Physical Activity Counseling in Primary Care in Germany—An Integrative Review


Abstract
1. Introduction
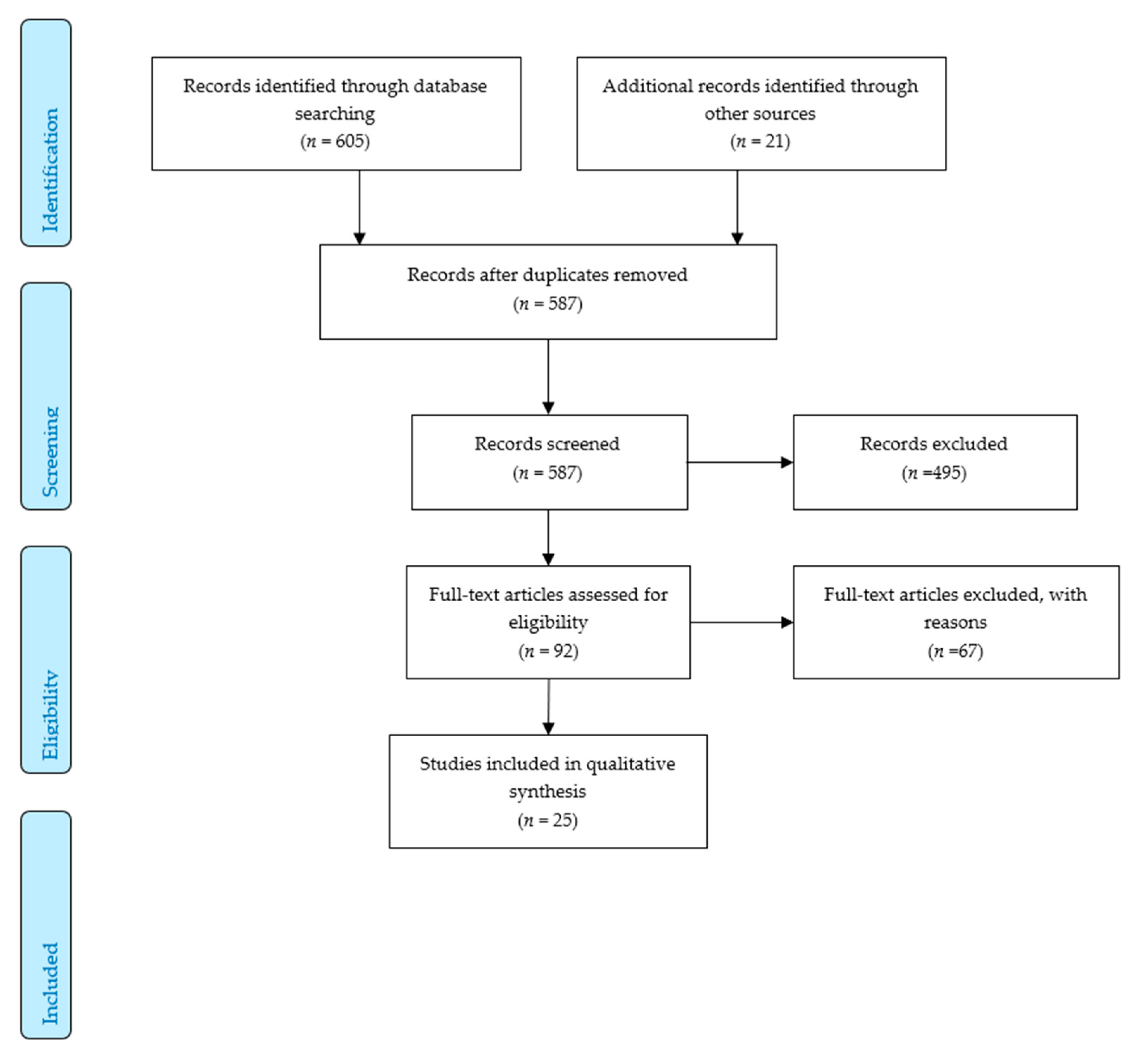
2. Materials and Methods
3. Results
3.1. Study Quality
3.2. Content of PA Counseling
3.3. Self-Assessed Competences and Knowledge, Ability to Motivate
3.4. Barriers
3.5. Effects of Counseling
4. Discussion
4.1. Prevalence of Counseling
4.2. Contents of Counseling
4.3. Barriers
4.4. Findings in Relation to Other Countries
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Füzéki, E.; Vogt, L.; Banzer, W. German National Physical Activity Recommendations for Adults and Older Adults: Methods, Database and Rationale. [Nationale Bewegungsempfehlungen für Erwachsene und ältere Erwachsene—Methodisches Vorgehen, Datenbasis und Begründung]. Gesundheitswesen 2017, 79, S20–S28. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Finger, J.D.; Mensink, G.B.M.; Lange, C. Health-enhancing physical activity during leisure time among adults in Germany. J. Health Monit. 2017, 2, 35–42. [Google Scholar]
- Physical Activity Strategy for the WHO European Region 2016–2025; World Health Organisation Regional Office for Europe: Copenhagen, Denmark, 2016; ISBN 9289051477.
