Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Assessment Tools
2.2. Intervention
2.2.1. Dry Land Therapy (Control Group)
2.2.2. Aquatic Ai Chi (Experimental Group)
2.2.3. Combined Therapy Group
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Soares, M.I.F.G. Acidente Vascular Cerebral Isqu-Êmico, Complicações Infecciosas Segundo o Volume e a Localização de Enfarte. Master’s Thesis, Universidade da Beira Interior, Covilhã, Portugal, 2011. [Google Scholar]
- Silva, L.R.V. Efeitos de um Programa de Imaginação no Controle Postural de Indivíduos pós Acidente Vascular Cerebral (AVC). Master’s Thesis, Universidade Federal do Paraná, Curitiba, PR, Brazil, 2011. [Google Scholar]
- O’Sullivan, S.B.; Schmitz, T.J.; Fulk, G.D. Physical Rehabilitation, 6th ed.; F. A. Davis Company: Philadelphia, PA, USA, 2007; p. 385. [Google Scholar]
- Hsu, A.-L.; Tang, P.-F.; Jan, M.-H. Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1185–1193. [Google Scholar] [CrossRef]
- Jung, T.; Lee, D.; Charalambous, C.; Vrongistinos, K. The Influence of Applying Additional Weight to the Affected Leg on Gait Patterns during Aquatic Treadmill Walking in People Poststroke. Arch. Phys. Med. Rehabil. 2010, 91, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Chon, S.C.; Oh, D.W.; Shim, J.H. Watsu approach for improving spasticity and ambulatory function in hemiparetic patients with stroke. Physiother. Res. Int. 2009, 14, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lima, M.J.M.; Brasileiro, I.C.; Lima, T.L.; Braga-Neto, P. Quality of life after stroke: Impact of clinical and sociodemographic factors. Clinics 2018, 73, 418. [Google Scholar] [CrossRef] [PubMed]
