Psychol. 2019, 10, 1835. [Google Scholar] [CrossRef] [Green Version]
- Baragash, R.S.; Al-Samarraie, H.; Alzahrani, A.I.; Alfarraj, O. Augmented reality in special education: A meta-analysis of single-subject design studies. Eur. J. Spec. Needs Educ. 2019, 1–16. [Google Scholar] [CrossRef]
- Marto, A.; Almeida, H.A.; Gonçalves, A. Using Augmented Reality in Patients with Autism: A Systematic Review. In Proceedings of the ECCOMAS Thematic Conference on Computational Vision and Medical Image Processing, Porto, Portugal, 16–18 October 2019; Springer: Cham, Switzerland, 2019; pp. 454–463. [Google Scholar]
- Khowaja, K.; Banire, B.; Al-Thani, D.; Sqalli, M.T.; Aqle, A.; Shah, A.; Salim, S.S. Augmented reality for learning of children and adolescents with autism spectrum disorder (ASD): A systematic review. IEEE Access 2020, 8, C78779–C78807. [Google Scholar] [CrossRef]
- Reichow, B. Development, procedures and application of evaluative method for determining the evidence-based practices in autism. In Evidence-Based Practices and Treatments for Children with Autism; Springer: Boston, MA, USA, 2011; pp. 25–39. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L. A Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2013. [Google Scholar]
- International Statistical Classification of Diseases and Related Health Problems; Tenth Revision; World Health Organisation: Geneva, Switzerland, 1992.
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S.L. ADOS. Autism Diagnostic Observation Schedule. Manual; Western Psychological Services (WPS): Los Angeles, CA, USA, 1999. [Google Scholar]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised; ADI-R; Western Psychological Services (WPS): Los Angeles, CA, USA, 2003. [Google Scholar]
- Schopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 1980, 10, 91–103. [Google Scholar] [CrossRef]
- Cihak, D.F.; Moore, E.J.; Wright, R.E.; McMahon, D.D.; Gibbons, M.M.; Smith, C. Evaluating augmented reality to complete a chain task for elementary students with autism. J. Spec. Educ. Tech. 2016, 31, 99–108. [Google Scholar] [CrossRef]
- Bai, Z.; Blackwell, A.F.; Coulouris, G. Using augmented reality to elicit pretend play for children with autism. IEEE Trans. Vis. Comput. Graph. 2015, 21, 598–610. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Lee, I.J.; Lin, L.Y. Augmented reality-based video-modeling storybook of nonverbal facial cues for children with autism spectrum disorder to improve their perceptions and judgments of facial expressions and emotions. Comput. Human Behav. 2016, 55, 477–485. [Google Scholar] [CrossRef]
- Chen, C.H.; Lee, I.J.; Lin, L.Y. Augmented reality-based self-facial modeling to promote the emotional expression and social skills of adolescents with autism spectrum disorders. Res. Dev. Disabil. 2015, 36, 396–403. [Google Scholar] [CrossRef]
- Escobedo, L.; Tentori, M.; Quintana, E.; Favela, J.; Garcia-Rosas, D. Using augmented reality to help children with autism stay focused. IEEE Pervasive Comput. 2014, 13, 38–46. [Google Scholar] [CrossRef]
- Antão, J.Y.F.D.L.; Abreu, L.C.D.; Barbosa, R.T.D.A.; Crocetta, T.B.; Guarnieri, R.; Massetti, T.; Pedrozo, T.; Tonks, J.; Monteiro, C. Use of Augmented Reality with a Motion-Controlled Game Utilizing Alphabet Letters and Numbers to Improve Performance and Reaction Time Skills for People with Autism Spectrum Disorder. Cyberpsychol Behav Soc. Netw. 2020, 23, C16–C22. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Salisbury, J.P.; Vahabzadeh, A.; Sahin, N.T. Feasibility of an autism-focused augmented reality smartglasses system for social communication and behavioral coaching. Front. Pediatr. 2017, 5, 145. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.J.; Chen, C.H.; Wang, C.P.; Chung, C.H. Augmented reality plus concept map technique to teach childrenwith ASD to use social cues when meeting and greeting. Asia-Pacific Educ. Res. 2018, 27, 227–243. [Google Scholar] [CrossRef]
