Review of Drug Utilization Studies in Neonatal Units: A Global Perspective




Abstract
1. Introduction
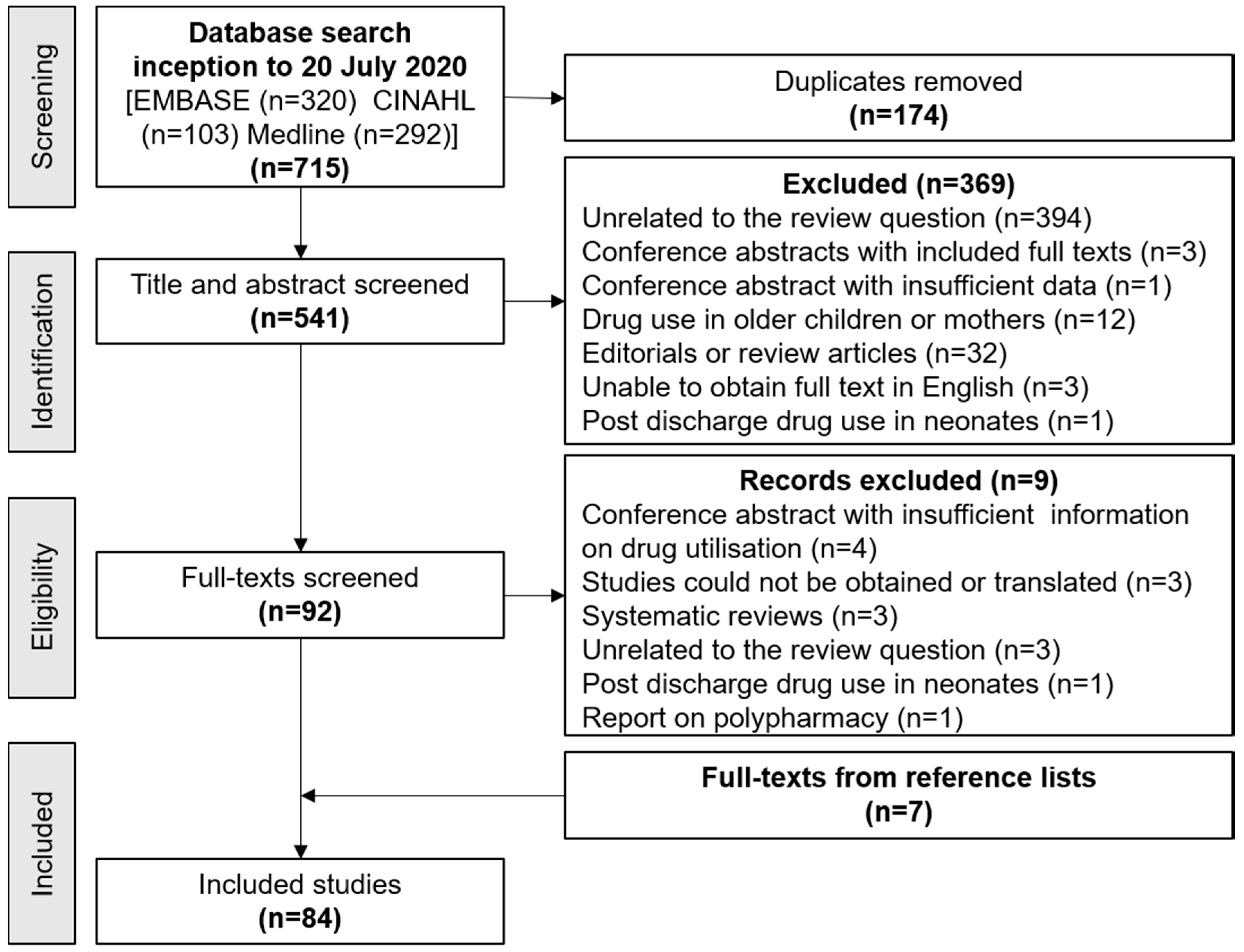
2. Materials and Methods
3. Results
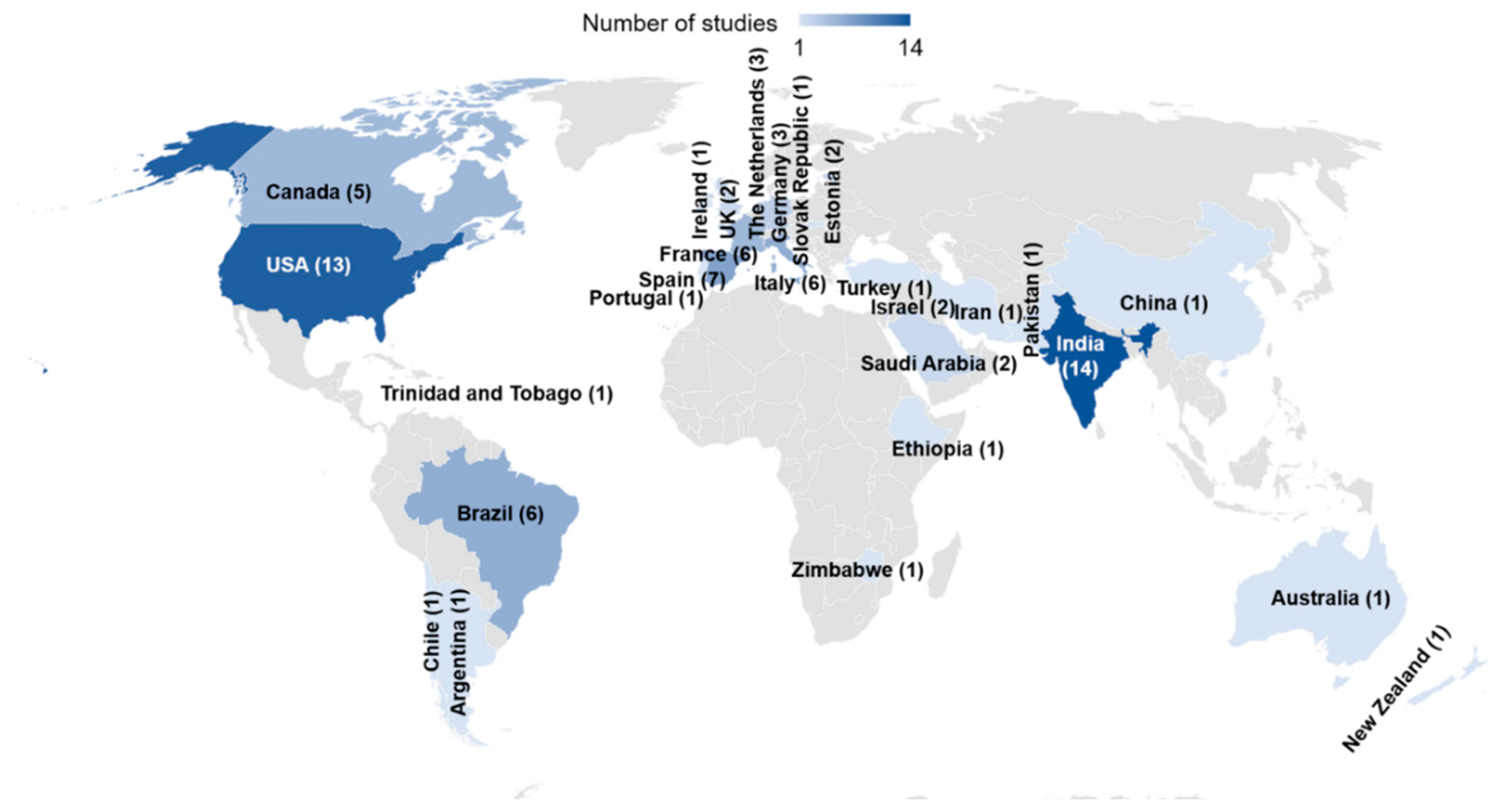
3.1. Characteristics of Included Studies
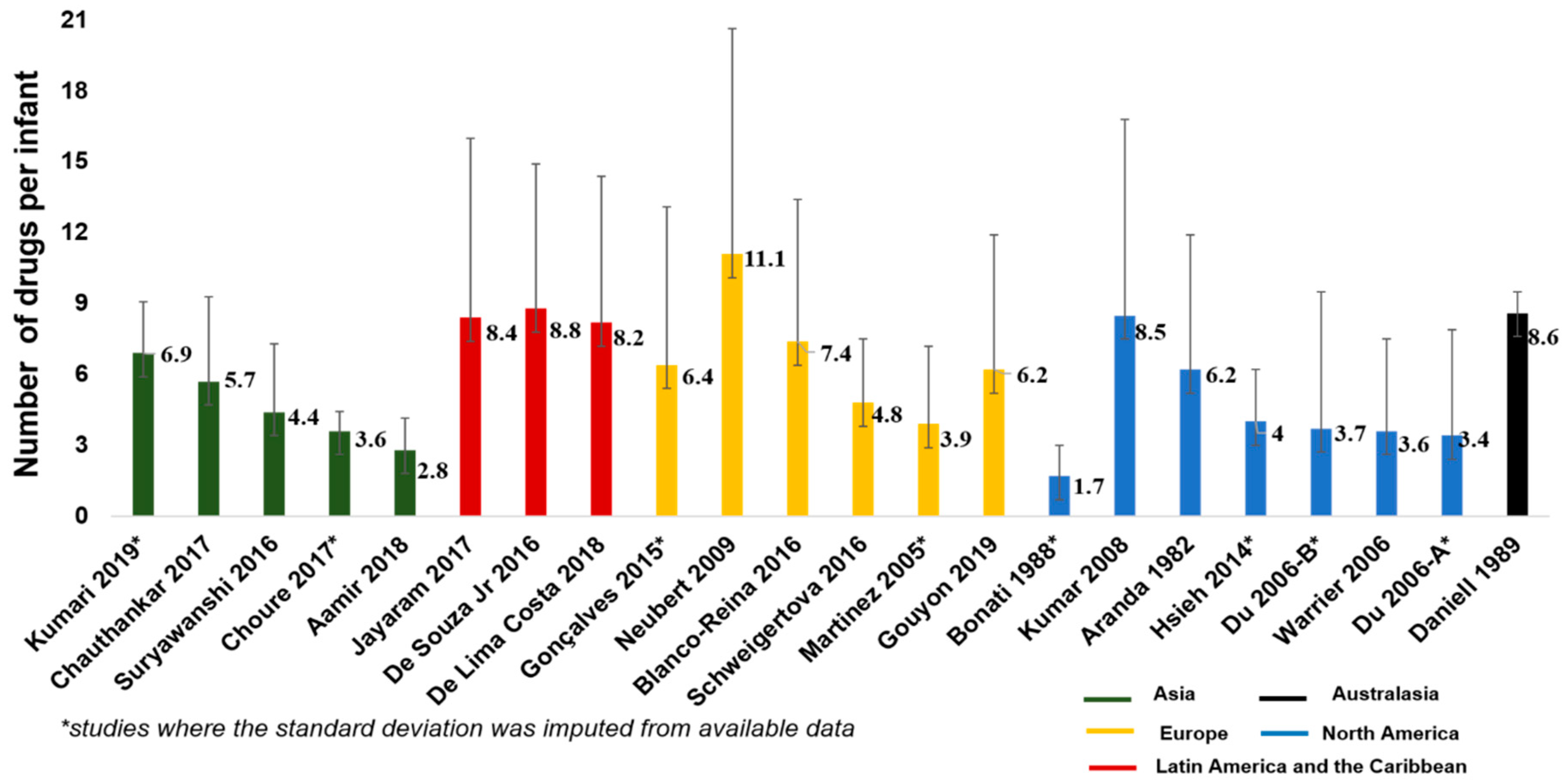
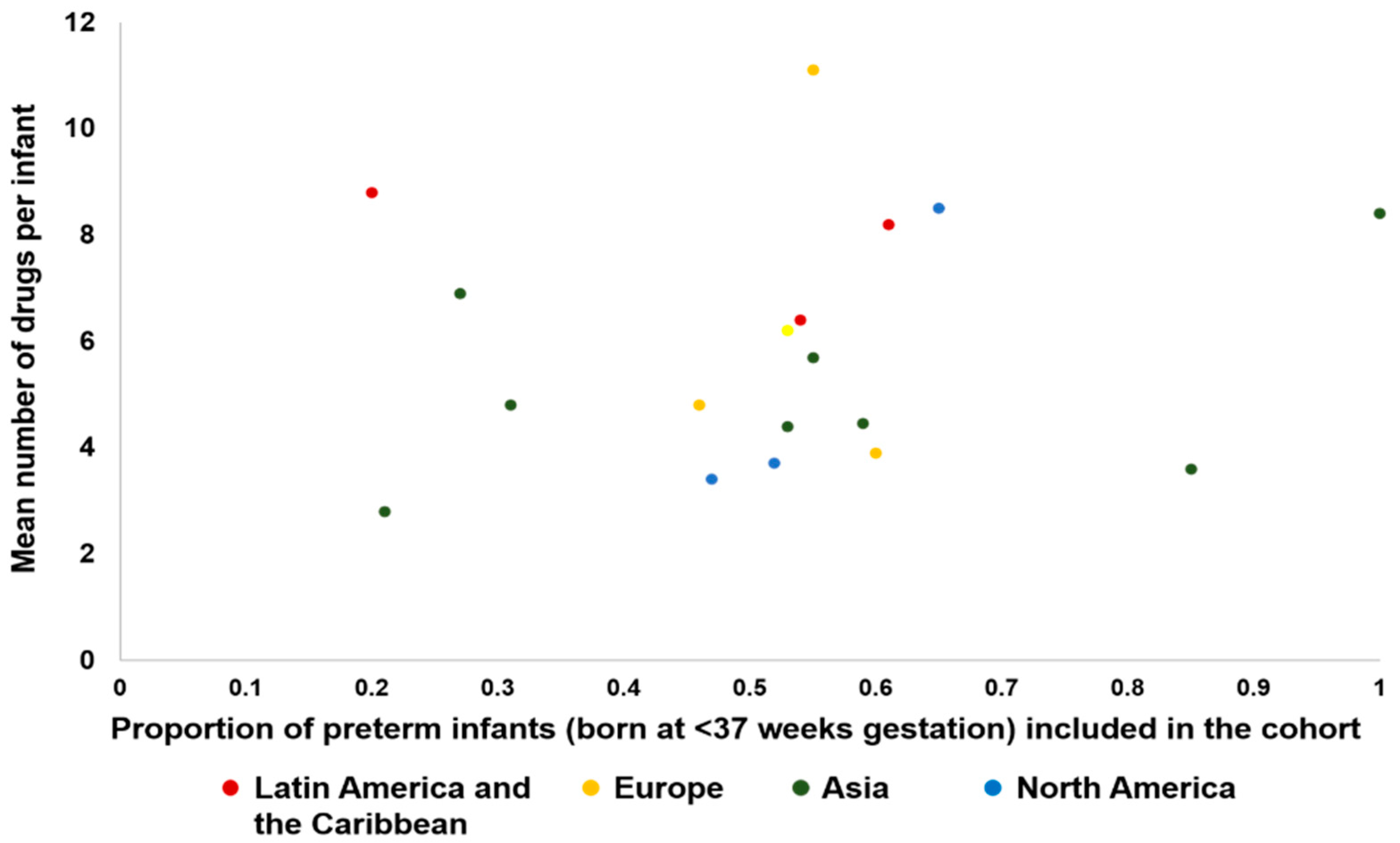
3.2. Number of Drugs Per Infant
3.3. Most Frequently Prescribed Pharmacological Groups
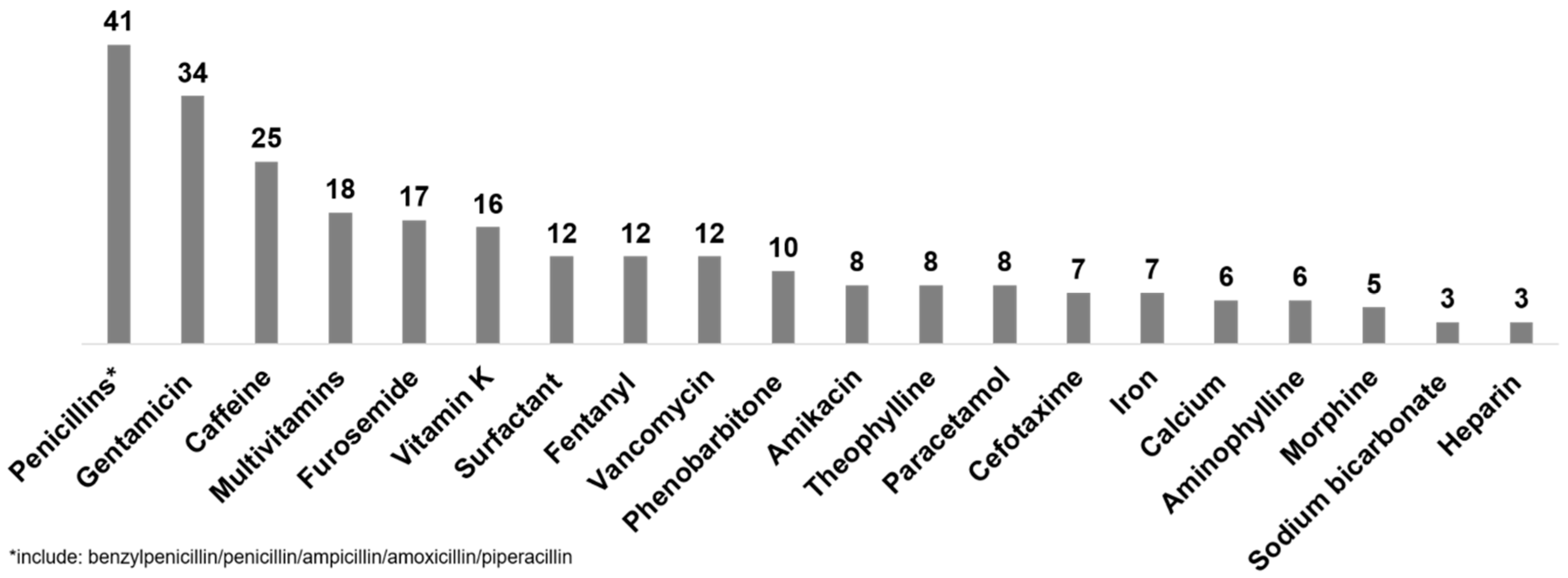
3.4. Most Frequently Prescribed Drugs
3.5. Most Frequently Prescribed Antibiotics
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terms | Combination of Search Terms (A Combination between Title Abstract Free Text Keywords and Mesh Terms) | Number of Hits |
|---|---|---|---|
| EMBASE (provided by Ovid) From 1974 to 9 April 2019 | Population search terms: Free text words: Infant*-newborn*-neonate* MeSH terms: INFANT-NEWBORN Drug utilization search terms: Free text words: “drug use”-drug utilization MeSH terms: DRUG UTILIZATION-”DRUG USE” Setting search terms: Free text words: neonatal intensive care unit*-neonatal unit* MeSH terms: NEWBORN INTENSIVE CARE- NEONATAL INTENSIVE CARE UNIT | ~”(((infant*).ti,ab OR (newborn*).ti,ab OR (neonate*).ti,ab OR *INFANT/OR exp INFANT/OR *NEWBORN/) AND ((“drug use”).ti,ab OR (“drug utilization”).ti,ab OR *”DRUG UTILIZATION”/OR exp “DRUG UTILIZATION”/OR *”DRUG USE”/OR exp “DRUG USE”/)) AND (*”NEWBORN INTENSIVE CARE”/OR *”NEONATAL INTENSIVE CARE UNIT”/)” | 232 |
| Medline (provided by ProQuest) From 1946 to 9 April 2019 | Population search terms: Free text words: Infant*-newborn*-neonate* MeSH terms: INFANT-INFANT, NEWBORN Drug utilization search terms: Free text words: “drug use”-drug utilization MeSH terms: DRUG UTILIZATION Setting search terms: Free text words: neonatal intensive care unit*-neonatal unit* MeSH terms: Care,neonatal intensive- intensive care units,neonatal infant,newborn,intensive care-neonatal intensive care-neonatal intensive care units | ~”(((infant*).ti,ab OR (neonate*).ti,ab OR (newborn*).ti,ab OR *INFANT/OR exp INFANT/OR *”INFANT, NEWBORN”/OR exp “INFANT, NEWBORN”/) AND ((“drug use”).ti,ab OR (drug utilization).ti,ab OR *”DRUG UTILIZATION”/OR exp “DRUG UTILIZATION”/OR *”DRUG UTILIZATION REVIEW”/OR exp “DRUG UTILIZATION REVIEW”/)) AND ((neonatal intensive care unit*).ti,ab OR (neonatal unit*).ti,ab OR *”INTENSIVE CARE UNITS, NEONATAL”/OR exp “INTENSIVE CARE UNITS, NEONATAL”/)” | 254 |
| CINAHL (provided by EBSCO) From 1937 to 9 April 2019 | Population search terms: Free text words: Infant*-newborn*-neonate*MeSH terms: INFANT-INFANT,NEWBORN Drug utilization search terms: Free text words: “drug useinfa”- drug utili?ationMeSH terms:DRUG UTILIZATION Setting search terms: Free text words: neonatal intensive care unit*-neonatal unit*MeSH terms: INTENSIVE CARE UNITS,NEONATAL | Combination of search terms(A combination between title abstract key words, and Mesh terms was done for a compressive search from inception of the database to February 2019 using OR, AND) ~”(((infant*).ti,ab OR (newborn*).ti,ab OR (neonate*).ti,ab OR *INFANT/OR exp INFANT/OR *”INFANT, NEWBORN”/OR exp “INFANT, NEWBORN”/) AND ((“drug use”).ti,ab OR (drug utilization).ti,ab OR *”DRUG UTILIZATION”/)) AND ((neonatal unit*).ti,ab OR (neonatal intensive care unit*).ti,ab OR *”INTENSIVE CARE UNITS, NEONATAL”/OR exp “INTENSIVE CARE UNITS, NEONATAL”/)” | 87 |
| Total hits | 573 | ||
Appendix B. Characteristics of Included Studies
Appendix B.1. Description of Drug Utilization Studies on Drug Use in All Categories (60 Studies)
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| Italy (6 studies) | |||||
| Bonati 1988 (75) | One year (year not reported) | Inclusion: all admitted neonates Exclusion: fluids and electrolytes, glucose, oxygen, vitamin K and prophylactic ophthalmic preparation | n = 706 (47%) | GA (mean, range): 33.3, 26–36 BW (mean, range): 2013, 510–3600 | Mean (SD): 1.7 (0–8) |
| Dell’ Aera 2007 (25) | July–August 2004 | Inclusion: all admitted neonates Exclusion: not reported | n = 34 (not reported) | Not reported | Not reported |
| Dessi 2010 (26) | March 2007 (1 month) | Inclusion: all admitted neonates receiving drugs Exclusion: saline, blood transfusions, oxygen | n = 38 (not reported) | GA not reported BW not reported | Range: 1–4 |
| Laforgia 2014 (67) | May 2011 (1 month) | Inclusion: all admitted neonates with at least one drug Exclusion: not reported | n = 126 (not reported) | GA (median, range): 31, 23–36 BW not reported | Median (range): 3 (1–7) |
| Cuzzolin 2016 (71) | May–July 2014 | Inclusion: all admitted neonates with at least one drug Exclusion: not reported | n = 220 (41%) | Not reported | Median (range): 4 (1–9) |
| Girardi 2017 (31) | January 2009–December 2011 (3 years) | Inclusion: all admitted neonates with GA < 37 weeks and BW ≤ 1500 g Exclusion: died within the first 48 h after birth | n = 159 (not reported) | Mean (range) 1000–1500 g group: 30 (27–36) <1000 g group: 26 (22–33) | Not reported |
| Spain (4 studies) | |||||
| Martinez 2005 (42) | October–December 2003 | Inclusion: all admitted neonates Exclusion: not reported | n = 48 (not reported) | Not reported | Mean (range): 3.9 (1–14) |
| Payares 2010 (47) | 8 months (year not reported) | Not reported | n = 52 (48%) | GA: 0–48 days BW (range): 550–3920 | Not reported |
| Blanco-Reina 2016 (13) | July–November (year not reported) | Inclusion: admitted neonates with at least one drug Exclusion: not reported | n = 48 (41%) | GA (mean (SD)): 34.5 (4.2) BW (mean (SD)): 2335 (949) | Mean (SD): 7.4 (6) |
| Alonso 2019 (7) | April–September 2018 | Inclusion: all admitted neonates Exclusion: blood products, TPN, fluids and oxygen | n = 84 (38%) | Not reported | Not reported |
| France (4 studies) | |||||
| Gouyon 2019 (74) | January 2017–December 2018 | Inclusion: all patients with a first prescription before 28th day of life and at least one electronic medication prescription Exclusion: no prescriptions, or none in first 28 days; handwritten prescriptions only | n = 27382 (55%) | GA (mean (SD)): 35.4 (4.3) BW (mean (SD)): 2457.8 (944.5) | Mean (SD): 6.2 (5.7) |
| Gortner 1991 (77) | August 1989–May 1990 (10 mo) | Inclusion: premature neonates with a need of intubation and mechanical ventilation Exclusion: vitamin K and heparin | n = 164 (46%) | GA (mean (SD)): 27.2 (1.2) BW (mean (SD)): 970 (145) | Not reported |
