Smokers’ and Nonsmokers’ Receptivity to Smoke-Free Policies and Pro- and Anti-Policy Messaging in Armenia and Georgia

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ongoing Study Overview
2.2. Data Collection
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Participant Characteristics
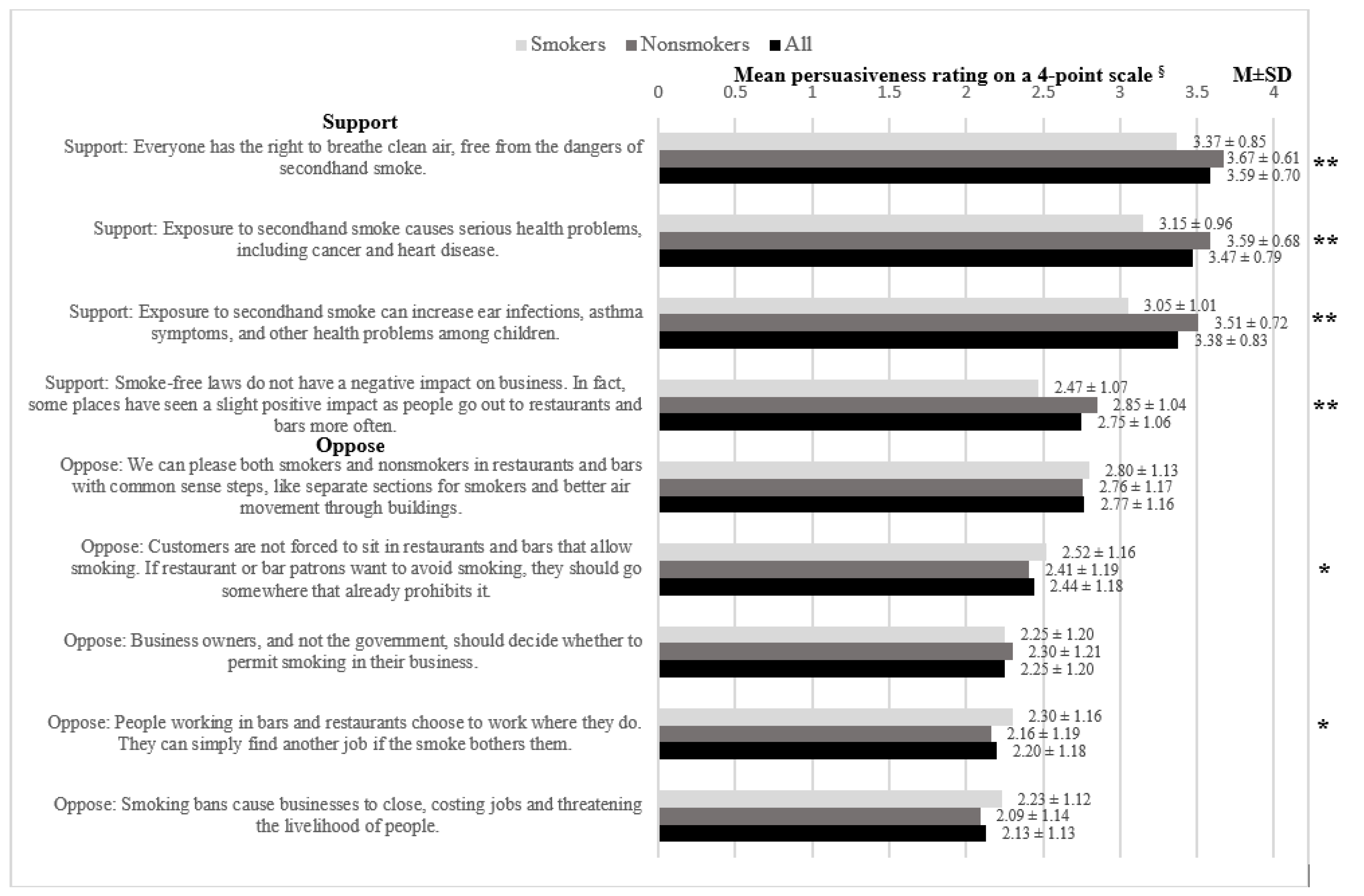
3.2. Persuasiveness of Messaging Strategies
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Report on the Global Tobacco Epidemic 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Roberts, B.; Anna, G.; Andrew, S.; David, R.; Vladimir, P.; Christian, H.; Martin, M. Changes in smoking prevalence in 8 countries of the former Soviet Union between 2001 and 2010. Am. J. Public Health 2012, 102, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevalence of Tobacco Smoking. 2015. Available online: http://gamapserver.who.int/gho/interactive_charts/tobacco/use/atlas.html (accessed on 23 August 2016).