- Tripp, F.; Krakow, K. Effects of an aquatic therapy approach (Halliwick-Therapy) on functional mobility in subacute stroke patients: A randomized controlled trial. Clin. Rehabil. 2014, 28, 432–439. [Google Scholar] [CrossRef]
- Becker, B.E. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM&R 2009, 1, 859–872. [Google Scholar]
- Batterham, S.I.; Heywood, S.; Keating, J.L. Systematic review and meta-analysis comparing land and aquatic exercise for people with hip or knee arthritis on function, mobility and other health outcomes. BMC Musculoskelet. Disord. 2011, 12, 123. [Google Scholar] [CrossRef]
- Neto, M.G.; Conceição, C.S.; de Jesus, F.L.; Oliveira Carvalho, V. Hydrotherapy on exercise capacity, muscle strength and quality of life in patients with heart failure: A metaanalysis. Int. J. Cardiol. 2015, 198, 216–219. [Google Scholar] [CrossRef]
- Plecash, A.R.; Leavitt, B.R. Aquatherapy for neurodegenerative disorders. J. Huntingtons Dis. 2014, 3, 5–11. [Google Scholar] [CrossRef]
- Methajarunon, P.; Eitivipart, C.; Diver, C.J.; Foongchomcheay, A. Systematic review of published studies on aquatic exercise for balance in patients with multiple sclerosis, Parkinson’s disease, and hemiplegia. Hong Kong Physiother. J. 2016, 35, 12–20. [Google Scholar] [CrossRef]
