Quantification of Exposure to Risk Postures in Truck Assembly Operators: Neck, Back, Arms and Wrists


Abstract
:1. Introduction
2. Materials and Methods
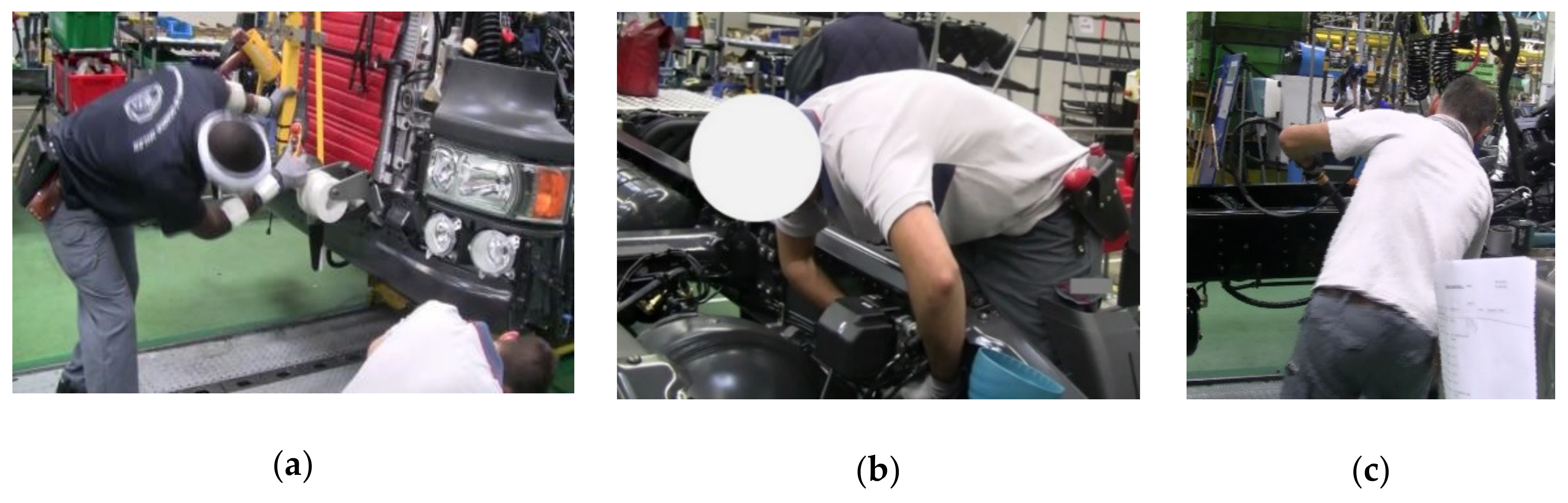
2.1. Workplace Description
2.2. Study Participants
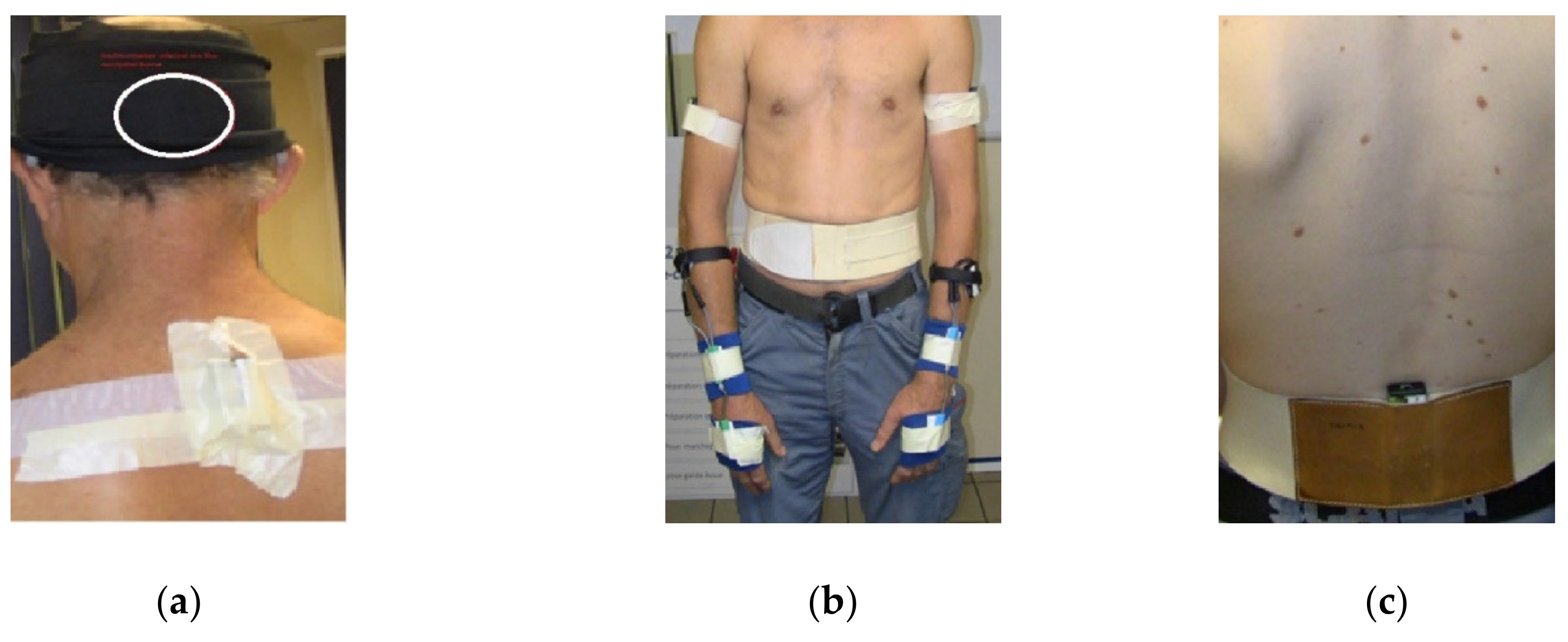
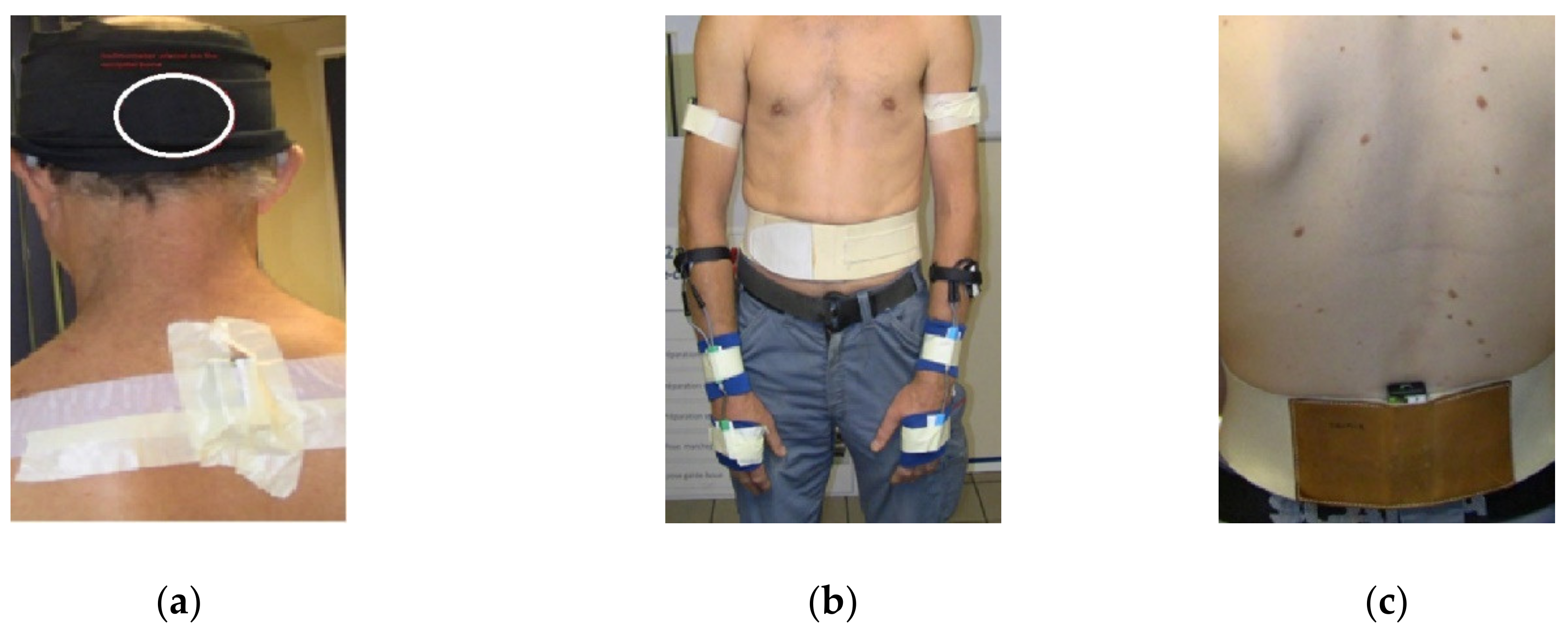
2.3. Measurement
2.4. Reference Position
2.5. Data Processing
2.6. Classification of Risk Exposure
2.7. Self-Reported Musculoskeletal Symptoms
2.8. Statistical Analysis
3. Results
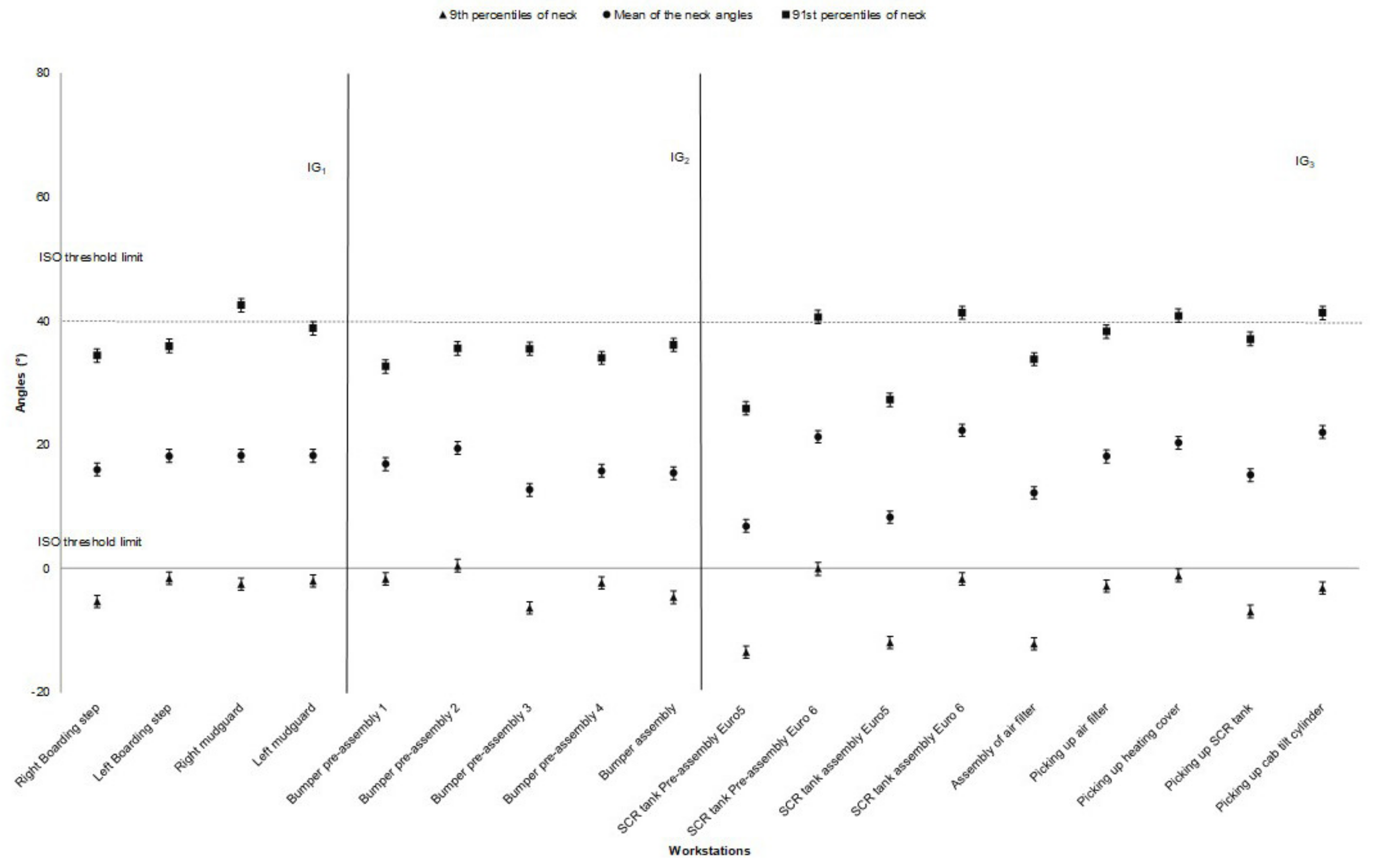
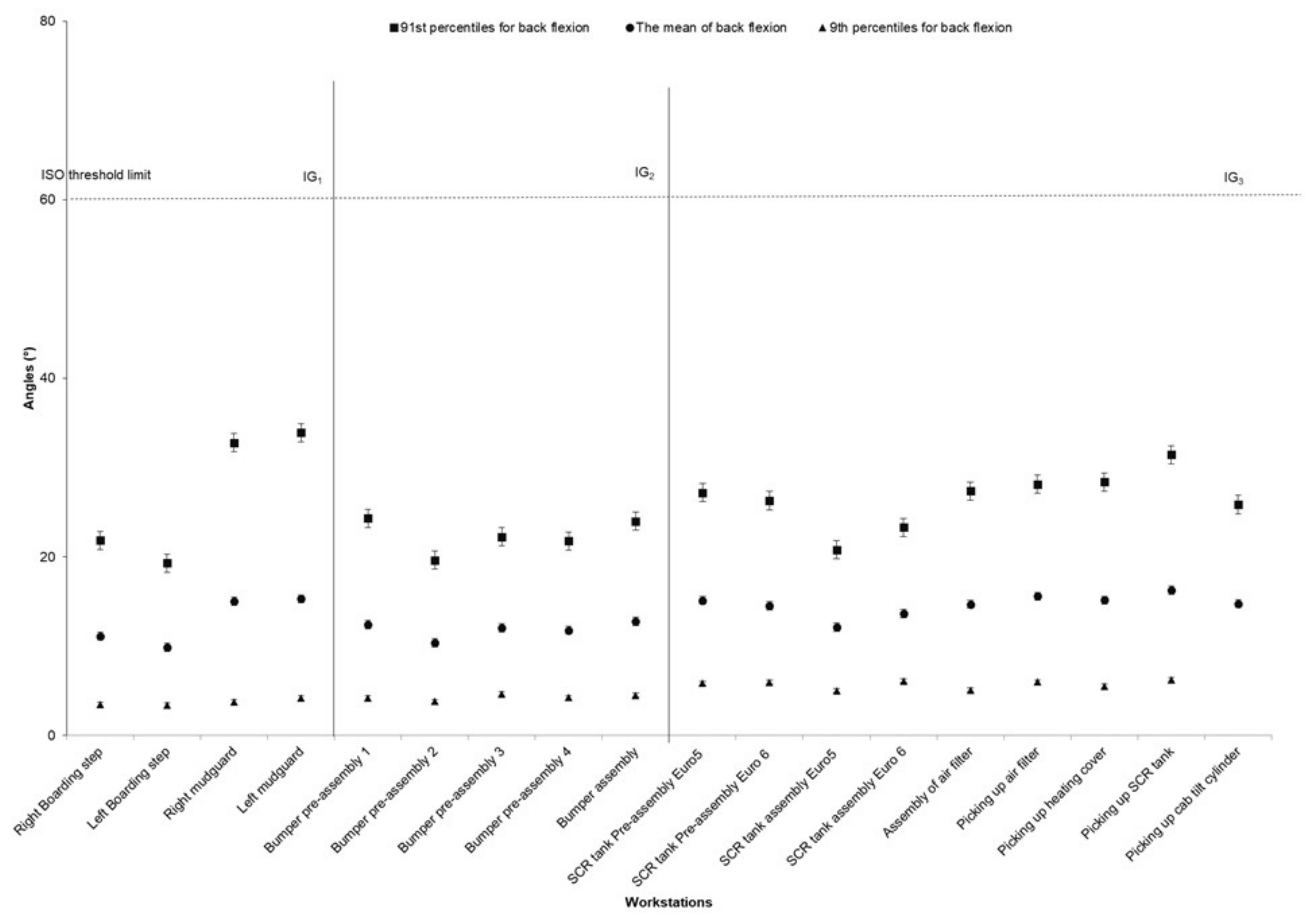
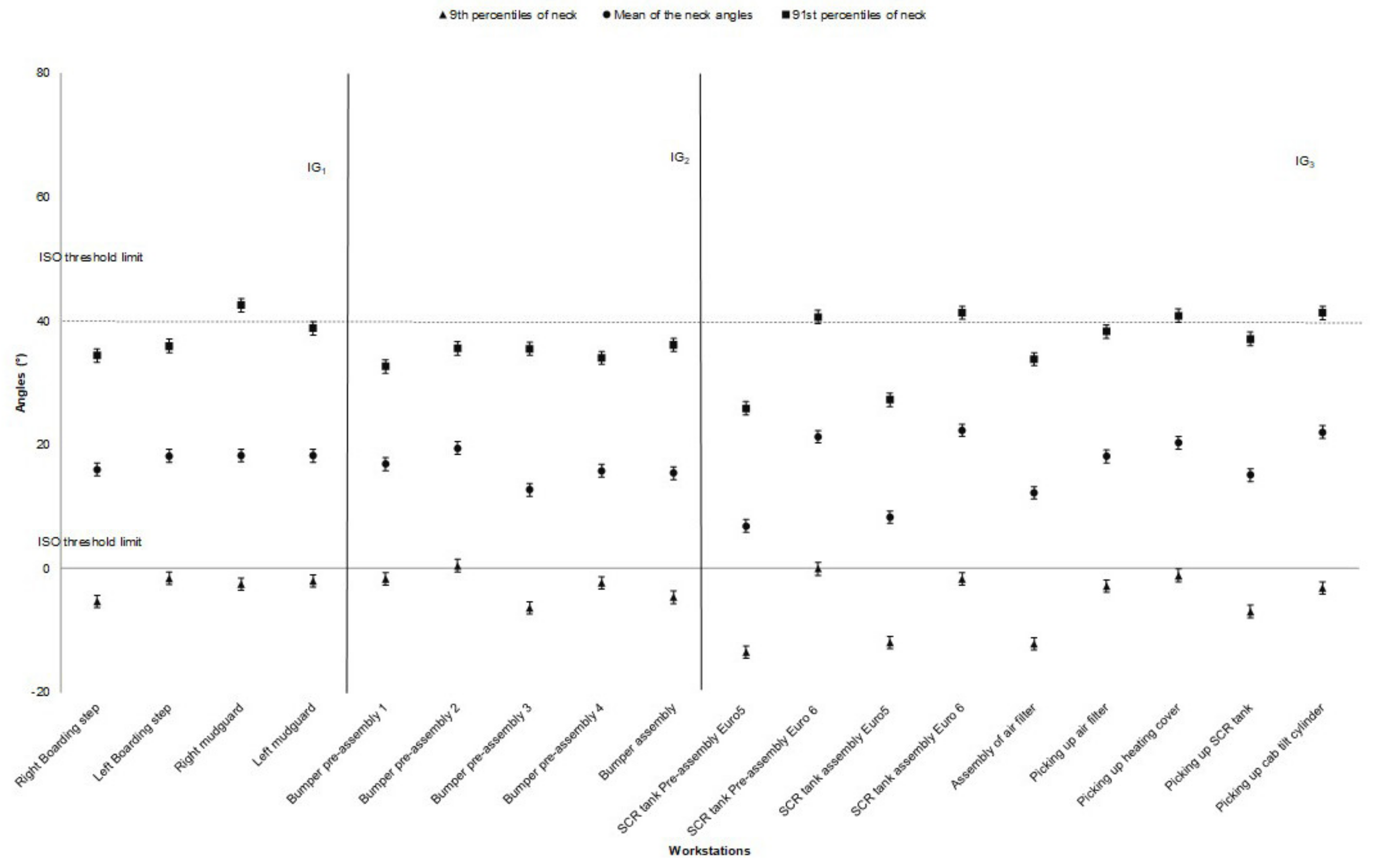
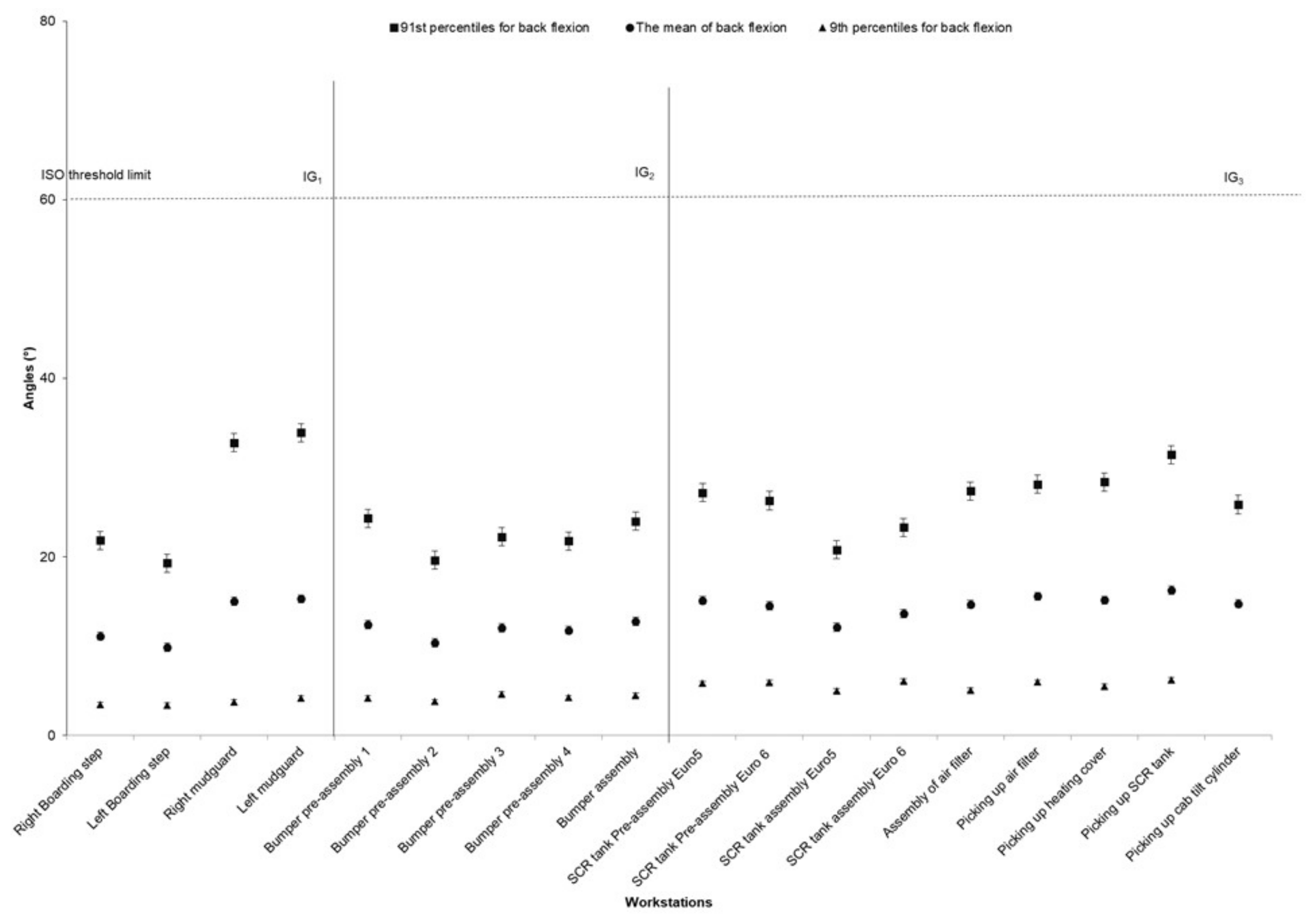
3.1. Neck and Back Risk Exposure
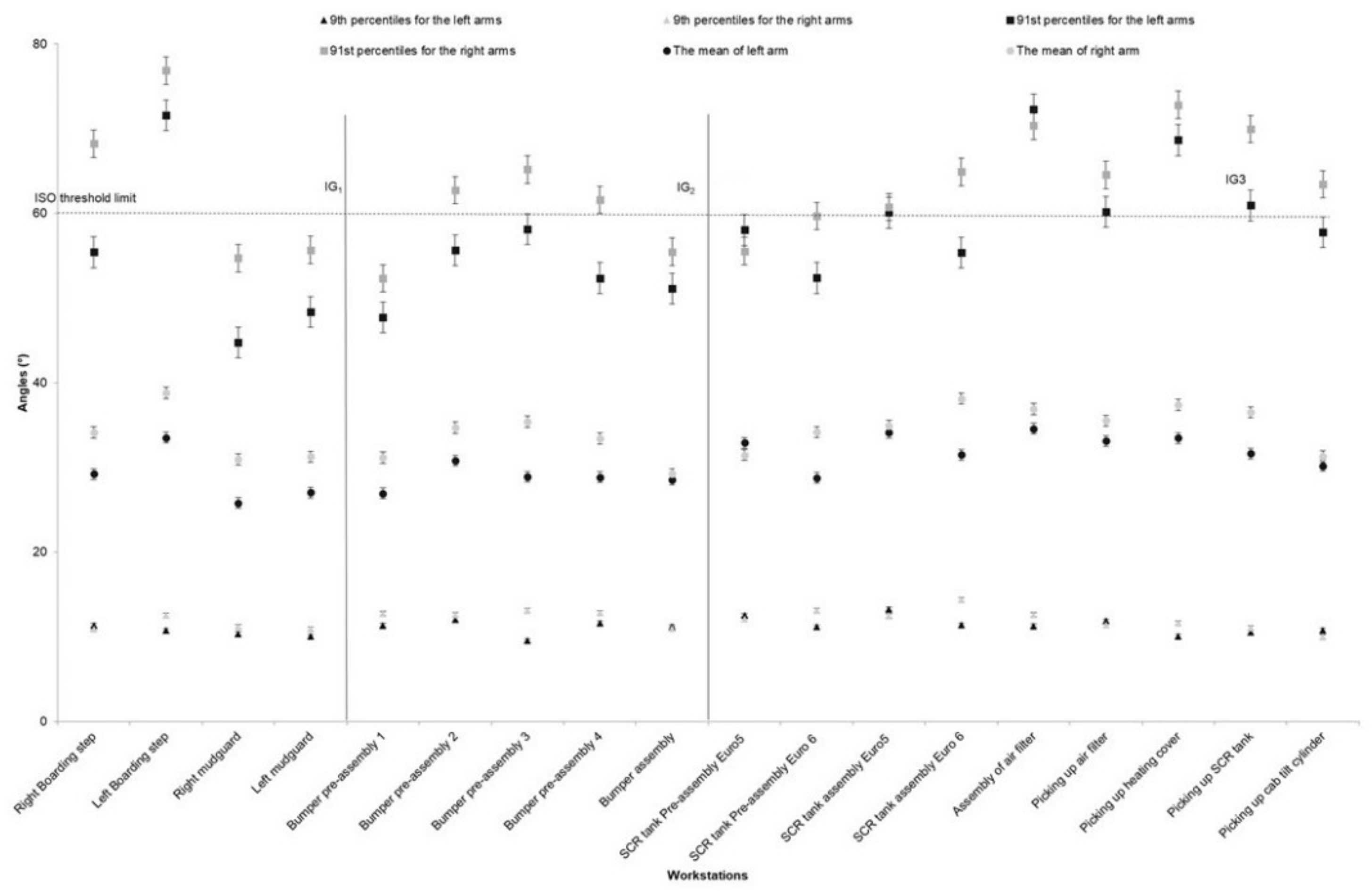
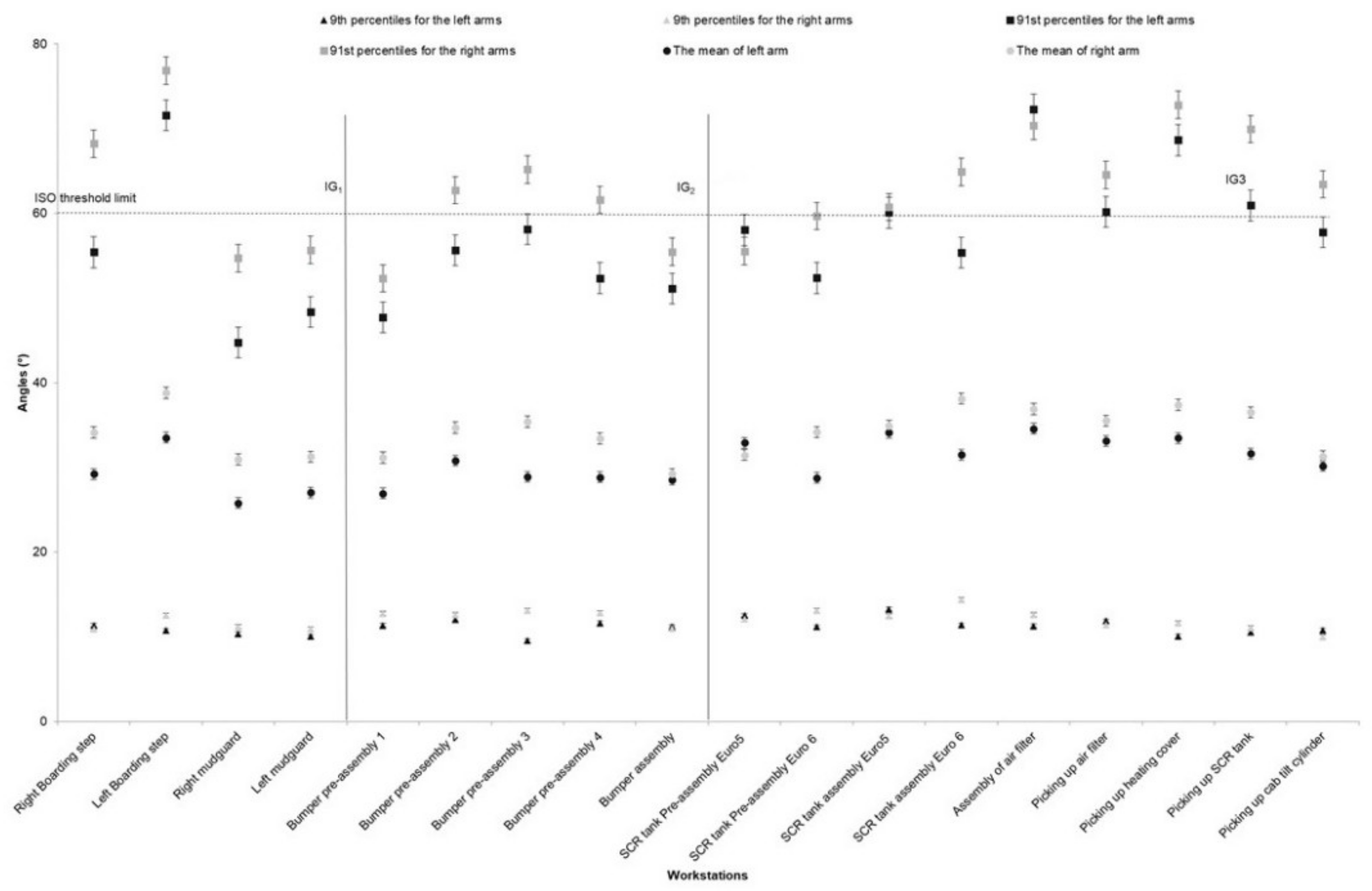
3.2. Arms Risk Exposure
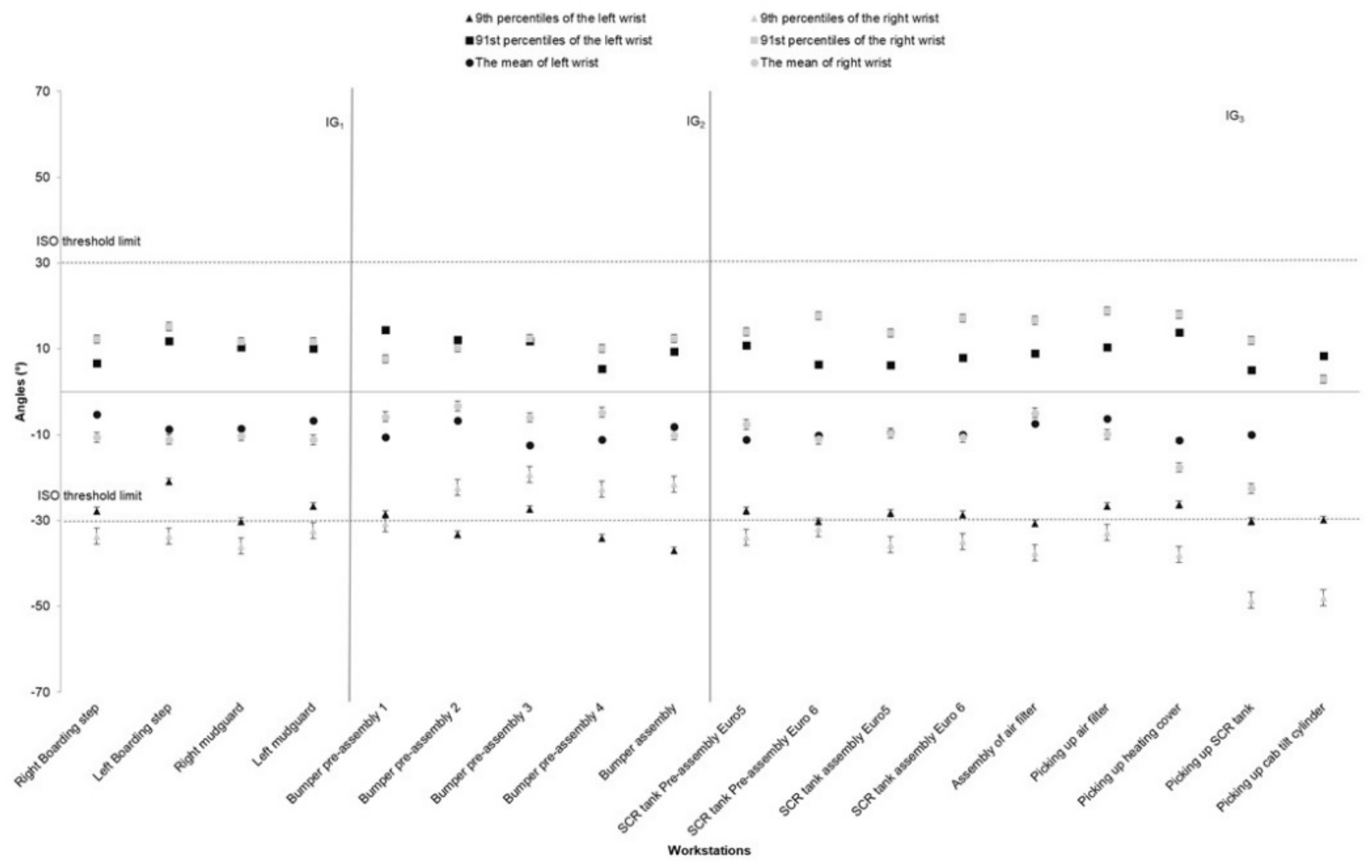
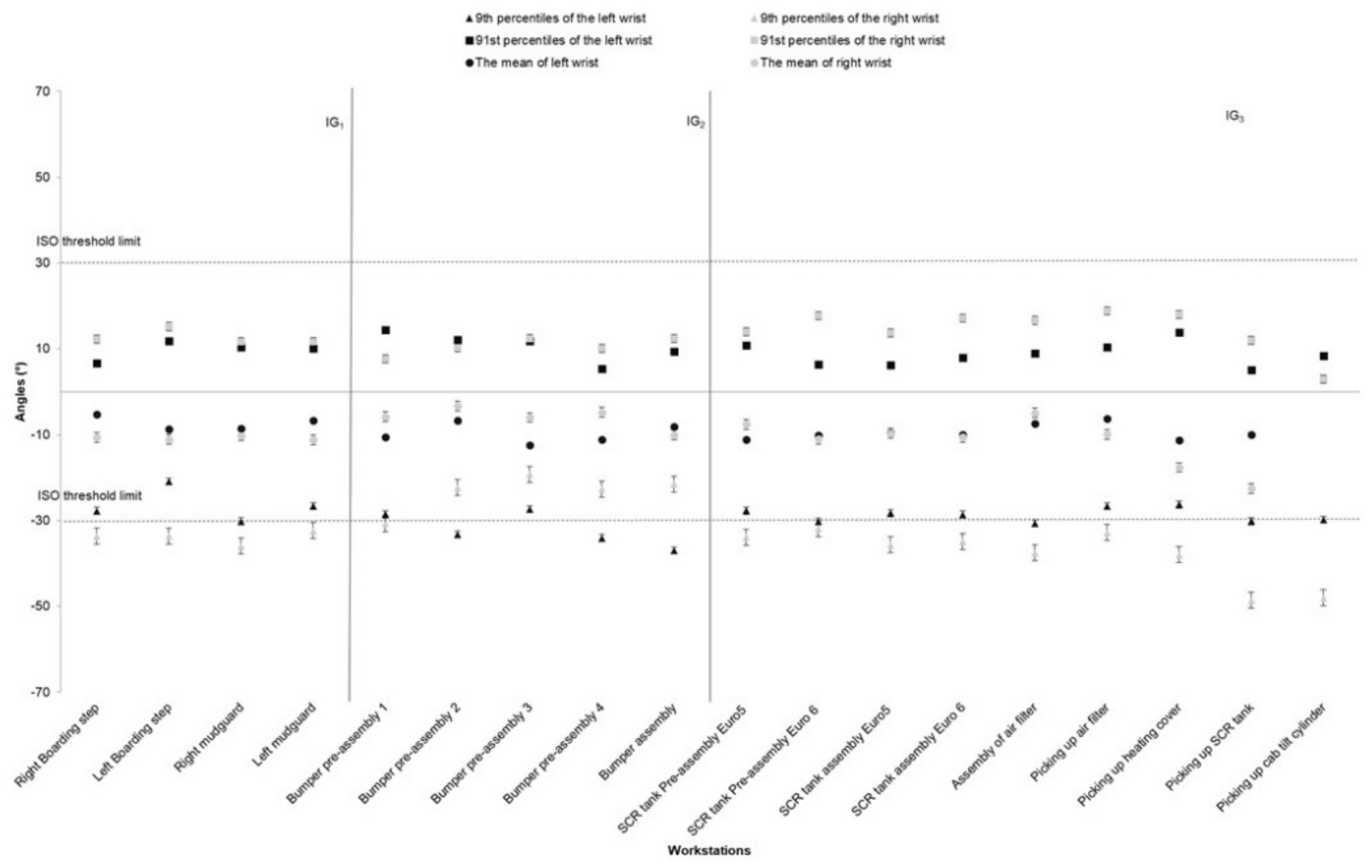
3.3. Wrists Risk Exposure
3.4. Movement of Body Segments
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- CNAM-TS. Données 2016 des Accidents du Travail et Maladies Professionnelles; Caisse Nationale D’assurance Maladie des Travailleurs Salariés: Paris, France, 2017.
- Roquelaure, Y.; Ha, C.; Leclerc, A.; Touranchet, A.; Sauteron, M.; Melchior, M.; Imbernon, E.; Goldberg, M. Epidemiologic surveillance of upper-extremity musculoskeletal disorders in the working population. Arthritis Care Res. 2006, 55, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Hägg, G.M. Corporate initiatives in ergonomics—An introduction. Appl. Ergon. 2003, 34, 3–15. [Google Scholar] [CrossRef]
- Neumann, W.P.; Village, J. Ergonomics action research II: A framework for integrating HF into work system design. Ergonomics 2012, 55, 1140–1156. [Google Scholar] [CrossRef]
- Zare, M.; Sagot, J.-C.; Roquelaure, Y. Within and between Individual Variability of Exposure to Work-Related Musculoskeletal Disorder Risk Factors. Int. J. Environ. Res. Public. Health 2018, 15, 1003. [Google Scholar] [CrossRef] [Green Version]