- Movsisyan, N.; Petrosyan, D.; Petrosyan, V. Monitoring compliance with smoke-free legislation to advance the FCTC implementation in Armenia. In Proceedings of the 15th World Conference on Tobacco or Health, Singapore, 20–24 March 2012. [Google Scholar]
- Berg, C.J.; Topuridze, M.; Maglakelidze, N.; Sturua, L.; Shishniashvili, M.; Kegler, M.C. Reactions to smoke-free public policies and smoke-free home policies in the Republic of Georgia: Results from a 2014 national survey. Int. J. Public Health 2016, 61, 409–416. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. ARMENIA STEPS Survey 2016–2017: Fact Sheet. 2017. Available online: https://nih.am/assets/pdf/researches/00380987c602e3895652446d141f5d7b.pdf (accessed on 10 January 2020).
- World Health Organization. Heated Tobacco Products (HTPs) Market Monitoring Information Sheet 2018, July. Available online: File:///T:/bsheprojs/CJ%20Berg/CJB%20Personal%208%2020%2016/Israel/WHO-NMH-PND-18.7-eng.pdf (accessed on 6 January 2020).
- World Health Organization. Global Youth Tobacco Survey: Georgia, 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Centers for Disease Control and Prevention. The Guide to Community Preventive Services. 2012. Available online: http://www.thecommunityguide.org/index.html (accessed on 10 February 2020).
- Movsisyan, N.; Petrosyan, V. Analytical Review of the Tobacco Control Policy in Armenia 2005–2007; Center for Health Services Research and Development: Yerevan, Armenia, 2008. [Google Scholar]
- Flynn, B.S.; Goldstein, A.O.; Solomon, L.J.; Bauman, K.E.; Gottlieb, N.H.; Cohen, J.E.; Munger, M.C.; Dana, G.S. Predictors of state legislators’ intentions to vote for cigarette tax increases. Prev. Med. 1998, 27, 157–165. [Google Scholar] [CrossRef]
- Dearing, J.W.; Rogers, E.M. Agenda-Setting; Sage Publications: Thousand Oaks, CA, USA, 1996. [Google Scholar]
- Levy, D.T.; Chaloupka, F.; Gitchell, J. The effects of tobacco control policies on smoking rates: A tobacco control scorecard. J. Public Health Manag. Pract. 2004, 10, 338–353. [Google Scholar] [CrossRef]
- Niederdeppe, J.; Farrelly, M.C.; Wenter, D. Media advocacy, tobacco control policy change and teen smoking in Florida. Tob. Control 2007, 16, 47–52. [Google Scholar] [CrossRef]
- Kowitt, S.D.; Goldstein, A.O.; Schmidt, A.M.; Hall, M.G.; Brewer, N.T. Attitudes toward FDA Regulation of Newly Deemed Tobacco Products. Tob. Regul. Sci. 2017, 3, 504–515. [Google Scholar] [CrossRef]
- Thrasher, J.F.; Huang, L.; Pérez-Hernández, R.; Niederdeppe, J.; Arillo-Santillán, E.; Alday, J. Evaluation of a social marketing campaign to support Mexico City’s comprehensive smoke-free law. Am. J. Public Health 2011, 101, 328–335. [Google Scholar] [CrossRef]
- U.S. National Cancer Institute. A Socioecological Approach to Addressing Tobacco-Related Health Disparities. National Cancer Institute Tobacco Control Monograph 22. NIH Publication No. 17-CA-8035A; U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 2017.
- Champagne, B.M.; Sebrie, E.; Schoj, V. The role of organized civil society in tobacco control in Latin America and the Caribbean. Salud Publica De Mexico 2010, 52, S330–S339. [Google Scholar] [CrossRef]
- Spicer, N.; Harmer, A.; Aleshkina, J.; Bogdan, D.; Chkhatarashvili, K.; Murzalieva, G.; Rukhadze, N.; Samiev, A.; Walt, G. Circus monkeys or change agents? Civil society advocacy for HIV/AIDS in adverse policy environments. Soc. Sci. Med. 2011, 73, 1748–1755. [Google Scholar] [CrossRef]
- Robert Wood Johnson Foundation; The Mellman Group Inc. Smoke-Free Laws: Overview of Public Opinion and Effective Messages; The Mellman Group Inc.: Washington, DC, USA, 2011. [Google Scholar]
- The Mellman Group Inc. Using the Tobacco Settlement for Prevention: Overview of Public Opinion and Effective Messages; The Mellman Group Inc.: Washington, DC, USA, 2006. [Google Scholar]
- Berg, C.J.; Ribisl, M.K.; Thrasher, J.F.; Haardörfer, R.; O’Connor, J.; Kegler, M.C. Reactions to Cigarette Taxes and Related Messaging: Is the South Different? Am. J. Health Behav. 2015, 39, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.J.; Thrasher, J.F.; O’Connor, J.; Haardörfer, R.; Kegler, M.C. Reactions to Smoke-free Policies and Messaging Strategies in Support and Opposition: A Comparison of Southerners versus non-Southerners in the U.S. Health Behav. Policy Rev. 2015, 2, 408–420. [Google Scholar] [CrossRef]
- Kumar, S. The Armenian People and Armenian Culture. WorldAtlas 2019. Available online: https://www.worldatlas.com/articles/the-armenian-people-cultures-of-the-world.html (accessed on 30 July 2020).