| Nguyen 2011 (44) | January–April 2009 | Inclusion: all admitted neonates Exclusion: TPN, IV fluids, oxygen and drugs used in research studies | n = 65 (not reported) | GA (median(range)): 34 (27–41) BW median(range)) 1930 (810–4520) | Median (range): 4 (1–7) |
| Riou 2015 (62) | 1 year (2012) | Inclusion: all admitted neonates with at least one drug Exclusion: blood products, oxygen therapy, enteral and parenteral nutrition, and standard intravenous replacement solutions | n = 910 (43%) | GA (median (IQR)): 34 (31–37) BW (median (IQR)): 2040 (1530–2270) | Median (IQR): 8 (5–13) |
| The Netherlands (3 studies) | |||||
| Jong 2001 (35) | February–March 1999 | Inclusion: all admitted neonates Exclusion: blood products, TPN, oxygen therapy, IV fluids | n = 64 (50%) | Not reported | Not reported |
| Flint 2014 (29) (abstract) | January 2007–June 2013 | Not reported | n = 4054 (45%) | GA (median, range): 32, 23+6–42+2 BW median, range): 1800, 360–5400) | Not reported |
| Flint 2018 (76) | September 2014–August 2015 (1 year) | Inclusion: all admitted neonates Exclusion: electrolytes, TPN, vaccines, dermatological products, contrast media | n = 1491 (48%) | GA (median, IQR): 32+5, 29+6 to 37+6 BW (median (IQR)): 1865,1253–3000 | Median (IQR):5 (3–10) |
| Germany (2 studies) | |||||
| Lindner 2008 (61) | Study period not reported) | Inclusion: all neonates with GA < 32 Exclusion: not reported | n = 113 (44%) | GA (mean (SD)): 26.9 (1.65) BW (mean (SD)) 930 (253) | Not reported |
| Neubert 2009 (43) | December 2004–October 2005 (11 months) | Inclusion: all admitted neonates for >24 h Exclusion: IV infusions (e.g., glucose or chloride), TPN and oxygen | n = 183 (44%) | GA (mean (SD)): 33.6 (4.66) BW (mean (SD)): 2134 (935) | Mean (SD): 11.1 (9.56) Range: 0–45 |
| UK (2 studies) | |||||
| Conroy 1999 (20) | February–May 1998 (13 weeks) | Inclusion: all admitted neonates Exclusion: IV fluids, flushes of sodium chloride 0.9% or heparin, blood products (other than albumin) and oxygen therapy | n = 70 (not reported) | GA (preterm only) (median, range): 33 (26 to 36) | Median (range): 3.5 (0–42) |
| Turner 2009 (79) | December 2007–April 2008 | Inclusion: all admitted neonates Exclusion: blood products, IV fluids, TPN | Not reported | Not reported | Not reported |
| Ireland (one study) | |||||
| Kieran 2013 (37) | February–March 2012 | Inclusion: all admitted neonatesExclusion: not reported | n = 110 (not reported) | GA (mean (SD)): 35 (5) BW (median, (IQR)): 2615 (1601 -3500) | Median (IQR): 4 (3–11) |
| Portugal (one study) | |||||
| Silva 2015 (50) | January–June 2013 | Inclusion: all admitted neonates Exclusion: oxygen, IV fluids and flushes, drugs used in surgeries, enteral and parenteral nutrition, contrast agents, vaccines, blood products (except albumin and immunoglobulins), basic creams, drugs on clinical trials | n = 218 (45%) | GA (mean (SD)): 36.07 (4.0) BW (mean (SD)): 2554 (910.5) | Median (range): 3 (0–34) |
| Estonia (one study) | |||||
| Lass 2011 (59) | February–August 2008 | Inclusion: all admitted neonates Exclusion: IV fluids, blood products, oxygen, nutritional and technical products, basic creams and ointments, TPN, vaccines and vitamins | n = 490 (not reported) | GA not reported BW (mean (SD)): 2446 (1124) | Median (IQR, max): 4 (2–7, 27) |
| Slovak Republic (one study) | |||||
| Schweigertova 2016 (63) | April–September 2012 | Inclusion: all admitted neonates Exclusion: IV replacement solutions, TPN, vaccines, blood products and oxygen | n = 202 (49%) | GA (mean (SD)): 36 (3.4) BW: Not reported | Mean (SD): 4.8 (2.7) |
| Turkey (one study) | |||||
| Oguz 2012 (68) | December 2011 | Inclusion: all admitted neonates Exclusion: standard IV solutions, sodium chloride 0.9% infusions, TPN, blood products (except albumin) and oxygen | n = 93 (not reported) | GA (mean (SD)): 32.5 (4.7) BW (mean (SD)): 2081 (951) | Median (range): 3 (1–11) |
| Multi-European countries (21 countries) | |||||
| Mesek 2019 (65) | January–June 2012 | Inclusion: all infants in the neonatal unit and receiving prescription on the day (at 8 AM) Exclusion: blood products, glucose and electrolyte solutions, vaccines, nursery care topical agents, herbal medicines and enteral nutrition including breast milk fortifiers | n = 726 (43%) | GA (median, (IQR)): 34 (30–38) BW (median, (IQR)): 1993 (1356–3006) | Not reported |
| BW, birthweight; GA, gestation age; IV, Intravenous; SD, standard deviation; TPN, total parenteral nutrition | |||||
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| Israel (2 studies) | |||||
| Barr 2002 (11) | April–July 2000 | Inclusion: all admitted neonates Exclusion: saline, heparin flush, blood transfusions, and oxygen | n = 105 (not reported) | Not reported | Range: 1–13 |
| Nir-Neuman 2018 (45) | December 2015–January 2016 | Inclusion: all admitted neonates Exclusion: TPN, blood products, fluids, oxygen therapy, nasal sprays, eye drops, ointments, and local creams | n = 134 (49%) | GA (median, IQR): (35, 33–38) BW (mean(SD)): 2424 (854) | Median (IQR): 6 (2–17) |
| BW, birthweight; GA, gestation age; SD, standard deviation; TPN, total parenteral nutrition | |||||
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| USA (9 studies) | |||||
| Russel 1983 (79) | Not reported | Not reported | Not reported | Not reported | Not reported |
| Lesko 1990 (60) | 1978–1986 | Inclusion: all admitted for >24 h Exclusion: vitamin K and topical products such as silver nitrate | n = 2690 (43%) | GA: not reported BW (median): 2220 | 8 |
| Clark 2006 (70) | February–May 1998 (13 weeks) | Inclusion: all neonates in database Exclusion: Not reported | n = 253651 (44%) | GA (median, IQR): 35 (33–38) BW (median, IQR): 2460 (1790–3200) | Not reported |
| Du 2006 (28) | January 1997–June 2004 (7 years) 2 periods 1st: 1997–1998 2nd: 2001–2004 | Inclusion: all admitted neonates with at least one drug Exclusion: TPN, oxygen administration, vitamin K prophylaxis, erythromycin ophthalmic prophylaxis, routine cord care, vaccinations, blood and blood products (except fresh frozen plasma) | 1st period: n = 2332 (47%) 2nd period: n = 2691 (44%) | 1st period:GA (mean): 35.7 BW (mean): 2580 2nd period: GA (mean): 35.3 BW (mean): 2499 | Median (range) 1st period: 3.37 (2, 1–28) 2nd period 3.72 (2, 1–36) |
| Warrier 2006 (53) | January 1997–June 2004 | Inclusion: all admitted neonates with at least one drug Exclusion: blood and blood products (except fresh frozen plasma), TPN, oxygen, vitamin K prophylaxis, erythromycin ophthalmic prophylaxis, routine cord care, vaccinations, TPN, normal saline except when treatment for hypotension | n = 6839 (46%) | GA (mean (SD)): 35 (5) BW (mean (SD)): 2498 (1000) | Mean (SD): 3.6 (3.9) |
