Household Air Pollution and Angina Pectoris in Low- and Middle-Income Countries: Cross-Sectional Evidence from the World Health Survey 2002–2003




Abstract
1. Introduction
2. Methods
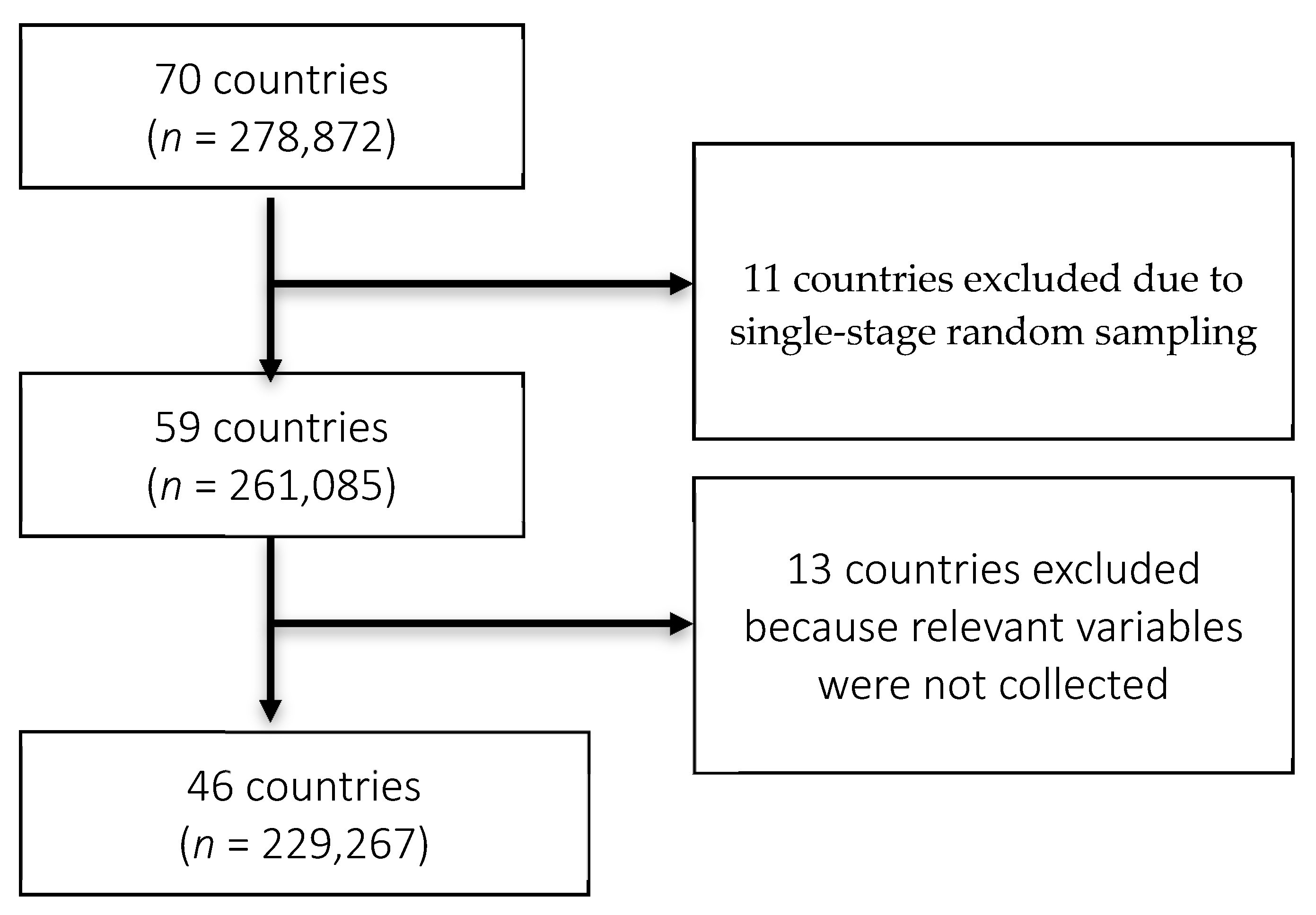
2.1. Study Population
2.2. Exposure
2.3. Outcome
2.4. Statistical Analysis
3. Results
3.1. Pooled Results (Angina Pectoris- Diagnosed, Treated, or Rose Criteria)
3.2. Sex-Stratified Distribution of Angina Pectoris—Diagnosed, Treated or Rose Criteria
4. Discussions
4.1. Household Fuel Use and Angina Pectoris
4.2. Sex Stratified Differences in Angina Pectoris and Household Fuel Use
4.3. Ambient Air Pollution and Angina Pectoris
4.4. Smoking and Angina Pectoris
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Household Air Pollution and Health. Available online: https://www.who.int/en/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 6 September 2019).