- Sen Nag, O. The Culture of Georgia. WorldAtlas 2019. Available online: https://www.worldatlas.com/articles/the-culture-of-georgia.html (accessed on 30 July 2020).
- Berg, C.J.; Smith, S.A.; Bascombe, T.M.; Maglakelidze, N.; Starua, L.; Topuridze, M. Smoke-Free Public Policies and Voluntary Policies in Personal Settings in Tbilisi, Georgia: A Qualitative Study. Int. J. Environ. Res. Public Health 2016, 13, 156. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.J.; Dekanosidze, A.; Torosyan, A.; Grigoryan, L.; Sargsyan, Z.; Hayrumyan, V.; Topuridze, M.; Sturua, L.; Harutyunyan, A.; Kvachantiradze, L.; et al. Examining smoke-free coalitions in Armenia and Georgia: Baseline community capacity. Health Educ. Res. 2019, 34, 495–504. [Google Scholar] [CrossRef]
- Kish, L. A procedure for objective respondent selection within the household. J. Am. Stat. Assoc. 1949, 247, 380–387. [Google Scholar] [CrossRef]
- Schmidt, A.M.; Ranney, L.M.; Goldstein, A.O. Communicating program outcomes to encourage policymaker support for evidence-based state tobacco control. Int. J. Environ. Res. Public Health 2014, 11, 12562–12574. [Google Scholar] [CrossRef]
- Flynn, B.S.; Dana, G.S.; Goldstein, A.O.; Bauman, K.E.; Cohen, J.E.; Gottlieb, N.H.; Solomon, L.J.; Munger, M.C. State legislators’ intentions to vote and subsequent votes on tobacco control legislation. Health Psychol. 1997, 16, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Thrasher, J.; Kim, S.-H.; Rose, I.; Craft, M.-K. Media coverage of smoke-free policies after their innovation. J. Health Commun. 2015, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Songer, D.; Dillon, S.; Kite, D. The influence of issues on choice of voting cues utilized by state legislators. West. Political Q. 1986, 39, 118–125. [Google Scholar]
- Hahn, E.J.; Toumey, C.P.; Rayens, M.K.; McCoy, M.C. Kentucky legislators’ views on tobacco policy. Am. J. Prev. Med. 1999, 16, 81–88. [Google Scholar] [CrossRef]
- Ministry of Economy of the Republic of Armenia. Cooperation of “Philip Morris Armenia” Company with YSU and NPUA has Launched. 2017. Available online: https://www.mineconomy.am/en/news/808?fbclid=IwAR0xPDmoKQAeSaa6xoXGk5vtrslHENXOdWepown5hL7X5WUTEL1HLysVAZM (accessed on 31 January 2020).