| Kumar 2008 (38) | September 2000–August 2003 (3 years) | Inclusion: all admitted neonates Exclusion: TPN, nutritional supplements such as vitamins, standard intravenous fluids, immunizations and drugs used in research studies | n = 2304 (43%) | GA (mean (SD)): 34.1 (4.6) BW (mean (SD)): 2325 (1014) | Mean (SD): 8.5 (8.3) |
| Hsieh 2014 (69) | 2005–2010 (5 years) | Inclusion: all admitted neonates Exclusion: after a day of life 120, and all vitamins (except vitamin A), nutritional supplements, vaccines, eye drops and topical medications. | n = 450,386 (44%) | GA (median, IQR): 35 (33–38) BW (median, IQR) 2490 (1830 to 3191) | Mean (range): 4 (1–14) For <1000 gm Mean (range): 17 (2–45) |
| Gulati 2016 (33) | 1990–2011 (22 years) | Inclusion: all very low BW neonates Exclusion: volume boluses, blood and blood products, TPN, and topical medications | n = 5529 (50%) | GA (median, IQR): 28 (26–30) BW (median, IQR): 1017 (745–1271) | Median (IQR): 9 (5–15) |
| Puia-Dumitrescu 2020 (72) | 2006–2016 (10 years) | Inclusion: 22–24 week admitted to the NICU without major congenital anomalies Exclusion: missing or incomplete discharge data or discharge home at <32 weeks postnatal age. All nutritional supplements, vitamins (except Vitamin A), vaccines, eye drops and topical medications | n = 7578 (47%) | GA: Not reported BW (median, (IQR)): 610 (540–680) | Median (IQR): 13 (8, 18) |
| Canada (3 studies) | |||||
| Aranda 1982 (8) | Not reported | Inclusion: all admitted neonates Exclusion: Drugs for routine prophylaxis (e.g., antimicrobial eye drops) | n = 293 (not reported) | GA (mean (SD)): 36.4 (0.25) BW (mean (SD)): 2687 (157) | Mean (SD): 6.2 (5.7) Range: 1–26 |
| Aranda 1983 (9) | 2 periods; 1st: July 1974–February 1975 2nd: February 1977–November 1977 | Inclusion: all admitted neonates Exclusion: vitamin K, ophthalmic preparations, fluids and electrolytes, IV amino acids/intralipids and/or glucose (except if for neonatal hypoglycaemia, phototherapy and oxygen | Not reported | GA (mean (SD)): 1st period: 36.9 (0.2); 2nd period: 36.42 (0.25); BW (mean (SD)): 1st period: 2612 (51) 2nd period: 2686.9 (156.7) | Mean (SD): 1st period: 3.40 (0.20) 2nd period: 6.19 (0.33) |
| Collinge 1988 (21) | Not reported | Inclusion: all admitted neonates Exclusion: not reported | n = 1200 (not reported) | Not reported | 5.7 |
| BW, birthweight; GA, gestation age; SD, standard deviation; TPN, total parenteral nutrition | |||||
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
| China (one study) | |||||
| Yue 2020 (55) | March–Apr 2018 | Inclusion: all inpatients Exclusion: IV solutions (including 0.9% sodium chloride, 5% or 10% glucose injection, and sterile solution for injection), blood products (except albumin), 1% silver nitrate eye drops, parenteral nutrition,, heparin for venous access, oxygen, and electrolytes (such as calcium gluconate, sodium bicarbonate, magnesium sulphate and potassium chloride) | n = 319 (44%) | GA (mean (SD)): 35.8 (3.9) BW (mean (SD)): 2570 (911) | Median (IQR): 3 (1, 5.5) |
| India (9 studies) | |||||
| Chatterjee 2007 (17) | Inclusion: all admitted neonates Exclusion: not reported | n = 176 (37%) | GA: not reported BW (mean (SD)): 2214 (774) | 4.8 | |
| Sharanappa 2014 (48) | January–June 2013 | Not reported | n = 100 (not reported) | Not reported | Not reported |
| Brijal 2015 (14) | March 2013–February 2014 (1 year) | Inclusion: all admitted neonates Exclusion: neonates who are discharged or die within 24 hours of NICU admission | n = 650 (38%) | GA: not reported BW (mean (SD)): 2160 (600) | 4.46 |
| Suryawanshi 2016 (51) | April–September 2014 | Not reported | n = 528 (39%) | GA (mean (SD)): 35 (3) BW (mean (SD)): 2000 (700) | Mean (SD): 4.37 (2.91) |
| Chauthankar 2017 (18) | July 2014–March 2015 (9 mo) | Inclusion: all admitted neonates with at least one drug Exclusion: blood, blood products, vitamin K prophylaxis, prophylactic ophthalmic treatment, vaccines or IV fluids | n = 460 (41%) | GA not reported BW (mean (SD)): 2000 (700) | Mean (SD) 5.7 (3.6) |
| Choure 2017 (19) | April–September 2014 (6 mo) | Inclusion: all admitted neonates Exclusion:IV fluids, parenteral nutrition, nutritional supplements, blood and blood products, oxygen, phototherapy and vaccinations | n = 220 (46%) | Not reported | Mean (range): 3.6 (1–6) |
| Jayaram 2017(34) | August–January 2016 (6 mo) | Inclusion: all admitted neonates Exclusion: IV fluids, TPN, routine oral nutritional supplements, vaccines, Vitamin K, topical anaesthetic cream, oxygen and blood products | n = 154 (46%) | GA (mean(SD)): 34 (2.75) BW (mean(SD)): 1712 (914) | Mean (SD): 8.4 (7.6) Range: 0–17 |
| Ashwin 2018 (10) | 6 months (year not reported) | Not reported | n = 70 (39%) | GA (mean (SD)): 35 (3.14) BW mean (SD)) 2200 (730) | Mean: 3 |
| Kumari 2019 (39) | October 2017–Dec 2017 | Inclusion: all admitted neonates Exclusion: IV fluids, vaccines, Vitamin K, oxygen, and blood products | n = 81 (33%) | GA: not reported BW (mean): 2261 | Mean (range): 6.9 (1–14) |
| Pakistan (one study) | |||||
| Aamir 2018 (73) | March–August 2005 (6 mo) | Inclusion: all admitted neonates Exclusion: topical medication, oxygen, IV solution | n = 1300 (32%) | GA (median, range): 33, 26–35 BW: not reported | Mean (SD): 2.85 (1.358) Range: 1–9 |
| BW, birthweight; GA, gestation age; SD, standard deviation; TPN, total parenteral nutrition | |||||
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| Brazil (5 studies) | |||||
| Marino 2011 (41) (abstract) | January 2006–December 2007 | Not reported | n = 827 (not reported) | 4 groups: a: <1000 g b: 1000–1499 c (1500 to 2499) d: ≥2500 g | Group a: 11.1 Group b: 6 Group c: 1.7 Group d: 1.2 |
| Carvalho 2012 (15) | July–August 2011 | Inclusion: all admitted neonates Exclusion: blood and blood products, parenteral nutrition, oxygen and other gases, vit K, silver nitrate, vaccines | n = 61 (41%) | Not reported | 5 |
| Gonçalves 2015 (32) | January–June 2012 | Inclusion: all admitted neonates for more than 24 h Exclusion: sodium chloride, 5% glucose, blood products (except albumin), heparin vaccines, phytonadione, 1% silver nitrate eye drops, TPN, oxygen, and electrolytes | n = 187 (42%) | GA (median, IQR): 36.6,33.9–38.3 BW (mean(SD)): 2473 (831) | Mean (range): 6.4 (0–40) |
