Self-Regulation in Children with Neurodevelopmental Disorders “SR-MRehab: Un Colegio Emocionante”: A Protocol Study

 ,
,  , , and
, , and
Abstract
1. Introduction
1.1. Aims and Hypotheses
1.1.1. Primary Objective
1.1.2. Hypotheses
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedure and Enrollment
2.2.1. Study Variables
2.2.2. Pre-Assessment, Post-Assessment and Follow-Up at 6 Months
2.2.3. Intervention
Experimental Group
Control Group
2.2.4. Outcome Measures
Primary Outcome Measure: Emotional Regulation
- (1)
- Emotional Perception
- (2)
- Emotional Regulation
Secondary Outcome Measure: Cognitive Regulation
- (1)
- Cognitive Flexibility
- (2)
- Planning and Sequencing
2.3. Data Mangement
2.4. Statistical Analysis
2.4.1. Sample Size
2.4.2. Data Analysis Plan
2.5. Ethical Approval, Ethical Considerations and Dissemination
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Villani, D.; Carissoli, C.; Triberti, S.; Marchetti, A.; Gilli, G.; Riva, G. Videogames for Emotion Regulation: A Systematic Review. Games Health J. 2018, 7, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Flores-Lázaro, J.; Castillo-Preciado, R.; Jiménez-Miramonte, N. Desarrollo de funciones ejecutivas, de la niñez a la juventud. Anales De Psicología 2014, 30, 463–473. [Google Scholar]
- Anastopoulos, A.D.; Smith, T.F.; Garrett, M.E.; Morrissey-Kane, E.; Schatz, N.K.; Sommer, J.L.; Kollins, S.H.; Ashley-Koch, A. Self-Regulation of Emotion, Functional Impairment, and Comorbidity Among ChildrenWith AD/HD. J. Atten. Disord. 2011, 15, 583–592. [Google Scholar] [CrossRef]
- Reyes, N.M.; Pickard, K.; Reaven, J. Emotion regulation: A treatment target for autism spectrum disorder. Bull. Menn. Clin. 2019, 83, 205–234. [Google Scholar] [CrossRef]
- Bisquerra Alzina, R.; Mateo Andrés, J. Competencias Emocionales Para Un Cambio De Paradigma En Educaciã³N; Horsori: Barcelona, Spain, 2019; p. 242. [Google Scholar]
- Cai, R.Y.; Richdale, A.L.; Dissanayake, C.; Uljarević, M. How Does Emotion Regulation Strategy Use and Psychological Wellbeing Predict Mood in Adults With and Without Autism Spectrum Disorder? A Naturalistic Assessment. J. Autism. Dev. Disord. 2019, 50, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Garland, T. Self-Regulation Interventions and Strategies. In Keeping the Body, Mind & Emotions on Task in Children with Autism, ADHD or Sensory Disorders; PESI Publising & Media: Eau Claire, WI, USA, 2014. [Google Scholar]
- Waddington, F.; Hartman, C.; de Bruijn, Y.; Lappenschaar, M.; Oerlemans, A.; Buitelaar, J.; Franke, B.; Lambregts-Rommelse, N.N.J. An emotion recognition subtyping approach to studying the heterogeneity and comorbidity of autism spectrum disorders and attention-deficit/hyperactivity disorder. J. Neurodev. Disord. 2018, 10, 31. [Google Scholar] [CrossRef]
- Moessnang, C.; Baumeister, S.; Tillmann, J.; Goyard, D.; Charman, T.; Ambrosino, S.; Baron-Cohen, S.; Beckmann, C.; Bölte, S.; Bours, C.; et al. Social brain activation during mentalizing in a large autism cohort: The Longitudinal European Autism Project. Mol. Autism. 2020, 11, 17. [Google Scholar] [CrossRef]
- Seng, G.J.; Tseng, W.L.; Chiu, Y.N.; Tsai, W.C.; Wu, Y.Y.; Gau, S.S. Executive functions in youths with autism spectrum disorder and their unaffected siblings. Psychol. Med. 2020. [Google Scholar] [CrossRef]
- Trimarco, B.; Manti, F.; Nardecchia, F.; Melogno, S.; Testa, M.; Meledandri, G.; Carducci, C.; Penge, R.; Leuzzi, V. Executive functioning, adaptive skills, emotional and behavioral profile: A comparison between autism spectrum disorder and phenylketonuria. Mol. Genet. Metab. Rep. 2020, 23, 100577. [Google Scholar] [CrossRef]
- Barkley, R.A. Attention-deficit/hyperactivity disorder, self-regulation, and time: Toward a more comprehensive theory. J. Dev. Behav. Pediatr. 1997, 18, 271–279. [Google Scholar] [CrossRef]
- Barkley, R.A.; Edwards, G.; Laneri, M.; Fletcher, K.; Metevia, L. Executive functioning, temporal discounting, and sense of time in adolescents with attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD). J. Abnorm. Child. Psychol. 2001, 29, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Predescu, E.; Sipos, R.; Costescu, C.A.; Ciocan, A.; Rus, D.I. Executive Functions and Emotion Regulation in Attention-Deficit/Hyperactivity Disorder and Borderline Intellectual Disability. J. Clin. Med. 2020, 9, 986. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Sonuga-Barke, E.J. Causal models of attention-deficit/hyperactivity disorder: From common simple deficits to multiple developmental pathways. Biol. Psychiatry 2005, 57, 1231–1238. [Google Scholar] [CrossRef]
