Identifying Social Network Conditions that Facilitate Sedentary Behavior Change: The Benefit of Being a “Bridge” in a Group-based Intervention

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Intervention
2.3. Data Collection
2.4. Measures
2.4.1. Sedentary Behavior
2.4.2. Intervention Group Social Networks
2.4.3. Data Analysis—Network Statistics
Network Statistics
3. Results
3.1. Baseline Characteristics
3.2. Social Networks
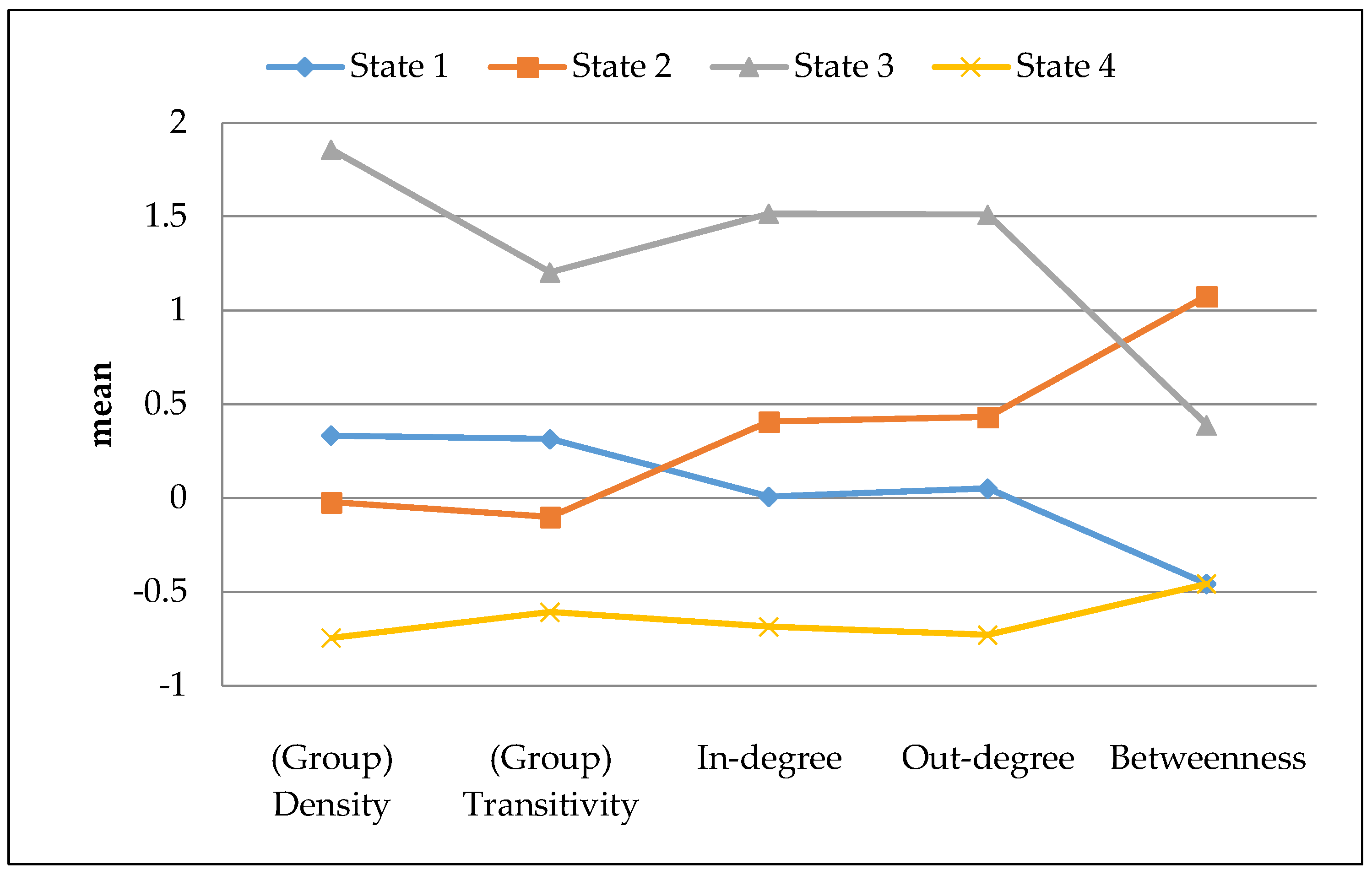
3.2.1. Network States
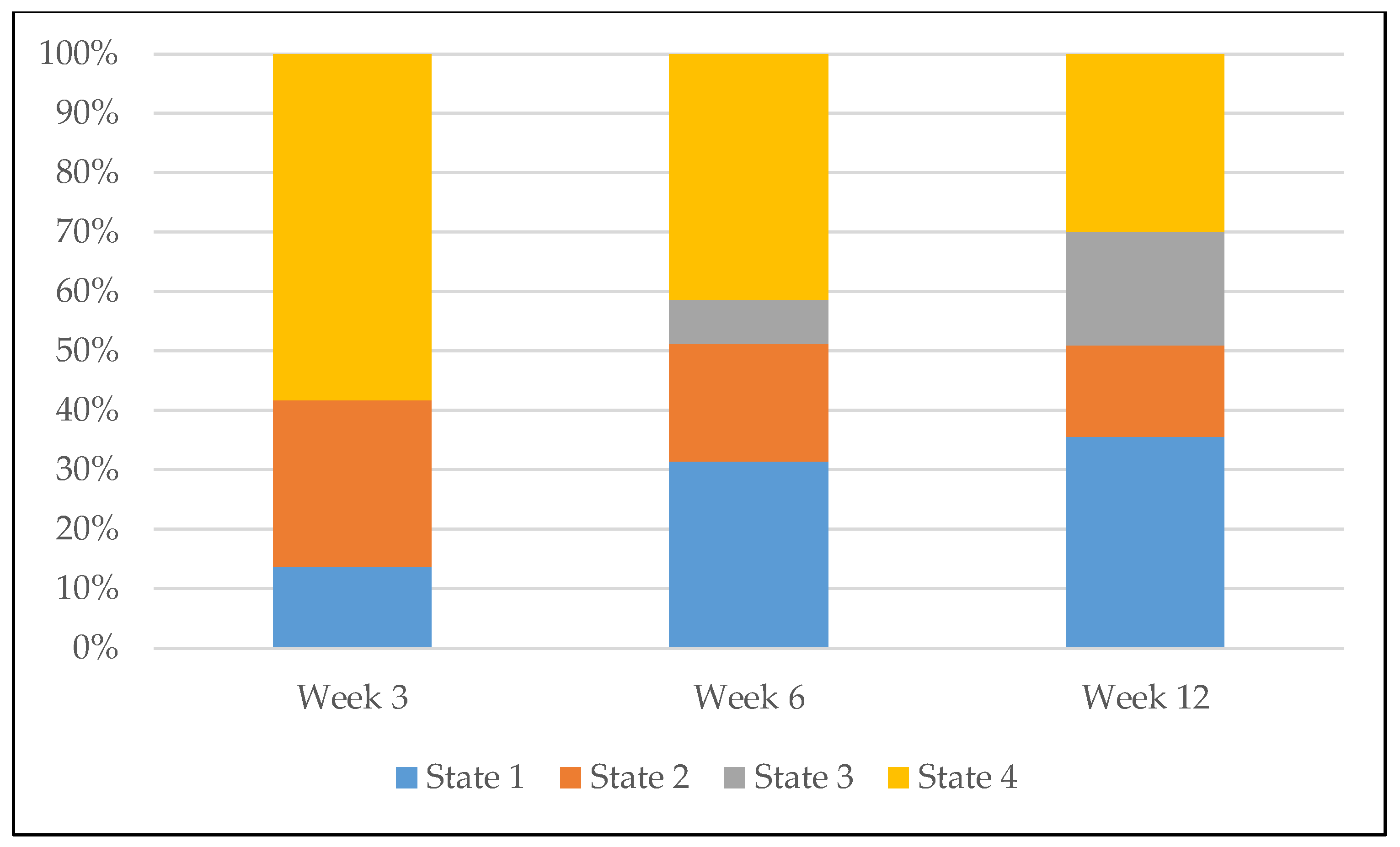
3.2.2. Network Trajectories
3.3. Predicting Sedentary Behavior from Network Trajectory
4. Discussion
4.1. Predicting Sedentary Behavior
4.2. Limitations
4.3. Implications for Intervention Design
4.4. Future Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef]
- Valente, T.W. Network interventions. Science 2012, 337, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Friedkin, N.E.; Johnsen, E.C. Social Influence Network Theory: A Sociological Examination of Small Group Dynamics; Cambridge University Press: Cambridge, United Kingdom, 2011. [Google Scholar]
- Valente, T.W. Social networks and health communication. In Handbook of Health Communication; Thompson, T.L., Parrott, R., Nussbaum, J.F., Eds.; Lawrence Erlbaum: New York, NY, USA, 2011; p. 33. [Google Scholar]
- Bahr, D.B.; Browning, R.C.; Wyatt, H.R.; Hill, J.O. Exploiting social networks to mitigate the obesity epidemic. Obesity (Silver Spring) 2009, 17, 723–728. [Google Scholar] [CrossRef] [PubMed]
- De la Haye, K.; Robins, G.; Mohr, P.; Wilson, C. How physical activity shapes, and is shaped by, adolescent friendships. Soc. Sci. Med. 2011, 73, 719–728. [Google Scholar] [CrossRef]
- Maturo, C.C.; Cunningham, S.A. Influence of friends on children’s physical activity: A review. Am. J. Public Health 2013, 103, e23–e38. [Google Scholar] [CrossRef] [PubMed]
- Gesell, S.B.; Tesdahl, E.; Ruchman, E. The distribution of physical activity in an after-school friendship network. Pediatrics 2012, 129, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Shoham, D.A.; Tesdahl, E.; Gesell, S.B. Network interventions on physical activity in an afterschool program: An agent-based social network study. Am. J. Public Health 2015, 105, S236–S243. [Google Scholar] [CrossRef]