- Marinho-Buzelli, A.R.; Bonnyman, A.M.; Verrier, M.C. The effects of aquatic therapy on mobility of individuals with neurological diseases: A systematic review. Clin. Rehabil. 2015, 29, 741–751. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.S.; Eng, J.J.; Dawson, A.S.; Harris, J.E.; Ozkaplan, A.; Gylfadottir, S. Water-based exercise for cardiovascular fitness in people with chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2004, 85, 870–874. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.H.; Du, D.C.; Jiang, K. Therapeutic efficacy of acupuncture combined with neuromuscular joint facilitation in treatment of hemiplegic shoulder pain. World J. Clin. Cases 2019, 7, 3964–3970. [Google Scholar] [CrossRef]
- Colombo, P.; Taveggia, G.; Chiesa, D.; Penati, R.; Tiboni, M.; De Armas, L.; Casale, R. Lower Tinetti scores can support an early diagnosis of spatial neglect in post-stroke patients. Eur. J. Phys. Rehabil. Med. 2019, 55, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Shubert, T.E.; Schrodt, L.; Mercer, V.S.; Busby-Whitehead, J.; Giuliani, C. Are scores on balance screening tests associated with mobility in older adults? J. Geriatr. Phys. Ther. 2006, 29, 35–39. [Google Scholar] [CrossRef]
- Stack, E.L.; Ashburn, A.M.; Jupp, K.E. Strategies used by people with Parkinson’s disease who report difficulty turning. Parkinsonism Relat. Disord. 2006, 12, 87–92. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Madeira, P.; Dominguez-Muñoz, F.J.; Villafaina, S.; Tomas-Carus, P.; Parraca, J.A. The Automatic Assessment of Strength and Mobility in Older Adults: A Test-Retest Reliability Study. Medicina 2019, 55, 270. [Google Scholar] [CrossRef]