- Van Cauwenberge, V.; Sonuga-Barke, E.J.; Hoppenbrouwers, K.; Van Leeuwen, K.; Wiersema, J.R. Turning down the heat: Is poor performance of children with ADHD on tasks tapping “hot” emotional regulation caused by deficits in “cool” executive functions? Res. Dev. Disabil. 2015, 47, 199–207. [Google Scholar] [CrossRef]
- Navarro, E.; González, P.; López-Jaquero, V.; Montero, F.; Molina, J.P.; Romero-Ayuso, D. Adaptive, Multisensorial, Physiological and Social: The Next Generation of Telerehabilitation Systems. Front. Neuroinform. 2018, 12, 43. [Google Scholar] [CrossRef]
- Radovic, A.; Badawy, S.M. Technology Use for Adolescent Health and Wellness. Pediatrics 2020, 145 (Suppl. S2), S186–S194. [Google Scholar] [CrossRef]
- Rizzo, A.; Buckwalter, J.G.; John, B.; Newman, B.; Parsons, T.; Kenny, P.; Williams, J. STRIVE: Stress Resilience In Virtual Environments: A pre-deployment VR system for training emotional coping skills and assessing chronic and acute stress responses. Stud. Health Technol. Inform. 2012, 173, 379–385. [Google Scholar]
- Parsons, T.D.; Bowerly, T.; Buckwalter, J.G.; Rizzo, A.A. A controlled clinical comparison of attention performance in children with ADHD in a virtual reality classroom compared to standard neuropsychological methods. Child. Neuropsychol. 2007, 13, 363–381. [Google Scholar] [CrossRef]
- Parsons, T.D. Virtual Reality for Enhanced Ecological Validity and Experimental Control in the Clinical, Affective and Social Neurosciences. Front. Hum. Neurosci. 2015, 9, 660. [Google Scholar] [CrossRef]
- Bashiri, A.; Ghazisaeedi, M.; Shahmoradi, L. The opportunities of virtual reality in the rehabilitation of children with attention deficit hyperactivity disorder: A literature review. Korean J. Pediatr. 2017, 60, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.A.; Gil-Gómez, J.A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef] [PubMed]
- Parsons, T.D.; Riva, G.; Parsons, S.; Mantovani, F.; Newbutt, N.; Lin, L.; Venturini, E.; Hall, T. Virtual Reality in Pediatric Psychology. Pediatrics 2017, 140 (Suppl. S2), S86–S91. [Google Scholar] [CrossRef] [PubMed]
- Voss, C.; Schwartz, J.; Daniels, J.; Kline, A.; Haber, N.; Washington, P.; Tariq, Q.; Robinson, T.N.; Desai, M.; Phillips, J.M.; et al. Effect of Wearable Digital Intervention for Improving Socialization in Children With Autism Spectrum Disorder: A Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Bekele, E.; Zheng, Z.; Swanson, A.; Crittendon, J.; Warren, Z.; Sarkar, N. Understanding how adolescents with autism respond to facial expressions in virtual reality environments. IEEE Trans. Vis. Comput. Graph. 2013, 19, 711–720. [Google Scholar] [CrossRef]
- Bekele, E.; Crittendon, J.; Zheng, Z.; Swanson, A.; Weitlauf, A.; Warren, Z.; Sarkar, N. Assessing the utility of a virtual environment for enhancing facial affect recognition in adolescents with autism. J. Autism. Dev. Disord. 2014, 44, 1641–1650. [Google Scholar] [CrossRef]
- Yuan, S.N.V.; Ip, H.H.S. Using virtual reality to train emotional and social skills in children with autism spectrum disorder. Lond. J. Prim. Care (Abingdon) 2018, 10, 110–112. [Google Scholar] [CrossRef]
- Alcañiz, M.; Chicchi Giglioli, I.A.; Sirera, M.; Minissi, E.; Abad, L. Autism spectrum disorder biomarkers based on biosignals, virtual reality and artificial intelligence. Medicina (B Aires) 2020, 80 (Suppl. S2), 31–36. [Google Scholar]
- Shema-Shiratzky, S.; Brozgol, M.; Cornejo-Thumm, P.; Geva-Dayan, K.; Rotstein, M.; Leitner, Y.; Hausdroff, J.M.; Mirelaman, A. Virtual reality training to enhance behavior and cognitive function among children with attention-deficit/hyperactivity disorder: Brief report. Dev. Neurorehabil. 2019, 22, 431–436. [Google Scholar] [CrossRef]
- Blume, F.; Hudak, J.; Dresler, T.; Ehlis, A.C.; Kühnhausen, J.; Renner, T.J.; Gawrilow, C. NIRS-based neurofeedback training in a virtual reality classroom for children with attention-deficit/hyperactivity disorder: Study protocol for a randomized controlled trial. Trials 2017, 18, 41. [Google Scholar] [CrossRef]
- Eom, H.; Kim, K.K.; Lee, S.; Hong, Y.J.; Heo, J.; Kim, J.J.; Kim, E. Development of Virtual Reality Continuous Performance Test Utilizing Social Cues for Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Areces, D.; Dockrell, J.; García, T.; González-Castro, P.; Rodríguez, C. Analysis of cognitive and attentional profiles in children with and without ADHD using an innovative virtual reality tool. PLoS ONE 2018, 13, e0201039. [Google Scholar] [CrossRef] [PubMed]