- German Federal Medical Chamber Minutes of the 122nd Annual Meeting of the German Federal Medical Chamber [Bundesärztekammer. Beschlussprotokoll 122. Deutscher Ärztetag]. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/downloads/pdf-Ordner/122.DAET/122DAETBeschlussprotokoll.pdf (accessed on 2 January 2020).
- Lion, A.; Vuillemin, A.; Thornton, J.S.; Theisen, D.; Stranges, S.; Ward, M. Physical activity promotion in primary care: A Utopian quest? Health Promot. Int. 2019, 34, 877–886. [Google Scholar] [CrossRef]
- Arsenijevic, J.; Groot, W. Physical activity on prescription schemes (PARS): Do programme characteristics influence effectiveness? Results of a systematic review and meta-analyses. BMJ Open 2017, 7, e012156. [Google Scholar] [CrossRef]
- Campbell, F.; Holmes, M.; Everson-Hock, E.; Davis, S.; Buckley Woods, H.; Anokye, N.; Tappenden, P.; Kaltenthaler, E. A systematic review and economic evaluation of exercise referral schemes in primary care: A short report. Health Technol. Assess. 2015, 19, 1–110. [Google Scholar] [CrossRef]
- Onerup, A.; Arvidsson, D.; Blomqvist, Å.; Daxberg, E.-L.; Jivegård, L.; Jonsdottir, I.H.; Lundqvist, S.; Mellén, A.; Persson, J.; Sjögren, P.; et al. Physical activity on prescription in accordance with the Swedish model increases physical activity: A systematic review. Br. J. Sports Med. 2019, 53, 383–388. [Google Scholar] [CrossRef]
- Orrow, G.; Kinmonth, A.-L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef]
- Sanchez, A.; Bully, P.; Martinez, C.; Grandes, G. Effectiveness of physical activity promotion interventions in primary care: A review of reviews. Prev. Med. 2015, 76, S56–S67. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Gabrys, L.; Jordan, S. Prevalence, Current Trends and Regional Differences of Physical Activity Counselling in Germany [Prävalenz, zeitliche Trends und regionale Unterschiede ärztlicher Bewegungsberatung in Deutschland]. Dtsch. Z. Sportmed. 2016, 67, 53–58. [Google Scholar] [CrossRef]
- Gabrys, L.; Jordan, S.; Schlaud, M. Prevalence and temporal trends of physical activity counselling in primary health care in Germany from 1997–1999 to 2008–2011. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 136. [Google Scholar] [CrossRef] [PubMed]
- Wangler, J.; Jansky, M. Importance of primary care providers for promotion of exercise and health in older patients—survey results. [Die Bedeutung des hausärztlichen Settings für die Bewegungs-und Gesundheitsförderung im höheren Lebensalter—Ergebnisse einer Befragung]. Präv. Gesundheitsf. 2019, 69, 401. [Google Scholar] [CrossRef]
- Vogt, L.; Hoppe, I.; Thoma, R.; Gabrys, L.; Friedrich, G.; Coester, E.; Fuzeki, E.; Banzer, W. Wirksamkeit des Rezepts für Bewegung aus Patientensicht—Die ärztliche Beratung und Handlungsabsichten/konsequenzen nach erfolgter Rezeptverschreibung. [Exercise on Prescription-Patients’ Perceptions on Effectiveness and Change in Physical Activity Behavior]. Dtsch. Med. Wochenschr. 2019, 144, e64–e69. [Google Scholar] [CrossRef]
- Hinrichs, T.; Moschny, A.; Klaassen-Mielke, R.; Trampisch, U.; Thiem, U.; Platen, P. General practitioner advice on physical activity: Analyses in a cohort of older primary health care patients (getABI). BMC Fam. Pract. 2011, 12, 26. [Google Scholar] [CrossRef]
- Tönges, S.; Weidmann, C.; Schneider, S. Compliance with medical advice on physical activity. Which patients are resistant to advice? [Compliance nach ärztlicher Sportempfehlung. Welche Patienten sind beratungsresistent?]. Präv. Gesundheitsf. 2006, 1, 108–114. [Google Scholar] [CrossRef]
- Mortsiefer, A.; Ludt, S.; Pentzek, M.; Wilm, S.; Brotons, C. Patients’ Needs and Expectations Concerning Prevention and Health Advice in Primary Care. Results from the EUROPREVIEW Survey. [Welche Erwartungen hinsichtlich Prävention und Gesundheitsberatung haben Patienten an ihre Hausärzte? Ergebnisse aus dem EUROPREVIEW—Patientensurvey]. Gesundheitswesen 2014, 76, 417–422. [Google Scholar] [CrossRef]
- Keil, J.; Brendler, V.; Sachse, C.; Zülke, A.; Zeynalova, S.; Engel, C.; Loeffler, M.; Riedel-Heller, S.G.; König, H.-H.; Stengler, K. Gender-Specific Differences in the Utilization of Health Care Services in an Urban Population Sample. [Geschlechterspezifische Inanspruchnahme von Gesundheitsleistungen in einer urbanen Erwachsenenpopulation]. Gesundheitswesen 2019. [Google Scholar] [CrossRef]