- Bakhturidze, G.; Peikrishvili, N.; Mittelmark, M. The influence of public opinion on tobacco control policy-making in Georgia: Perspectives of governmental and non-governmental stakeholders. Tob. Prev. Cessat. 2016. [Google Scholar] [CrossRef][Green Version]
- Getachew, B.; Payne, J.B.; Vu, M.; Pillai, D.; Shah, J.; Levine, H.; Berg, C.J. Perceptions of alternative tobacco products, anti-tobacco media, and tobacco regulation among young adults: A qualitative study. Am. J. Health Behav. 2018, 42, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.J.; Bar-Zeev, Y.; Levine, H. Informing IQOS regulations in the United States: A synthesis of what we know. Sage Open 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.; Caciappo, J. Communication and Persuasion: Central and Peripheral Routes to Attitude Change; Springer: New York, NY, USA, 1986. [Google Scholar]



{kind=link}
{kind=link}
| Variable | All Participants, N = 1456 n (%) or M (SD) | Nonsmokers, n = 1058 (72.7%) n (%) or M (SD) | Smokers, n = 398 (27.3%) n (%) or M (SD) | p |
|---|---|---|---|---|
| Country, N (%) | <0.001 | |||
| Armenia | 705 (48.4) | 561 (53.0) | 144 (36.2) | |
| Georgia | 751 (51.6) | 497 (47.0) | 254 (63.8) | |
| Sociodemographics | ||||
| Age, M (SD) | 43.35 (13.49) | 43.34 (13.59) | 43.38 (13.26) | 0.957 |
| Sex, N (%) | <0.001 | |||
| Male | 575 (39.5) | 207 (19.6) | 368 (92.5) | |
| Female | 881 (60.5) | 851 (80.4) | 30 (7.5) | |
| Education, N (%) | 0.027 | |||
| Less than high school | 223 (15.3) | 157 (14.8) | 66 (16.6) | |
| High school | 260 (17.9) | 175 (16.5) | 85 (21.4) | |
| Vocational school | 407 (28.0) | 307 (29.0) | 100 (25.1) | |
| Some college | 98 (6.7) | 64 (6.0) | 34 (8.5) | |
| College degree or more | 468 (32.1) | 355 (33.6) | 113 (38.4) | |
| Employment, N (%) | <0.001 | |||
| Employed | 713 (49.0) | 438 (41.4) | 275 (69.1) | |
| Unemployed/other | 743 (51.0) | 620 (58.6) | 123 (30.9) | |
| Income per month, N (%) | 0.111 | |||
| ≤500 GEL/100,000 AMD | 563 (45.1) | 423 (47.7) | 140 (42.3) | |
| >500 GEL/100,000 AMD | 685 (54.9) | 463 (52.3) | 191 (57.7) | |
| Marital status, N (%) | 0.050 | |||
| Married/cohabitating | 1061 (72.9) | 784 (74.1) | 277 (69.6) | |
| Other | 395 (27.1) | 274 (25.9) | 121 (30.4) | |
| Children under 18 in the home, N (%) | 0.097 | |||
| No | 702 (49.0) | 497 (47.9) | 205 (51.9) | |
| Yes | 731 (51.0) | 541 (52.1) | 190 (48.1) | |
| Smoking characteristics | ||||
| Former smoker, N (%) | - | |||
| No | - | 956 (90.4) | - | |
| Yes | - | 102 (9.6) | - | |
| Number of days smoked, past 30, N (%) | - | |||
| Every day | - | - | 350 (87.9) | |
| Some days | - | - | 48 (12.1) | |
| CPD, M (SD) | - | - | 21.27 (10.79) | - |
