Prioritizing Training Needs of School Health Staff: The Example of Vietnam

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Measures
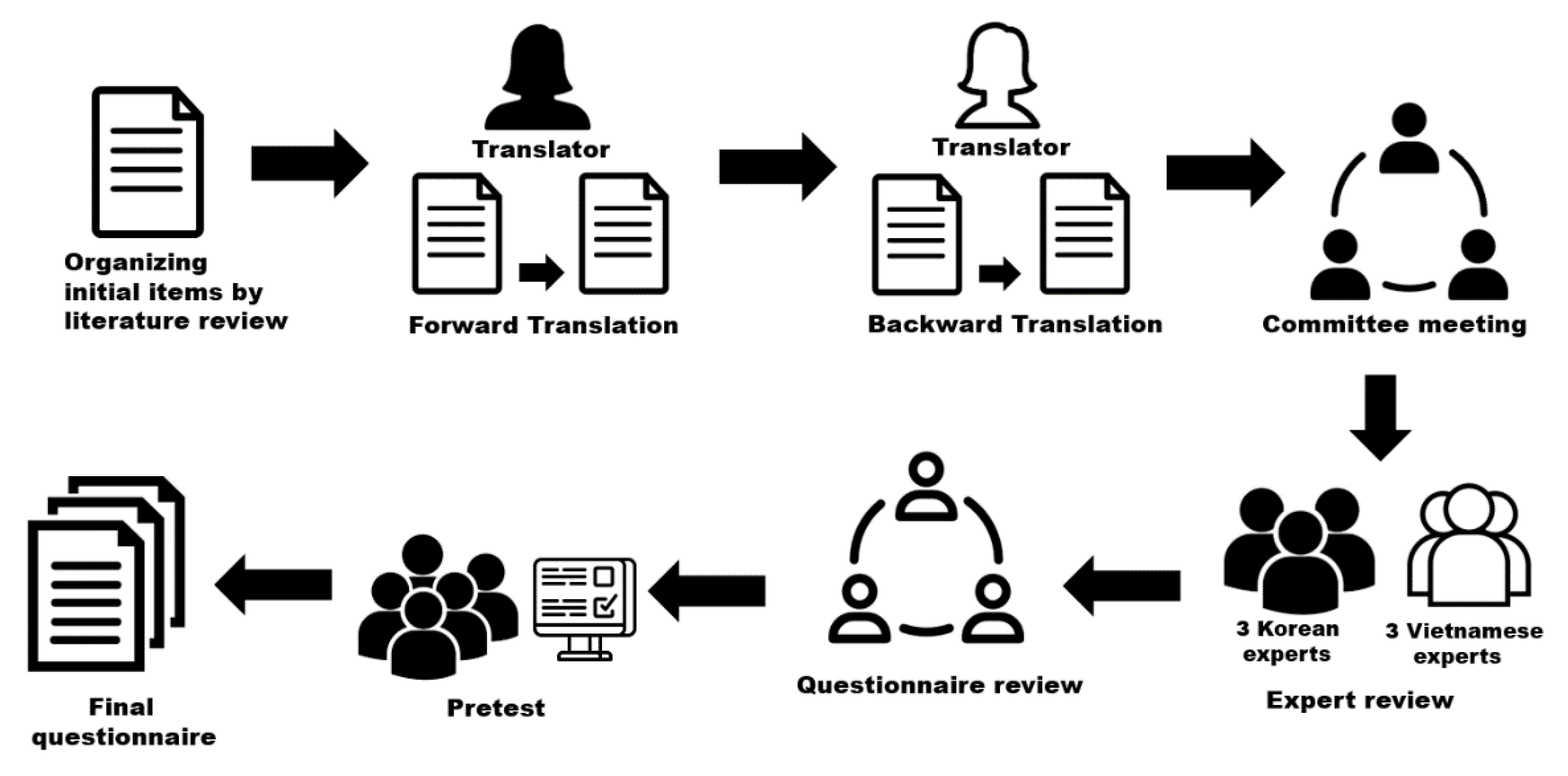
2.2.1. Organizing Initial Items
2.2.2. Back Translation
2.2.3. Expert Review Using a Content Validity Index
2.2.4. Pretest and Finalization
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Participants’ Characteristics and Differences in Performance
3.2. SHS members’ Training Needs
3.3. Consensus Regarding SHS Members’ Training Needs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moore, G.F.; Littlecott, H.J.; Fletcher, A.; Hewitt, G.; Murphy, S. Variations in schools’ commitment to health and implementation of health improvement activities: A cross-sectional study of secondary schools in Wales. BMC Public Health 2016, 16, 138. [Google Scholar] [CrossRef]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J. Youth risk behavior surveillance-United States, 2017. MMWR Surveill Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef]
- Jacob, C.M.; Baird, J.; Barker, M.; Cooper, C.; Hanson, M. The Importance of a Life-Course Approach to Health: Chronic Disease Risk from Preconception through Adolescence and Adulthood. Available online: https://www.who.int/life-course/publications/importance-of-life-course-approach-to-health/en/ (accessed on 9 June 2020).