- Hunter, R.F.; De la Haye, K.; Murray, J.M.; Badham, J.; Valente, T.W.; Clarke, M.; Kee, F. Social network interventions for health behaviours and outcomes: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002890. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef]
- Gesell, S.B.; Bess, K.D.; Barkin, S.L. Understanding the social networks that form within the context of an obesity prevention intervention. J. Obes. 2012, 2012, 749832. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of time spent in sedentary behaviors in the United States, 2003–2004. Am. J. Epidemiol 2008, 167, 875–881. [Google Scholar] [CrossRef]
- Koyanagi, A.; Stubbs, B.; Vancampfort, D. Correlates of sedentary behavior in the general population: A cross-sectional study using nationally representative data from six low- and middle-income countries. PLoS ONE 2018, 13, e0202222. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Herring, M.P.; Hallgren, M.; Koyanagi, A. Sedentary behavior and anxiety: Association and influential factors among 42,469 community-dwelling adults in six low-and middle-income countries. Gen. Hosp. Psychiatry 2018, 50, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Compernolle, S.; DeSmet, A.; Poppe, L.; Crombez, G.; De Bourdeaudhuij, I.; Cardon, G.; Van der Ploeg, H.P.; Van Dyck, D. Effectiveness of interventions using self-monitoring to reduce sedentary behavior in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 63. [Google Scholar] [CrossRef] [PubMed]
- Barkin, S.L.; Heerman, W.J.; Sommer, E.C.; Martin, N.C.; Buchowski, M.S.; Schlundt, D.; Po’e, E.K.; Burgess, L.E.; Escarfuller, J.; Pratt, C.; et al. Effect of a behavioral intervention for underserved preschool-age children on change in Body Mass Index: A randomized clinical trial. JAMA 2018, 320, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC growth charts for the United States: Methods and development. Vital Health Stat. 11 2002, 246, 1–190. [Google Scholar]