- Rana, J.; Uddin, J.; Peltier, R.; Oulhote, Y. Associations between Indoor Air Pollution and Acute Respiratory Infections among Under-Five Children in Afghanistan: Do SES and Sex Matter? Int. J. Environ. Res. Public Health 2019, 16, 2910. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.S.; Yacyshyn, E.; Jhangri, G.S.; Chopra, A.; Parmar, D.; Jones, C.A. Household Air Pollution and Arthritis in Lowand Middle-Income Countries: Cross-Sectional Evidence from the World Health Organization’s Study on Global Ageing and Adult Health. PLoS ONE 2019, 14, e0226738. [Google Scholar] [CrossRef] [PubMed]
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 23 May 2020).
- Von Klot, S.; Peters, A.; Aalto, P.; Bellander, T.; Berglind, N.; D’Ippoliti, D.; Elosua, R.; Hörmann, A.; Kulmala, M.; Lanki, T.; et al. Ambient Air Pollution Is Associated with Increased Risk of Hospital Cardiac Readmissions of Myocardial Infarction Survivors in Five European Cities. Circulation 2005, 112, 3073–3079. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; De Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long Term Exposure to Ambient Air Pollution and Incidence of Acute Coronary Events: Prospective Cohort Study and Meta-Analysis in 11 European Cohorts from the Escape Project. BMJ 2014, 348, f7412. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.L.; Donaldson, K.; Hadoke, P.W.; Boon, N.A.; MacNee, W.; Cassee, F.R.; Sandström, T.; Blomberg, A.; Newby, D.E. Adverse Cardiovascular Effects of Air Pollution. Nat. Clin. Pract. Cardiovasc. Med. 2008, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Angina—Symptoms and Causes—Mayo Clinic. Available online: https://www.mayoclinic.org/diseases-conditions/angina/symptoms-causes/syc-20369373 (accessed on 29 June 2020).
- Moran, A.E.; Forouzanfar, M.H.; Roth, G.A.; Mensah, G.A.; Ezzati, M.; Flaxman, A.; Murray, C.J.L.; Naghavi, M. The Global Burden of Ischemic Heart Disease in 1990 and 2010: The Global Burden of Disease 2010 Study. Circulation 2014, 129, 1493–1501. [Google Scholar] [CrossRef]
- Lee, W.; Hwang, S.H.; Choi, H.; Kim, H. The Association between Smoking or Passive Smoking and Cardiovascular Diseases Using a Bayesian Hierarchical Model: Based on the 2008–2013 Korea Community Health Survey. Epidemiol. Health 2017, 39, e2017026. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Chrysohoou, C.; Skoumas, J.; Tzioumis, K.; Stefanadis, C.; Toutouzas, P. Association between Exposure to Environmental Tobacco Smoke and the Development of Acute Coronary Syndromes: The CARDIO2000 Case-Control Study. Tob. Control 2002, 11, 220–225. [Google Scholar] [CrossRef]
- Lin, C.A.; Amador Pereira, L.A.; De Souza Conceição, G.M.; Kishi, H.S.; Milani, R.J.; Ferreira Braga, A.L.; Nascimento Saldiva, P.H.; de Souza Conceicao, G.M.; Kishi, H.S.; Milani, R.J.; et al. Association between Air Pollution and Ischemic Cardiovascular Emergency Room Visits. Environ. Res. 2003, 92, 57–63. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Chrysohoou, C.; Pitsavos, C.; Papaioannou, I.; Skoumas, J.; Stefanadis, C.; Toutouzas, P. The Association between Secondhand Smoke and the Risk of Developing Acute Coronary Syndromes, among Non-Smokers, under the Presence of Several Cardiovascular Risk Factors: The CARDIO2000 Case-Control Study. BMC Public Health 2002, 2, 9. [Google Scholar] [CrossRef]
- Xie, J.; He, M.; Zhu, W. Acute Effects of Outdoor Air Pollution on Emergency Department Visits Due to Five Clinical Subtypes of Coronary Heart Diseases in Shanghai, China. J. Epidemiol. 2014, 24, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Hemingway, H.; Langenberg, C.; Damant, J.; Frost, C.; Pyörälä, K.; Barrett-Connor, E. Prevalence of Angina in Women versus Men: A Systematic Review and Meta-Analysis of International Variations across 31 Countries. Circulation 2008, 117, 1526–1536. [Google Scholar] [CrossRef] [PubMed]