- Takala, E.-P.; Pehkonen, I.; Forsman, M.; Hansson, G.A.; Mathiassen, S.E.; Neumann, W.P.; Sjøgaard, G.; Veiersted, K.B.; Westgaard, R.H.; Winkel, J. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand. J. Work. Environ. Health 2010, 3–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falck, A.-C.; Örtengren, R.; Högberg, D. The impact of poor assembly ergonomics on product quality: A cost–benefit analysis in car manufacturing. Hum. Factors Ergon. Manuf. Serv. Ind. 2010, 20, 24–41. [Google Scholar] [CrossRef]
- Malaisé, A.; Maurice, P.; Colas, F.; Charpillet, F.; Ivaldi, S. Activity Recognition with Multiple Wearable Sensors for Industrial Applications. In Proceedings of the Advances in Computer-Human Interactions, Rome, Italy, 25–29 March 2018. [Google Scholar]
- Murray, M.; Lange, B.; Chreiteh, S.S.; Olsen, H.B.; Nørnberg, B.R.; Boyle, E.; Søgaard, K.; Sjøgaard, G. Neck and shoulder muscle activity and posture among helicopter pilots and crew-members during military helicopter flight. J. Electromyogr. Kinesiol. 2016, 27, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Schall, M.C.; Fethke, N.B.; Chen, H. Working postures and physical activity among registered nurses. Appl. Ergon. 2016, 54, 243–250. [Google Scholar] [CrossRef]
- Nordander, C.; Hansson, G.A.; Ohlsson, K.; Arvidsson, I.; Balogh, I.; Strömberg, U.; Rittner, R.; Skerfving, S. Exposure–response relationships for work-related neck and shoulder musculoskeletal disorders–Analyses of pooled uniform data sets. Appl. Ergon. 2016, 55, 70–84. [Google Scholar] [CrossRef]
- Granzow, R.F.; Schall, M.C.; Smidt, M.F.; Chen, H.; Fethke, N.B.; Huangfu, R. Characterizing exposure to physical risk factors among reforestation hand planters in the Southeastern United States. Appl. Ergon. 2018, 66, 1–8. [Google Scholar] [CrossRef]