- Po’e, E.K.; Heerman, W.J.; Mistry, R.S.; Barkin, S.L. Growing Right Onto Wellness (GROW): A family-centered, community-based obesity prevention randomized controlled trial for preschool child-parent pairs. Contemp Clin. Trials 2013, 36, 436–449. [Google Scholar]
- Gesell, S.B.; Barkin, S.L.; Valente, T.W. Social network diagnostics: A tool for monitoring group interventions. Implement. Sci. 2013, 8, 116. [Google Scholar] [CrossRef]
- Wasserman, S.; Faust, K. Social Network Analysis: Methods and Applications; Cambridge University Press: Cambridge, UK, 1994. [Google Scholar]
- Matthews, C.E. Calibration of accelerometer output for adults. Med. Sci. Sports Exerc. 2005, 37, S512–S522. [Google Scholar] [CrossRef]
- Perry, B.L.; Pescosolido, B.A. Functional specificity in discussion networks: The influence of general and problem-specific networks on health outcomes. Soc. Netw. 2010, 32, 345–357. [Google Scholar] [CrossRef]
- Saint-Charles, J.; Mongeau, P. Different relationships for coping with ambiguity and uncertainty in organizations. Soc. Netw. 2009, 31, 33–39. [Google Scholar] [CrossRef]
- Carrington, P.J.; Scott, J.; Wasserman, S. Models and Methods in Social Network Analysis; Cambridge University Press: Cambridge, UK, 1994. [Google Scholar]
- Ip, E.H.; Zhang, Q.; Rejeski, W.J.; Harris, T.B.; Kritchevsky, S. Partially ordered mixed hidden Markov model for the disablement process of older adults. J. Am. Stat. Assoc. 2013, 108, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Ip, E.H.; Zhang, Q.; Schwartz, R.; Tooze, J.; Leng, X.; Han, H.; Williamson, D.A. Multi-profile hidden Markov model for mood, dietary intake, and physical activity in an intervention study of childhood obesity. Stat. Med. 2013, 32, 3314–3331. [Google Scholar] [CrossRef]
- Rejeski, W.J.; Ip, E.H.; Bertoni, A.G.; Bray, G.A.; Evans, G.; Gregg, E.W.; Zhang, Q.; Look AHEAD Research Group. Lifestyle change and mobility in obese adults with type 2 diabetes. N. Engl. J. Med. 2012, 366, 1209–1217. [Google Scholar] [CrossRef]