| De Souza Jr 2016 (24) | 6 months (year not reported) | Inclusion: neonates with electronic records of more than 24 h who drug Exclusion: incomplete clinical data, vaccines, blood products, TPN, silver nitrate eye drops or IM vitamin K in delivery room or IV fluids | n = 192 (50%) | GA (mean (SD)): 33.3 (4.3) BW (mean (SD)): 1909.5 (886) | Mean (SD): 8.8 (6.1) |
| De Lima Costa 2018 (50) | August 2015–July 2016 | Inclusion: all admitted neonates Exclusion: TPN, IV fluids, oxygen, blood products or electrolytes | n = 220 (46%) | GA (mean (SD)): 32.4 (4.4) BW (mean (SD)): 1932.7 (1127.6) | Mean (SD): 8.2 (6.2) Range: 1–33 |
| Argentina (one study) | |||||
| Fungo 2013 (30) | January–December 2011 | Inclusion: not reported Exclusion: preparations made locally or donated or acquired by family | Not reported | Not reported | Not reported |
| BW, birthweight; GA, gestation age; IV, intravenous; SD, standard deviation; TPN, total parenteral nutrition | |||||
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| New Zealand (one study) | |||||
| Daniell 1989 (22) | November 1987–February 1988 | Inclusion: all admitted neonates Exclusion: IV glucose, TPN, oxygen, blood products, sodium chloride flush, expressed milk and milk formula | n = 79 (not reported) | GA (mean (SD)): 34 (0.6) BW (mean (SD)): 2185 (112) | Mean (SD): 8.6 (0.9) Range: 0–30 |
| Australia (one study) | |||||
| O’Donnell 2002 (46) | December 2001–February 2002 | Inclusion: all admitted neonates Exclusion: TPN, IV fluids, oxygen, and drugs used in research studies | n = 97 (not reported) | GA (median, range): 31, 22.7–41.1 BW (median, range): 1560, 414- 4790 | Not reported |
| BW, birthweight; GA, gestation age; IV, intravenous; SD, standard deviation; TPN, total parenteral nutrition | |||||
Appendix B.2. Description of Drug Utilization Studies for Antibiotics Use Only (11 Studies)
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| Asia -India (4 studies) | |||||
| Gandra 2018 | February 2016–February 2017 (one year) | Inclusion: all admitted neonates with active antimicrobial prescriptions Exclusion: not reported | n = 403 (32%) | GA (median, IQR): 34.5 (31–38) BW (median (IQR): 1737, 1210–2710 | Not reported |
| Hauge 2017 | April 2008–March 2010 (3 years) | Inclusion: neonates with sepsis Exclusion: not reported | Hospital: Teaching: 217 (63%) Non-teaching: 1572 (49%) | Not reported | Teaching 7 Non-teaching: 4 |
| Shinde 2017 (49) | October 2011–September 2012 | Inclusion: neonates with sepsis Exclusion: discharged or transferred or died within 2 days in NICU | N= 84 (29%) | GA: not reported BW (mean (SD)): 2000(620) | Not reported |
| Subash 2015 (52) | February–April 2013 | Inclusion: suspected or diagnosed sepsis Exclusion: surgical problems, major congenital malformations, on antibiotics or if mother received antibiotics before delivery | n = not reported (42%) | Not reported | Not reported |
| Latin America and Caribbean-Trinidad and Tobago (one study ) | |||||
| Hariharan 2013 | September–November 2008 | Inclusion: all infants receiving antimicrobials Exclusion: not receiving antimicrobials | n = 353 (not reported) | GA: <40 weeks BW (mean (SD)): 2960 (940) | Not reported |
| Middle East- Saudi Arabia (one study) | |||||
| Balkhy 2019 (54) | October 2012–June 2013 (33 mo) | Inclusions: <16 years (data on neonates reported separately) who received at least one antimicrobials Exclusion: antimicrobial by route other than parenteral or oral routes | n = 1813 (not reported) | Not reported | Not reported |
| Africa-Zimbabwe (one study) | |||||
| Chiminhi 2020 (6) | May–November 2018 | Inclusion: all admitted infants Exclusion: none mentioned | n = 459 (49%) | GA: not reported BW (median, (IQR)): 2800 (2–3.4) | Not reported |
| Latin America and Caribbean-Chile (one study) | |||||
| Jimenez 2017 | Four years | Inclusion: all admitted infants Exclusion: not reported | n = 5,619 (46.5%) | GA (mean (SD)): 36.2 (3.6) BW: not reported | Not reported |
| North America-USA (2 studies) | |||||
| Cantey 2015 (5) | October 2011–November 2012 (4 mo) | Inclusion: all neonates admitted to NICU Exclusion: not reported | Retrospective: 593 (57%) Prospective: 1014 (43%) | GA (median, IQR): Retrospective: 38, 34.5–39.4 Prospective: 37.4, 34.1–39.1 BW (median, IQR) Retrospective: 2860, 2145–3457 BW (median, IQR): 2793, 2070–3435 | Not reported |
| Grohskopf 2005 | August 1999–February 2000 | Inclusion: infants admitted at NICU at each participating hospital on study dates Exclusion: not reported | n = 1580 (45%) | Not reported | Median (range) 2 (1–5) |
| Europe-Brazil and Germany (one study) | |||||
| Silva 2020 (50) | January–December 2018 (Brazil) May–August 2016 (Germany) | Inclusion: neonatal or paediatric intensive care unit admissions, had antimicrobial for >24h. Exclusion: topical and inhaled antibiotics | n = 2567 (not reported) | Not reported | Not reported |
| BW, birthweight; GA, gestation age; NICU; neonatal intensive care unit; PPS, point prevalence survey; SD; standard deviation | |||||
Appendix B.3. Description of Drug Utilization Studies on Off-Label and Unlicensed Drugs Only (6 Studies)
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| Europe- Spain (one study) | |||||
| Casan 2017 | November 2015–February 2016 | Inclusion: all admissions Exclusion: crystalloid fluids, plasma-expanding serums (except for albumin), parenteral nutrition, antiseptics, and heparins for preventing catheter block | n = 41 (32%) | GA (mean (SD)): 35.9 (4.22) BW (mean (SD)): 3280 (860) | Mean (SD): 6.65 (3.28) |
| North America-Canada (one study) | |||||
| Doherty 2010 (27) | May 2009 (1 mo) | Inclusion: all admissions Exclusion: not reported | n = 38 (53%) | Not reported | Not reported |
| Asia-India (one study) | |||||
| Jain 2014 (57) | June–August 2009 | Inclusion: all inpatients for >6 h and had a drug Exclusion: nutritional supplements, IV fluids, inotropes, vaccines, vitamin K, topical anaesthetic cream, fluid or heparin for flushing IV lines, oxygen and blood products | n = 156 (not reported) | GA (median, IQR): 32, 30–35 BW (median, IQR): 1348, 1076–1800 | Median (IQR): 6, 1–6 |
| Middle East -Iran (one study) | |||||
| Kouti 2019 (58) | January–March 2016 (3 mo) | Inclusion: admitted for at least 24 h who received at least one medication Exclusion: oxygen, vaccines, blood products (except immunoglobulin), vitamins, electrolytes, TPN, IV fluids | n = 193 (41%) | GA (mean (SD)): 34 (4.4) BW (mean (SD)): 2463 (955) | Mean (SD): 4.5 (3) Range: 1–17 |
| Middle East-Saudi Arabia (one study) | |||||