- Faggiano, F.; Minozzi, S.; Versino, E.; Buscemi, D. Universal school-based prevention for illicit drug use. Cochrane Database Syst. Rev. 2014, 12, CD003020. [Google Scholar] [CrossRef]
- Walsh, K.; Zwi, K.; Woolfenden, S.; Shlonsky, A. School-based education programmes for the prevention of child sexual abuse. Cochrane Database Syst. Rev. 2015, 4, CD004380. [Google Scholar] [CrossRef] [PubMed]
- Das, J.; Holla, A.; Das, V.; Mohanan, M.; Tabak, D.; Chan, B. In urban and rural India, a standardized patient study showed low levels of provider training and huge quality gaps. Health Aff. 2012, 31, 2774–2784. [Google Scholar] [CrossRef] [PubMed]
- Baltag, V.; Pachyna, A.; Hall, J. Global overview of school health services: Data from 102 countries. Health Behav. Policy Rev. 2015, 2, 268–283. [Google Scholar] [CrossRef]
- Ministry of Health and Ministry of Education and Training, Vietnam. Join Circular: Regulations on School Health Work. Available online: https://thuvienphapluat.vn/van-ban/giao-duc/Thong-tu-13-2016-TTLT-BYT-BGDDT-huong-dan-thuc-hien-cong-tac-y-te-truong-hoc-295062.aspx (accessed on 3 March 2020).
- Yi, C.R.; Song, H.-D. DACUM job analysis on elementary health teachers’ roles. J. Korean Acad. Community Health Nurs. 2014, 25, 187–197. [Google Scholar] [CrossRef][Green Version]
- United Nations Educational, Scientific and Cultural Organization. Monitoring and Evaluation Guidance for School Health Programs. Appendices. Available online: https://hivhealthclearinghouse.unesco.org/sites/default/files/resources/FRESH_M%26E_Appendices.pdf (accessed on 3 March 2020).
- World Health Organization. Management of Substance Abuse—Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 9 June 2020).
- Lynn, M.R. Determination and quantification of content validity. Nurs.Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Borich, G.D. A needs assessment model for conducting follow-up studies. J. Teach. Edu. 1980, 31, 39–42. [Google Scholar] [CrossRef]
- Mink, O.; Shultz, J.; Mink, B. Developing and Managing Open Organizations: A Model and Method for Maximizing Organizational Potential; Somerset Consulting Group, Inc: Austin, TX, USA, 1991; pp. 13–20. [Google Scholar]
- Cho, D.Y. Exploring how to set priority in need analysis with survey. J. Res. Educ. 2009, 35, 165–187. [Google Scholar]
- Kim, Y.B.; Kim, H.K.; Kim, M. Developing strategies to improve efficiency of school health education in an outbreak of pandemic disease. Korean J. Health Edu. Promot. 2012, 29, 71–81. [Google Scholar]
- Ministry of Education, Korea. Manual for Prevention and Crisis Action of Infectious Disease. 2016. Available online: http://www.schoolhealth.kr/web/search/selectTotalSearchList.do?bbsId=&lstnum1=2589&pageIndex=1&pageUnit=10&sortOrder=&searchWrd=%ED%95%99%EC%83%9D+%EA%B0%90%EC%97%BC%EB%B3%91+%EC%98%88%EB%B0%A9 (accessed on 3 March 2020).
- Jun, E.; Lee, G. Elementary, middle, and high school health teachers’ countermeasures against an outbreak of pandemic diseases, including MERS. J. Korean Acad. Community Health Nurs. 2018, 29, 65–75. [Google Scholar] [CrossRef]
- Tuck, C.M.; Haynie, K.; Davis, C. Emergency Preparedness and Response in the School Setting – the Role of the School Nurse (NASN Position Statement, 2014). Available online: https://files.eric.ed.gov/fulltext/ED558439.pdf (accessed on 9 June 2020).