- Henry, T.; Gesell, S.B.; Ip, E. Social position predicting physical activity level in youth: An application of Hidden Markov Modeling on network statistics. In Social, Cultural, and Behavioral Modeling; Xu, K., Reitter, D., Lee, D., Osgood, N., Eds.; Springer: Washington, DC, USA, 2016; pp. 97–106. [Google Scholar]
- Ip, E.H.; Snow Jones, A.; Heckert, D.A.; Zhang, Q.; Gondolf, E.D. Latent Markov Model for analyzing temporal configuration for violence profiles and trajectories in a sample of batterers. Sociol. Methods Res. 2010, 39, 222–255. [Google Scholar] [CrossRef]
- Ip, E.H. Dynamic Multichain Graphical Modeling Tool. 2017. Available online: http://dmgm.wfuhs.arane.us/2017 (accessed on 30 January 2020).
- Martin, A.; Fitzsimons, C.; Jepson, R.; Saunders, D.H.; Van der Ploeg, H.P.; Teixeira, P.J.; Gray, C.M.; Mutrie, N.; EuroFIT Consortium. Interventions with potential to reduce sedentary time in adults: Systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1056–1063. [Google Scholar] [CrossRef]
- 2018 Physical Activity Guidelines Advisory Committee. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 10 June 2020).
- Long, J.C.; Cunningham, F.C.; Braithwaite, J. Bridges, brokers and boundary spanners in collaborative networks: A systematic review. BMC Health Serv. Res. 2013, 13, 158. [Google Scholar] [CrossRef]
- Burt, R.S. Structural Holes: The Social Structure of Competition; Harvard University Press: Cambridge, MA, USA, 1992. [Google Scholar]
- Selden, M.; Goodie, A.S. Review of the effects of Five Factor Model personality traits on network structures and perceptions of structure. Soc. Netw. 2018, 52, 81–99. [Google Scholar] [CrossRef]
- Josey, M.J.; Moore, S. The influence of social networks and the built environment on physical inactivity: A longitudinal study of urban-dwelling adults. Health Place 2018, 54, 62–68. [Google Scholar] [CrossRef]
- Booth, M. Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 2000, 71, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Ripley, R.; Snijders, T.A.B. Manual for SIENA Version 4.0. 2009. Available online: http://www.stats.ox.ac.uk/~snijders/siena/ (accessed on 30 January 2020).