- Aronow, W.S. Effect of Passive Smoking on Angina Pectoris. N. Engl. J. Med. 1978, 299, 21–24. [Google Scholar] [CrossRef] [PubMed]
- Rabinoff, M. Passive Smoking and Coronary Heart Disease. N. Engl. J. Med. 1999, 341, 699–700. [Google Scholar] [PubMed]
- Hosseinpoor, A.R.; Forouzanfar, M.H.; Yunesian, M.; Asghari, F.; Naieni, K.H.; Farhood, D. Air Pollution and Hospitalization Due to Angina Pectoris in Tehran, Iran: A Time-Series Study. Environ. Res. 2005, 99, 126–131. [Google Scholar] [CrossRef]
- Lee, M.S.; Hang, J.Q.; Zhang, F.Y.; Dai, H.L.; Su, L.; Christiani, D.C. In-Home Solid Fuel Use and Cardiovascular Disease: A Cross-Sectional Analysis of the Shanghai Putuo Study. Environ. Health A Glob. Access Sci. Source 2012, 11, 18. [Google Scholar] [CrossRef]
- Chatterji, S.; Kowal, P.; Mathers, C.; Naidoo, N.; Verdes, E.; Smith, J.P.; Suzman, R. The Health of Aging Populations in China and India. Health Aff. 2008, 27, 1052–1063. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Parikh, J.; Sankar, S.; Padmavathi, R.; Srividya, K.; Venugopal, V.; Prasad, S.; Pandey, V.L. Daily Average Exposures to Respirable Particulate Matter from Combustion of Biomass Fuels in Rural Households of Southern India. Environ. Health Perspect. 2002, 110, 1069–1075. [Google Scholar] [CrossRef]
- Parikh, J. Hardships and Health Impacts on Women Due to Traditional Cooking Fuels: A Case Study of Himachal Pradesh, India. Energy Policy 2011, 39, 7587–7594. [Google Scholar] [CrossRef]
- Torres-Duque, C.; Maldonado, D.; Perez-Padilla, R.; Ezzati, M.; Viegi, G. Biomass Fuels and Respiratory Diseases: A Review of the Evidence. Proc. Am. Thorac. Soc. 2008, 5, 577–590. [Google Scholar] [CrossRef]
- Palipudi, K.M.; Gupta, P.C.; Sinha, D.N.; Andes, L.J.; Asma, S.; McAfee, T. Social Determinants of Health and Tobacco Use in Thirteen Low and Middle Income Countries: Evidence from Global Adult Tobacco Survey. PLoS ONE 2012, 7, e33466. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Parker, L.A.; Tursan d’Espaignet, E.; Chatterji, S. Socioeconomic Inequality in Smoking in Low-Income and Middle-Income Countries: Results from the World Health Survey. PLoS ONE 2012, 7, e42843. [Google Scholar] [CrossRef] [PubMed]
- Loerbroks, A.; Bosch, J.A.; Mommersteeg, P.M.C.; Herr, R.M.; Angerer, P.; Li, J. The Association of Depression and Angina Pectoris across 47 Countries: Findings from the 2002 World Health Survey. Eur. J. Epidemiol. 2014, 29, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Mommersteeg, P.M.C.; Herr, R.; Pouwer, F.; Holt, R.I.G.; Loerbroks, A. The Association between Diabetes and an Episode of Depressive Symptoms in the 2002 World Health Survey: An Analysis of 231 797 Individuals from 47 Countries. Diabet. Med. 2013, 30, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Loerbroks, A.; Bosch, J.A.; Sheikh, A.; Yamamoto, S.; Herr, R.M. Reports of Wheezing and of Diagnosed Asthma Are Associated with Impaired Social Functioning: Secondary Analysis of the Cross-Sectional World Health Survey Data. J. Psychosom. Res. 2018, 105, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Üstün, B.; Chatterji, S.; Villanueva, M.; Benib, L. WHO Multi-Country Survey Study on Health and Responsiveness 2000-2001. 2001. Available online: https://www.semanticscholar.org/paper/WHO-Multi-country-Survey-Study-on-Health-and-%C3%9Cst%C3%BCn-Chatterji/5e6db20961c15c0c349ff37d779e5c1d7ac21d2f (accessed on 23 May 2020).