- Neguț, A.; Jurma, A.M.; David, D. Virtual-reality-based attention assessment of ADHD: ClinicaVR: Classroom-CPT versus a traditional continuous performance test. Child. Neuropsychol. 2017, 23, 692–712. [Google Scholar] [CrossRef] [PubMed]
- Vahabzadeh, A.; Keshav, N.U.; Abdus-Sabur, R.; Huey, K.; Liu, R.; Sahin, N.T. Improved Socio-Emotional and Behavioral Functioning in Students with Autism Following School-Based Smartglasses Intervention: Multi-Stage Feasibility and Controlled Efficacy Study. Behav. Sci. 2018, 8, 85. [Google Scholar] [CrossRef]
- Keshav, N.U.; Vogt-Lowell, K.; Vahabzadeh, A.; Sahin, N.T. Digital Attention-Related Augmented-Reality Game: Significant Correlation between Student Game Performance and Validated Clinical Measures of Attention-Deficit/Hyperactivity Disorder (ADHD). Children 2019, 6, 72. [Google Scholar] [CrossRef]
- Newbutt, N.; Bradley, R.; Conley, I. Using Virtual Reality Head-Mounted Displays in Schools with Autistic Children: Views, Experiences, and Future Directions. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 23–33. [Google Scholar] [CrossRef]
- Fernández, M.A.; Morillo, M.D.; Gilibert, N.; Carvalho, C.; Bello, S. The technological tools of the diagnosis and treatment of attention deficit disorder and hyperactivity. Medicina (B Aires) 2020, 80 (Suppl. S2), 67–71. [Google Scholar]
- Oliver, M.; Teruel, M.A.; Molina, J.P.; Romero-Ayuso, D.; González, P. Ambient Intelligence Environment for Home Cognitive Telerehabilitation. Sensors 2018, 18, 3671. [Google Scholar] [CrossRef]
- Oliver, M.; González, P.; Montero, F.; Molina, J.P.; Fernández-Caballero, A. Smart Computer-Assisted Cognitive Rehabilitation for the Ageing Population. In Advances in Intelligent Systems and Computing; Springer International Publishing: New York, NY, USA, 2016; pp. 197–205. [Google Scholar]
- Esnaola, I.; Freeman, J.; Sarasa, M.; Fernández-Zabala, A.; Axpe, I. Validity Evidence based on Internal Structure of Scores of the Emotional Quotient-Inventory: Youth Version Short (EQ-i: YV-S) in a Spanish Sample. Span. J. Psychol. 2016, 19, E12. [Google Scholar] [CrossRef]
- Barron-Linnankoski, S.; Reinvall, O.; Lahervuori, A.; Voutilainen, A.; Lahti-Nuuttila, P.; Korkman, M. Neurocognitive performance of children with higher functioning autism spectrum disorders on the NEPSY-II. Child. Neuropsychol. 2015, 21, 55–77. [Google Scholar] [CrossRef] [PubMed]
- Baron, I.S. Neuropsychological Evaluation of the Child; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Romero-Ayuso, D.; Toledano-González, A.; Segura-Fragoso, A.; Treviño-Juárez, J.; Rodríguez-Martínez, M. Assessment of Sensor Processing and Executive Functions at the School: Development, Reliability and Validity of EPYFEI-Escolar. Front. Pediatr. 2020, 8, 275. [Google Scholar] [CrossRef]
- Romero-Ayuso, D.; Jorquera-Cabrera, S.; Segura-Fragoso, A.; Toledano-González, A.; Rodríguez-Martínez, M.C.; Triviño-Juárez, J.M. Assessment of Sensory Processing and Executive Functions in Childhood: Development, Reliability, and Validity of the EPYFEI. Front. Pediatr. 2018, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Sim, G.; Horton, M. Investigating Children’s Opinions of Games: Fun Toolkit vs This or That. In Proceeding of the 11th International Conference on Interaction Design and Children, Bremen, Germany, 12–15 June 2012; Association for Computing Machinery: New York, NY, USA, 2012. [Google Scholar]
- Bisquerra, R. Educación emocional y competencias básicas para la vida. Rev. Investig. Educ. 2003, 21, 7–43. [Google Scholar]
- Martos-Pérez, J.; Llorente-Comí, M.; González-NAvarro, A.; Ayuda-Pascual, R.; Freire, S. Los Niños Pequeños Con AUTISMO; CEPE: Madrid, Spain, 2014. [Google Scholar]
- Bisquerra Alzina, R. Universidad de Barcelona. Grup de Recerca en Orientació Psicopedagògica. In Actividades para el desarrollo de la inteligencia emocional en los niños; Parramón: Barcelona, Spain, 2009; p. 192. [Google Scholar]
- Birnie, K.A.; Kulandaivelu, Y.; Jibb, L.; Hroch, P.; Positano, K.; Robertson, S.; Campbell, F.; Abla, O.; Stinson, J. Usability Testing of an Interactive Virtual Reality Distraction Intervention to Reduce Procedural Pain in Children and Adolescents With Cancer [Formula: See text]. J. Pediatr. Oncol. Nurs. 2018, 35, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.; Hovenden, M.; Ramage, E.; Ling, N.; Pham, J.H.; Rahim, A.; Lam, C.; Liu, L.; Foster, S.; Sambell, R.; et al. Virtual Reality for Pediatric Needle Procedural Pain: Two Randomized Clinical Trials. J. Pediatr. 2019, 209, 160–167.e4. [Google Scholar] [CrossRef]