- McClellan, A.J.; Albert, W.J.; Fischer, S.L.; Seaman, F.A.; Callaghan, J.P. Shoulder loading while performing automotive parts assembly tasks: A field study. Occup. Ergon. 2009, 8, 81–90. [Google Scholar] [CrossRef]
- Punnett, L.; Fine, L.J.; Keyserling, W.M.; Herrin, G.D.; Chaffin, D.B. Shoulder disorders and postural stress in automobile assembly work. Scand. J. Work. Environ. Health 2000, 26, 283–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordander, C.; Ohlsson, K.; Åkesson, I.; Arvidsson, I.; Balogh, I.; Hansson, G.-Å.; Strömberg, U.; Rittner, R.; Skerfving, S. Exposure–response relationships in work-related musculoskeletal disorders in elbows and hands—A synthesis of group-level data on exposure and response obtained using uniform methods of data collection. Appl. Ergon. 2013, 44, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Liljedahl, A.; Muftic, A. Managing Production Deviations: A Case Study at Scania AB; Master of Science—Production Engineering and Management, KTH: Stockholm, Sweden, 2012. [Google Scholar]
- Hansson, G.A.; Balogh, I.; Byström, J.U.; Ohlsson, K.; Nordander, C.; Asterland, P.; Sjölander, S.; Rylander, L.; Winkel, J.; Skerfving, S.; et al. Questionnarie versus direct technical measurements in assessing postures and movements of the head, upper back, arms and hands. Scand. J. Work. Environ. Health 2001, 27, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazmierczak, K.; Mathiassen, S.E.; Forsman, M.; Winkel, J. An integrated analysis of ergonomics and time consumption in Swedish ‘craft-type’ car disassembly. Appl. Ergon. 2005, 36, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Zare, M.; Biau, S.; Brunet, R.; Gourlay, A.; Roquelaure, Y. A comparison of neck bending and flexion measurement methods for assessment of ergonomic risk. Int. J. Occup. Saf. Ergon. 2015, 21, 330–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernmark, E.; Wiktorin, C. A triaxial accelerometer for measuring arm movements. Appl. Ergon. 2002, 33, 541–547. [Google Scholar] [CrossRef]