- Maleki, M.; Imanian, K.; Bayat, Z.S.; Mehrabi, Y. Assessment of the risk of falls related to imbalance among patients with multiple sclerosis referred to the ms society of Tehran 2014. Adv. Nurs. Midwifery 2016, 25, 1–8. [Google Scholar]
- Salinet, A.S.M. Hidroterapia e Reabilitação Cardiorespiratoria após Acidente Vascular Cerebral. Stroke 2012, 7, 157–162. [Google Scholar] [CrossRef]
- Dimitrijević, L.; Aleksandrović, M.; Madić, D.; Okičić, T.; Radovanović, D.; Daly, D. The effect of aquatic intervention on the gross motor function and aquatic skills in children with cerebral palsy. J. Hum. Kinet. 2012, 32, 167–174. [Google Scholar] [CrossRef]
- Park, J.; Lee, D.; Lee, S.; Lee, C.; Yoon, J.; Lee, M.; Lee, J.; Choi, J.; Roh, H. Comparison of the Effects of Exercise by Chronic Stroke Patients in Aquatic and Land Environments. J. Phys. Ther. Sci. 2011, 23, 821–824. [Google Scholar] [CrossRef][Green Version]
- Montagna, J.C.; Santos, B.C.; Battistuzzo, C.R.; Loureiro, A.P.C. Effects of aquatic physiotherapy on the improvement of balance and corporal symmetry in stroke. Int. J. Clin. Exp. Med. 2014, 7, 1182–1187. [Google Scholar] [PubMed]
