Evaluation of Gross Motor Coordination and Physical Fitness in Children: Comparison between Soccer and Multisport Activities

 ,
,  , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedure
2.2.1. Motor Coordination
2.2.2. Physical Fitness
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting Public Health Priorities: Recommendations for Physical Education and Physical Activity Promotion in Schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Pion, J.; Vandendriessche, J.; Vandorpe, B.; Vaeyens, R.; Lenoir, M.; Philippaerts, R.M. Differences in physical fitness and gross motor coordination in boys aged 6–12 years specializing in one versus sampling more than one sport. J. Sports Sci. 2012, 30, 379–386. [Google Scholar] [CrossRef]
- Lai, S.K.; Costigan, S.A.; Morgan, P.J.; Lubans, D.R.; Stodden, D.F.; Salmon, J.; Barnett, L.M. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014, 44, 67–79. [Google Scholar] [CrossRef]
- Nazario, P.F.; Vieira, J.L.L. Sport context and the motor development of children. Braz. J. Kinanthrop. Hum. Perform. 2014, 16, 86–95. [Google Scholar]
- Queiroz, D.D.R.; Ré, A.H.N.; Henrique, R.D.S.; Moura, M.D.S.; Cattuzzo, M.T. Participation in sports practice and motor competence in preschoolers. Motriz. Rev. Educ. Fis. 2014, 20, 26–32. [Google Scholar] [CrossRef]
- Vandorpe, B.; Vandendriessche, J.; Vaeyens, R.; Pion, J.; Matthys, S.; Lefevre, J.; Philippaerts, R.; Lenoir, M. Relationship between sports participation and the level of motor coordination in childhood: A longitudinal approach. J. Sci. Med. Sport 2012, 15, 220–225. [Google Scholar] [CrossRef]
- Batista, M.B.; Romanzini, C.L.P.; Barbosa, C.C.L.; Shigaki, G.B.; Romanzini, M.; Ronque, E.R.V. Participation in sports in childhood and adolescence and physical activity in adulthood: A systematic review. J. Sports Sci. 2019, 37, 2253–2262. [Google Scholar] [CrossRef]
- Côté, J.; Fraser-Thomas, J. The health and developmental benefits of youth sport participation. In Sport Psychology: A Canadian Perspective; Pearson Education: London, UK, 2007; pp. 266–294. ISBN 01319657279780131. [Google Scholar]
- Côté, J.; Baker, J.; Abernethy, B. From Play to Practice: “A Developmental Framework for the Acquisition of Expertise in Team Sport”. In Expert Performance in Sports: Advances in Research on Sport Expertise; Human Kinetics: Champaign, IL, USA, 2003; pp. 89–110. [Google Scholar]