| Readiness to quit, next 6 months, N (%) | - | |||
| No | - | - | 242 (83.4) | |
| Yes | - | - | 48 (16.6) | |
| Lifetime quit attempt, N (%) | - | |||
| No | - | - | 166 (43.7) | |
| Yes | - | - | 214 (56.3) | |
| Importance of quitting, M (SD) | - | - | 5.74 (3.23) | - |
| Confidence in quitting, M (SD) | - | - | 4.79 (3.18) | - |
| Support for bans index scores, M (SD) | ||||
| Cigarettes | 4.20 (0.66) | 4.38 (0.56) | 3.72 (0.66) | <0.001 |
| ENDS/HTPs | 4.24 (0.92) | 4.34 (0.89) | 3.99 (0.94) | <0.001 |
| Both | 4.21 (0.63) | 4.37 (0.56) | 3.80 (0.65) | <0.001 |
| Messaging persuasiveness index scores, M (SD) | ||||
| Support | 3.30 (0.66) | 3.41 (0.57) | 3.01 (0.79) | <0.001 |
| Opposition | 2.36 (0.94) | 2.33 (0.93) | 2.43 (0.94) | 0.081 |
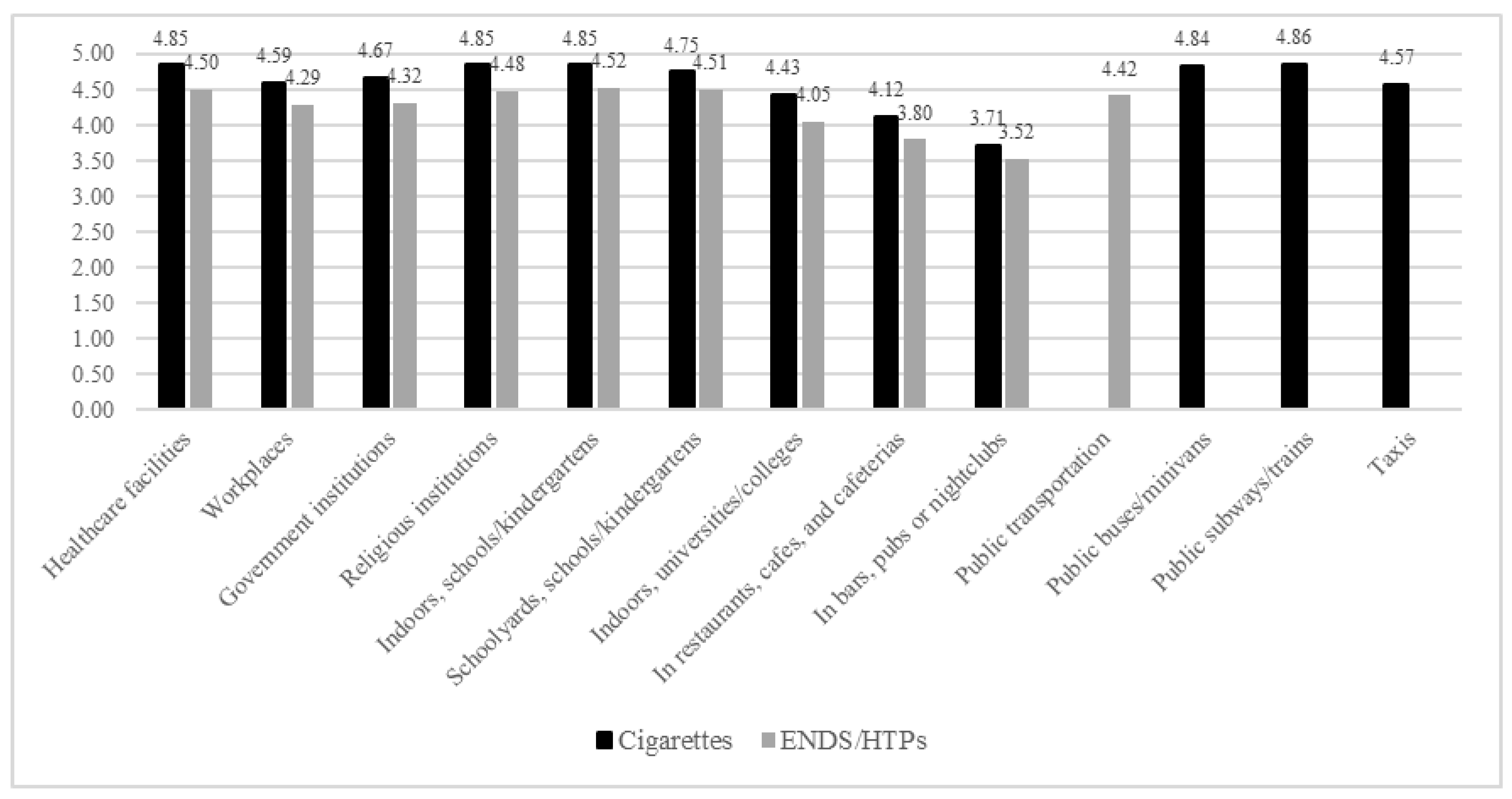
| Cigarettes | All, N = 1456 | Nonsmokers, n = 1058 | Smokers, n = 398 | p | Georgia, n = 751 | Armenia, n = 705 | p |
|---|---|---|---|---|---|---|---|
| Healthcare facilities | 4.85 (0.62) | 4.89 (0.54) | 4.74 (0.78) | <0.001 | 4.89 (0.46) * | 4.81 (0.76) * | 0.019 |
| Workplaces | 4.59 (0.90) | 4.76 (0.66) | 4.11 (1.23) | <0.001 | 4.57 (0.91) ** | 4.60 (0.90) ** | 0.595 |
| Government institutions | 4.67 (0.78) | 4.79 (0.61) | 4.34 (1.03) | <0.001 | 4.66 (0.75) ** | 4.68 (0.81) ** | 0.612 |
| Religious institutions | 4.85 (0.60) | 4.88 (0.53) | 4.77 (0.75) | 0.002 | 4.93 (0.35) ** | 4.77 (0.77) ** | <0.001 |
| Indoor areas of schools, kindergartens | 4.85 (0.60) | 4.88 (0.55) | 4.79 (0.71) | 0.018 | 4.86 (0.49) * | 4.85 (0.69) * | 0.772 |
| Schoolyards of schools, kindergartens | 4.75 (0.78) | 4.77 (0.73) | 4.66 (0.89) | 0.015 | 4.87 (0.44) * | 4.60 (1.00) *** | <0.001 |
| Indoor areas of universities, institutes, colleges | 4.43 (1.14) | 4.56 (1.02) | 4.09 (1.36) | <0.001 | 4.07 (1.33) * | 4.81 (0.73) * | <0.001 |
| In outdoor areas of university, college campuses | 4.42 (1.09) | 4.46 (1.05) | 4.32 (1.21) | 0.025 | 4.82 (0.53) * | 4.00 (1.35) *** | <0.001 |
| In restaurants, cafes, cafeterias | 4.12 (1.30) | 4.41 (1.04) | 3.34 (1.55) | <0.001 | 4.17 (1.27) * | 4.05 (1.32) *** | 0.075 |
| Outdoor terrace of restaurants, cafes, cafeterias | 2.98 (1.60) | 3.35 (1.53) | 2.01 (1.35) | <0.001 | 2.78 (1.63) *** | 3.19 (1.54) *** | <0.001 |
| In bars, pubs, or nightclubs | 3.71 (1.48) | 4.02 (1.31) | 2.90 (1.48) | <0.001 | 3.85 (1.43) * | 3.57 (1.52) *** | <0.001 |
| Outdoor terrace of bars, pubs, nightclubs | 2.88 (1.60) | 3.23 (1.54) | 1.94 (1.32) | <0.001 | 2.72 (1.63) *** | 3.04 (1.54) *** | <0.001 |
| Indoor common areas of apts, condos | 3.99 (1.38) | 4.30 (1.16) | 3.16 (1.56) | <0.001 | 3.98 (1.33) * | 4.00 (1.43) *** | 0.783 |
| Outdoor common areas of apts, condos | 3.76 (1.43) | 4.06 (1.24) | 2.96 (1.57) | <0.001 | 3.74 (1.43) *** | 3.77 (1.42) *** | 0.697 |