- Chen, L.; Lo, W.L.; Mao, Y.R.; Ding, M.H.; Lin, Q.; Li, H.; Zhao, J.L.; Xu, Z.Q.; Bian, R.H.; Huang, D.F. Effect of Virtual Reality on Postural and Balance Control in Patients with Stroke: A Systematic Literature Review. BioMed Res. Int. 2016, 2016, 7309272. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.H.; Lee, J.Y.; Chung, E.J.; Kim, K. The effect of obstacle training in water on static balance of chronic stroke patients. J. Phys. Ther. Sci. 2014, 26, 437. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Lee, K.J.; Shin, D.C.; Shin, S.H.; Lee, M.M.; Song, C.H. The effect of underwater gait training on balance ability of stroke patients. J. Phys. Ther. Sci. 2014, 26, 899. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhu, Z.; Cui, L.; Yin, M.; Yu, Y.; Zhou, X.; Wang, H.; Yan, H. Hydrotherapy vs. Conventional land-based exercise for improving walking and balance after stroke: A randomized controlled trial. Clin. Rehabil. 2015, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Coco, M.; Maugeri, A.; Perciavalle, V. Effects induced by swim on a patient with multiple sclerosis. Case report. Acta Med. Mediterr. 2006, 21, 85–92. [Google Scholar]
- Corvillo, I.; Varela, E.; Armijo, F.; Alvarez-Badillo, A.; Armijo, O.; Maraver, F. Efficacy of aquatic therapy for multiple sclerosis: A systematic review. Eur. J. Phys. Rehabil. Med. 2017, 53, 944–952. [Google Scholar]
- Salem, Y.; Scott, A.H.; Karpatkin, H.; Concert, G.; Haller, L.; Kaminsky, E.; Weisbrot, R.; Spatz, E. Community-based group aquatic programme for individuals with multiplesclerosis: A pilot study. Disabil. Rehabil. 2011, 33, 720–728. [Google Scholar] [CrossRef]