- Reimers, C.D.; Reuter, I.; Straube, A.; Tettenborn, B.; Braumann, K.M.; Reimers, A.K. Physician Counseling about Physical and Sports Activity in Neurological Practices in Germany: Results of a Survey Among Members of the German Neurological Society. [Beratung zu körperlicher und sportlicher Aktivität in neurologischen Praxen in Deutschland. Ergebnisse einer Umfrage unter den Mitgliedern der Deutschen Gesellschaft für Neurologie e.V.]. Fortschr. Neurol. Psychiatr. 2016, 84, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Schwab, M.; Faller, H.; Meng, K. Training for physicians for physical activity promotion in older adults. Needs assessment and formative evaluation of a first offer. [Schulung für Ärzte zur Bewegungsförderung bei Älteren Bedarfsanalyse und Bewertung eines ersten Angebots]. Präv. Gesundheitsf. 2017, 12, 218–225. [Google Scholar] [CrossRef]
- Curbach, J.; Apfelbacher, C.; Knoll, A.; Herrmann, S.; Szagun, B.; Loss, J. Physicians’ perspectives on implementing the prevention scheme “Physical Activity on Prescription”: Results of a survey in Bavaria. Z. Evid. Fortbild. Qual. Gesundhwes. 2018, 131–132, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Diehl, K.; Bock, C.; Herr, R.M.; Mayer, M.; Görig, T. Modifying health behavior to prevent cardiovascular diseases: A nationwide survey among German primary care physicians. Int. J. Environ. Res. Public Health 2014, 11, 4218–4232. [Google Scholar] [CrossRef]
- Görig, T.; Diehl, K.; Herr, R.M.; Bock, C.; Mayer, M.; Schneider, S. Differences in the Provision of Lifestyle Counseling for Cardiovascular Disease Prevention Between Urban and Rural Regions in Germany. Findings from a National Survey of Primary Care Physicians. [Stadt-Land-Unterschiede im Angebot von Lebensstilberatung zur Prävention kardiovaskulärer Erkrankungen in der Hausarztpraxis. Ergebnisse einer bundesweiten Hausärztebefragung]. Gesundheitswesen 2016, 78, 533–538. [Google Scholar] [CrossRef]
- Diehl, K.; Gansefort, D.; Herr, R.M.; Gorig, T.; Bock, C.; Mayer, M.; Schneider, S. Physician Gender and Lifestyle Counselling to Prevent Cardiovascular Disease: A Nationwide Representative Study. J. Public Health Res. 2015, 4, 534. [Google Scholar] [CrossRef]
- Diehl, K.; Mayer, M.; Mayer, F.; Gorig, T.; Bock, C.; Herr, R.M.; Schneider, S. Physical activity counseling by primary care physicians: Attitudes, knowledge, implementation, and perceived success. J. Phys. Act. Health 2015, 12, 216–223. [Google Scholar] [CrossRef]
- Bock, C.; Diehm, C.; Schneider, S. Physical activity promotion in primary health care: Results from a German physician survey. Eur. J. Gen. Pract. 2012, 18, 86–91. [Google Scholar] [CrossRef]
- Holmberg, C.; Sarganas, G.; Mittring, N.; Braun, V.; Dini, L.; Heintze, C.; Rieckmann, N.; Muckelbauer, R.; Muller-Nordhorn, J. Primary prevention in general practice—Views of German general practitioners: A mixed-methods study. BMC Fam. Pract. 2014, 15, 103. [Google Scholar] [CrossRef]
- Holmberg, C.; Muckelbauer, R.; Sarganas, G.; Braun, V.; Heintze, C.; Dini, L.; Müller-Nordhorn, J. Primary Prevention in General Medical Practice: A Survey. [Primärprävention in der Allgemeinarztpraxis: Eine Befragung]. Gesundheitswesen 2018, 80, 465–470. [Google Scholar] [CrossRef]
- Karl, T. Health Promotion, Primary and Secondary Prevention in General Practice. Ph.D. Thesis, Charité Berlin, Berlin, Germany, 2013. Unpublished medical. [Google Scholar]
- Rosemann, T.; Wensing, M.; Joest, K.; Backenstrass, M.; Mahler, C.; Szecsenyi, J. Problems and needs for improving primary care of osteoarthritis patients: The views of patients, general practitioners and practice nurses. BMC Musculoskelet. Disord. 2006, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Heintze, C.; Metz, U.; Hahn, D.; Niewohner, J.; Schwantes, U.; Wiesner, J.; Braun, V. Counseling overweight in primary care: An analysis of patient-physician encounters. Patient Educ. Couns. 2010, 80, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Sonntag, U.; Henkel, J.; Renneberg, B.; Bockelbrink, A.; Braun, V.; Heintze, C. Counseling overweight patients: Analysis of preventive encounters in primary care. Int. J. Qual. Health Care 2010, 22, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Kroll, M.M.C. Obesity Management in Primary Care from the View of the Affected: A Qualitative Analysis of Patients’ Interviews [Adipositasmanagement in der Hausarztpraxis aus der Sicht Betroffener: Eine qualitative Analyse von Patienteninterviews]. Ph.D. Thesis, Berlin Free University, Berlin, Germany, Unpublished medical. 2014. [Google Scholar]
- Brinck, Anna Gerda Sieglinde Lieselotte. Care of Overweight Patients in Family Practice: A Qualitative Analysis of Interviews with Family Doctors from Berlin and Brandenburg [Betreuung Übergewichtiger Patienten in der Hausarztpraxis: Eine Qualitative Analyse von Interviews Mit Hausärzten aus Berlin und Brandenburg]. Ph.D. Thesis, Charité Berlin, Berlin, Germany, 2012. Unpublished medical.