- Zare, M.; Malinge-Oudenot, A.; Höglund, R.; Biau, S.; Roquelaure, Y. Evaluation of ergonomic physical risk factors in a truck manufacturing plant: Case study in SCANIA Production Angers. Ind. Health 2016, 54, 163–176. [Google Scholar] [CrossRef] [Green Version]
- Lowe, B.D. Accuracy and validity of observational estimates of shoulder and elbow posture. Appl. Ergon. 2004, 35, 159–171. [Google Scholar] [CrossRef]
- Lowe, B.D. Accuracy and validity of observational estimates of wrist and forearm posture. Ergonomics 2004, 47, 527–554. [Google Scholar] [CrossRef]
- Lowe, B.D.; Krieg, E.F. Relationships between observational estimates and physical measurements of upper limb activity. Ergonomics 2009, 52, 569–583. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.D.; Weir, P.; Andrews, D. Observation-Based Posture Assessment: Review of Current Practice and Recommendations for Improvement; Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH): Cincinnati, OH, USA, July 2014.
- International Organization for Standardization (ISO). Ergonomics—Evaluation of Static Working Postures; Standard No. ISO 11226:2000/COR 1:2006; ISO: Geneva, Switzerland, 2000. [Google Scholar]
- Ha, C.; Roquelaure, Y. Réseau Expérimental de Surveillance Epidémiologique des Troubles Musculo-Squelettiques Dans les Pays de la Loire: Protocole de la Surveillance dans les Entreprises (2002–2004) [Experimental Monitoring Network for the Epidemiological Surveillance of Musculoskeletal Disorders in the Pays de la Loire region: Surveillance Protocol in the Workplace (2002–2004)]; InVS: Saint-Maurice, France, 2007.
- Hansson, G.Å.; Balogh, I.; Ohlsson, K.; Granqvist, L.; Nordander, C.; Arvidsson, I.; Åkesson, I.; Unge, J.; Rittner, R.; Strömberg, U.; et al. Physical workload in various types of work: Part II. Neck, shoulder and upper arm. Int. J. Ind. Ergon. 2010, 40, 267–281. [Google Scholar] [CrossRef]