| Mazhar 2018 (40) | January–March 2015 (3 mo) | Inclusion: all admitted neonates for a minimum of 24 h and prescribed at least one drug | n = 138 (48%) | GA (median, IQR): 35, 35–39 BW: not reported | Mean (SD): 3.5 (2.3) |
| Africa-Ethiopia (one study) | |||||
| Gidey 2020 (56) | March–April 2019 | Inclusion: admitted for at least 24h; prescribed at least one medication Exclusion: oxygen therapy, parenteral nutrition, blood products, antiseptics, vaccines and IV fluid (e.g., normal saline, dextrose); incomplete information in their prescription | n = 122 (41%) | GA: not reported BW (mean (SD)): 2540 (790) | Mean (SD): 3.02 (1.40) |
| BW, birthweight; GA, gestation age; IV; intravenous; NICU; neonatal intensive care unit; SD; standard deviation | |||||
Appendix B.4. Description of Drug Utilization Studies on Specific Pharmacologic Groups Only (7 Studies):
| Study ID | Study Period | Inclusion and Exclusion Criteria | Number of Neonates (% Female) | Gestation Age (Weeks) Birth Weight (Grams) | Number of Drugs Per Neonate |
|---|---|---|---|---|---|
| North America-USA (one study)-Antiepileptics | |||||
| Ahmad 2017 (64) | January 2005–December 2014 | Inclusion: all with diagnosis of seizure or seizure disorder and received one of the following AED: phenobarbital, phenytoin/fosphynytoin/levetiracetam, topiramate, lidocaine or carbamazepine Exclusion: benzodiazepine for sedation | n = 9134 (42%) | GA (mean (SD)): 34.8 (5.8) BW (mean (SD)): 2500(1200) | Not reported |
| North America-Canada (one study)-Sedatives and narcotics | |||||
| Toye 2018 | 2004–2009 | Inclusion: born at <35 weeks of GA admitted to NICUs contributing data to Canadian Neonatal Network 2004–2009 Exclusion: not reported | n = 12,415 (not reported) | Not reported | Not reported |
| North America-USA (one study)-Drugs used in BPD | |||||
| Bamat 2019 | January 2007–August 2016 | Inclusion: diagnosed with symptomatic bronchopulmonary dysplasia Exclusion: born at ≥32 weeks of GA, admitted after 36 weeks postmenstrual age; admitted for <1 week | n = 3252 (40%) | GA (median, (IQR)): 26 (24–28) BW (median, (IQR)): 790 (640–1040) | Range: 22–50 |
| Europe-Spain (one study)-Sedatives and analgesics | |||||
| Avila-Alvarez 2015 (7) | November 2012 (one mo) | Inclusion: all admissions during study period with corrected age of 44 Exclusion: not reported | n = 468 (45%) | GA (mean (SD)): 34.3 (4.6) BW (mean (SD)): 2182 (9764) | Not reported |
| Europe-France (one study)-Analgesics | |||||
| Benahmed-Canat 2019 (12) | January 2012–June 2013 | Inclusion: all infants undergoing surgery Exclusion: not reported | n = 168 (40%) | GA (mean (SD)): 35.1 (4.6) BW (mean (SD)): 2337(1006) | Mean (SD): 2.6 (1.3) |
| Europe-Estonia (one study)-Cardiovascular drugs | |||||
| Hallik 2014 (abstract) | Not reported | Not reported | n = 726 (not reported) | GA (median, range): 34, 23–42 BW (median, range): 1993, 400–4720 | Not reported |
| Europe-Spain (one study)-Intravenous drugs | |||||
| De Basagoiti 2019 (84) | January–February 2018 | Not reported | Not reported | Not reported | Not reported |
| BW, birthweight; GA, gestation age; NICU; neonatal intensive care unit; IQR, interquartile range; SD; standard deviation | |||||
References
- World Health Organization. International Working Group for Drug Statistics Methodology, Organizzazione Mondiale Della Sanità, Collaborating Centre for Drug Statistics Methodology, Organizzazione Mondiale Della Sanità, Collaborating Centre for Drug Utilization Research and clinical Pharmacological Services. Introduction to Drug Utilization Research; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Avorn, J. The Psychology of Clinical Decision Making—Implications for Medication Use. N. Engl. J. Med. 2018, 378, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Simons, S.; Van Den Anker, J. Research on medication use in the neonatal intensive care unit. Expert Rev. Clin. Pharmacol. 2019, 12, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Cantey, J.B.; Wozniak, P.S.; Sánchez, P.J. Prospective surveillance of antibiotic use in the neonatal intensive care unit: Results from the SCOUT study. Pediatr. Infect. Dis. J. 2015, 34, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Chimhini, G.; Chimhuya, S.; Madzudzo, L.; Heys, M.; Crehan, C.; Robertson, V.; Ferrand, R.; Sado, B.; Sharland, M.; Walker, A.; et al. Auditing use of antibiotics in Zimbabwean neonates. Infect. Prev. Pract. 2020, 2, 100046. [Google Scholar] [CrossRef]
- Sucasas, A.A.; Avila-Alvarez, A.; Combarro, E.M.; Martínez, R.C.; Yáñez, G.P.; Codias, L.A.; Luis, F.T.J.; Pertega, S.D. Use of off-label drugs in neonatal intensive care. An. Pediatr. 2019, 91, 237–243. [Google Scholar] [CrossRef]
- Aranda, J.V.; Collinge, J.M.; Clarkson, S. Epidemiologic aspects of drug utilization in a newborn intensive care unit. Semin. Perinatol. 1982, 6, 148–154. [Google Scholar]
- Aranda, J.V.; Clarkson, S.; Collinge, J.M. Changing pattern of drug utilization in a neonatal intensive care unit. Am J. Perinatol. 1983, 1, 28–30. [Google Scholar] [CrossRef]
- Ashwin, B.; Prashanth, M.V. Assessment of Medicine Prescribing Trends in Neonatal Intensive Care Unit: A Prospective Observational Study. In Proceedings of the 3rd International Conference on Academic and Industrial Innovations: Transitions in Pharmaceutical, Medical and Biosciences, Goa, India, 22–23 October 2018; p. 166. Available online: http://innopharm3.innovareacademics.in/wp-content/uploads/2018/03/Innopharm3-abstract-book.pdf (accessed on 4 August 2020).
- Barr, J.; Brenner, Z.G.; Heiman, E.; Pareth, G.; Bulkowstein, M.; Greenberg, R.; Berkovitch, M. Unlicensed and off-label medication use in a neonatal intensive care unit: A prospective study. Am. J. Perinatol. 2002, 19, 67–72. [Google Scholar] [CrossRef]
- Benahmed, C.A.; Plaisant, F.; Riche, B.; Rabilloud, M.; Canat, G.; Paret, N.; Claris, O.; Kassai, B.; Nguyen, K.A. Postsurgery analgesic and sedative drug use in a French neonatal intensive care unit: A single-center retrospective cohort study. Arch. Pediatr. Organe Soc. Fr. Pediatr. 2019, 26, 145–150. [Google Scholar] [CrossRef]
- Blanco, R.E.; Medina, C.A.F.; Vega-J, M.A.; Ocaña, R.R.; Márquez, R.E.I.; Ruiz, E.Á. Drug utilization pattern in children and off-label use of medicines in a pediatric intensive care unit. Med. Intensiva 2016, 40, 1–8. [Google Scholar]
- Brijal, S.P.; Kubavat, R.; Sondarva, B.; Piparva, G. Drug utilization study in neonatal intensive care unitat tertiary care hospital, rajkot, Gujarat: A prospective study. World J. Pharm. Pharm. Sci. 2015, 4, 2034–2042. [Google Scholar]