- Ruhmann, L. Survey of Selected Berlin Physicians for an Evaluation of the Exercise on Prescription in Berlin [Befragung von Ausgewählten Berliner Ärztinnen und Ärzten für Eine Evaluation des Rezeptes für Bewegung in Berlin]. Master’s Thesis, Charité Berlin, Berlin, Germany, 2014. Unpublished. [Google Scholar]
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing risk of bias in prevalence studies: Modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf (accessed on 23 November 2019).
- Andersen, P.; Holmberg, S.; Lendahls, L.; Nilsen, P.; Kristenson, M. Physical Activity on Prescription with Counsellor Support: A 4-Year Registry-Based Study in Routine Health Care in Sweden. Healthcare (Basel) 2018, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.M.; Schoenborn, C.A. Trends in adults receiving a recommendation for exercise or other physical activity from a physician or other health professional. NCHS Data Brief. 2012, 41, 1–8. [Google Scholar]
- Smith, A.W.; Borowski, L.A.; Liu, B.; Galuska, D.A.; Signore, C.; Klabunde, C.; Huang, T.T.-K.; Krebs-Smith, S.M.; Frank, E.; Pronk, N.; et al. U.S. Primary Care Physicians’ Diet, Physical Activity, and Weight-Related Care of Adult Patients. Am. J. Prev. Med. 2011, 41, 33–42. [Google Scholar] [CrossRef]
- Hébert, E.T.; Caughy, M.O.; Shuval, K. Primary care providers’ perceptions of physical activity counselling in a clinical setting: A systematic review. Br. J. Sports Med. 2012, 46, 625–631. [Google Scholar] [CrossRef]
- Andersen, P.; Lendahls, L.; Holmberg, S.; Nilsen, P. Patients’ experiences of physical activity on prescription with access to counsellors in routine care: A qualitative study in Sweden. BMC Public Health 2019, 19, 210. [Google Scholar] [CrossRef]
- Costello, E.; Leone, J.E.; Ellzy, M.; Miller, T.A. Older adult perceptions of the physicians’ role in promoting physical activity. Disabil. Rehabil. 2013, 35, 1191–1198. [Google Scholar] [CrossRef]
- Horne, M.; Skelton, D.; Speed, S.; Todd, C. The influence of primary health care professionals in encouraging exercise and physical activity uptake among White and South Asian older adults: Experiences of young older adults. Patient Educ. Couns. 2010, 78, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Short, C.E.; Hayman, M.; Rebar, A.L.; Gunn, K.M.; de Cocker, K.; Duncan, M.J.; Turnbull, D.; Dollman, J.; van Uffelen, J.G.Z.; Vandelanotte, C. Physical activity recommendations from general practitioners in Australia. Results from a national survey. Aust. N. Z. J. Public Health 2016, 40, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Florindo, A.A.; Mielke, G.I.; Gomes, G.A.d.O.; Ramos, L.R.; Bracco, M.M.; Parra, D.C.; Simoes, E.J.; Lobelo, F.; Hallal, P.C. Physical activity counseling in primary health care in Brazil: A national study on prevalence and associated factors. BMC Public Health 2013, 13, 794. [Google Scholar] [CrossRef] [PubMed]
- Petrella, R.J.; Lattanzio, C.N.; Overend, T.J. Physical activity counseling and prescription among canadian primary care physicians. Arch. Intern. Med. 2007, 167, 1774–1781. [Google Scholar] [CrossRef]
- O’Brien, S.; Prihodova, L.; Heffron, M.; Wright, P. Physical activity counselling in Ireland: A survey of doctors’ knowledge, attitudes and self-reported practice. BMJ Open Sport Exerc. Med. 2019, 5, e000572. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, H.; Fortier, M.; Hogg, W. Physical activity counseling in primary care: Who has and who should be counseling? Patient Educ. Couns. 2006, 64, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.; Khangura, S.; Brehaut, J.C.; Graham, I.D.; Moher, D.; Potter, B.K.; Grimshaw, J.M. Reporting guidelines for survey research: An analysis of published guidance and reporting practices. PLoS Med. 2010, 8, e1001069. [Google Scholar] [CrossRef]


{kind=link}
| Patients Surveys | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study | Primary Research Question | Secondary Research Question | Survey Instrument and Survey Mode | Sample | Place and Time of the Survey | Response Rate | Statistics, Dealing with Missing Values | Main Results | Risk of Bias According to Hoy et al. |
| [15] | Representative data on health of the general population. Health services utilization | Prevalence of physicians’ PA 1 counseling in the 12 previous months; time trends and regional differences | Self-developed 1-item instrument Validity n.r. 2 Paper-pencil survey. Self-report | BGS 98 3 und DEGS 1 4; representative sample n = 11,907 Between 18 and 64 years | Nationwide; 1997–1999 and 2008–2011 | n.r. | Logistic regression; missing values: n.r. | Prevalence of physicians’ PA counseling dropped significantly from 10.1% (BGS 98) to 8.6% (DEGS 1) (OR 5 0.83, 95% CI 6 0.72–096) Higher prevalence in larger cities than in rural regions (BGS 98: OR 1.8, 95% CI 1.26–2.58; DEGS 1: 1.49, 95% CI 1.01–2.20) | 5/10 |