- Balogh, I.; Ørbæk, P.; Ohlsson, K.; Nordander, C.; Unge, J.; Winkel, J.; Hansson, G.Å.; Malmö Shoulder/Neck Study Group. Self-assessed and directly measured occupational physical activities—Influence of musculoskeletal complaints, age and gender. Appl. Ergon. 2004, 35, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Hansson, G.Å.; Arvidsson, I.; Ohlsson, K.; Nordander, C.; Mathiassen, S.E.; Skerfving, S.; Balogh, I. Precision of measurements of physical workload during standardised manual handling. Part II: Inclinometry of head, upper back, neck and upper arms. J. Electromyogr. Kinesiol. 2006, 16, 125–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdorf, A.; Laan, J. Comparison of methods for the assessment of postural load on the back. Scand. J. Work Environ. Health 1991, 425–429. [Google Scholar] [CrossRef]
- Driessen, M.T.; Proper, K.I.; van Tulder, M.W.; Anema, J.R.; Bongers, P.M.; van der Beek, A.J. The effectiveness of physical and organisational ergonomic interventions on low back pain and neck pain: A systematic review. Occup. Environ. Med. 2010, 67, 277–285. [Google Scholar] [CrossRef] [Green Version]
- Wai, E.K.; Roffey, D.M.; Bishop, P.; Kwon, B.K.; Dagenais, S. Causal assessment of occupational lifting and low back pain: Results of a systematic review. Spine J. 2010, 10, 554–566. [Google Scholar] [CrossRef]
- Kwon, B.K.; Roffey, D.M.; Bishop, P.B.; Dagenais, S.; Wai, E.K. Systematic review: Occupational physical activity and low back pain. Occup. Med. 2011, 61, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Balogh, I.; Ohlsson, K.; Nordander, C.; Skerfving, S.; Hansson, G.A. Precision of measurements of physical workload during standardized manual handling part III: Goniometry of the wrists. J. Electromyogr. Kinesiol. 2009, 19, 1005–1012. [Google Scholar] [CrossRef]