- Carvalho, C.; Silveira, R. Describing the use of off-label and not approved medications in a neonatal intensive care unit in south Brazil. Arch. Dis. Child. 2012, 97, A464–A465. [Google Scholar] [CrossRef][Green Version]
- Arocas, C.V.; Cabezuelo, E.B.; Garrido, -C.B.; De la Cruz, M.P.; Blázquez, Á.M.J.; De la Rubia, N.M.A. Off-label and unlicensed drug use in a Spanish Neonatal Intensive Care Unit. Farm Hosp Organo of Expresion Cient Soc. Espanola. Farm. Hosp. 2017, 41, 371–381. [Google Scholar]
- Chatterjee, S.; Mandal, A.; Lyle, N.; Mukherjee, S.; Singh, A.K. Drug utilization study in a neonatology unit of a tertiary care hospital in eastern India. Pharmacoepidemiol. Drug Saf. 2007, 16, 1141–1145. [Google Scholar] [CrossRef]
- Chauthankar, S.A.; Marathe, P.A.; Potey, A.V.; Nanavati, R.N. Drug Utilization in Neonatal Intensive Care Unit of a Tertiary-care Hospital in Mumbai, India. Indian Pediatr. 2017, 54, 931–934. [Google Scholar] [CrossRef]
- Mangal, K.C.; Jadhav, R.R.; Padwal, S.L. Drug utilization study in neonatal intensive care unit at rural tertiary care hospital. Asian J. Pharm. Clin. Res. 2017, 10, 102. [Google Scholar]
- Conroy, S.; McIntyre, J.; Choonara, I. Unlicensed and off label drug use in neonates. Arch Dis Child Fetal Neonatal Ed. 1999, 80, F142–F145. [Google Scholar] [CrossRef]
- Collinge, J.; Horton, L.; Aranda, J.V. Drug utilization and adversev drug reactions in a neonatal intensive care unit. NICU 1988, 5, 6. [Google Scholar]
- Daniell, A.J.; Darlow, B.A. Audit of drug usage in a regional neonatal intensive care unit. Aust. Paediatr. J. 1989, 25, 207–210. [Google Scholar] [CrossRef]
- de L. Costa, H.T.M.; Costa, T.X.; Martins, R.R.; Oliveira, A.G. Use of off-label and unlicensed medicines in neonatal intensive care. PLoS ONE 2018, 13, e0204427. [Google Scholar] [CrossRef] [PubMed]
- de Souza, A.S.; Dos Santos, D.B.; Rey, L.C.; Medeiros, M.G.; Vieira, M.G.; Coelho, H.L.L. Off-label use and harmful potential of drugs in a NICU in Brazil: A descriptive study. BMC Pediatr. 2016, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aera, M.; Gasbarro, A.R.; Padovano, M.; Laforgia, N.; Capodiferro, D.; Solarino, B.; Quaranta, R.; Dell’Erba, A. Unlicensed and off-label use of medicines at a neonatology clinic in Italy. Pharm. World Sci. 2007, 29, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Dessì, A.; Salemi, C.; Fanos, V.; Cuzzolin, L. Drug treatments in a neonatal setting: Focus on the off-label use in the first month of life. Pharm. World Sci. 2010, 32, 120–124. [Google Scholar] [CrossRef]
- Doherty, D.R.; Pascuet, E.; Ni, A.; Stewart, P.; Splinter, W.; Vaillancourt, R. Off-label drug use in pediatric anesthesia and intensive care according to official and pediatric reference formularies. Can. J. Anesth. J. Can. d’anesthésie 2010, 57, 1078–1088. [Google Scholar] [CrossRef]
- Du, W.; Warrier, I.; Tutag-Lehr, V.; Salari, V.; Ostrea, E.; Aranda, J. Changing Patterns of Drug Utilization in a Neonatal Intensive Care Population. Am. J. Perinatol. 2006, 23, 279–286. [Google Scholar] [CrossRef]
- Flint, R.; Simons, S.; Burger, D.; De Groot, R.; Reiss, I.; Tibboel, D. O-102 Analyses of Current Unlicensed And Off-label For Age Drug Prescriptions At A Neonatal Intensive Care Unit: Abstract O-102 Table 1. Arch. Dis. Child. 2014, 99, A63. [Google Scholar] [CrossRef]
- Fungo, M.S.M.; Vega, E.M. Drugs dispensed at the Division of Neonatology at University Hospital in Río Cuarto, Córdoba, Argentina. Arch. Argent. Pediatr. 2013, 111, 120–127. [Google Scholar]
- Girardi, A.; Galletti, S.; Raschi, E.; Koci, A.; Poluzzi, E.; Faldella, G.; Ponti, F. Pattern of drug use among preterm neonates: Results from an Italian neonatal intensive care unit. Ital. J. Pediatr. 2017, 43, 37. [Google Scholar] [CrossRef]
- Gonçalves, A.C.; de S. Reis, A.M.M.; Gusmão, A.C.M.; Bouzada, M.C.F. Drug utilization profile in the neonatal unit of a university hospital: A prospective observational study in Brazil. Int. J. Clin. Pharm. 2015, 37, 645–655. [Google Scholar]
- Gulati, R.; Elabiad, M.; Talati, A.J.; Dhanireddy, R. Trends in Medication Use in Very Low-Birth-Weight Infants in a Level 3 NICU over 2 Decades. Am. J. Perinatol. 2015, 33, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, K.; Usha, D.; Divya, J. Usage of off-label drugs among preterm babies admitted in a level III neonatal intensive care unit attached to a medical college in Southern Karnataka. J. Evol. Med Dent. Sci. 2017, 6, 6664–6667. [Google Scholar] [CrossRef]
- Jong, G.W.T.; Vulto, A.G.; De Hoog, M.; Schimmel, K.J.M.; Tibboel, D.; Anker, J.N.V.D. A survey of the use of off-label and unlicensed drugs in a Dutch children’s hospital. Pediatrics 2001, 108, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, E.; Valls, N.; Astudillo, P.; Valls, C.; Cavada, G.; Sandoval, A.; Alegría, A.; Ortega, G.; Núñez, D.; Mena, P. Evaluation of antimicrobial consumption in a Neonatology Unit: A team work to promote the rational use of antibiotics. Rev. Chil. Infectol. Organo Soc. Chil. Infectol. 2017, 34, 544–552. [Google Scholar] [CrossRef] [PubMed]
- A Kieran, E.; O’Callaghan, N.; O’Donnell, C. Unlicensed and off-label drug use in an Irish neonatal intensive care unit: A prospective cohort study. Acta Paediatr. 2014, 103, e139–e142. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Walker, J.K.; Hurt, K.M.; Bennett, K.M.; Grosshans, N.; Fotis, M.A. Medication Use in the Neonatal Intensive Care Unit: Current Patterns and Off-Label Use of Parenteral Medications. J. Pediatr. 2008, 152, 412–415. [Google Scholar] [CrossRef]
- Kumari, A.; Prasad, P. Satyender Drug utilization pattern in neonatal intensive care unit of a tertiary care hospital with particular emphasis on off-label drug use. J. Clin. Neonatol. 2019, 8, 15. [Google Scholar] [CrossRef]
- Mazhar, F.; Akram, S.; Haider, N.; Hadi, M.A.; Sultana, J. Off-label and unlicensed drug use in hospitalized newborns in a Saudi tertiary care hospital: A cohort study. Int. J. Clin. Pharm. 2018, 40, 700–703. [Google Scholar] [CrossRef]
- Marino, W.M. Patterns of drug utilization in neonatal intensive care unit (NICU) in different body weight groups of newborns. J. Perinat. Med. 2011. [Google Scholar]
- Martínez, R.L.; Poy, M.J.C.; Arenas, M.O.; Bautista, S.C. Drug use in a neonatal ICU: A prospective study. Farm. Hosp. 2005, 29. [Google Scholar]