| [16] | Representative data on health of the general population. Health services utilization | Prevalence of physicians’ PA counseling in the 12 previous months. Participation in preventive PA courses | Self-developed 1-item instrument Validity n.r. Paper-pencil survey. Self-report | BGS 98 and DEGS 1; representative sample n = 11,907 Between 18 and 64 years | Nationwide; 1997–1999 and 2008–2011 | n.r. | Logistic regression; missing values: n.r. | Prevalence of physicians’ PA counseling dropped between 1997–1999 and 2008–2011, increased prevalence of physicians’ PA counseling in diabetics (OR 3.42, 95 % CI 1.68–6.96) and patients with cardiometabolic risk factors (OR 5.33, 95 % CI 1.89–15.00) Individuals who receive counseling are more likely to participate in preventive PA courses | 5/10 |
| [17] | Relevance and role of general practitioners in increasing PA in elderly patients | Exercise | Self-developed instrument with four thematic blocks pretest Validity n.r. Paper-pencil survey in waiting room. Self-report | n = 400 ≥70 years | 25 practices in the Federal State of Rhineland-Palatinate; November 2018–April 2019 | 324/400 (81%) | Descriptive analysis; missing values: n.r. | 48% have received counseling at least once; 52% report to be “more or less active”; 52% would like to become more active, of which 93% has no information on suitable courses; 88% would welcome in physicians cooperated more with health oriented PA providers | 4/10 |
| [18] | Perceived quality of counseling on Exercise on Prescription. Intention and consequences following a counseling on Exercise on Prescription | Self-developed 17-item instrument Validity n.r. Paper-pencil survey. Self-report | Patients who have received counseling on Exercise on Prescription n = 173 | 12 Practices in 8 “Sports Regions” in the Federal State of Hessia January–March 2014 | 51/173 (29.48%) | Contingency table, OR, missing values: n.r. | Counseling mainly perceived as positive, increased awareness for PA and health, 53% report doing more exercise, 51% more active in daily life | 4/10 | |
| [19] | Prevalence of peripheral arterial disease in the elderly in family practice | Prevalence of family practitioners’ PA counseling in the 12 previous months in the elderly | Self-developed 1 item instrument in the getABI Study 7 Computer-assisted telephone interview Validity n.r. | Participants of the getABI Study n = 5578, ≥65 years | Family practitioners nationwide 2008 | 1937/5578 (7 years follow-up) 193/1627 (29.16%) | Logistic regression missing values: n.r. | 32.8% of patients report having received PA counseling men (OR 1.34, 95% CI 1.06–1.70). patients with pain (OR 1.43, 95% CI 1.13–1.81). with coronary heart disease and/or myocardial infarction (OR 1.56, 95% CI 1.21–2.01). Diabetes mellitus (OR 1.79, 95% CI 1.39–2.30) and arthritis (OR 1.37, 95% CI 1.08–1.73). and patients with multi-medication (>5 medications (OR 1.41, 95% CI 1.11–1.80) | 5/10 |
| [20] | Representative data on health of the general population. Health services utilization | Compliance following physicians PA counseling; prevalence of physicians’ PA counseling in the 12 previous months | Self-developed 2-item instrument Validity n.r. Paper-pencil survey. Self-report | BGS 98 representative sample n = 7124 Between 18 and 79 years | Nationwide; October 1997–March 1999 | n.r. | Chi-square test, t-test, logistic regression missing values: n.r. | Prevalence of physicians’ PA counseling: 6.85%, in patients ≥70: 0% Compliance: ca. 50%. Compliance higher in women, non-smokers, and healthy eaters | 5/10 |
| [21] | Attitude, perceived need of counseling, counseling received in family practice patients | Mentioning PA and health | Self-developed instrument, Tested and validated in a pilot study Validity n.r. | EUROPREVIEW-Study 8 n = 370 between 30 and 70 years | In and around the City of Cologne September 2008–September 2009 | Rate of consenting practices 66%. Rate of participation among patients 70% | 2-sided Chi- square test missing values: n.r. | PA and health mentioned in the previous 12 months: 39.4%. PA and health ever mentioned: 54.7% 31% patients would welcome more support and counseling on PA (vs. 57% in Europe) | 3/10 |
| [22] | Population study on chronic diseases | Prevalence of physicians’ PA counseling (sub-sample) | Self-developed instrument Validity n.r. | Life-Adult Study; n = 2244 between 19 and 79 years | Leipzig March 2012–May 2013 | 1171/2244 patients received health counseling, of those 482 received PA counseling | Chi-square test missing values: n.r. | 21.5% of all patients have received PA counseling | 3/10 |
| Physician Surveys | |||||||||
| Study | Primary Research Question | Secondary Research Question | Survey Instrument and Survey Mode | Sample | Place and Time of the Survey | Response Rate | Statistics, Dealing Missing Values | Main Results | Risk of Bias According to Hoy et al. |
| [23] | PA counseling by neurologists | Facilitators and barriers | Self-developed instrument with closed and open questions Validity n.r. Online survey | Members of the German Neurologist Association | Nationwide September 2015 | 169/784 (21.6%) | Cramer’s Index, Contingency table, OR, missing values n.r. | Prevalence of physicians’ PA counseling: 80.5% often, 13% occasionally, 77.5% provide general information, 66.9% detailed information regarding specific exercise forms. 82.2% consider individual and disease-specific circumstances, 69.2% would provide PA counseling more often and more in depth. Barrier: patients’ disinterest, physically active physicians provide counseling more often | 5/10 |