- Côté, J.; Baker, J.; Abernethy, B. Practice and play in the development of sport expertise. In Handbook of Sport Psychology, 3rd ed.; John Wiley: Hoboken, NJ, USA, 2007. [Google Scholar]
- Ford, P.R.; Ward, P.; Hodges, N.J.; Williams, A.M. The role of deliberate practice and play in career progression in sport: The early engagement hypothesis. High Abil. Stud. 2009, 20, 65–75. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Rizzo, N.S.; Hurtig-Wennlöf, A.; Ortega, F.B.; Wàrnberg, J.; Sjöström, M. Relations of total physical activity and intensity to fitness and fatness in children: The European Youth Heart Study. Am. J. Clin. Nutr. 2006, 84, 299–303. [Google Scholar] [CrossRef]
- Ortega, F.B.; Labayen, I.; Ruiz, J.R.; Kurvinen, E.; Loit, H.M.; Harro, J.; Veidebaum, T.; Sjöström, M. Improvements in fitness reduce the risk of becoming overweight across puberty. Med. Sci. Sports Exerc. 2011, 43, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Silventoinen, K.; Tynelius, P.; Rasmussen, F. Muscular strength in male adolescents and premature death: Cohort study of one million participants. BMJ 2012, 345, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Moliner-Urdiales, D.; Ortega, F.B.; Vicente-Rodriguez, G.; Rey-Lopez, J.P.; Gracia-Marco, L.; Widhalm, K.; Sjöström, M.; Moreno, L.A.; Castillo, M.J.; Ruiz, J.R. Association of physical activity with muscular strength and fat-free mass in adolescents: The HELENA study. Eur. J. Appl. Physiol. 2010, 109, 1119–1127. [Google Scholar] [CrossRef]
- Morales, P.F.; Sánchez-López, M.; Moya-Martínez, P.; García-Prieto, J.C.; Martínez-Andrés, M.; García, N.L.; Martínez-Vizcaíno, V. Health-related quality of life, obesity, and fitness in schoolchildren: The Cuenca study. Qual. Life Res. 2013, 22, 1515–1523. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- Catley, M.J.; Tomkinson, G.R. Normative health-related fitness values for children: Analysis of 85347 test results on 9–17-year-old Australians since 1985. Br. J. Sports Med. 2013, 47, 98–108. [Google Scholar] [CrossRef]
- Lopes, V.P.; Stodden, D.F.; Bianchi, M.M.; Maia, J.A.R.; Rodrigues, L.P. Correlation between BMI and motor coordination in children. J. Sci. Med. Sport 2012, 15, 38–43. [Google Scholar] [CrossRef]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef]
- Venetsanou, F.; Kambas, A. Environmental Factors Affecting Preschoolers’ Motor Development. Early Child. Educ. J. 2010, 37, 319–327. [Google Scholar] [CrossRef]