| Within individual apt/condo units | 3.79 (1.47) | 4.10 (1.27) | 3.00 (1.64) | <0.001 | 3.63 (1.52) *** | 3.96 (1.39) *** | <0.001 |
| Public bus or minivan stops | 4.10 (1.29) | 4.30 (1.12) | 3.58 (1.54) | <0.001 | 4.03 (1.32) *** | 4.18 (1.25) *** | 0.023 |
| In public buses, minivans | 4.84 (0.62) | 4.88 (0.54) | 4.73 (0.78) | <0.001 | 4.85 (0.49) * | 4.82 (0.73) * | 0.367 |
| Public subway, train stations | 4.53 (0.96) | 4.62 (0.85) | 4.29 (1.19) | <0.001 | 4.62 (0.84) * | 4.44 (1.08) * | <0.001 |
| In public subways, trains | 4.86 (0.60) | 4.89 (0.53) | 4.77 (0.75) | 0.001 | 4.88 (0.45) * | 4.83 (0.73) * | 0.142 |
| Taxis | 4.57 (1.01) | 4.77 (0.72) | 4.05 (1.40) | <0.001 | 4.37 (1.15) *** | 4.79 (0.78) *** | <0.001 |
| Within 5 m public building entrances | 3.33 (1.50) | 3.62 (1.41) | 2.56 (1.48) | <0.001 | 3.45 (1.39) *** | 3.20 (1.61) *** | 0.002 |
| Private vehicles with children <18 | 4.75 (0.72) | 4.83 (0.62) | 4.55 (0.93) | <0.001 | 4.70 (0.68) *** | 4.81 (0.77) *** | 0.004 |
| Playgrounds | 4.37 (1.10) | 4.55 (0.88) | 3.89 (1.43) | <0.001 | 4.21 (1.18) ** | 4.54 (0.98) *** | <0.001 |
| Parks, beaches | 3.53 (1.47) | 3.83 (1.35) | 2.73 (1.49) | <0.001 | 3.21 (1.48) *** | 3.88 (1.39) *** | <0.001 |
| Other public outdoor areas (e.g., open stadiums) | 3.41 (1.56) | 3.72 (1.43) | 2.59 (1.58) | <0.001 | 3.00 (1.61) *** | 3.84 (1.38) *** | <0.001 |
| ENDS/HTPs | |||||||
| Healthcare facilities | 4.50 (1.03) | 4.53 (0.99) | 4.42 (1.11) | 0.077 | 4.49 (0.97) * | 4.51 (1.09) *** | 0.737 |
| Workplaces | 4.29 (1.13) | 4.37 (1.07) | 4.09 (1.26) | <0.001 | 4.29 (1.09) * | 4.30 (1.19) *** | 0.860 |
| Government institutions | 4.32 (1.09) | 4.39 (1.02) | 4.12 (1.22) | <0.001 | 4.30 (1.07) * | 4.35 (1.11) *** | 0.471 |
| Religious institutions | 4.47 (1.03) | 4.50 (1.00) | 4.41 (1.13) | 0.174 | 4.53 (0.95) * | 4.43 (1.12) *** | 0.076 |
| Indoors of schools, kindergartens | 4.51 (1.00) | 4.55 (0.95) | 4.42 (1.13) | 0.033 | 4.49 (0.99) * | 4.55 (1.03) *** | 0.238 |
| Schoolyards of schools, kindergartens | 4.51 (1.00) | 4.53 (0.96) | 4.44 (1.08) | 0.131 | 4.50 (0.98) * | 4.53 (1.03) *** | 0.536 |
| Indoors of universities, colleges | 4.04 (1.34) | 4.18 (1.24) | 3.68 (1.52) | <0.001 | 3.63 (1.45) * | 4.49 (1.05) *** | <0.001 |
| In restaurants, cafes, cafeterias | 3.80 (1.38) | 4.05 (1.20) | 3.13 (1.59) | <0.001 | 3.67 (1.37) | 3.95 (1.38) *** | <0.001 |
| In bars, pubs, nightclubs | 3.51 (1.48) | 3.77 (1.35) | 2.84 (1.59) | <0.001 | 3.48 (1.45) | 3.56 (1.52) *** | 0.261 |
| Public transportation | 4.42 (1.08) | 4.46 (1.03) | 4.32 (1.18) | 0.031 | 4.42 (1.04) | 4.43 (1.13) *** | 0.862 |