- Ugalde, M.R.; Guffey, D.; Minard, C.G.; Giardino, A.P.; Johnson, G.A. A survey of school nurse emergency preparedness 2014–2015. J. Sch. Nurs. 2018, 34, 398–408. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics Council on School Health. Role of the school nurse in providing school health services. Pediatrics 2016, 137, e20160852. [Google Scholar] [CrossRef] [PubMed]
- Do, T.T.H.; Correa-Velez, I.; Dunne, M.P. Trauma exposure and mental health problems among adults in Central Vietnam: A randomized cross-sectional survey. Front. Psychiatry 2019, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Selimbasic, Z.; Sinanovic, O.; Avdibegovic, E.; Brkic, M.; Hamidovic, J. Behavioral problems and emotional difficulties at children and early adolescents of the veterans of war with post-traumatic stress disorder. Med. Arch. (Sarajevo Bosnia Herzeg.) 2017, 71, 56–61. [Google Scholar] [CrossRef]
- Le, L.C.; Blum, R.W. Road traffic injury among young people in Vietnam: Evidence from two rounds of national adolescent health surveys, 2004–2009. Glob. Health Action 2013, 6, 18757. [Google Scholar] [CrossRef]
- Vostanis, P.; Maltby, J.; Duncan, C.; O’Reilly, M. Stakeholder perspectives on children’s mental health needs and supports in six low- and middle-income countries. Child. Soc. 2018, 32, 457–469. [Google Scholar] [CrossRef]
- Chandra-Mouli, V.; Patel, S.V. Mapping the knowledge and understanding of menarche, menstrual hygiene and menstrual health among adolescent girls in low- and middle-income countries. Reprod. Health 2017, 14, 30. [Google Scholar] [CrossRef]
- WHO and UNESCO. Global Standard for Health Promoting Schools. Available online: https://www.who.int/publications-detail/global-standards-for-health-promoting-schools (accessed on 30 January 2020).
- Hoying, J.; Melnyk, B.M.; Arcoleo, K. Effects of the COPE Cognitive Behavioral Skills Building TEEN Program on the healthy lifestyle behaviors and mental health of Appalachian early adolescents. J. Pediat. Health Care 2016, 30, 65–72. [Google Scholar] [CrossRef]
- Huong, L.T.T.; Long, T.K.; Anh, L.V.; Cook, M.; Capra, M. Decreasing in-home smoking of adults—Results from a school-based intervention program in Vietnam. AIMS Public Health 2016, 3, 863–879. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, H.S.; Şahin, F.N.; Maksimovic, N.; Drid, P.; Bianco, A. School-based intervention programs for preventing obesity and promoting physical activity and fitness: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 347. [Google Scholar] [CrossRef] [PubMed]
- Gaspard, J.; Yang, C.M. Training needs assessment of health care professionals in a developing country: The example of Saint Lucia. BMC Medical Educ. 2016, 16, 112. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Categories | Mean ± SD/n (%) | Performance Level | |
|---|---|---|---|---|
| Mean ± SD | T (p) | |||
| Age | 34.28 ± 6.76 | |||
| Gender | Male | 28 (13.7) | 3.73 ± 0.81 | 1.69 (0.092) |
| Female | 176 (86.3) | 3.43 ± 0.87 | ||
| Type of school health staff | Assistant doctor, Nurse | 92 (45.1) | 3.78 ± 0.64 | 5.06 (<0.001) |
| Other | 112 (54.9) | 3.21 ± 0.95 | ||
| Type of school | Primary | 114 (55.9) | 3.34 ± 0.93 | −2.59 (0.010) |
| Secondary | 90 (44.1) | 3.64 ± 0.76 | ||
| Place of residence | Urban | 32 (15.7) | 3.51 ± 0.87 | 0.33 (0.744) |