- Teixeira, R.; Pérez, L.; Lambeck, J.; Neto, F. The influence of Ai Chi on balance and fear of falling in older adults: A randomized clinical trial. Physiotherapy 2010, 97, 654. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
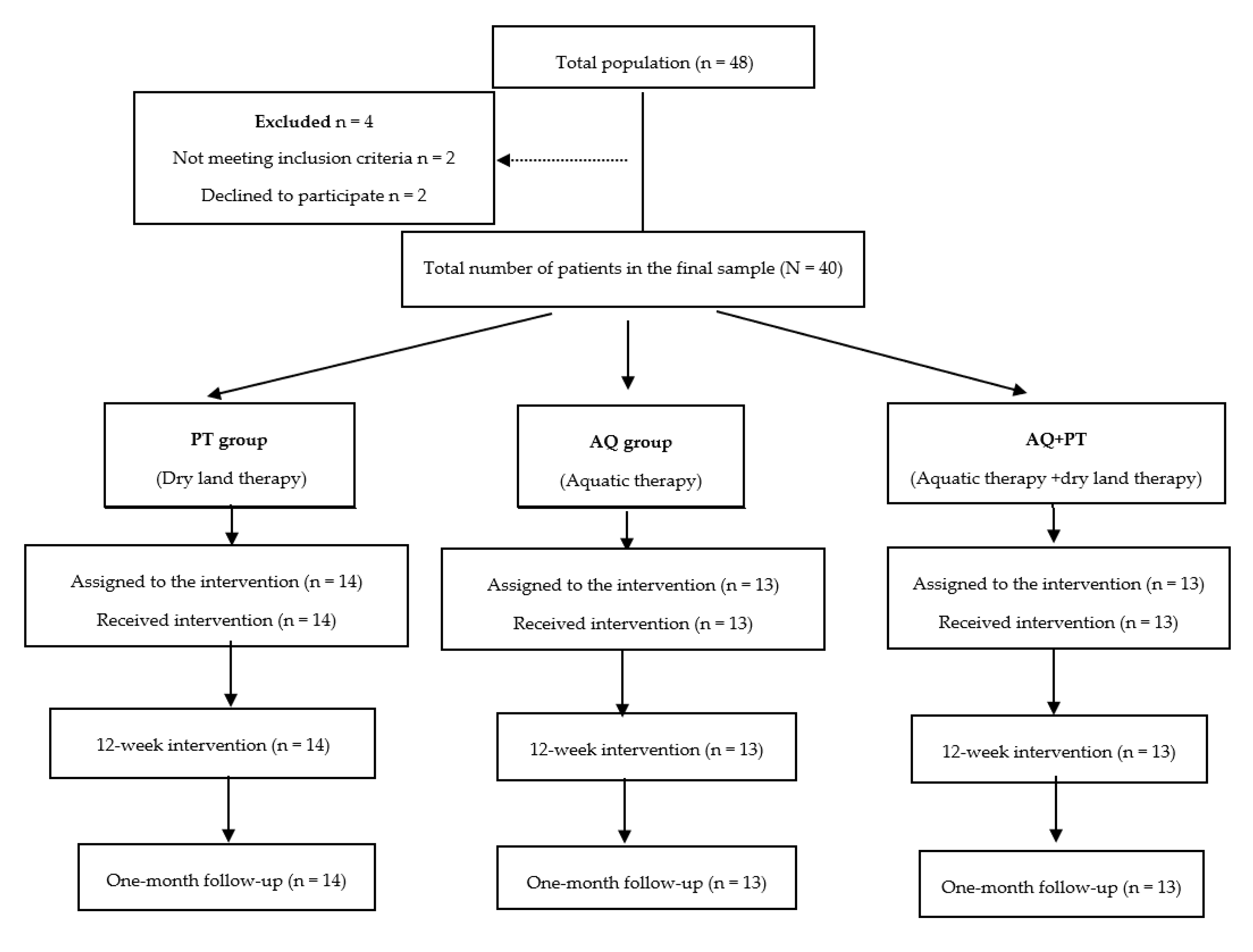
| Characteristics | Treatment | p | ||
|---|---|---|---|---|
| AQ + PT Group (n = 13) | PT Group (n = 14) | AQ Group (n = 13) | ||
| Age (years) | 53.1 ±11.5 | 54.6 ±12.1 | 54.2 ±13.4 | 0.789 |
| Sex (%) | 0.634 | |||
| Females | 5 (38.5) | 7 (50.0) | 7 (53,8) | |
| Males | 8 (61.5) | 7 (50.0) | 6 (46.1) | |
| Previous history (%) | 0.709 | |||
| No | 9 (69.3) | 10 (71.4) | 9 (69.2) | |
| Yes | 4 (30.7) | 4 (28.6) | 4 (30.7) | |
| Surgical interventions (%) | 0.311 | |||
| No | 4 (31) | 7 (50.0) | 5 (28.4) | |
| Yes | 9 (69) | 7 (50.0) | 8 (61.5) | |
| Medication (%) | 0.047 | |||
| No | 4 (30.7) | 0 (0) | 2 (15.3) | |
| Yes | 9 (69.3) | 14 (100) | 11 (84.6) | |
| BMI (kg/m2) | 26.5 ±2.7 | 25.8 ±2.9 | 25.3 ±3.3 | 0.836 |
| Time since the lesion (years) | 6.6 ±3.2 | 5.7 ±2.6 | 5.4 ±4.7 | 0.162 |
| Rating Scale | Pre | Post | 1 Month | Time | Treatment *Time |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | F(g.l.); p-Value (eta2) | F(g.l.); p-Value (eta2) | |
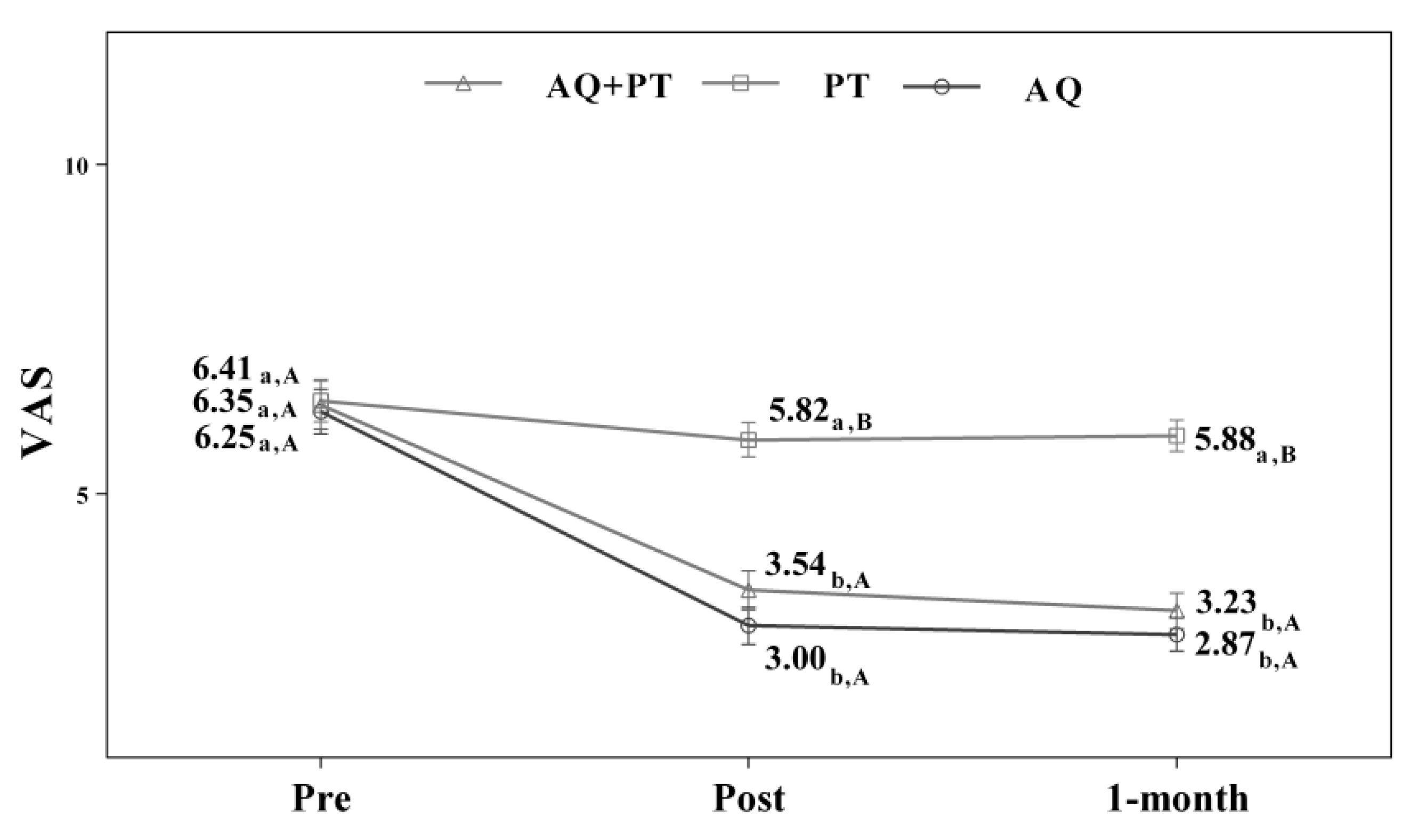
| VAS_SCALE | F(1.2; 55.7) = 156.82; p < 0.001 (0.788) | F(2.9; 55.8) = 24.64; p < 0.001 (0.551) | |||
| AQ + PT group | 6.53 ± 1.1 | 3.68 ± 1.2 | 3.38 ± 0.8 | ||
| PT group | 6.61 ± 1,6 | 5.91 ± 1.3 | 5.78 ± 1.2 | ||
| AQ group | 6.46 ± 1,5 | 3.11 ± 1.4 | 2.89 ± 1.0 | ||