- Morgan, P.J.; Barnett, L.M.; Cliff, D.P.; Okely, A.D.; Scott, H.A.; Cohen, K.E.; Lubans, D.R. Fundamental movement skill interventions in youth: A systematic review and meta-analysis. Pediatrics 2013, 132, 1361–1383. [Google Scholar] [CrossRef]
- Bardid, F.; Rudd, J.R.; Lenoir, M.; Polman, R.; Barnett, L.M. Cross-cultural comparison of motor competence in children from Australia and Belgium. Front. Psychol. 2015, 6, 964–972. [Google Scholar] [CrossRef]
- Bogataj, Š.; Pajek, J.; Ponikvar, J.B.; Hadžić, V.; Pajek, M. Kinesiologist-guided functional exercise in addition to intradialytic cycling program in end-stage kidney disease patients: A randomised controlled trial. Sci. Rep. 2020, 10, 5717–5726. [Google Scholar] [CrossRef]
- McAuley, E.; Lox, C.; Duncan, T.E. Long-term Maintenance of Exercise, Self-Efficacy, and Physiological Change in Older Adults. J. Gerontol. 1993, 48, 218–224. [Google Scholar] [CrossRef]
- Sember, V.; Starc, G.; Jurak, G.; Golobič, M.; Kovač, M.; Samardžija, P.P.; Morrison, S.A. Results from the republic of Slovenia’s 2016 report card on physical activity for children and youth. J. Phys. Act. Heal. 2016, 13, 256–264. [Google Scholar] [CrossRef][Green Version]
- Bogataj, Š.; Pajek, M.; Andrašić, S.; Trajković, N. Concurrent Validity and Reliability of My Jump 2 App for Measuring Vertical Jump Height in Recreationally Active Adults. Appl. Sci. 2020, 10, 3805. [Google Scholar] [CrossRef]
- Reid, R.E.R.; Fillon, A.; Thivel, D.; Henderson, M.; Barnett, T.A.; Bigras, J.L.; Mathieu, M.E. Can anthropometry and physical fitness testing explain physical activity levels in children and adolescents with obesity? J. Sci. Med. Sport 2020, 23, 580–585. [Google Scholar] [CrossRef]
- Bogataj, Š.; Pajek, M.; Hadžić, V.; Andrašić, S.; Padulo, J.; Trajković, N. Validity, Reliability, and Usefulness of My Jump 2 App for Measuring Vertical Jump in Primary School Children. Int. J. Environ. Res. Public Health 2020, 17, 3708. [Google Scholar] [CrossRef]
- Barreiros, A.; Côté, J.; Fonseca, A.M. From early to adult sport success: Analysing athletes’ progression in national squads. Eur. J. Sport Sci. 2014, 14, 1–5. [Google Scholar] [CrossRef]
- Barreiros, A.; Côté, J.; Fonseca, A.M. Training and psychosocial patterns during the early development of Portuguese national team athletes. High Abil. Stud. 2013, 24, 49–61. [Google Scholar] [CrossRef][Green Version]