| Rural | 172 (84.3) | 3.46 ± 0.87 | ||
| Schools with minority students | Yes | 59 (28.9) | 3.45 ± 0.89 | −0.21 (0.837) |
| No | 145 (71.1) | 3.47 ± 0.86 | ||
| Type of health education provider | School health staff | 136 (66.7) | 3.69 ± 0.78 | 5.51 (<0.001) |
| Other | 68 (33.3) | 3.03 ± 0.88 | ||
| Regular health education at school | Yes | 186 (91.2) | 3.55 ± 0.83 | 4.08 (<0.001) |
| No | 18 (8.8) | 2.70 ± 0.90 | ||
| School health training within the past 2 years | Yes | 169 (82.8) | 3.55 ± 0.83 | 2.92 (0.004) |
| No | 35 (17.2) | 3.09 ± 0.98 | ||
| Item | Importance Mean ± SD | Performance Mean ± SD | t | Borich Needs Score | Rank |
|---|---|---|---|---|---|
| Domain 1. Providing emergency care | |||||
| 1. Carrying out health assessment | 4.56 ± 0.67 | 3.32 ± 1.20 | 14.63 *** | 5.68 | 4 |
| 2. Administering first aid | 4.71 ± 0.49 | 3.42 ± 1.12 | 16.32 *** | 6.10 | 2 |
| 3. Providing mental support | 4.37 ± 0.69 | 3.77 ± 0.94 | 8.26 *** | 2.61 | 52 |
| 4. Administering first-aid medicine | 4.40 ± 0.74 | 3.48 ± 1.18 | 10.41 *** | 4.08 | 23 |
| 5. Guiding self-healthcare | 4.36 ± 0.71 | 3.73 ± 0.96 | 8.21 *** | 2.78 | 49 |
| 6. Guiding follow-up management | 4.22 ± 0.77 | 3.65 ± 0.96 | 7.23 *** | 2.40 | 55 |
| 7. Making requests to medical institutions | 4.58 ± 0.61 | 4.00 ± 0.89 | 8.05 *** | 2.63 | 51 |
| 8. Building an emergency medical system | 4.47 ± 0.65 | 3.36 ± 1.08 | 14.15 *** | 4.95 | 11 |
| Domain 2. Providing health education | |||||
| 9. Establishing annual operation plans for health education curriculum | 4.35 ± 0.68 | 3.59 ± 1.00 | 10.22 *** | 3.28 | 38 |
| 10. Teaching students about health | 4.54 ± 0.61 | 3.62 ± 0.94 | 12.79 *** | 4.18 | 20 |
| 11. Teaching teachers about health | 4.36 ± 0.69 | 3.50 ± 1.00 | 10.71 *** | 3.78 | 28 |
| 12. Teaching parents about health | 4.26 ± 0.83 | 3.47 ± 1.02 | 8.70 *** | 3.40 | 37 |
| 13. Offering health information | 4.43 ± 0.65 | 3.54 ± 0.97 | 11.72 *** | 3.95 | 25 |
| 14. Providing broadcasting education | 4.20 ± 0.78 | 3.32 ± 1.12 | 10.34 *** | 3.66 | 30 |
| Domain 3. Operating the school health room | |||||
| 15.Establishing annual operation plans for health management | 4.37 ± 0.66 | 3.65 ± 1.01 | 10.22 *** | 3.17 | 40 |
| 16. Producing budgets | 4.38 ± 0.64 | 3.38 ± 1.06 | 12.38 *** | 4.38 | 17 |
| 17. Managing a daily record of health work | 4.35 ± 0.65 | 3.81 ± 0.96 | 7.67 *** | 2.35 | 56 |
| 18. Managing medicines | 4.55 ± 0.62 | 3.73 ± 1.06 | 10.60 *** | 3.75 | 29 |
| 19. Managing medical instruments | 4.44 ± 0.66 | 3.77 ± 1.05 | 8.69 *** | 2.96 | 45 |
| 20. Taking care of official documents | 4.20 ± 0.76 | 3.78 ± 0.93 | 5.68 *** | 1.73 | 58 |
| 21. Obtaining necessary or suggested items | 4.24 ± 0.74 | 3.42 ± 1.05 | 9.84 *** | 3.47 | 34 |
| 22. Managing other related documents | 3.88 ± 0.85 | 3.48 ± 0.96 | 5.08 *** | 1.54 | 59 |
| Domain 4. Implementing health screening for students | |||||
| 23. Investigating health conditions | 4.53 ± 0.66 | 3.41 ± 1.11 | 13.14 *** | 5.09 | 9 |
| 24. Implementing health screening | 4.48 ± 0.67 | 3.11 ± 1.19 | 14.76 *** | 6.13 | 1 |
| 25. Managing children requiring protection | 4.39 ± 0.68 | 3.46 ± 1.03 | 11.64 *** | 4.09 | 21 |
| 26. Providing aftercare based on results | 4.20 ± 0.86 | 3.13 ± 1.14 | 12.06 *** | 4.47 | 14 |