| [24] | PA counseling by family physicians for elderly patients Barriers to knowledge and skills Need and interest in training Perceived quality of a training | Self-developed 42 and 32 item instruments respectively Validity n.r. paper-pencil survey (per mail and in person) self-report | Family physicians n = 60 n = 22 | City of Würzburg and vicinity June–September 2015 | 60/291 20.62% (Counseling) 22/23 95% (Training) | Descriptive analysis | Approx. 50% of patients receive counseling Barriers: Lack of time, patients’ disinterest Physicians highly interested in training on PA counseling | 5/10 | |
| [25] | physicians’ knowledge and use of Exercise on Prescription, barriers to use | Self-developed instrument Validity n.r. Pre-test paper-pencil survey per mail Self-report | All general practitioners in two districts of Eastern Bavaria n = 2821 | Oberpfalz and Nieder-Bayern June–November 2013 | 923/2821 (32.7%) | Descriptive analysis | 26.4% know Exercise on Prescription, 70.1% of those do not use it Barriers: lack of information on Exercise on Prescription, local offers, lack of reimbursement of costs of courses | 8/10 | |
| [26] | Family physicians’ attitude to lifestyle counseling Barriers to lifestyle counseling | PA counseling. Significance of PA, skills and techniques to motivate patients | Self-developed instrument Validated via cognitive interviews Pre-tested in pilot study Validity n.r. Paper-pencil survey per mail and online survey Self-report Compensation of €20 for participation | ÄSP-kardio-Study 9 Representative sample of German family physicians, a priori defined sample of 13,294 | Nationwide; October 2011–March 2012 | 4074/13,294 (RR3 33.9%) | Descriptive analysis | 71.8% routinely provide PA counseling (i.e., to more than 50% of the patients) 100% of physicians judge PA to be important. 87% report good or very good knowledge, 48% report being successful in PA counseling | 8/10 |
| [27] | Regional differences in physicians’ (1) attitudes to lifestyle counseling, (2) lifestyle counseling, (3) perceived barriers to lifestyle counseling | Assessment of PA, PA counseling, monitoring | Self-developed instrumentValidated via cognitive interviews Pre-tested in pilot study Validity n.r. Paper-pencil survey per mail and online survey Self-report Compensation of €20 for participation | ÄSP-kardio-Study Representative sample of German family physicians, a priori defined sample of 13,294 | Nationwide; October 2011–March 2012 | 4074/13,294 (RR3 33.9%) | Chi-square test. Kruskal–Wallis test. Logistic regressions, missing values n.r. | Physicians in practices in rural regions provide assessment of PA, PA counseling, and monitoring less frequently than physicians in urban areas | 8/10 |
| [28] | Gender differences in lifestyle counseling | PA counseling | Self-developed instrument Validated via cognitive interviews Pre-tested in pilot study Validity n.r. Paper-pencil survey per mail and online survey Self-report Compensation of €20 for participation | ÄSP-kardio-Study Representative sample of German family physicians, a priori defined sample of 13,294 | Nationwide; October 2011–March 2012 | 4074/13,294 (RR3 33.9%) | Chi-square test. Mann–Whitney U test. Logistic regressions, missing values n.r. | Female physicians assess PA more often (OR 1.39) | 8/10 |
| [29] | Aspects of PA counseling (5 A) | Self-developed instrumentValidated via cognitive interviews Pre-tested in pilot study Validity n.r. Paper-pencil survey per mail and online survey Self-report Compensation of €20 for participation | ÄSP-kardio-Study Representative sample of German family physicians A priori defined sample of 13,294 | Nationwide; October 2011–March 2012 | 4074/13,294 (33.9%) | Chi-square test, logistic regressions, missing values n.r. | 80.7% assess and 81.3% recommends more PA 87.2% report high or very high competence, 52.3% rated their skills to motivate patients to increase PA as “not good”. Female physicians assess PA more often and provide counseling more often Physicians with a higher proportion of patients at risk for cardiovascular disease provide counseling more often | 8/10 | |
| [30] | Current state of lifestyle counseling in family practice in the Federal State of Baden-Württemberg. Facilitators and barriers to preventive offers | PA counseling | Self-developed instrument Pre-test Validity n.r. Paper-pencil survey per mail Self-report Expense allowance for participation | General practitioners in Baden-Württemberg randomly selected sample of n = 2000 | Baden-Württemberg May 2009 | 260/2000 (13%) | Chi-square test, logistic regressions, missing values n.r. | 70.1% assess PA always or often in new patients 54.9% assess and advise PA promotion is offered more often in larger cities and by physicians with high self-reported skill to motivate patients | 7/10 |