- Lee, I.J. Kinect-for-windows with augmented reality in an interactive roleplay system for children with an autism spectrum disorder. Interac. Learn. Environ. 2020, 1–17. [Google Scholar] [CrossRef]
- Magrini, M.; Curzio, O.; Carboni, A.; Moroni, D.; Salvetti, O.; Melani, A. Augmented Interaction Systems for Supporting Autistic Children. Evolution of a Multichannel Expressive Tool: The SEMI Project Feasibility Study. Appl. Sci. 2019, 9, 3081. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo, G.; Gómez-Puerta, M.; Arráez-Vera, G.; Lorenzo-Lledó, A. Preliminary study of augmented reality as an instrument for improvement of social skills in children with autism spectrum disorder. Educ. Inf. Technol. 2019, 24, 181–204. [Google Scholar] [CrossRef]
- Farr, W.; Yuill, N.; Hinske, S. An augmented toy and social interaction in children with autism. Int. J. Arts Technol. 2012, 5, 104–125. [Google Scholar] [CrossRef] [Green Version]
- Sahin, N.T.; Keshav, N.U.; Salisbury, J.P.; Vahabzadeh, A. Second Version of Google Glass as a Wearable Socio-Affective Aid: Positive School Desirability, High Usability, and Theoretical Framework in a Sample of Children with Autism. JMIR Hum. Factors 2018, 5. [Google Scholar] [CrossRef]
- Nazaruddin, M.A.; Efendi, M. The book of pop up augmented reality to increase focus and object recognition capabilities for children with autism. J. ICSAR 2018, 2, 9–14. [Google Scholar] [CrossRef]
- Keshav, N.U.; Vahabzadeh, A.; Abdus-Sabur, R.; Huey, K.; Salisbury, J.P.; Liu, R.; Sahin, N. Longitudinal socio-emotional learning intervention for autism via smartglasses: Qualitative school teacher descriptions of practicality, usability, and efficacy in general and special education classroom settings. Educ. Sci. 2018, 8, 107. [Google Scholar] [CrossRef] [Green Version]
- Vahabzadeh, A.; Keshav, N.U.; Abdus-Sabur, R.; Huey, K.; Liu, R.; Sahin, N.T. Improved socio-emotional and behavioral functioning in students with autism following school-based smartglasses intervention: Multi-stage feasibility and controlled efficacy study. Behav. Sci. 2018, 8, 85. [Google Scholar] [CrossRef] [Green Version]
- Chung, P.J.; Vanderbilt, D.L.; Soares, N.S. Social behaviors and active videogame play in children with autism spectrum disorder. Games Health J. 2015, 4, 225–234. [Google Scholar] [CrossRef]
- Soares, K.P.; Burlamaqui, A.M.F.; Goncalves, L.M.G.; da Costa, V.F.; Cunha, M.E.; da Silva, A.A.R.S. Preliminary studies with augmented reality tool to help in psycho-pedagogical tasks with children belonging to autism spectrum disorder. IEEE Lat. Am. Trans. 2017, 15, 2017–2023. [Google Scholar] [CrossRef]
- Escobedo, L.; Nguyen, D.H.; Boyd, L.; Hirano, S.; Rangel, A.; Garcia-Rosas, D.; Tentori, M.; Hayes, G. MOSOCO: A mobile assistive tool to support children with autism practicing social skills in real-life situations. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, May 2012; pp. 2589–2598. [Google Scholar] [CrossRef]
- Nag, A.; Haber, N.; Voss, C.; Tamura, S.; Daniels, J.; Ma, J.; Chiang, B.; Ramachandran, S.; Schwatz, J.; Winograd, T.; et al. Toward Continuous Social Phenotyping: Analyzing Gaze Patterns in an Emotion Recognition Task for Children With Autism Through Wearable Smart Glasses. J. Med. Internet Res. 2020, 22, e13810. [Google Scholar] [CrossRef]