| TINETTI_BALANCE | F(1.1; 45.2) = 54.81; p < 0.001 (0.566) | F(2.2; 45.2) = 4.81; p = 0.011 (0.186) | |||
| AQ + PT group | 8.00 ± 3.4 | 10.69 ± 2.6 | 11.15 ± 2.7 | ||
| PT group | 7.18 ± 2.2 | 8.18 ± 2.0 | 8.12 ± 1.9 | ||
| AQ group | 7.73 ± 2.5 | 10.47 ± 2.8 | 10.47 ± 2.8 | ||
| TINETTI_GAIT | F(1.2; 48.4) = 76.87; p < 0.001 (0.647) | F(2.3; 48.4) = 6.89; p = 0.002 (0.247) | |||
| AQ + PT group | 5.31 ± 3.0 | 7.92 ± 2.6 | 8.23 ± 2.5 | ||
| PT group | 5.47 ± 2.1 | 6.53 ± 1.7 | 6.24 ± 1.8 | ||
| AQ group | 5.33 ± 2.6 | 7.27 ± 2.5 | 7.27 ± 2.5 | ||
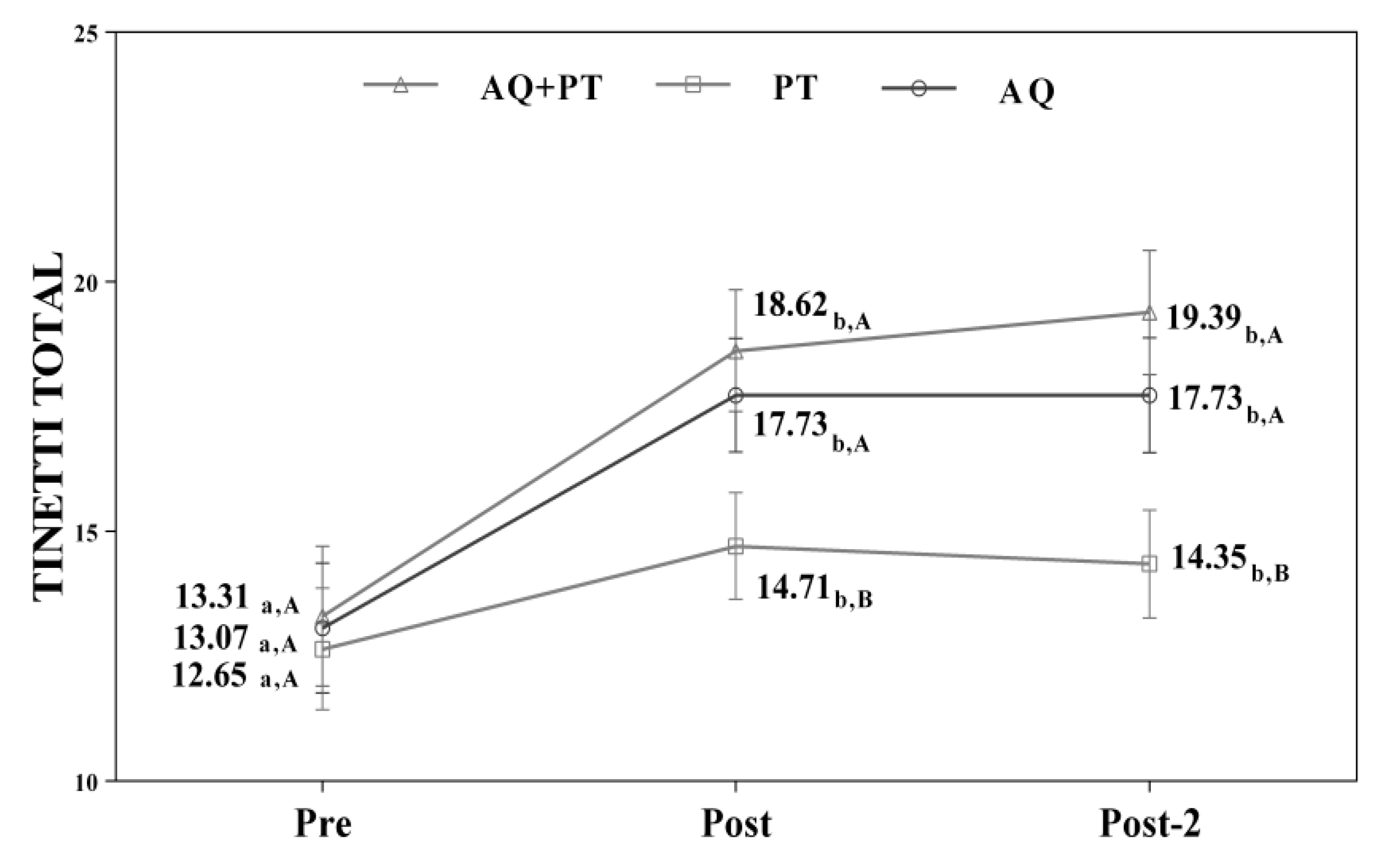
| TINETTI_TOTAL | F(1.1; 45.2) = 77.90; p < 0.001 (0.650) | F(2.2; 45.2) = 6.67; p = 0.002 (0.241) | |||
| AQ + PT group | 13.31 ± 4.2 | 18.62 ± 4.8 | 19.39 ± 4.9 | ||
| PT group | 12.65 ± 4.0 | 14.71 ± 3.3 | 14.35 ± 3.4 | ||
| AQ group | 13.07 ± 4.9 | 17.73 ± 5.1 | 17.73 ± 5.1 | ||
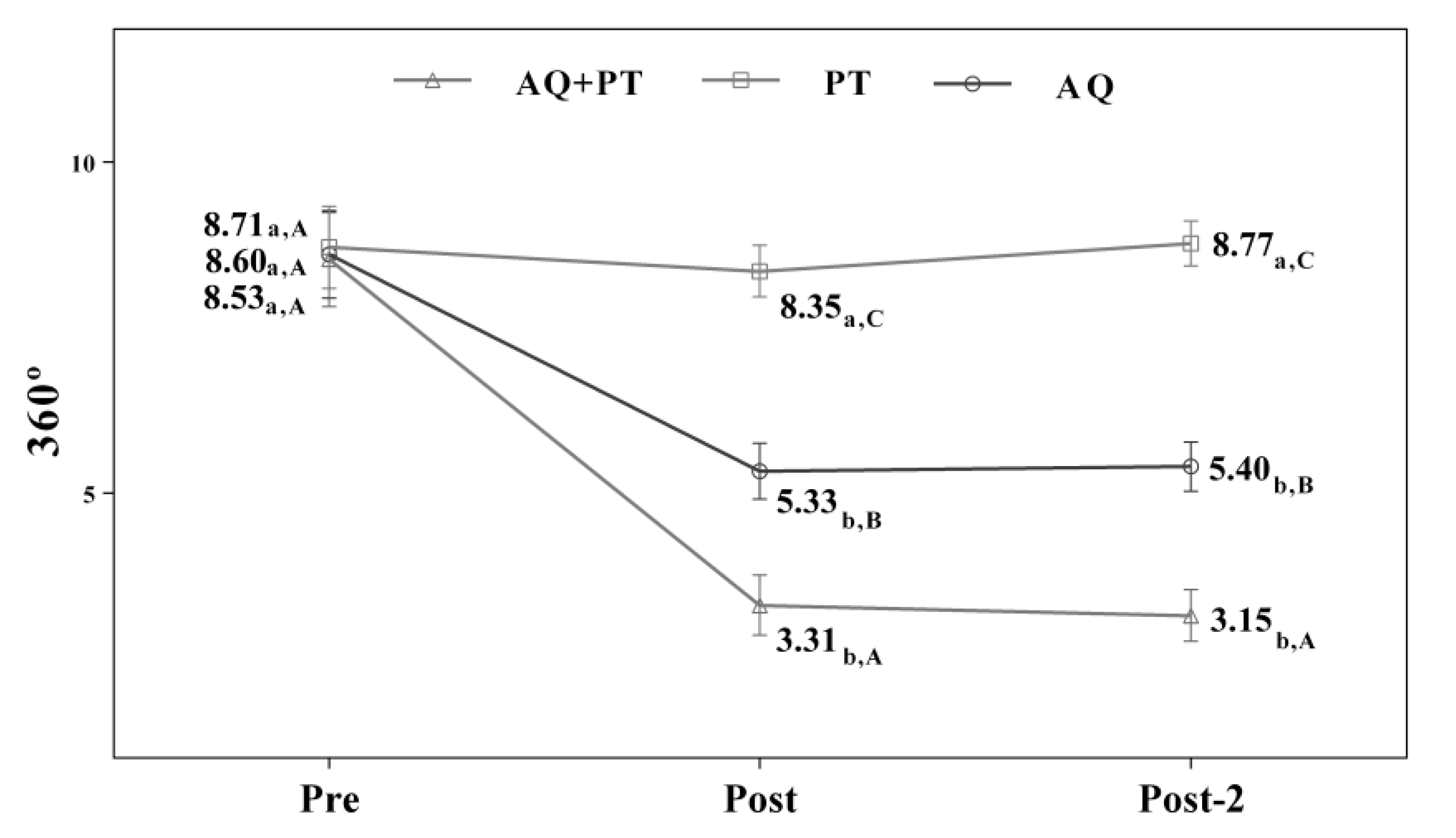
| 360° | F(1.2; 50.3) = 49.39; p < 0.001 (0.540) | F(2.4; 50.3) = 11.77; p < 0.001 (0.359) | |||
| AQ + PT group | 8.53 ± 2.0 | 3.31 ± 1.1 | 3.15 ± 1.0 | ||
| PT group | 8.71 ± 2.7 | 8.35 ± 2.3 | 8.77 ± 1.9 | ||
| AQ group | 8.60 ± 2.7 | 5.33 ± 1.0 | 5.40 ± 1.0 | ||
| RIGHT SINGLE-LEG- STANCE-BALANCE | F(1.1;45.4) = 21.19; p < 0.001 (0.335) | F(2.2;45.4) = 7.63; p = 0.001 (0.266) | |||
| AQ + PT group | 4.90 ± 3.1 | 19.31 ± 3.1 | 21.54 ± 3.7 | ||
| PT group | 3.88 ± 3.6 | 4.24 ± 3.1 | 3.94 ± 3.1 | ||
| AQ group | 4.80 ± 6.0 | 10.60 ± 9.0 | 11.80 ± 8.2 | ||