- Kiphard, E.; Schilling, F. Körperkoordinationstest für Kinder: KTK; Beltz Test GmbH: Weinheim, Germany, 2007. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Inc.: New York, NY, USA, 1988. [Google Scholar]
- Trajković, N.; Bogataj, Š. Effects of neuromuscular training on motor competence and physical performance in young female volleyball players. Int. J. Environ. Res. Public Health 2020, 17, 1755. [Google Scholar] [CrossRef]
- Goodway, J.; Ozmun, J.; Gallahue, D. Understanding Motor Development: Infants, Children, Adolescents, Adults; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Goodway, J.; Crystal, F. Influence of a Motor Skill Intervention on Fundamental Motor Skill Development of Disadvantaged Preschool Children. Res. Q. Exerc. Sport 2003, 74, 36–46. [Google Scholar] [CrossRef]
- Šalaj, S.; Krmpotić, M.; Stamenković, I. Are specific programs a threat to overall motor development of preschool children? Kinesiol. Slov. 2016, 22, 47–55. [Google Scholar]
- Jaakkola, T.; Watt, A.; Kalaja, S. Differences in the Motor Coordination Abilities among Adolescent Gymnasts, Swimmers, and Ice Hockey Players. Hum. Mov. 2017, 18, 44–49. [Google Scholar] [CrossRef]
- Söğüt, M. Gross Motor Coordination in Junior Tennis Players. J. Sports Sci. 2016, 34, 2149–2152. [Google Scholar] [CrossRef]
- Haugen, T.; Johansen, B.T. Difference in Physical Fitness in Children with Initially High and Low Gross Motor Competence: A Ten-Year Follow-up Study. Hum. Mov. Sci. 2018, 62, 143–149. [Google Scholar] [CrossRef]
- López-Gil, J.F.; Brazo-Sayavera, J.; Lucas, J.L.Y.; Cavichiolli, F.R. Weight Status Is Related to Health-Related Physical Fitness and Physical Activity but Not to Sedentary Behaviour in Children. Int. J. Environ. Res. Public Health 2020, 17, 4518. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Soccer | Multisport |
|---|---|---|
| Age (years) | 7.49 ± 0.90 | 7.79 ± 0.68 |
| Body height (cm) | 125.73 ± 5.85 | 128.83 ± 5.85 |
| Body mass (kg) | 24.11 ± 4.97 | 27.62 ± 6.72 |
| BMI (weight (kg)/height (m2)) | 15.29 ± 2.31 | 15.34 ± 2.91 |
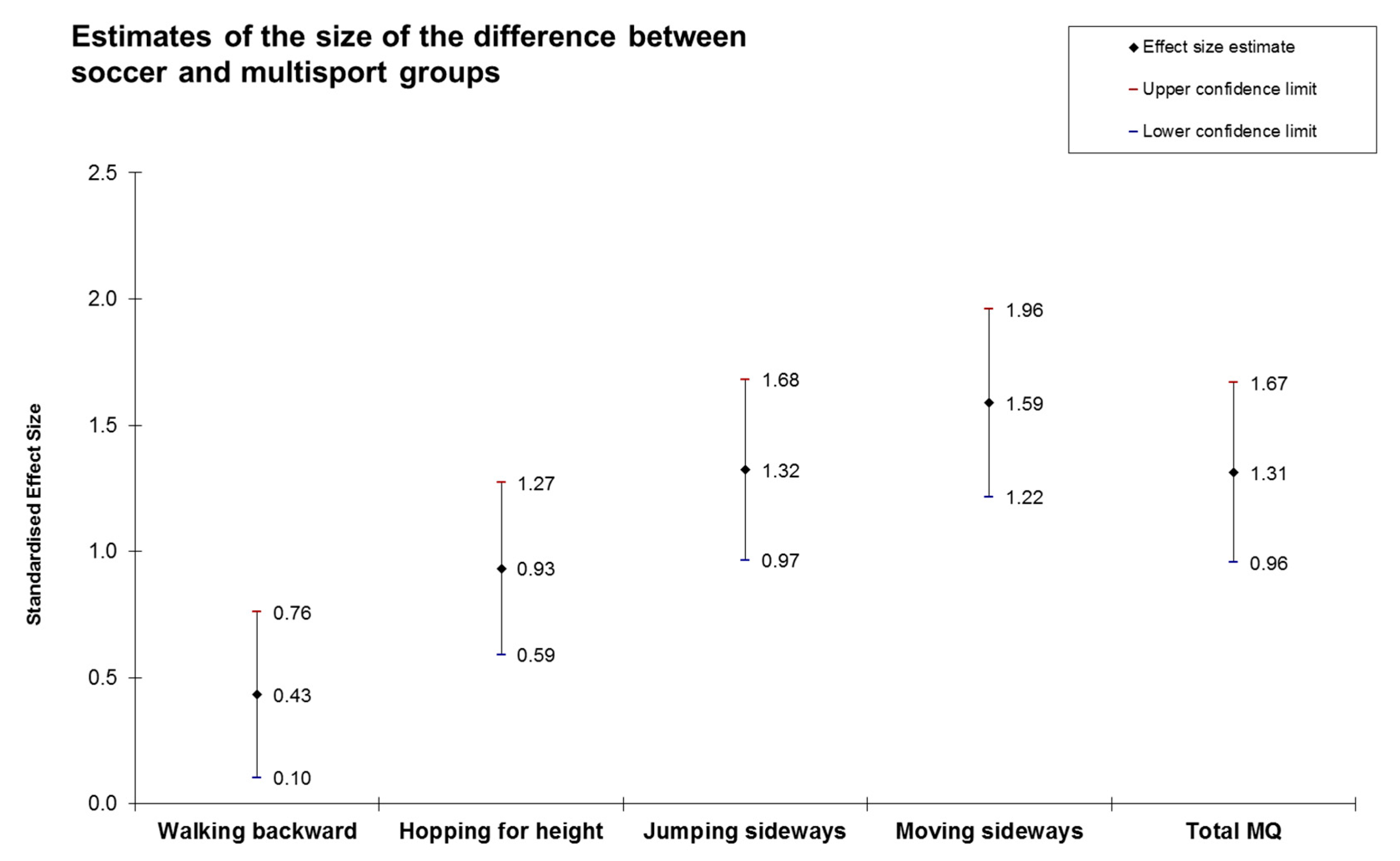
| Motor Coordination Tests | Soccer | Multisport | ANCOVA | ||
|---|---|---|---|---|---|
| GROUP F(1, 144) | AGE F(1, 144) | GENDER F(1, 144) | |||
| Walking backward | 32.21 ± 14.65 | 38.41 ± 13.93 | 6.18 * | 1.28 | 0.94 |