- Eijlers, R.; Utens, E.M.W.J.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic Review and Meta-analysis of Virtual Reality in Pediatrics: Effects on Pain and Anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef]
- Bortone, I.; Leonardis, D.; Mastronicola, N.; Crecchi, A.; Bonfiglio, L.; Procopio, C.; Solazzi, M.; Frisoli, A. Wearable Haptics and Immersive Virtual Reality Rehabilitation Training in Children With Neuromotor Impairments. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1469–1478. [Google Scholar] [CrossRef]
- Cho, C.; Hwang, W.; Hwang, S.; Chung, Y. Treadmill Training with Virtual Reality Improves Gait, Balance, and Muscle Strength in Children with Cerebral Palsy. Tohoku J. Exp. Med. 2016, 238, 213–218. [Google Scholar] [CrossRef]
- Bioulac, S.; de Sevin, E.; Sagaspe, P.; Claret, A.; Philip, P.; Micoulaud-Franchi, J.A.; Bouvard, M.P. What do virtual reality tools bring to child and adolescent psychiatry? Encephale 2018, 44, 280–285. [Google Scholar] [CrossRef]
- Ashburner, J.; Ziviani, J.; Rodger, S. Sensory processing and classroom emotional, behavioral, and educational outcomes in children with autism spectrum disorder. Am. J. Occup. Ther. 2008, 62, 564–573. [Google Scholar] [CrossRef]
- Chang, Y.S.; Owen, J.P.; Desai, S.S.; Hill, S.S.; Arnett, A.B.; Harris, J.; Marco, E.J. Autism and sensory processing disorders: Shared white matter disruption in sensory pathways but divergent connectivity in social-emotional pathways. PLoS ONE 2014, 9, e103038. [Google Scholar] [CrossRef] [PubMed]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; p. 947. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Dimension/Processes | Instruments | Participants | Baseline | During Intervention | Immediately Post-Intervention | 24 Weeks Post-Intervention | ||
|---|---|---|---|---|---|---|---|---|---|
| Parents | Teachers | Students | |||||||
| Gender Age Special Needs Diagnosis | X X X | X | X X X X | ||||||
| Parent’s Educational level | X | ||||||||
| Previous experience with VR and serious games | X | X | |||||||
| Emotional Regulation | Emotional Awareness | NEPSY-II: Affect Recognition | X | X | X | X | |||
| Emotional Awareness | NEPSY-II: Theory of Mind | X | X | X | X | ||||
| Self-regulation | EPYFEI | X | X | X | X | ||||
| Self-regulation | EPYFEI-Escolar | X | X | X | X | ||||
| Emotional Competencies | EQ-i: YV * | X | X | X | X | ||||
| Cognitive Regulation/Executive Functions | WM, IC. Pln, Sq | EPYFEI | X | X | X | X | |||
| WK, IC, Pln, Sq | EPYFEI-Escolar | X | X | X | X | ||||
| Pl. Sq, Fl | NEPSY-II: Design Fluency | X | X | X | X | ||||
| Pl, Sq | NEPSY-II: Clock * | X | X | X | X | ||||
| Executive Attention | Trail Making Test A & Trail Making Test B | X | X | X | X | ||||
| IC | Stroop Test | X | X | X | X | ||||
| Virtual Tasks SR-MRehab | Percent Completed Nº of Errors Type of errors Activity Time Time without interaction Reason for non-attendance or early withdrawal | X X X X X X X | |||||||
| Acceptability | X | X |
| Variables/Aims Session | Emotional Regulation | Aim | Description | Cognitive Regulation/Executive Functions | Aim | Description |
|---|---|---|---|---|---|---|
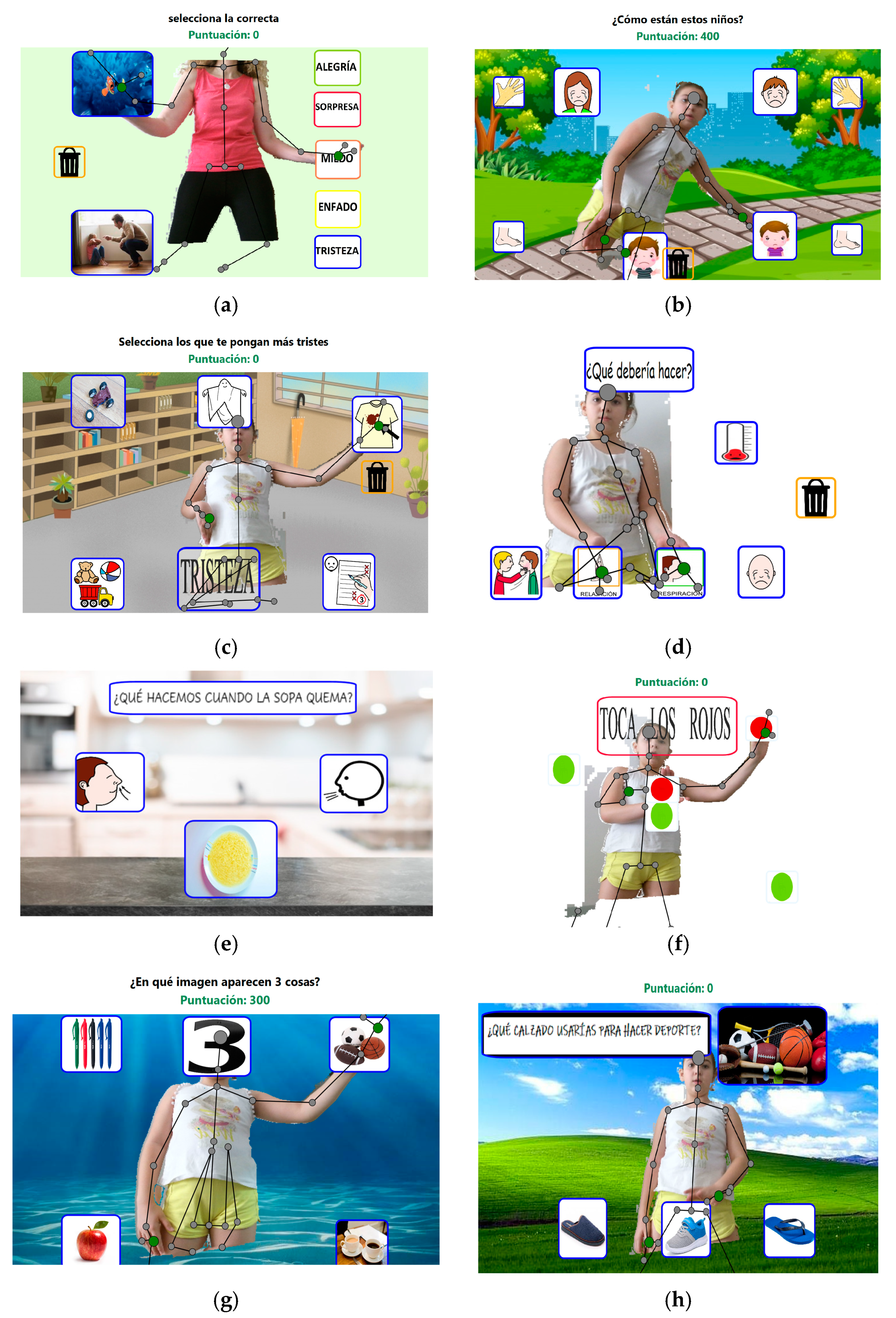
| 1 | Do you know the emotions? | Emotional perception | In the virtual school environment, children must identify the emotions on the faces of different children and adults. | Figure selection | Inhibitory control Working memory Flexibility | This activity consists in the selection of geometric figures that will appear on the left/right or top/bottom of the screen. The figures are organized in pairs, and the objective is to select the correct item from the appearance or disappearance of a signal. In the first two levels, an arrow indicates which option is correct. In the third and fourth levels, pairs of arrows will initially appear, one of which will then disappear, with the remaining one indicating the correct answer. In the fifth level, the signal will be a colored star (red or green), which will indicate the option to select. Finally, at level 6, the mechanism is similar to that of the third and fourth levels, that is, pairs of stars of different colors (red and green) will appear, of which one will disappear, with the color of the remaining one indicating the correct answer of the two options |