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, Chronic Diseases, and Decrements in Health: Results from the World Health Surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]
- Fullerton, D.G.; Bruce, N.; Gordon, S.B. Indoor Air Pollution from Biomass Fuel Smoke Is a Major Health Concern in the Developing World. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 843–851. [Google Scholar] [CrossRef]
- Kim, K.H.; Jahan, S.A.; Kabir, E. A Review of Diseases Associated with Household Air Pollution Due to the Use of Biomass Fuels. J. Hazard. Mater. 2011, 192, 425–431. [Google Scholar] [CrossRef]
- Romieu, I.; Riojas-Rodríguez, H.; Marrón-Mares, A.T.; Schilmann, A.; Perez-Padilla, R.; Masera, O. Improved Biomass Stove Intervention in Rural Mexico: Impact on the Respiratory Health of Women. Am. J. Respir. Crit. Care Med. 2009, 180, 649–656. [Google Scholar] [CrossRef]
- WHO. World Health Survey Guide to Administration and Question by Question Specifications. 2002. Available online: http://www.who.int/healthinfo/survey/whsshortversionguide.pdf (accessed on 10 August 2020).
- Desalu, O.O.; Adekoya, A.O.; Ampitan, B.A. Risco Aumentado de Sintomas Respiratórios e Bronquite Crônica Em Mulheres Que Utilizam Biocombustíveis Na Nigéria. J. Bras. Pneumol. 2010, 36, 441–446. [Google Scholar] [CrossRef]
- Fatmi, Z.; Ntani, G.; Coggon, D. Coronary Heart Disease, Hypertension and Use of Biomass Fuel among Women: Comparative Cross-Sectional Study. BMJ Open 2019, 9, e030881. [Google Scholar] [CrossRef]
- Ingale, L.T.; Dube, K.J.; Sarode, D.B.; Attarde, S.B.; Ingle, S.T. Monitoring and Respiratory Health Assessment of the Population Exposed to Cooking Fuel Emissions in a Rural Area of Jalgaon District, India. Asia-Pacific J. Public Health 2013, 25, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Alves, L.; Cesar, J.A.; Horta, B.L. Prevalence of Angina Pectoris in Pelotas (South of Brazil). Arq. Bras. Cardiol. 2010, 95, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Farmer, S.A.; Nelin, T.D.; Falvo, M.J.; Wold, L.E. Ambient and Household Air Pollution: Complex Triggers of Disease. Am. J. Physiol.—Hear. Circ. Physiol. 2014, 307, H467–H476. [Google Scholar] [CrossRef]
- Nautiyal, J.; Garg, M.L.; Kumar, M.S.; Khan, A.A.; Thakur, J.S.; Kumar, R. Air Pollution and Cardiovascular Health in Mandi-Gobindgarh, Punjab, India—A Pilot Study. Int. J. Environ. Res. Public Health 2007, 4, 268–282. [Google Scholar] [CrossRef] [PubMed]
- Kuźma, A.Ł.; Pogorzelski, S.; Struniawski, K.; Dobrzycki, S.; Bachórzewska, H. Effects of Air Pollution on the Number of Hospital Admissions for Acute Coronary Syndrome in Elderly Patients (BIA-ACS Registry). Polish Arch. Intern. Med. 2020, 130, 38–46. [Google Scholar] [CrossRef]