| LEFT SINGLE-LEG- STANCE-BALANCE | F(1.1; 48.0) = 14.21; p < 0.001 (0.253) | F(2.3; 48.0) = 5.84; p = 0.004 (0.218) | |||
| AQ + PT group | 3.24 ± 3.5 | 21.23 ± 2.8 | 28.62 ± 2.7 | ||
| PT group | 3.59 ± 3.3 | 3.77 ± 2.8 | 3.59 ± 2.8 | ||
| AQ group | 3.87 ± 4.6 | 9.73 ± 6.6 | 11.53 ± 5.2 | ||
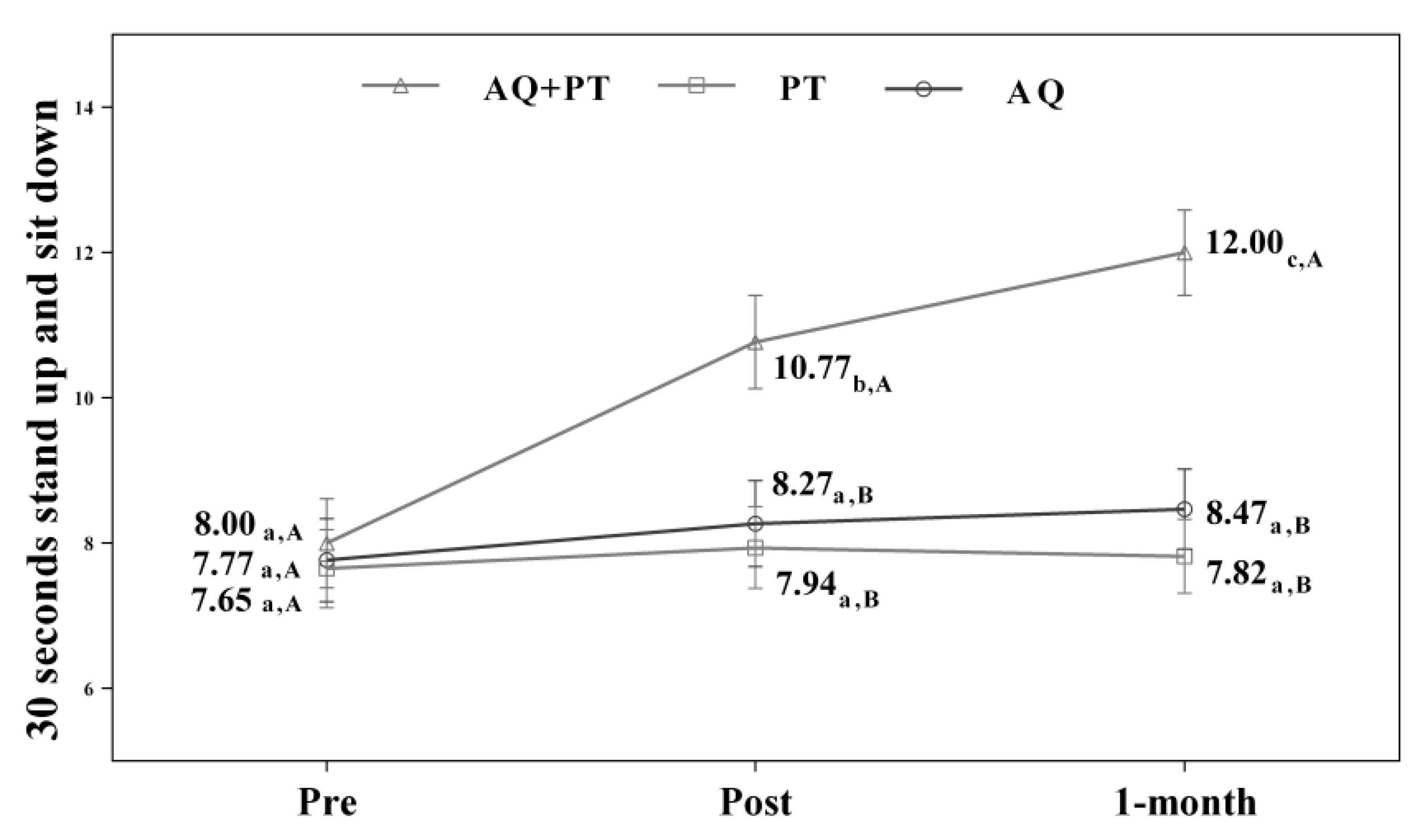
| CS-30 | F(1.6; 65.5) = 84.75; p < 0.001 (0.669) | F(3.1; 65.5) = 22.24; p < 0.001 (0.514) | |||
| AQ + PT group | 8.00 ± 1.7 | 10.77 ± 1.9 | 12.00 ± 1.8 | ||
| PT group | 7.65 ± 2.2 | 7.94 ± 2.2 | 7.82 ± 2.1 | ||
| AQ group | 7.77 ± 2.6 | 8.27 ± 2.7 | 8.47 ± 2.4 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-de la Cruz, S. Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients. Int. J. Environ. Res. Public Health 2020, 17, 4728. https://doi.org/10.3390/ijerph17134728
Pérez-de la Cruz S. Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients. International Journal of Environmental Research and Public Health. 2020; 17(13):4728. https://doi.org/10.3390/ijerph17134728
Chicago/Turabian StylePérez-de la Cruz, Sagrario. 2020. "Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients" International Journal of Environmental Research and Public Health 17, no. 13: 4728. https://doi.org/10.3390/ijerph17134728
APA StylePérez-de la Cruz, S. (2020). Comparison of Aquatic Therapy vs. Dry Land Therapy to Improve Mobility of Chronic Stroke Patients. International Journal of Environmental Research and Public Health, 17(13), 4728. https://doi.org/10.3390/ijerph17134728