| Hopping for height | 30.95 ± 10.98 | 42.27 ± 12.99 | 30.60 ** | 3.07 | 5.04 * |
| Jumping sideways | 40.18 ± 11.16 | 57.19 ± 14.10 | 54.77 ** | 6.84 * | 1.32 |
| Moving sideways | 29.93 ± 5.76 | 39.31 ± 5.98 | 77.82 ** | 6.1 * | 1.69 |
| Total MQ | 91.39 ± 16.61 | 111.86 ± 14.45 | 58.97 ** | 4.25 * | 6.49 * |
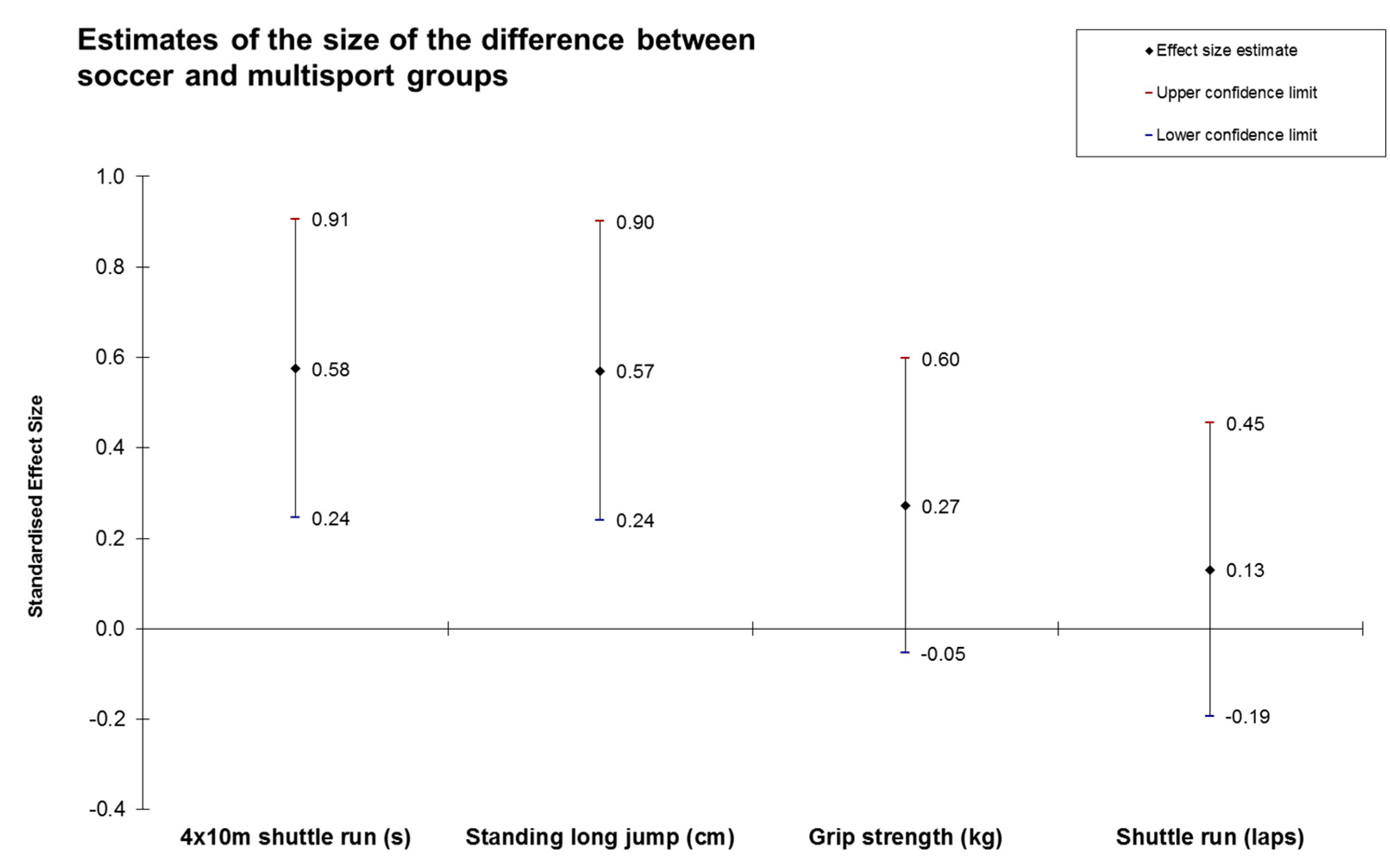
| Physical Fitness Tests | Soccer | Multisport | ANCOVA | ||
|---|---|---|---|---|---|
| GROUP F(1, 144) | AGE F(1, 144) | GENDER F(1, 144) | |||
| 4 × 10 m shuttle run (s) ¥ | 13.81 ± 0.88 | 14.27 ± 0.71 | 0.01 | 0.51 | 0.36 |
| Standing long jump (cm) | 118.81 ± 15.01 | 127.08 ± 13.27 | 0.62 | 0.02 | 1.77 |
| Handgrip strength (kg) | 12.43 ± 2.24 | 13.22 ± 2.89 | 0.01 | 0.78 | 8.01 ** |
| 20 m shuttle run (laps) | 37.05 ± 9.23 | 38.22 ± 8.62 | 1.07 | 0.00 | 6.49 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popović, B.; Gušić, M.; Radanović, D.; Andrašić, S.; Madić, D.M.; Mačak, D.; Stupar, D.; Đukić, G.; Grujičić, D.; Trajković, N. Evaluation of Gross Motor Coordination and Physical Fitness in Children: Comparison between Soccer and Multisport Activities. Int. J. Environ. Res. Public Health 2020, 17, 5902. https://doi.org/10.3390/ijerph17165902
Popović B, Gušić M, Radanović D, Andrašić S, Madić DM, Mačak D, Stupar D, Đukić G, Grujičić D, Trajković N. Evaluation of Gross Motor Coordination and Physical Fitness in Children: Comparison between Soccer and Multisport Activities. International Journal of Environmental Research and Public Health. 2020; 17(16):5902. https://doi.org/10.3390/ijerph17165902
Chicago/Turabian StylePopović, Boris, Marko Gušić, Danilo Radanović, Slobodan Andrašić, Dejan M. Madić, Draženka Mačak, Dušan Stupar, Goran Đukić, Dragan Grujičić, and Nebojša Trajković. 2020. "Evaluation of Gross Motor Coordination and Physical Fitness in Children: Comparison between Soccer and Multisport Activities" International Journal of Environmental Research and Public Health 17, no. 16: 5902. https://doi.org/10.3390/ijerph17165902
APA StylePopović, B., Gušić, M., Radanović, D., Andrašić, S., Madić, D. M., Mačak, D., Stupar, D., Đukić, G., Grujičić, D., & Trajković, N. (2020). Evaluation of Gross Motor Coordination and Physical Fitness in Children: Comparison between Soccer and Multisport Activities. International Journal of Environmental Research and Public Health, 17(16), 5902. https://doi.org/10.3390/ijerph17165902