| (a) Nonsmokers’ and Smokers’ Support for Use Bans of Cigarettes and ENDS/HTPs | Nonsmokers | Smokers | ||||||
| Cigarettes, n = 1019 | ENDS/HTPs, n = 1015 | Cigarettes, n = 372 | ENDS/HTPs, n = 376 | |||||
| B (95% CI) | p | B (95% CI) | p | B (95% CI) | p | B (95% CI) | p | |
| Intercept | 4.14 (3.95, 4.33) | <0.001 | 4.38 (4.04, 4.71) | <0.001 | 3.31 (2.93, 3.68) | <0.001 | 3.97 (3.40, 4.54) | <0.001 |
| Georgia (vs. Armenia) | 0.11 (−0.06, 0.28) | 0.198 | 0.00 (−0.32, 0.32) | 0.977 | −0.17 (−0.40, 0.06) | 0.141 | −0.18(−0.57, 0.20) | 0.350 |
| Sociodemographics | ||||||||
| Age | 0.001 (−0.001, 0.001) | 0.380 | 0.00 (0.00, 0.00) | 0.507 | 0.00 (0.00, 0.01) | 0.324 | 0.00 (−0.01, 0.01) | 0.795 |
| Female (vs. male) | 0.19 (0.08, 0.23) | <0.001 | 0.02 (−0.15, 0.18) | 0.845 | 0.13 (−0.12, 0.38)) | 0.309 | 0.07 (−0.31, 0.44) | 0.730 |
| Unemployed/other (vs. employed) | 0.02 (−0.04, 0.08) | 0.544 | 0.00(−0.10, 0.10) | 0.982 | −0.07 (−0.21, 0.06) | 0.286 | 0.06(−0.15, 0.26) | 0.589 |
| Other (vs. married/cohabitating) | −0.01 (−0.09, 0.06) | 0.714 | −0.09 (−0.22, 0.03) | 0.126 | −0.04 (−0.20, 0.12) | 0.619 | −0.11 (−0.34, 0.13) | 0.367 |
| Children <18 in home (vs. no) | 0.01 (−0.05, 0.08) | 0.677 | 0.07 (−0.04, 0.18) | 0.227 | 0.01 (−0.12, 0.15) | 0.872 | 0.04 (−0.16, 0.24) | 0.675 |
| Smoking Characteristics | ||||||||
| Former smoker (vs. never) | −0.21 (−0.35, −0.08) | 0.002 | −0.03 (−0.24, 0.18) | 0.763 | - | - | - | - |
| Smoking some days (vs. every) | - | - | - | - | 0.36 (0.14, 0.57) | 0.001 | 0.23 (−0.08, 0.55) | 0.151 |
| Importance of quitting | - | - | - | - | 0.07 (0.05, 0.09) | <0.001 | 0.03 (0.00, 0.06) | 0.047 |
| Confidence in quitting | - | - | - | - | −0.01 (−0.03, 0.01) | 0.517 | −0.01 (−0.04, 0.02) | 0.494 |
| Unconditional Model ICC | 16.83% | 19.58% | 11.00% | 21.18% | ||||
| Full Model ICC | 15.79% | 21.42% | 15.31% | 21.12% | ||||
| (b) Nonsmokers’ and Smokers’ Rated Persuasiveness of Smoke-free Policy Messages | Nonsmokers | Smokers | ||||||
| Support, n = 1023 | Opposition, n = 1016 | Support, n = 375 | Opposition, n = 373 | |||||
| B (95% CI) | p | B (95% CI) | p | B (95% CI) | p | B (95% CI) | p | |
| Intercept | 3.31 (3.11, 3.52) | <0.001 | 2.66 (2.36, 2.95) | <0.001 | 3.41 (2.98, 3.84) | <0.001 | 2.83 (2.34, 3.33) | <0.001 |
| Georgia (vs. Armenia) | −0.13 (−0.32, 0.06) | 0.187 | −0.95 (−1.21, −0.69) | <0.001 | −0.46 (−0.66, −0.27) | <0.001 | −0.82 (−1.06, −0.58) | <0.001 |
| Sociodemographics | ||||||||
| Age | 0.002 (−0.001, 0.004) | 0.176 | 0.001 (−0.003, 0.005) | 0.678 | −0.01 (−0.01, −0.001) | 0.026 | 0.00 (0.00, 0.01) | 0.639 |
| Female (vs. male) | 0.06 (−0.05, 0.16) | 0.289 | 0.14 (−0.01, 0.29) | 0.074 | −0.02 (−0.32, 0.29) | 0.900 | −0.29 (−0.64, 0.06) | 0.105 |