| 2 | Match and differences | Emotional perception Theory of Mind | Different family scenarios are presented at school and children are asked to identify the emotions on the faces and those shown by the body, in order to stimulate mentalization. What is this child thinking? How does the child feel? Do you choose a similar emotion in these two scenarios? Do you select contexts and situations where you can feel the same way? | Select equal and opposite emotions | Inhibitory control Working memory Flexibility | This activity is similar to the previous one, with the exception that this one is focused on emotions. |
| 3 | How are you? Virtual Emotion-Meter | Emotional perception | First, the child must identify or select how he/she feels and then indicate the intensity of the emotion. | Red No, green Yes: Traffic light One | Inhibitory control Working memory Flexibility Reasoning | Simulating a traffic light, it is explained that red indicates that we must stop before acting, for example, when we do not know the solution of a task, or at a certain indication, for example, from the teacher, such as when we cross a street. The yellow color means that we must be careful, think before acting (How can I solve the problem or situation?), and green can be applied when we know the solution to a problem very well. Different everyday situations arise, which pose a challenge for the child to inhibit impulsive behavior. The child must identify each red, yellow or green situation based on his/her own characteristics and situations in real life. Also, when a red signal comes out, the child cannot move. Otherwise, it will be counted as an error of commission. |
| 4 | How is your engine? | Emotional perception | In this task, the child has to indicate how calm or nervous he/she feels, and the intensity of such feeling. Finally, he/she is asked to think about how he/she can feel calmer and select among the different options to relax and feel good. | Simon says | Inhibitory control Flexibility | In this task, the child is asked to follow the instruction on the screen, only when the command is “Simon Says”. Upon any other request, that is, without the “Simon Says” command, the child must not move, in order to work the inhibitory control. |
| 5 | The Volcano | Emotional perception and regulation | The child has to indicate how angry or happy he/she feels. Finally, he/she is asked to think about how he/she can feel happier, how to generate positive feelings and select among the different alternatives to relax and feel good. | Find the difference! | Inhibitory control Flexibility Reasoning Problem solving | This task is divided into two blocks of 5 levels each. In the first block, a number from 1 to 5 will appear, along with several images containing different amounts of objects (1 to 5). The task is to match the indicated number with the image that represents that number. In the second block, all the numbers will appear, and, again, images with different amounts of objects. The task is to re-match each number that appears on the screen with the quantity that it represents. |
| 6 | Emotional traffic light | Emotional regulation | Simulating a traffic light, it is explained that red indicates that we must stop before acting, for example, when we are angry, yellow means that we have to think how we feel and how we can solve the problem or situation, and green can be applied when we are relaxed and can act calmly. The child must identify each red, yellow or green situation based on his/her own characteristics and situations in real life | Find your treasure! | Inhibitory control Flexibility Reasoning Solving problems | The child is asked to create a collage with words, short sentences and images that reflects how he/she can help other people and positive qualities of oneself. Later, the child must select actions that help him/her at home, at school, that is, what and how makes him/her feel useful and self-competent, and how others see him/her when he/she is useful. |