| 27. Managing record of results | 4.23 ± 0.85 | 3.38 ± 1.07 | 10.13 *** | 3.61 | 31 |
| 28. Using statistical results | 4.21 ± 0.86 | 3.36 ± 1.08 | 9.52 *** | 3.57 | 32 |
| Domain 5. Controlling infectious diseases | |||||
| 29. Building a system of infectious disease control | 4.57 ± 0.62 | 3.30 ± 1.16 | 14.76 *** | 5.80 | 3 |
| 30. Monitoring infectious diseases | 4.61 ± 0.58 | 3.39 ± 1.19 | 14.40 *** | 5.65 | 5 |
| 31. Providing preventive education on infectious disease | 4.65 ± 0.54 | 3.56 ± 1.10 | 13.77 *** | 5.06 | 10 |
| 32. Managing infected students | 4.62 ± 0.59 | 3.44 ± 1.13 | 14.30 *** | 5.46 | 6 |
| 33. Checking for necessary vaccinations | 4.34 ± 0.79 | 3.24 ± 1.21 | 12.26 *** | 4.77 | 13 |
| 34. Monitoring epidemiologically infectious environments | 4.44 ± 0.70 | 3.26 ± 1.13 | 13.83 *** | 5.22 | 7 |
| Domain 6. Establishing a healthy and safe physical environment | |||||
| 35. Assessing and managing available latrines for boys and girls | 4.36 ± 0.71 | 3.73 ± 0.91 | 9.09 *** | 2.78 | 50 |
| 36. Assessing and managing safe drinking water | 4.63 ± 0.58 | 3.75 ± 0.98 | 12.01 *** | 4.09 | 22 |
| 37. Assessing and managing available hand washing facilities | 4.35 ± 0.68 | 3.81 ± 0.91 | 7.42 *** | 2.35 | 57 |
| 38. Assessing and managing well-constructed and maintained learning areas and spaces | 4.23 ± 0.75 | 3.65 ± 0.91 | 8.40 *** | 2.47 | 54 |
| 39. Assessing and managing garbage removal from school grounds | 4.49 ± 0.66 | 3.85 ± 0.86 | 9.36 *** | 2.88 | 46 |
| 40. Protecting children from danger from road traffic, animals, and fire | 4.54 ± 0.75 | 3.57 ± 1.01 | 12.93 *** | 4.38 | 16 |
| 41. Assessing and managing endocrine disrupting chemicals (e.g., plastics, pesticides, detergent, Styrofoam, batteries) | 4.23 ± 0.87 | 3.28 ± 1.13 | 11.03 *** | 4.02 | 24 |
| Domain 7. Providing health counseling | |||||
| 42. Teaching putting healthy lifestyle habits into practice | 4.35 ± 0.74 | 3.64 ± 0.95 | 9.11 *** | 3.07 | 43 |
| 43. Providing health information to satisfy counseling needs | 4.23 ± 0.74 | 3.55 ± 0.95 | 9.25 *** | 2.88 | 47 |
| 44. Counseling students about health | 4.36 ± 0.69 | 3.64 ± 0.97 | 9.64 *** | 3.14 | 42 |
| 45. Providing counseling to students with health problems | 4.39 ± 0.71 | 3.58 ± 0.98 | 10.67 *** | 3.55 | 33 |
| 46. Guiding student with their family on health problems | 4.34 ± 0.72 | 3.46 ± 1.05 | 10.82 *** | 3.85 | 26 |
| 47. Providing counseling to students with mental or psychological trauma | 4.38 ± 0.74 | 3.27 ± 1.14 | 12.61 *** | 4.85 | 12 |
| 48. Making requests to related institution | 4.49 ± 0.66 | 3.73 ± 0.93 | 11.12 *** | 3.41 | 36 |
| Domain 8. Implementing health promotion programs | |||||
| 49. Understanding needs | 4.18 ± 0.74 | 3.41 ± 1.03 | 10.27 *** | 3.22 | 39 |
| 50. Setting order of priority | 4.07 ± 0.81 | 3.46 ± 0.98 | 8.39 *** | 2.49 | 53 |
| 51. Planning health promotion programs | 4.14 ± 0.75 | 3.42 ± 1.04 | 10.53 *** | 2.98 | 44 |
| 52. Utilizing human and material resources | 4.08 ± 0.78 | 3.38 ± 0.98 | 9.15 *** | 2.88 | 48 |
| 53. Running health promotion programs | 3.94 ± 0.83 | 3.13 ± 1.12 | 9.60 *** | 3.17 | 41 |
| 54. Evaluating results | 4.27 ± 0.71 | 3.39 ± 1.00 | 11.50 *** | 3.79 | 27 |
| Domain 9. Developing professionalism | |||||