- Wong, C.; Odom, S.; Hume, K.; Cox, A.; Fettig, A.; Kucharczyk, S.; Brock, M.; Plavnik, J.; Fleoury, V.; Schultz, T. Evidence-based practices for children, youth, and young adults with autism spectrum disorder: A comprehensive review. J. Autism Dev. Disord. 2015, 45, 1951–1966. [Google Scholar] [CrossRef]
- Knight, V.; McKissick, B.; Saunders, A. A review of technology-based interventions to teach academic skills to students with autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 3805–3819. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.M.; Gagie, B. Learning through seeing and doing: Visual supports for children with autism. Teach. Except. Child. 2006, 38, 26–33. [Google Scholar] [CrossRef] [Green Version]
- Sahin, N.T.; Keshav, N.U.; Salisbury, J.P.; Vahabzadeh, A. Safety and lack of negative effects of wereable augmented-reality social communication aid for children and adults with autism. J. Clin. Med. 2018, 7, 188. [Google Scholar] [CrossRef] [Green Version]
- Karamanoli, P.; Tsinakos, A.; Karagiannidis, C. The application of augmented reality for intervention to people with Autism, Spectrum Disorders. J. Mob. Comput. Appl. 2017, 4, 42–51. [Google Scholar] [CrossRef]
| Reference | Elicit Pretended Play | Emotion Recognition | Functional Life Skills | Attention Skills | Social Interaction | Motor Skills |
|---|---|---|---|---|---|---|
| Cihak et al. [24] | X | |||||
| Bai et al. [25] | X | |||||
| Chen et al. [26] | X | |||||
| Chen et al. [27] | X | |||||
| Escobedo et al. [28] | X | |||||
| Antão et al. [29] | X | |||||
| Liu et al. [30] | X | |||||
| Lee et al. [31] | X | |||||
| Lee et al. [32] | X | |||||
| Magrini et al. [33] | X | |||||
| Lorenzo et al. [34] | X | |||||
| Farr et al. [35] | X | |||||
| Sahin et al. [36] | X | |||||
| Nazaruddin et al. [37] | X | |||||
| Keshav et al. [38] | X | |||||
| Vahabzadeh et al. [39] | X | |||||
| Chung et al. [40] | X | |||||
| Soares et al. [41] | X | X | ||||
| Escobedo et al. [42] | X | |||||
| Nag et al. [43] | X |
| Reference | Strength Rating (Reichow [17]) |
|---|---|
| Cihak et al. [24] | Adequate |
| Bai et al. [25] | Adequate |
| Chen et al. [26] | Adequate |
| Chen et al. [27] | Adequate |
| Escobedo et al. [28] | Weak |
| Antão et al. [29] | Adequate |
| Liu et al. [30] | Adequate |
| Lee et al. [31] | Adequate |
| Lee et al. [32] | Adequate |
| Magrini et al. [33] | Adequate |
| Lorenzo et al. [34] | Adequate |
| Farr et al. [35] | Adequate |
| Sahin et al. [36] | Weak |
| Nazaruddin et al. [37] | Weak |
| Keshav et al. [38] | Weak |
| Vahabzadeh et al. [39] | Adequate |
| Chung et al. [40] | Weak |
| Soares et al. [41] | Weak |
| Escobedo et al. [42] | Weak |
| Nag et al. [43] | Adequate |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berenguer, C.; Baixauli, I.; Gómez, S.; Andrés, M.d.E.P.; De Stasio, S. Exploring the Impact of Augmented Reality in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6143. https://doi.org/10.3390/ijerph17176143
Berenguer C, Baixauli I, Gómez S, Andrés MdEP, De Stasio S. Exploring the Impact of Augmented Reality in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(17):6143. https://doi.org/10.3390/ijerph17176143
Chicago/Turabian StyleBerenguer, Carmen, Inmaculada Baixauli, Soledad Gómez, María de El Puig Andrés, and Simona De Stasio. 2020. "Exploring the Impact of Augmented Reality in Children and Adolescents with Autism Spectrum Disorder: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 17: 6143. https://doi.org/10.3390/ijerph17176143