| 7 | Hot soup! The Lazarillo | Emotional regulation | The child must learn to relax through breathing, which is why the metaphor of hot soup is used, in which one has to blow and practice breathing. The child has to imitate the images and follow the prompts to blow the hot soup. In addition, at a later stage the child will be a “guide”, guiding the process of cooling the soup and must select the appropriate image | Looking at all sides | Flexibility Working memory | The aim of this task is for the participant to remember which animals previously appeared. To do this, an image will first be shown in which various animals will appear for 30 s, during which the patient will have to retain the displayed information. Once prepared, the participant will press GO! To make way for a new screen where animal drawings will appear. The patient’s task will be to select those animals that appeared in the previous image and discard those that did not. The difficulty increases proportionally with the number of animals and distractors that will appear |
| 8 | Bubbles or stones? | Emotional regulation | Through a story, they must explain which stones are the negative feelings (anger, sadness...) and the bubbles are positive feelings (happy, peace, calm). The child is asked to indicate what the backpack of different children would be filled with in different situations. Later, he/she is asked to choose what he/she wants to fill his/her backpack with, that is, bubbles or stones | Discover the stones and touch the bubbles!! How’s your backpack? | Reasoning Planning Problem solving Flexibility | In this task, starting from the story of the stones and bubbles, questions will be asked and various response options will be provided, which the children must correctly select using logic. Difficulty increases through with number of correct options and their similarity to distractors |
| 9 | Glasses to think well!! | Emotional regulation | Thoughts and feelings are related. Sometimes a positive thought can make us feel good and negative thoughts can make us feel bad. The child must choose those positive thoughts that make him/her feel good and learn to use it in his/her daily life | The turtle | Working memory Inhibitory control Flexibility Reasoning Problem solving | From the story of the turtle, as a self-control strategy, in this task, the image of a turtle will be exposed to the participant, who must observe it for a given period of time, until it disappears. When the participant is ready, he/she will press GO! To be launched to a screen, where an incomplete puzzle from the previous image will appear. Different pieces appear on the right, of which only one completes the puzzle. The participant’s task is to select that piece. The difficulty increases as the participant advances through the levels, adding more pieces as options and using more complex images |
| 10 | Letter of thanks | Emotional regulation | Thanksgiving can be a way to generate positive feelings in others and in oneself. The child must select situations in which it is appropriate to say “thanks” and images that show gratitude and allow us to “write” a letter of thanks to a friend, teacher, or family member. | 10 point Check-In | Inhibitory control Working memory Flexibility Reasoning Planning Problem solving | This task consists of 10 stages in a countdown sequence: (10) the children have to select 10 images that make them feel relaxed; (9) select 9 things that being with a certain letter or which can be found in a certain space (classroom, schoolyard, etc); (8) select 8 known people; (7) select 7 colors; (6) choose 6 things that make them feel happy; (5) choose images that reflect relaxation and imitate them; (4) select 4 objects they hear; (3) select 3 things that are in the room that they like to play with; (2) choose two images of techniques to relax and imitate them; (1) select the current emotion and thoughts |
| Variables/Aims Session | Emotional Regulation | Aim | Description | Cognitive Regulation/Executive Functions | Aim | Description |
|---|---|---|---|---|---|---|
| 1 | Do you know the emotions? | Emotional perception | Children must identify the emotions on cards of different children and adults. | Choose a number! | Inhibitory control Working memory Flexibility | In this activity, the children have to choose a number from 1–10. Depending on the number, a card corresponds to it. Each card has a red/green right/left or up/down arrow. So the child has to take a step as indicated by the arrow when the color of the arrow is green or make the opposite movement when the color of the arrow on the chosen card is red. |