- Hansson, G.A.; Balogh, I.; Ohlsson, K.; Granqvist, L.; Nordander, C.; Arvidsson, I.; Åkesson, I.; Unge, J.; Rittner, R.; Strömberg, U. Physical workload in various types of work: Part I. Wrist and forearm. Int. J. Ind. Ergon. 2009, 39, 221–233. [Google Scholar] [CrossRef]
- Arvidsson, I.; Balogh, I.; Hansson, G.A.; Ohlsson, K.; Åkesson, I.; Nordander, C. Rationalization in meat cutting—Consequences on physical workload. Appl. Ergon. 2012, 43, 1026–1032. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Working Group | Number of Workstations | Number of Operators | Number of Operators Participated in the Study | Type of Task | Tool |
|---|---|---|---|---|---|
| Improvement group 1 (IG1) | 4 | 6 | 4 | Assembly of left/right boarding steps and left/right mudguards | Electric screwdrivers, hoists, Manual torque wrench |
| Improvement group 2 (IG2) | 5 | 7 | 5 | Preassembly and assembly of the bumper | Electric and pneumatic screwdrivers, nutrunners, trolleys |
| Improvement group 3 (IG3) | 5 | 8 | 4 | Preassembly and assembly of Selective Catalytic Reduction (SCR) system, preassembly and assembly of air filter, cab tilt cylinder and material picking | Electric and pneumatic screwdrivers, electric assembly systems |
| Body Segment | Low Risk (Green) | Moderate Risk (Yellow) | High Risk (Red) |
|---|---|---|---|
| Neck | −30° to 20° | 20° to 45° | >45° or <−30° |
| Back | 0° to 20° | 20° to 45° | >45° |
| Arms | 0° to 45° | 45° to 90° | >90° |
| Wrists | −30° to 45° | - | <−30° and >45° |
| Body Segment | Risk Zone | IG1 | IG2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| WS1 * Right Boarding Steps | WS 2 Left Boarding Steps | WS 3 Right Mudguard | WS 4 Left Mudguard | WS 1 Bumper Pre-Assembly | WS 2 Bumper Pre-Assembly | WS 3 Bumper Pre-Assembly | WS 4 Bumper Pre-Assembly | WS 5 Bumper Assembly | ||
| Neck (%) | Low | 53.3 | 68.6 | 57.1 | 55.3 | 58.1 | 47.1 | 69.9 | 59.9 | 59.1 |
| Moderate | 43.8 | 29.2 | 35.1 | 38.5 | 40.2 | 49.8 | 28.1 | 37.8 | 37.1 | |
| High | 2.9 | 2.2 | 7.8 | 6.2 | 1.7 | 3.1 | 2.0 | 2.3 | 3.8 | |