| 55. Receiving teacher training | 4.36 ± 0.74 | 3.18 ± 1.16 | 13.73 *** | 5.15 | 8 |
| 56. Searching for the latest medical information | 4.34 ± 0.72 | 3.32 ± 1.11 | 12.67 *** | 4.43 | 15 |
| 57. Searching for the latest teaching materials | 4.28 ± 0.74 | 3.29 ± 1.12 | 12.26 *** | 4.24 | 18 |
| 58. Developing health education materials | 4.19 ± 0.82 | 3.19 ± 1.09 | 11.67 *** | 4.19 | 19 |
| 59. Participating in job-related organization | 4.16 ± 0.79 | 3.33 ± 1.09 | 10.51 *** | 3.47 | 35 |
| Total | 4.35 ± 0.50 | 3.48 ± 0.86 | 13.65 *** | 3.79 | |
| Domain | Item | Rank(Borich Needs Assessment) | Quadrant(Locus for Focus Model) | High Priority |
|---|---|---|---|---|
| 4 | 24. Implementing health screening | 1 | Ⅰ | O |
| 1 | 2. Administering first aid | 2 | Ⅰ | O |
| 5 | 29. Building a system of infectious disease control | 3 | Ⅰ | O |
| 1 | 1. Carrying out health assessment | 4 | Ⅰ | O |
| 5 | 30. Monitoring infectious diseases | 5 | Ⅰ | O |
| 5 | 32. Managing infected students | 6 | Ⅰ | O |
| 5 | 34. Monitoring epidemiologically infectious environments | 7 | Ⅰ | O |
| 9 | 55. Receiving teacher training | 8 | Ⅰ | O |
| 4 | 23. Investigating health conditions | 9 | Ⅰ | O |
| 5 | 31. Providing preventive education on infectious disease | 10 | Ⅰ | O |
| 1 | 8. Building an emergency medical system | 11 | Ⅰ | O |
| 7 | 47. Providing counseling to students with mental or psychological trauma | 12 | Ⅰ | O |
| 5 | 33. Checking for necessary vaccinations | 13 | Ⅱ | |
| 4 | 26. Providing aftercare based on results | 14 | Ⅱ | |
| 9 | 56. Searching for the latest medical information | 15 | II | |
| 6 | 40. Protecting children from danger from road traffic, animals, and fire | 16 | Ⅰ | O |
| 3 | 16. Producing budgets | 17 | Ⅰ | O |
| 9 | 57. Searching for the latest teaching materials | 18 | II | |
| 9 | 58. Developing health education materials | 19 | II | |
| 2 | 10. Teaching students about health | 20 | Ⅰ | |
| 4 | 25. Managing children requiring protection | 21 | Ⅰ | |
| 6 | 36. Assessing and managing safe drinking water | 22 | Ⅰ | |
| 1 | 4. Administering first-aid medicine | 23 | Ⅰ | |
| 2 | 13. Offering health information | 25 | Ⅰ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Lee, H.; Lee, H.; Loan, B.T.T.; Huyen, L.T.T.; Huong, N.T.T. Prioritizing Training Needs of School Health Staff: The Example of Vietnam. Int. J. Environ. Res. Public Health 2020, 17, 5563. https://doi.org/10.3390/ijerph17155563
Kim S, Lee H, Lee H, Loan BTT, Huyen LTT, Huong NTT. Prioritizing Training Needs of School Health Staff: The Example of Vietnam. International Journal of Environmental Research and Public Health. 2020; 17(15):5563. https://doi.org/10.3390/ijerph17155563
Chicago/Turabian StyleKim, Sookyung, Hyeonkyeong Lee, Hyeyeon Lee, Bui Thi Thanh Loan, Le Thi Thanh Huyen, and Nguyen Thi Thanh Huong. 2020. "Prioritizing Training Needs of School Health Staff: The Example of Vietnam" International Journal of Environmental Research and Public Health 17, no. 15: 5563. https://doi.org/10.3390/ijerph17155563
APA StyleKim, S., Lee, H., Lee, H., Loan, B. T. T., Huyen, L. T. T., & Huong, N. T. T. (2020). Prioritizing Training Needs of School Health Staff: The Example of Vietnam. International Journal of Environmental Research and Public Health, 17(15), 5563. https://doi.org/10.3390/ijerph17155563