| 2 | Match and differences | Emotional perception Theory of Mind | Different pictures are presented and children are asked to identify the emotions on the faces and those shown by the body, in order to stimulate mentalization. What is this child thinking? How does the child feel? Do you choose a similar emotion in these two scenarios? Do you select contexts and situations where you can feel the same way? | Select equal and opposite emotions | Inhibitory control Working memory Flexibility | This activity is similar to the previous one, with the exception that this one is focused on emotions. |
| 3 | How are you? Emotion-Meter | Emotional perception | First, it is explained to the child that our emotions can be graded in intensity like a thermometer. Then, the child must identify or select how he/she feels and finally they must indicate the intensity of the emotion. | Red No, green Yes: Traffic light One | Inhibitory control Working memory Flexibility Reasoning | With different colored ballons, simulating a traffic light, it is explained that red indicates that we must stop before acting, for example, when we do not know the solution of a task, or at a certain indication, for example, from the teacher, such as when we cross a street. The yellow color means that we must be careful, think before acting (How can I solve the problem or situation?), and green can be applied when we know the solution to a problem very well. Different everyday situations arise, which pose a challenge for the child to inhibit impulsive behavior. The child must identify each red, yellow or green situation based on his/her own characteristics and situations in real life. Also, when a red signal comes out, the child cannot move. Otherwise, it will be counted as an error of commission. |
| 4 | How is your engine? | Emotional perception | In this task, the child has to indicate how calm or nervous he/she feels, and the intensity of such feeling. Finally, he/she is asked to think about how he/she can feel calmer and select among the different options to relax and feel good. | Simon says | Inhibitory control Flexibility | In this task, the child is asked to follow the oral instruction given by therapist, only when the command is “Simon Says he/she must do it. Upon any other request, that is, without the “Simon Says” command, the child must not move, in order to work the inhibitory control. |
| 5 | The Volcano | Emotional perception and regulation | The child has to indicate how angry or happy he/she feels. Finally, he/she is asked to think about how he/she can feel happier, how to generate positive feelings and select among the different alternatives to relax and feel good. | Find the difference! | Inhibitory control Flexibility Reasoning Problem solving | In this task, a child is given two daily scenes, the objective is to find subtle differences. To do this, the rest of the group should give verbal clues or directions if the child asks for help to solve it. Each time it is up to a child to find the differences. |
| 6 | Emotional traffic light | Emotional regulation | Simulating a traffic light, with colored cards, it is explained that red indicates that we must stop before acting, for example, when we are angry, yellow means that we have to think how we feel and how we can solve the problem or situation, and green can be applied when we are relaxed and can act calmly. The child must identify each red, yellow or green situation based on his/her own characteristics and situations in real life | Find your treasure! | Inhibitory control Flexibility Reasoning Solving problems | The child is asked to create a collage with words, short sentences and images that reflects how he/she can help other people and positive qualities of oneself. Later, the child must select actions that help him/her at home, at school, that is, what and how makes him/her feel useful and self-competent, and how others see him/her when he/she is useful. |
| 7 | Hot soup! The Lazarillo | Emotional regulation | The child must learn to relax through breathing, which is why the metaphor of hot soup is used, in which you have to blow and practice breathing. The child has to imitate the therapist and follow the prompts to blow the hot soup. In addition, at a later stage, the child will be a “guide” who will guide the process of cooling the soup to her classmates. | The right sequence! | Flexibility Working memory | The objective of this task is for the participant to pay attention to the sequences of activities, objects or animals (because they are usually significant for children). First, an image will be shown in which several objects/animals or activity sequences will appear for 30 s, during which the patient will have to retain the displayed information. When the therapist hides the images, the child should try to construct the same sequence with other similar images. The difficulty increases proportionally with the number of distractors displayed on the cards. |