| Lower Back (%) | Low | 87.9 | 93.9 | 74.1 | 74.7 | 81.7 | 90.6 | 83.5 | 84.4 | 85.0 |
| Moderate | 11.6 | 6.0 | 25.0 | 23.2 | 17.9 | 9.0 | 16.3 | 14.7 | 13.0 | |
| High | 0.5 | 0.1 | 0.9 | 2.1 | 0.4 | 0.4 | 0.2 | 0.9 | 2.0 | |
| Right Arm (%) | Low | 73.3 | 68.3 | 79.8 | 79.9 | 81.1 | 73.2 | 74.3 | 76.4 | 82.7 |
| Moderate | 23.4 | 26.5 | 19.7 | 19.7 | 17.9 | 26.0 | 23.1 | 23.1 | 17.1 | |
| High | 3.3 | 5.2 | 0.5 | 0.4 | 1.0 | 0.8 | 2.6 | 0.5 | 0.2 | |
| Left Arm (%) | Low | 84.7 | 76.8 | 89.7 | 86.1 | 89.1 | 81.4 | 84.1 | 85.5 | 85.5 |
| Moderate | 13.4 | 19.7 | 10.2 | 13.8 | 10.9 | 18.0 | 15.1 | 14.0 | 13.9 | |
| High | 1.9 | 3.5 | 0.1 | 0.1 | 0 | 0.6 | 0.8 | 0.5 | 0.6 | |
| Right wrist (%) | Low | 83.7 | 84.7 | 84.9 | 84.1 | 88.3 | 97.3 | 95.6 | 96.8 | 96.1 |
| High | 16.3 | 15.3 | 15.1 | 15.9 | 11.7 | 2.7 | 4.4 | 3.2 | 3.9 | |
| Left wrist (%) | Low | 89.3 | 95.4 | 89.2 | 90.6 | 89.7 | 83.2 | 93.4 | 83.8 | 83.9 |
| High | 10.7 | 4.6 | 10.8 | 9.4 | 10.3 | 16.8 | 6.6 | 16.2 | 16.1 | |
| Body Segment | Risk Zone | WS1 * SCR Tank Pre-Assembly | WS 2 SCR Tank Assembly | WS 3 Assembly of Air Filter | WS 4 Picking up Air Filter | WS5 Picking up SCR Tank | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Euro5 ** | Euro6 ** | Euro5 | Euro6 | Air Filter | Heating Cover | SCR Tank | Cab Tilt Cylinder | |||
| Neck (%) | Low | 66.3 | 38.5 | 49.1 | 46.5 | 65.6 | 56.7 | 62.9 | 39.4 | 48.0 |
| Moderate | 29.3 | 57.0 | 36.0 | 47.3 | 30.9 | 40.1 | 32.6 | 54.7 | 46.3 | |
| High | 4.4 | 4.5 | 14.9 | 6.2 | 3.5 | 3.2 | 4.5 | 5.9 | 5.7 | |
| Lower Back (%) | Low | 88.8 | 84.2 | 76.8 | 79.6 | 79.4 | 78.0 | 73.6 | 78.9 | 77.3 |
| Moderate | 10.9 | 15.4 | 22.0 | 19.4 | 18.9 | 19.2 | 24.6 | 20.1 | 20.9 | |
| High | 0.3 | 0.4 | 1.2 | 1.0 | 1.7 | 2.8 | 1.8 | 1.0 | 1.8 | |
| Right Arm (%) | Low | 72.5 | 67.9 | 80.5 | 74.6 | 69.6 | 71.9 | 69.8 | 79.6 | 69.4 |
| Moderate | 26.6 | 31.5 | 19.2 | 25.0 | 27.8 | 26.7 | 27.4 | 19.2 | 27.0 | |