- Neubert, A.; Lukas, K.; Leis, T.; Dormann, H.; Brune, K.; Rascher, W. Drug utilization on a preterm and neonatal intensive care unit in Germany: A prospective, cohort-based analysis. Eur. J. Clin. Pharmacol. 2010, 66, 87. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.-A.; Claris, O.; Kassai, B. Unlicensed and off-label drug use in a neonatal unit in France. Acta Paediatr. Oslo Nor. 1992 2011, 100, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Nir-Neuman, H.; Abu-Kishk, I.; Toledano, M.; Heyman, E.; Ziv-Baran, T.; Berkovitch, M. Unlicensed and Off-Label Medication Use in Pediatric and Neonatal Intensive Care Units: No Change Over a Decade. Adv. Ther. 2018, 35, 1122–1132. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, B.; Stone, R.J.; Morley, C.; Davies, P.; Cheng, D.; Lee, L.; Fox, A. Unlicensed and Off-Label Drug Use in an Australian Neonatal Intensive Care Unit. Pediatrics 2002, 110, e52. [Google Scholar] [CrossRef]
- Payares, M.C.; Galiana, F.J. Off-label use of medications in the Paediatric and Neonatal Intensive Care Units. Br. J. Clin. Pharmacol. 2009, 286. [Google Scholar]
- Sharanappa, M.; Vishwanath, Y.; Lakshminarayana, K.; Swathi, A. Pattern of Drug Utilization in Neonatal Intensive Care Unit in a Tertiary Care Hospital. J. Biomed. Res. 2014, 5. [Google Scholar]
- Shinde, A.; Shinde, R.; Mohite, R. Pattern of antibiotics utilization in neonatal septicemia: A cross-sectional study from rural tertiary care hospital western Maharashtra, India. Int. J. Pharm. Pharm. Sci. 2017, 9, 60. [Google Scholar] [CrossRef]
- Silva, J.; De Lima, F.F.; Soares, H.; Guimarães, H. Off-Label and Unlicensed Drug Use in Neonatology: Reality in a Portuguese University Hospital. Acta Médica Portuguesa 2015, 28, 297–306. [Google Scholar] [CrossRef][Green Version]
- Suryawanshi, S.; Suryawanshi, P.; Pandit, V. Drug utilization study in a neonatology unit of a tertiary care hospital in pune city. World J. Pharmacol. Pharm. Sci. 2016, 5, 1236–1246. [Google Scholar]
- Subash, K.; Shanmugapriyan, S. A study on prescription of antibiotics utilization in neonatal intensive care at a tertiary care center. Int. J. Med. Res. Health Sci. 2015, 4, 265. [Google Scholar] [CrossRef]
- Warrier, I.; Du, W.; Natarajan, G.; Salari, V.; Aranda, J. Patterns of Drug Utilization in a Neonatal Intensive Care Unit. J. Clin. Pharmacol. 2006, 46, 449–455. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Balkhy, H.; El-Saed, A.; AlShehri, A.; Alshaalan, M.; Hijazi, O.; El-Metwally, A.A.S.; Aljohany, S.M.; Al Saif, S. Antimicrobial consumption in three pediatric and neonatal intensive care units in Saudi Arabia: 33-month surveillance study. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Chen, L.; Choonara, I.; Xiong, T.; Ojha, S.; Tang, J.; Wang, Y.; Zeng, L.; Shi, J.; Wang, H.; et al. Cross-sectional study of drug utilization in a Chinese neonatal unit. J. Int. Med. Res. 2020, 48, 300060520914197. [Google Scholar] [CrossRef] [PubMed]
- Gidey, M.T.; Gebretsadkan, Y.G.; Tsadik, A.G.; Welie, A.G.; Assefa, B.T. Off-label and unlicensed drug use in Ayder comprehensive specialized hospital neonatal intensive care unit. Ital. J. Pediatr. 2020, 46, 41–47. [Google Scholar] [CrossRef]
- Jain, S.; Saini, S.S.; Chawla, D.; Kumar, P.; Dhir, S. Off-label use of drugs in neonatal intensive care units. Indian Pediatr. 2014, 51, 644–646. [Google Scholar] [CrossRef]
- Kouti, L.; Aletayeb, M.; Aletayeb, S.M.H.; Hardani, A.K.; Eslami, K. Pattern and extent of off-label and unlicensed drug use in neonatal intensive care units in Iran. BMC Pediatr. 2019, 19, 3. [Google Scholar] [CrossRef]
- Lass, J.; Käär, R.; Jõgi, K.; Varendi, H.; Metsvaht, T.; Lutsar, I. Drug utilization pattern and off-label use of medicines in Estonian neonatal units. Eur. J. Clin. Pharmacol. 2011, 67, 1263–1271. [Google Scholar] [CrossRef]
- Lesko, S.M.; Epstein, M.F.; Mitchell, A.A. Recent patterns of drug use in newborn intensive care. J. Pediatr. 1990, 116, 985–990. [Google Scholar] [CrossRef]
- Lindner, U.; Hilgendorff, A.; Frey, G.; Gortner, L. Drug utilization in very preterm infants: Any changes during the past decade? Klin. Padiatr. 2008, 220, 238–242. [Google Scholar] [CrossRef]
- Riou, S.; Plaisant, F.; Maucort-Boulch, D.; Kassai-Koupai, B.; Claris, O.; Nguyen, K.A.; Plaisant, F. Unlicensed and off-label drug use: A prospective study in French NICU. Acta Paediatr. 2015, 104, e228–e231. [Google Scholar] [CrossRef]
- Schweigertova, J.; Durisova, A.; Dolnikova, D.; Ondriasova, E.; Balazova, M.; Slezakova, V.; Kuzelova, M. Off-label and unlicensed use of medicinal products in the neonatal setting in the Slovak Republic. Pediatr. Int. 2015, 58, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.A.; Desai, S.J.; Bennett, M.M.; Ahmad, S.F.; Ng, Y.-T.; Clark, R.H.; Tolia, V.N. Changing antiepileptic drug use for seizures in US neonatal intensive care units from 2005 to 2014. J. Perinatol. 2016, 37, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Mesek, I.; Nellis, G.; Lass, J.; Metsvaht, T.; Varendi, H.; Visk, H.; Turner, M.A.; Nunn, A.J.; Duncan, J.; Lutsar, I. Medicines prescription patterns in European neonatal units. Int. J. Clin. Pharm. 2019, 41, 1578–1591. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.R.A.; Jaszkowski, E.; Schober, T.; Von Both, U.; Meyer-Buehn, M.; Marques, A.F.; Farkas, B.; De Abreu, B.S.; Di Biase, C.B.; Takahashi, J.M.; et al. Patterns of antimicrobial consumption in neonatal and pediatric intensive care units in Germany and Brazil. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 39, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Laforgia, N.; Nuccio, M.M.; Schettini, F.; Dell’Aera, M.; Gasbarro, A.R.; Dell’Erba, A.; Solarino, B. Off-label and unlicensed drug use among neonatal intensive care units in Southern Italy. Pediatr. Int. 2014, 56, 57–59. [Google Scholar] [CrossRef]
- Oğuz, Ş.S.; Kanmaz, H.G.; Dilmen, U. Off-label and unlicensed drug use in neonatal intensive care units in Turkey: The old-inn study. Int. J. Clin. Pharm. 2012, 34, 136–141. [Google Scholar] [CrossRef]
- Hsieh, E.M.; Hornik, C.P.; Clark, R.H.; Laughon, M.M.; Benjamin, D.K.; Smith, P.B.; Network, B.P.F.C.A.T. Medication use in the neonatal intensive care unit. Am. J. Perinatol. 2013, 31, 811–821. [Google Scholar] [CrossRef]
- Clark, R.H.; Bloom, B.T.; Spitzer, A.R.; Gerstmann, D.R. Reported Medication Use in the Neonatal Intensive Care Unit: Data from a Large National Data Set. Pediatrics 2006, 117, 1979–1987. [Google Scholar] [CrossRef]