| [31] (quantitative study part) | State of primary prevention in general practitioners’ practices | PA counseling | Self-developed instrument Pre-test Validity n.r. Paper-pencil survey per mail Self-report | General practitioners in Berlin n = 1168 | Berlin November 2010–February 2011 | 474/1168/ (41%) | Descriptive analysis | Approx. 90% of physicians raise the issue of PA if it is indicated | 6/10 |
| [32] | Recommendations for preventive offers | Self-developed instrument Pre-test Validity n.r. Paper-pencil survey per mail Self-report | General practitioners in Berlin n = 1168 | Berlin November 2010–February 2011 | 474/1168 (41%) 98% of all items were fully answered | Descriptive analysis, Chi-square test | 77% of the physicians recommend offers of sports clubs and fitness studios | 6/10 | |
| Study Based on Patient Records | |||||||||
| Study | Primary Research Question | Secondary Research Question | Data Source | Sample | Place and Time of the Survey | Response Rate | Statistics, Dealing Missing Values | Main Results | Risk of Bias According to Hoy et al. |
| [33] | Health promotion, primary and secondary prevention on family practice | PA Counseling | Patient records in 10 family practices in Berlin with more than 1000 patients. Patient at least for three years in the practice | n = 500 | Berlin 1998 2000 | 25 practices invited, the first 10 to accept invitation were included | Chi-square test | In 107 (21.4%) patient records, PA counseling was recorded for 63 females vs. 44 males (significantly different) Elderly significantly more often than younger adults | 6/10 |
| Study | Primary Research Question | Secondary Research Question | Methods | Sample | Study Place and Time | Data Analysis | Main Results |
|---|---|---|---|---|---|---|---|
| [34] | Care of arthrosis patients in general practice, views of patients, general practitioners, and practice nurses | Non-drug therapy options for arthrosis patients | Semi-structured interviews with open questions (approx. 45 min.) in the practices | 20 general practitioners and 20 practice nurses | Place not reported 2004 | Recorded digitally, transcribed literally and analyzed by four different researchers with ATLAS.ti software categorized by four researchers independently | Almost all physicians report regularly mentioning muscle strengthening. Physicians tend to provide general advice. Self-assessed success rate in motivating patients was considered low. |
| [35] | General practitioners’ and patients’ practices and attitudes regarding overweight encountered during preventive counseling | PA in preventive counseling of overweight patients in general practice | Audiotaped preventive counseling | 70 general practitioners were invited, n = 12 accepted the invitation, invited n = 52 dialogues recorded | Berlin March–September 2007 | Recorded digitally, transcribed literally and analyzed by three different researchers with ATLAS.ti softwareQualitative content analysis according to Mayring | PA is the second most common topic in the counseling. |
| [36] | General practitioners’ and patients’ practices and attitudes regarding overweight encountered during preventive counseling | PA in preventive counseling of overweight patients in general practice | Audiotaped preventive counseling | 70 general practitioners were invited, n = 12 accepted invitation, invited n = 50 dialogues recorded | Berlin Time not reported | Recorded digitally, analysis according to the Roter Interaction Analysis System (RIAS), major themes: cardiovascular risk factors, diet, PA | PA seldom mentioned. |
| [37] | Obesity management of in general practice from patients’ views | PA as part of the obesity management in general practice | Semi-structured interviews | Overweight and obese patients (n = 15; 11 female) out of 52 potential patients | Berlin and Brandenburg | Recorded digitally, transcribed literally using the transcription software “f4” version 3.0.3. Qualitative content analysis according to Mayring Some of the interviews analyzed by two researchers independently | In individual cases a medical history of preferred exercise forms; concrete suggestions for physical activities; Frequent recommendations on the regularity and intensity of PA, with concrete advice on frequency or advice on integrating exercise into everyday life. |
| [38] | General practitioners’ understanding of prevention, especially as part of the counseling of obese and overweight patients | PA as part of the obesity management in general practice | Semi-structured interviews approx. 54 min in the practices | General practitioners (n = 15; 9 female), out of n = 78 invited | Berlin and Brandenburg 2006–2007 | Recorded digitally, transcribed literally using the transcription software “f4” version 3.0.3. Data analysis ATLAS.ti (Version 5.0) Qualitative content analysis according to Mayring One of the interviews analyzed by two researchers independently | Compared to nutrition, the topic of physical activity receives much less attention. Two physicians recommend patients to participate in cardio sport groups. If at all, physicians typically give general recommendations, recommendations for PA in everyday life, mentioning courses of the health insurance companies or own offers. In one counseling PA is not mentioned at all. |