| High | 0.9 | 0.6 | 0.3 | 0.4 | 2.6 | 1.4 | 2.8 | 1.2 | 3.6 | |
| Left Arm (%) | Low | 75.4 | 77.5 | 76.9 | 84.0 | 74.3 | 77.9 | 78.0 | 81.0 | 73.3 |
| Moderate | 23.1 | 21.6 | 22.4 | 15.7 | 23.0 | 20.5 | 20.7 | 17.5 | 24.0 | |
| High | 1.5 | 0.9 | 0.7 | 0.3 | 2.7 | 1.6 | 1.3 | 1.5 | 2.7 | |
| Right wrist (%) | Low | 83.1 | 81.3 | 84.5 | 87.2 | 83.2 | 81.8 | 66.1 | 57.9 | 81.9 |
| High | 16.9 | 18.7 | 15.5 | 12.8 | 16.8 | 18.2 | 33.9 | 42.1 | 18.1 | |
| Left wrist (%) | Low | 89.9 | 90.7 | 91.6 | 89.8 | 89.9 | 89.8 | 90.0 | 86.7 | 92.6 |
| High | 10.1 | 9.3 | 8.4 | 10.2 | 10.1 | 10.2 | 10.0 | 13.3 | 7.4 | |
| Body Segment | Musculoskeletal Symptom (n = 11) | |
|---|---|---|
| n | % | |
| Neck, VAS * ≥ 5 | 1 | 9 |
| Arm, VAS ≥ 5 | 4 | 36 |
| Forearms, VAS ≥ 5 | 4 | 36 |
| Wrist and hands, VAS ≥ 5 | 3 | 27 |
| Fingers, VAS ≥ 5 | 2 | 18 |
| Upper back, VAS ≥ 5 | 2 | 18 |
| Lower back, VAS ≥ 5 | 3 | 27 |
| Hip and thigh, VAS ≥ 5 | 1 | 9 |
| Knee and leg, VAS ≥ 5 | 3 | 27 |
| Ankle/Foot, VAS ≥ 5 | 2 | 18 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zare, M.; Bodin, J.; Sagot, J.-C.; Roquelaure, Y. Quantification of Exposure to Risk Postures in Truck Assembly Operators: Neck, Back, Arms and Wrists. Int. J. Environ. Res. Public Health 2020, 17, 6062. https://doi.org/10.3390/ijerph17176062
Zare M, Bodin J, Sagot J-C, Roquelaure Y. Quantification of Exposure to Risk Postures in Truck Assembly Operators: Neck, Back, Arms and Wrists. International Journal of Environmental Research and Public Health. 2020; 17(17):6062. https://doi.org/10.3390/ijerph17176062
Chicago/Turabian StyleZare, Mohsen, Julie Bodin, Jean-Claude Sagot, and Yves Roquelaure. 2020. "Quantification of Exposure to Risk Postures in Truck Assembly Operators: Neck, Back, Arms and Wrists" International Journal of Environmental Research and Public Health 17, no. 17: 6062. https://doi.org/10.3390/ijerph17176062