- Koskela, R.S.; Mutanen, P.; Sorsa, J.A.; Klockars, M. Factors Predictive of Ischemic Heart Disease Mortality in Foundry Workers Exposed to Carbon Monoxide. Am. J. Epidemiol. 2000, 152, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Tárnoki, Á.D.; Tárnoki, D.L.; Travers, M.J.; Hyland, A.; Dobson, K.; Mechtler, L.; Cummings, K.M. Tobacco Smoke Is a Major Source of Indoor Air Pollution in Hungary’s Bars, Restaurants and Transportation Venues. Clin. Exp. Med. J. 2009, 3, 131–138. [Google Scholar] [CrossRef]
- Glantz, S.A.; Parmley, W.W. Passive Smoking and Heart Disease. Epidemiology, Physiology, and Biochemistry. Circulation 1991, 83, 1–12. [Google Scholar] [CrossRef]
- Hole, D.J.; Gillis, C.R.; Chopra, C.; Hawthorne, V.M. Passive Smoking and Cardiorespiratory Health in a General Population in the West of Scotland. Br. Med. J. 1989, 299, 423–427. [Google Scholar] [CrossRef]
- Dasgupta, S.; Huq, M.; Khaliquzzaman, M.; Pandey, K.; Wheeler, D. Indoor Air Quality for Poor Families: New Evidence from Bangladesh. Indoor Air 2006, 16, 426–444. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.Y.; Urpelainen, J. Fuel Stacking in India: Changes in the Cooking and Lighting Mix, 1987–2010. Energy 2014, 76, 306–317. [Google Scholar] [CrossRef]
- Masera, O.R.; Saatkamp, B.D.; Kammen, D.M. From Linear Fuel Switching to Multiple Cooking Strategies: A Critique and Alternative to the Energy Ladder Model. World Dev. 2000, 28, 2083–2103. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Africa (n = 69,147) | Americas (n = 60,869) | Asia (n = 79,567) | Europe (n = 19,684) | Total (n = 229,267) |
|---|---|---|---|---|---|
| Angina pectoris diagnosed (%) a | 8.4% | 5.2% | 6.1% | 16.8% | 7.9% |
| Angina pectoris treated (%) b | 4.9% | 4.6% | 5.4% | 18.4% | 7.3% |
| Rose angina pectoris (%) c | 10.4% | 4.8% | 9.5% | 11.3% | 9.0% |
| Angina pectoris diagnosed, treated or Rose | 16.3% | 9.5% | 14.1% | 24.6% | 15.2% |
| Household fuel used for cooking or heating d | |||||
| - Gas | 6.3% | 83.6% | 20.5% | 52.3% | 36.2% |
| - Electricity | 12.8% | 0.4% | 0.8% | 6.3% | 2.9% |
| - Kerosene | 3.6% | 0.0% | 1.7% | 3.9% | 1.9% |
| - Coal/charcoal | 7.6% | 1.8% | 6.1% | 0.9% | 4.6% |
| - Wood | 49.5% | 10.3% | 55.4% | 5.0% | 37.9% |
| - Agriculture/dung/shrubs/other | 4.2% | 0.2% | 10.9% | 0.2% | 6.4% |
| - Mixed solid/liquid/gas/electricity | 6.9% | 1.7% | 3.3% | 17.5% | 5.6% |
| - Mixed solid only | 7.5% | 0.1% | 0.9% | 0.3% | 1.4% |
| Household fuel used for cooking or heating e | |||||
| - Gas/electricity/kerosene | 22.6% | 84.1% | 22.9% | 62.5% | 41.0% |
| - Coal/charcoal/wood/agriculture/crop/shrub/grass | 61.4% | 12.3% | 72.3% | 6.1% | 48.9% |
| - Mixed fuel use | 16.0% | 3.6% | 4.8% | 31.4% | 10.1% |
| Mean age (years) | 36.84 | 40.91 | 38.86 | 49.00 | 40.65 |
| Sex (%) | |||||
| - Men | 49.5% | 44.5% | 51.1% | 38.3% | 47.6% |
| - Women | 50.5% | 55.5% | 48.9% | 61.7% | 52.4% |
| BMI (kg/m2) | |||||
| - Underweight (<18.5) | 9.2% | 4.2% | 14.8% | 2.7% | 10.1% |
| - Normal (18.5 ≤ BMI < 25.0) | 59.1% | 52.7% | 57.1% | 45.8% | 54.4% |
| - Overweight (25.0 ≤ BMI < 30.0) | 20.1% | 30.9% | 18.4% | 35.5% | 24.0% |