| Unemployed/other (vs. employed) | 0.03 (−0.04, 0.10) | 0.379 | 0.001 (−0.09, 0.10) | 0.980 | 0.04 (−0.13, 0.21) | 0.630 | −0.01 (−0.20, 0.18) | 0.929 |
| Other (vs. married/cohabitating) | −0.05 (−0.12, 0.03) | 0.262 | −0.11 (−0.22, 0.01) | 0.065 | −0.09 (−0.29, 0.10) | 0.340 | 0.16 (−0.06, 0.38) | 0.150 |
| Children <18 in home (vs. no) | 0.06 (−0.1, 0.13) | 0.118 | 0.02 (−0.08. 0.13) | 0.647 | −0.13 (−0.3, 0.03) | 0.112 | 0.00 (−0.19, 0.19) | 0.986 |
| Smoking Characteristics | ||||||||
| Former smoker (vs. never) | −0.01 (−0.15, 0.13) | 0.846 | −0.05 (−0.25, 0.15) | 0.622 | - | - | - | - |
| Smoking some days (vs. every) | - | - | - | - | 0.31 (0.04, 0.58) | 0.022 | 0.51 (0.21, 0.81) | 0.001 |
| Importance of quitting | - | - | - | - | 0.05 (0.02, 0.07) | <0.001 | 0.01 (−0.01, 0.04) | 0.345 |
| Confidence in quitting | - | - | - | - | −0.01 (−0.03, 0.02) | 0.462 | −0.02 (−0.05, 0.01) | 0.117 |
| Unconditional model ICC | 17.79% | 39.73% | 13.90% | 25.5% | ||||
| full model ICC | 17.93% | 16.49% | 3.82% | 5.7% | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Topuridze, M.; Berg, C.J.; Dekanosidze, A.; Torosyan, A.; Grigoryan, L.; Bazarchyan, A.; Sargsyan, Z.; Hayrumyan, V.; Maglakelidze, N.; Sturua, L.; et al. Smokers’ and Nonsmokers’ Receptivity to Smoke-Free Policies and Pro- and Anti-Policy Messaging in Armenia and Georgia. Int. J. Environ. Res. Public Health 2020, 17, 5527. https://doi.org/10.3390/ijerph17155527
Topuridze M, Berg CJ, Dekanosidze A, Torosyan A, Grigoryan L, Bazarchyan A, Sargsyan Z, Hayrumyan V, Maglakelidze N, Sturua L, et al. Smokers’ and Nonsmokers’ Receptivity to Smoke-Free Policies and Pro- and Anti-Policy Messaging in Armenia and Georgia. International Journal of Environmental Research and Public Health. 2020; 17(15):5527. https://doi.org/10.3390/ijerph17155527
Chicago/Turabian StyleTopuridze, Marina, Carla J. Berg, Ana Dekanosidze, Arevik Torosyan, Lilit Grigoryan, Alexander Bazarchyan, Zhanna Sargsyan, Varduhi Hayrumyan, Nino Maglakelidze, Lela Sturua, and et al. 2020. "Smokers’ and Nonsmokers’ Receptivity to Smoke-Free Policies and Pro- and Anti-Policy Messaging in Armenia and Georgia" International Journal of Environmental Research and Public Health 17, no. 15: 5527. https://doi.org/10.3390/ijerph17155527
APA StyleTopuridze, M., Berg, C. J., Dekanosidze, A., Torosyan, A., Grigoryan, L., Bazarchyan, A., Sargsyan, Z., Hayrumyan, V., Maglakelidze, N., Sturua, L., Haardörfer, R., & Kegler, M. C. (2020). Smokers’ and Nonsmokers’ Receptivity to Smoke-Free Policies and Pro- and Anti-Policy Messaging in Armenia and Georgia. International Journal of Environmental Research and Public Health, 17(15), 5527. https://doi.org/10.3390/ijerph17155527