- Cuzzolin, L.; Agostino, R. Off-label and unlicensed drug treatments in Neonatal Intensive Care Units: An Italian multicentre study. Eur. J. Clin. Pharmacol. 2015, 72, 117–123. [Google Scholar] [CrossRef]
- Puia, D.M.; Younge, N.; Benjamin, D.K.; Lawson, K.; Hume, C.; Hill, K.; Mengistu, J.; Wilson, A.; Zimmerman, K.O.; Ahmad, K.; et al. Medications and in-hospital outcomes in infants born at 22–24 weeks of gestation. J. Perinatol. 2020, 40, 781–789. [Google Scholar] [CrossRef]
- Aamir, M.; Khan, J.A.; Shakeel, F.; Shareef, R.; Shah, N. Drug utilization in neonatal setting of Pakistan: Focus on unlicensed and off label drug prescribing. BMC Pediatr. 2018, 18, 242. [Google Scholar] [CrossRef] [PubMed]
- Gouyon, B.; Martin-Mons, S.; Iacobelli, S.; Razafimahefa, H.; Kermorvant-Duchemin, E.; Brat, R.; Caeymaex, L.; Couringa, Y.; Alexandre, C.; Lafon, C.; et al. Characteristics of prescription in 29 Level 3 Neonatal Wards over a 2-year period (2017-2018). An inventory for future research. PLoS ONE 2019, 14, e0222667. [Google Scholar] [CrossRef] [PubMed]
- Bonati, M.; Colombo, F.; Brambilla, C. Early neonatal drug utilization in preterm newborns in neonatal intensive care units. Italian Collaborative Group on Preterm Delivery. Dev. Pharmacol. Ther. 1988, 11, 1–7. [Google Scholar]
- Flint, R.B.; Van Beek, F.; Andriessen, P.; Zimmermann, L.J.; Liem, K.D.; Reiss, I.K.; De Groot, R.; Tibboel, D.; Burger, D.M.; Simons, S.H.; et al. Large differences in neonatal drug use between NICUs are common practice: Time for consensus? Br. J. Clin. Pharmacol. 2018, 84, 1313–1323. [Google Scholar] [CrossRef]
- Gortner, L.; Bernsau, U.; Brand, M.; Hellwege, H.; Hieronimie, G.; Jorch, G.; Reiter, H.; Versmold, I. Drug Utilization in Very Premature Infants in Neonatal Intensive Care Units. Dev. Pharmacol. Ther. 1991, 17, 167–171. [Google Scholar] [CrossRef]
- Russell, W.L.; McKenzie, M.W. Drug usage in newborn intensive care units. Hosp. Formul. 1983, 18, 631. [Google Scholar]
- Turner, M.A.; Lewis, S.; Hawcutt, D.B.; Field, D. Prioritising neonatal medicines research: UK Medicines for Children Research Network scoping survey. BMC Pediatr. 2009, 9, 50. [Google Scholar] [CrossRef]
- World Health Organization. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/193736 (accessed on 3 June 2017).
- Million Death Study Collaborators; Bassani, D.G.; Kumar, R.; Awasthi, S.; Morris, S.K.; Paul, V.K.; Shet, A.; Ram, U.; Gaffey, M.F.; E Black, R.; et al. Causes of neonatal and child mortality in India: A nationally representative mortality survey. Lancet 2010, 376, 1853–1860. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; E Lawn, J.; Cousens, S.; Mathers, C.; E Black, R. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef]
- Korang, S.K.; Safi, S.; Gluud, C.; Lausten-Thomsen, U.; Jakobsen, J.C. Antibiotic regimens for neonatal sepsis—A protocol for a systematic review with meta-analysis. Syst. Rev. 2019, 8, 1–13. [Google Scholar] [CrossRef]
- Laxminarayan, R.; A Bhutta, Z. Antimicrobial resistance-a threat to neonate survival. Lancet Glob. Heal. 2016, 4, e676–e677. [Google Scholar] [CrossRef]
- Chaurasia, S.; Sivanandan, S.; Agarwal, R.; Ellis, S.; Sharland, M.; Sankar, M.J. Neonatal sepsis in South Asia: Huge burden and spiralling antimicrobial resistance. BMJ 2019, 364, k5314. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, C.B.; Cantey, J.B. Antibiotic Resistance in the Neonatal Intensive Care Unit. NeoReviews 2019, 20, e135–e144. [Google Scholar] [CrossRef] [PubMed]
- Rosli, R.; Dali, A.F.; Aziz, N.A.; Abdullah, A.H.; Ming, L.C.; Manan, M.M. Drug Utilization on Neonatal Wards: A Systematic Review of Observational Studies. Front. Pharmacol. 2017, 8. [Google Scholar] [CrossRef]
- Krzyzaniak, N.; Pawłowska, I.; Bajorek, B. Review of drug utilization patterns in NICUs worldwide. J. Clin. Pharm. Ther. 2016, 41, 612–620. [Google Scholar] [CrossRef]






| Geographic Region (Number of Studies) (Ref) | Most Frequently Prescribed Drugs (Number of Studies Citing the Drug among the 10 Most Frequently Prescribed Drugs) |
|---|---|
| Europe (24 studies) [7,13,20,25,26,29,31,35,37,42,43,44,50,59,62,63,65,67,68,71,74,75,76,79] | caffeine (18 studies), gentamicin (17 studies), ampicillin (11 studies), furosemide (9 studies), multivitamins (9 studies), vitamin K (11 studies), benzylpenicillin (8 studies), amikacin (6 studies), morphine (5 studies), paracetamol (6 studies) |
| North America (10 studies) [8,9,28,38,53,60,69,70,72,78] | ampicillin (8 studies), gentamicin (8 studies), furosemide (6 studies), surfactant (6 studies), penicillin (5 studies), vancomycin (6 studies), caffeine citrate* (6 studies), cefotaxime (4 studies), dopamine (5 studies), calcium gluconate (4 studies) |
| Asia (6 studies) [14,17,19,51,55,73] | phenobarbitone (4 studies), vitamin K (4 studies), amikacin (3 studies), aminophylline (3 studies), ceftriaxone (2 studies), ceftazidime (2 studies), gentamicin (2 studies), phenytoin (2 studies), penicillin/sulbactam (2 studies),caffeine (1 study) |
| Latin America and Caribbean (4 studies) [15,24,32,41] | fentanyl (4 studies), gentamicin (3 studies), vancomycin (3 studies), multivitamins (3 studies), amikacin (2 studies), ampicillin (2 studies), furosemide (2 studies), aminophylline (2 studies), morphine (1 study), metamizole (1 study) |
| Middle East (2 studies) [11,45] | gentamicin, ampicillin, amoxicillin, vitamins |
| Australasia (2 studies) [22,46] | vancomycin, gentamicin |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Turkait, A.; Szatkowski, L.; Choonara, I.; Ojha, S. Review of Drug Utilization Studies in Neonatal Units: A Global Perspective. Int. J. Environ. Res. Public Health 2020, 17, 5669. https://doi.org/10.3390/ijerph17165669
Al-Turkait A, Szatkowski L, Choonara I, Ojha S. Review of Drug Utilization Studies in Neonatal Units: A Global Perspective. International Journal of Environmental Research and Public Health. 2020; 17(16):5669. https://doi.org/10.3390/ijerph17165669
Chicago/Turabian StyleAl-Turkait, Asma, Lisa Szatkowski, Imti Choonara, and Shalini Ojha. 2020. "Review of Drug Utilization Studies in Neonatal Units: A Global Perspective" International Journal of Environmental Research and Public Health 17, no. 16: 5669. https://doi.org/10.3390/ijerph17165669
APA StyleAl-Turkait, A., Szatkowski, L., Choonara, I., & Ojha, S. (2020). Review of Drug Utilization Studies in Neonatal Units: A Global Perspective. International Journal of Environmental Research and Public Health, 17(16), 5669. https://doi.org/10.3390/ijerph17165669