| - Obese (BMI ≥ 30.0) | 11.6% | 12.2% | 9.7% | 16.0% | 11.5% |
| Marital status (%) | |||||
| - Married/cohabitating | 58.8% | 63.0% | 73.7% | 57.3% | 67.3% |
| - Single/separated/divorced/widowed | 41.2% | 37.0% | 26.3% | 42.7% | 32.7% |
| Highest level of education (%) | |||||
| - No formal schooling/primary school completed | 69.7% | 42.6% | 63.5% | 14.5% | 52.3% |
| - Secondary school | 16.6% | 30.1% | 15.9% | 26.0% | 20.3% |
| - High school or above | 13.7% | 27.3% | 20.6% | 59.6% | 27.3% |
| Smoking (%) | |||||
| - Never/former | 86.3% | 77.2% | 66.0% | 71.4% | 71.3% |
| - Current | 13.7% | 22.8% | 34.0% | 28.6% | 28.7% |
| Alcohol consumption (%) | |||||
| - Never/former | 69.7% | 33.3% | 83.5% | 26.1% | 62.8% |
| - Current | 30.3% | 66.7% | 16.5% | 73.9% | 37.2% |
| Physical activity (%) | |||||
| - Low | 13.6% | 20.4% | 10.6% | 10.3% | 12.9% |
| - Moderate | 22.2% | 29.0% | 20.1% | 27.0% | 23.3% |
| - High | 64.2% | 50.6% | 69.3% | 62.7% | 63.8% |
| Diabetes (%) | 2.5% | 5.9% | 2.3% | 5.0% | 3.4% |
| Characteristic | Africa | Americas | Asia | Europe | Pooled Sample | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | ||
| Household fuel used for cooking or heating | Gas | 1 | 1 | 1 | 1 | 1 | |||||
| Electricity | 0.72 | 0.53–0.99 | 0.61 | 0.14–2.65 | 0.74 | 0.47–1.16 | 0.44 | 0.31–0.61 | 0.68 | 0.56–0.83 | |
| Kerosene | 0.87 | 0.55–1.37 | n/a | n/a | 1.43 | 1.05–1.95 | 0.21 | 0.14–0.31 | 0.84 | 0.66–1.06 | |
| Coal/charcoal | 1.08 | 0.84–1.39 | 1.42 | 0.82–2.46 | 0.61 | 0.48–0.79 | 0.67 | 0.28–1.59 | 0.80 | 0.66–0.97 | |
| Wood | 1.68 | 1.37–2.05 | 0.86 | 0.65–1.14 | 0.91 | 0.73–1.13 | 0.10 | 0.65–1.53 | 1.14 | 0.97–1.33 | |
| Agriculture/dung/shrubs/other | 1.81 | 1.06–3.09 | 1.24 | 0.57–2.73 | 1.30 | 1.01–1.67 | 1.01 | 0.33–3.12 | 1.65 | 1.30–2.09 | |
| Mixed solid/liquid/gas/electricity | 1.55 | 1.15–2.07 | 1.46 | 0.94–2.27 | 1.08 | 0.79–1.49 | 0.91 | 0.69–1.20 | 1.31 | 1.09–1.56 | |
| Mixed solid only | 1.99 | 1.50–2.65 | 4.08 | 1.55–10.75 | 1.14 | 0.58–2.25 | 1.06 | 0.20–5.73 | 1.59 | 1.12–2.25 | |
| Mixed liquid/gas/electricity only | 1.17 | 0.73–1.87 | 2.12 | 1.13–3.98 | 0.73 | 0.50–1.07 | 0.59 | 0.41–0.86 | 0.94 | 0.69–1.28 | |
| Household fuel used for cooking or heating (grouped) | Gas/electricity/kerosene | 1 | 1 | 1 | 1 | 1 | |||||
| Coal/charcoal/wood/agriculture/crop/shrub/grass | 1.83 | 1.52–2.21 | 0.96 | 0.73–1.25 | 0.88 | 0.74–1.05 | 1.14 | 0.77–1.70 | 1.15 | 1.01–1.31 | |
| Mixed fuel use | 1.95 | 1.57–2.44 | 1.84 | 1.28–2.64 | 1.02 | 0.78–1.35 | 0.92 | 0.73–1.14 | 1.22 | 1.06–1.42 | |
| Characteristic | Pooled Sample | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Angina Diagnosed b | Angina Treated c | Rose d | |||||||||||
| Men | Women | Men | Women | Men | Women | ||||||||
| OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | OR a | (95% CI) a | ||
| Household fuel used for cooking or heating | Gas | 1 | 1 | 1 | 1 | 1 | 1 | ||||||