| [39] | Exercise on Prescription within the campaign “Berlin on the move” (“Berlin komm(t) auf die Beine”) | Use and relevance of Exercise on Prescription, Benefits and barriers | Semi-structured expert interviews (discussion and pretest) 15–59 min, in th e practices | General practitioners (n = 7), who know the campaign “Berlin on the move”, n = 244 invited | Berlin September–October 2013 | Recorded digitally, transcribed literally using the transcription software “f4” version data analysis according to Meuser and Nagel | None of the physicians use the exercise on prescription in the intended sense; physicians attribute high to very high significance of routine PA counseling in both healthy and diseased patients, the perceived effectiveness of the counseling is either very high or very low. |
| Patient Surveys | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | External Validity | Internal Validity | Overall Score | ||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
| [15] | low | high | low | high | low | high | high | low | high | low | 5/10 |
| [16] | low | high | low | high | low | high | high | low | high | low | 5/10 |
| [17] | high | high | high | low | low | high | high | low | high | low | 4/10 |
| [18] | high | high | high | high | low | high | high | low | low | low | 4/10 |
| [19] | high | low | high | low | low | high | high | low | high | low | 5/10 |
| [20] | low | high | low | high | low | high | high | low | high | low | 5/10 |
| [21] | high | high | high | high | low | high | high | low | high | low | 3/10 |
| [22] | high | high | high | high | low | high | high | low | high | low | 3/10 |
| Physician Surveys | Overall Score | ||||||||||
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| [23] | high | low | low | high | low | high | high | low | high | low | 5/10 |
| [24] | high | low | low | high | low | high | high | low | high | low | 5/10 |
| [25] | low | low | low | low | low | high | high | low | low | low | 8/10 |
| [26] | low | low | low | low | low | high | high | low | low | low | 8/10 |
| [27] | low | low | low | low | low | high | high | low | low | low | 8/10 |
| [28] | low | low | low | low | low | high | high | low | low | low | 8/10 |
| [29] | low | low | low | low | low | high | high | low | low | low | 8/10 |
| [30] | high | low | low | low | low | high | high | low | low | low | 7/10 |
| [31] (quantitative part) | high | low | low | high | low | high | high | low | low | low | 6/10 |
| [32] | high | low | low | high | low | high | high | low | low | low | 6/10 |
| Study | Was There a Clear Statement of the Aims of the Research? | Is a Qualitative Methodology Appropriate? | Was the Research Design Appropriate to Address the Aims of the Research? | Was the Recruitment Strategy Appropriate to the Aims of the Research? | Was the Data Collected in a Way that Addressed the Research Issue? | Has the Relationship between Researcher and Participants Been Adequately Considered? | Have Ethical Issues Been Taken into Consideration? | Was the Data Analysis Sufficiently Rigorous? | Is There a Clear Statement of Findings? | How Valuable Is the Research? |
|---|---|---|---|---|---|---|---|---|---|---|
| [34] | yes | yes | cannot tell | Yes | yes | cannot tell | yes | yes | yes | yes |
| [35] | yes | yes | cannot tell | cannot tell | yes | cannot tell | cannot tell | yes | yes | yes |
| [36] | yes | yes | cannot tell | No | yes | cannot tell | yes | yes | cannot tell | yes |
| [37] | yes | yes | yes | cannot tell | yes | yes | yes | yes | yes | yes |
| [38] | yes | cannot tell | yes | Yes | yes | yes | yes | yes | yes | yes |
| [39] | yes | yes | yes | Yes | yes | yes | yes | yes | yes | yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Füzéki, E.; Weber, T.; Groneberg, D.A.; Banzer, W. Physical Activity Counseling in Primary Care in Germany—An Integrative Review. Int. J. Environ. Res. Public Health 2020, 17, 5625. https://doi.org/10.3390/ijerph17155625
Füzéki E, Weber T, Groneberg DA, Banzer W. Physical Activity Counseling in Primary Care in Germany—An Integrative Review. International Journal of Environmental Research and Public Health. 2020; 17(15):5625. https://doi.org/10.3390/ijerph17155625
Chicago/Turabian StyleFüzéki, Eszter, Theresa Weber, David A. Groneberg, and Winfried Banzer. 2020. "Physical Activity Counseling in Primary Care in Germany—An Integrative Review" International Journal of Environmental Research and Public Health 17, no. 15: 5625. https://doi.org/10.3390/ijerph17155625
APA StyleFüzéki, E., Weber, T., Groneberg, D. A., & Banzer, W. (2020). Physical Activity Counseling in Primary Care in Germany—An Integrative Review. International Journal of Environmental Research and Public Health, 17(15), 5625. https://doi.org/10.3390/ijerph17155625