| 8 | Bubbles or stones? | Emotional regulation | Through a story, they must explain which stones are the negative feelings (anger, sadness...) and the bubbles are positive feelings (happy, peace, calm). The child is asked to indicate what the backpack of different children would be filled with in different situations. Later, he/she is asked to choose what he/she wants to fill his/her backpack with, that is, bubbles or stones | Discover the stones and touch the bubbles!! How’s your backpack? | Reasoning Planning Problem solving Flexibility | In this task, starting from the story of the stones and bubbles, questions will be asked and various response options will be provided, which the children must correctly select using logic. Difficulty increases through with number of correct options and their similarity to distractors To make it more playful, it is done in a similar way to “Goose Game”. |
| 9 | Glasses to think well!! | Emotional regulation | Thoughts and feelings are related. Sometimes a positive thought can make us feel good and negative thoughts can make us feel bad. The child must choose those positive thoughts that make him/her feel good and learn to use it in his/her daily life | The turtle | Working memory Inhibitory control Flexibility Reasoning Problem solving | In this activity, children are told the story of the turtle. They are taught how a turtle does to reflect and think when she has a problem. Finally, to reinforce what has been learned, a bookmark is made with the children with the image of a turtle. |
| 10 | Letter of thanks | Emotional regulation | Thanksgiving can be a way to generate positive feelings in others and in oneself. The child must select situations in which it is appropriate to say “thanks” and images that show gratitude and allow us to “write” a letter of thanks to a friend, teacher, or family member. | 10 point Check-In | Inhibitory control Working memory Flexibility Reasoning Planning Problem solving | This task consists of 10 stages in a countdown sequence: (10) the children have to select 10 images that make them feel relaxed; (9) select 9 things that being with a certain letter or which can be found in a certain space (classroom, schoolyard, etc); (8) select 8 known people; (7) select 7 colors; (6) choose 6 things that make them feel happy; (5) choose images that reflect relaxation and imitate them; (4) select 4 objects they hear; (3) select 3 things that are in the room that they like to play with; (2) choose two images of techniques to relax and imitate them; (1) select the current emotion and thoughts |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Ayuso, D.; Alcántara-Vázquez, P.; Almenara-García, A.; Nuñez-Camarero, I.; Triviño-Juárez, J.M.; Ariza-Vega, P.; Molina, J.-P.; González, P. Self-Regulation in Children with Neurodevelopmental Disorders “SR-MRehab: Un Colegio Emocionante”: A Protocol Study. Int. J. Environ. Res. Public Health 2020, 17, 4198. https://doi.org/10.3390/ijerph17124198
Romero-Ayuso D, Alcántara-Vázquez P, Almenara-García A, Nuñez-Camarero I, Triviño-Juárez JM, Ariza-Vega P, Molina J-P, González P. Self-Regulation in Children with Neurodevelopmental Disorders “SR-MRehab: Un Colegio Emocionante”: A Protocol Study. International Journal of Environmental Research and Public Health. 2020; 17(12):4198. https://doi.org/10.3390/ijerph17124198
Chicago/Turabian StyleRomero-Ayuso, Dulce, Pablo Alcántara-Vázquez, Ana Almenara-García, Irene Nuñez-Camarero, José Matías Triviño-Juárez, Patrocinio Ariza-Vega, José-Pascual Molina, and Pascual González. 2020. "Self-Regulation in Children with Neurodevelopmental Disorders “SR-MRehab: Un Colegio Emocionante”: A Protocol Study" International Journal of Environmental Research and Public Health 17, no. 12: 4198. https://doi.org/10.3390/ijerph17124198
APA StyleRomero-Ayuso, D., Alcántara-Vázquez, P., Almenara-García, A., Nuñez-Camarero, I., Triviño-Juárez, J. M., Ariza-Vega, P., Molina, J.-P., & González, P. (2020). Self-Regulation in Children with Neurodevelopmental Disorders “SR-MRehab: Un Colegio Emocionante”: A Protocol Study. International Journal of Environmental Research and Public Health, 17(12), 4198. https://doi.org/10.3390/ijerph17124198