| Electricity | 0.53 | 0.38–0.76 | 0.54 | 0.39–0.75 | 0.75 | 0.52–1.09 | 0.59 | 0.43–0.81 | 0.80 | 0.53–1.20 | 0.64 | 0.45–0.92 | |
| Kerosene | 0.85 | 0.56–1.30 | 0.62 | 0.40–0.97 | 0.80 | 0.52–1.22 | 0.57 | 0.40–0.83 | 0.93 | 0.65–1.32 | 1.13 | 0.82–1.56 | |
| Coal/charcoal | 0.55 | 0.39–0.80 | 0.91 | 0.70–1.19 | 0.71 | 0.47–1.05 | 1.02 | 0.76–1.37 | 0.64 | 0.47–0.87 | 0.94 | 0.72–1.21 | |
| Wood | 1.06 | 0.85–1.33 | 1.16 | 0.94–1.43 | 1.02 | 0.80–1.29 | 1.03 | 0.83–1.29 | 1.35 | 1.06–1.73 | 1.16 | 0.97–1.39 | |
| Agriculture/dung/shrubs/other | 1.17 | 0.72–1.92 | 0.84 | 0.49–1.44 | 1.89 | 1.10–3.24 | 0.90 | 0.55–1.47 | 2.51 | 1.69–3.72 | 1.45 | 1.02–2.06 | |
| Mixed solid/liquid/gas/electricity | 1.10 | 0.78–1.56 | 0.95 | 0.72–1.26 | 1.31 | 0.91–1.89 | 1.17 | 0.88–1.55 | 1.70 | 1.20–2.41 | 1.32 | 1.02–1.72 | |
| Mixed solid only | 1.21 | 0.61–2.41 | 1.20 | 0.65–2.24 | 1.26 | 0.59–2.70 | 1.12 | 0.57–2.21 | 1.42 | 0.83–2.44 | 2.35 | 1.53–3.62 | |
| Mixed liquid/gas/electricity only | 1.32 | 0.62–2.78 | 0.65 | 0.47–0.91 | 1.26 | 0.61–2.63 | 0.73 | 0.53–1.01 | 1.13 | 0.61–2.08 | 0.82 | 0.62–1.08 | |
| Household fuel used for cooking or heating (grouped) | Gas/electricity/kerosene | 1 | 1 | 1 | 1 | 1 | 1 | ||||||
| Coal/charcoal/wood/agriculture/crop/shrub/grass | 1.04 | 0.85–1.28 | 1.15 | 0.95–1.40 | 1.07 | 0.86–1.32 | 1.08 | 0.88–1.31 | 1.35 | 1.11–1.63 | 1.15 | 0.97–1.35 | |
| Mixed fuel use | 1.24 | 0.87–1.78 | 0.89 | 0.71–1.12 | 1.33 | 0.94–1.88 | 1.04 | 0.83–1.30 | 1.49 | 1.11–2.01 | 1.22 | 1.01–1.47 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiwari, I.; Herr, R.M.; Loerbroks, A.; Yamamoto, S.S. Household Air Pollution and Angina Pectoris in Low- and Middle-Income Countries: Cross-Sectional Evidence from the World Health Survey 2002–2003. Int. J. Environ. Res. Public Health 2020, 17, 5802. https://doi.org/10.3390/ijerph17165802
Tiwari I, Herr RM, Loerbroks A, Yamamoto SS. Household Air Pollution and Angina Pectoris in Low- and Middle-Income Countries: Cross-Sectional Evidence from the World Health Survey 2002–2003. International Journal of Environmental Research and Public Health. 2020; 17(16):5802. https://doi.org/10.3390/ijerph17165802
Chicago/Turabian StyleTiwari, Ishwar, Raphael M. Herr, Adrian Loerbroks, and Shelby S. Yamamoto. 2020. "Household Air Pollution and Angina Pectoris in Low- and Middle-Income Countries: Cross-Sectional Evidence from the World Health Survey 2002–2003" International Journal of Environmental Research and Public Health 17, no. 16: 5802. https://doi.org/10.3390/ijerph17165802
APA StyleTiwari, I., Herr, R. M., Loerbroks, A., & Yamamoto, S. S. (2020). Household Air Pollution and Angina Pectoris in Low- and Middle-Income Countries: Cross-Sectional Evidence from the World Health Survey 2002–2003. International Journal of Environmental Research and Public Health, 17(16), 5802. https://doi.org/10.3390/ijerph17165802