- NetLogo. The Center for Connected Learning and Computer-Based Modeling Web Site. 1995. Available online: http://ccl.northwestern.edu/netlogo (accessed on 3 June 2020).



{kind=link}
{kind=link}
| Network State | State1 | State2 | State3 | State4 |
|---|---|---|---|---|
| State1 | 0.51 | 0.16 | 0.23 | 0.09 |
| State2 | 0.32 | 0.40 | 0.21 | 0.08 |
| State3 2 | 0.21 | 0.00 | 0.79 | 0.00 |
| State4 | 0.25 | 0.11 | 0.04 | 0.60 |
| Characteristic | Mean or Percentage (Isolated) N = 67 | Mean or Percentage (Bridge) N = 103 | Mean or Percentage (Average) N = 69 | Mean or Percentage (Popular) N = 22 | Mean or Percentage (Total) N = 261 |
|---|---|---|---|---|---|
| Gender | |||||
| Male | 2 (3.0%) | 1 (1.0%) | 1 (1.5%) | 4 (1.5%) | |
| Female | 65 (97.0%) | 102 (99.0%) | 68 (98.6%) | 22 (100%) | 257 (98.5%) |
| Age (years) | 32.8 (6.2) | 31.7 (5.9) | 32.9 (6.5) | 33.9 (6.4) | 32.5 (6.2) |
| Body mass index (kg/m2) | 29.4 (5.9) | 29.0 (6.2) | 31.4 (7.0) | 30.7 (6.7) | 29.9 (6.4) |
| Race/Ethnicity | |||||
| Hispanic | 62 (92.5%) | 98 (95.2%) | 59 (85.5%) | 19 (86.4%) | 238 (91.2%) |
| Non-Hispanic | 5 (7.5%) | 5 (4.9%) | 10 (14.5%) | 3 (13.6%) | 23 (8.8%) |
| Household Income | |||||
| $14,999 or less | 17 (25.4%) | 31 (30.1%) | 17 (24.6%) | 6 (27.3%) | 71 (27.2%) |
| $15,000–$24,999 | 21 (31.3%) | 28 (27.2%) | 20 (29.0%) | 5 (22.7%) | 74 (28.4%) |
| $25,000–$34,999 | 9 (13.4%) | 15 (14.6%) | 10 (14.5%) | 2 (9.1%) | 36 (13.8%) |
| $35,000–$49,999 | 1 (1.0%) | 3 (4.4%) | 1 (4.6%) | 5 (1.9%) | |
| $50,000–$74,999 | 1 (1.0%) | 1 (4.6%) | 2 (0.8%) | ||
| Don’t know | 20 (29.9%) | 27 (26.2%) | 19 (27.5%) | 7 (31.8%) | 73 (28.0%) |
| Education | |||||
| High school incomplete | 44 (65.7%) | 64 (62.1%) | 33 (47.8%) | 17 (77.3%) | 158 (60.5%) |
| High school degree or equivalent | 23 (34.3%) | 39 (37.9%) | 36 (52.2%) | 5 (22.7%) | 103 (39.5%) |
| Accelerometry | |||||
| Mean daily total wear time (min) | 999 (157) | 1000 (166) | 999 (147) | 1018 (143) | 1001 (156) |
| Mean daily moderate/vigorous physical activity (min) | 45.1 (40.2) | 45.4 (29.9) | 44.0 (33.4) | 72.6 (65.0) | 47.4 (38.5) |
| Mean daily sedentary behavior (min) | 469 (138) | 470 (127) | 491 (132) | 461 (124) | 475 (131) |
| Effect | Level | Estimate (min/day) | Lower 95% CL | Upper 95% CL | p-Value |
|---|---|---|---|---|---|
| Intercept | −152.76 | −315.72 | 10.2 | 0.07 | |
| Trajectory 1 | Popular | −7.94 | −51.95 | 36.06 | 0.72 |
| Bridge | −31.26 | −61.45 | −1.07 | 0.04 | |
| Average | 6.89 | −26.57 | 40.34 | 0.68 | |
| Isolated | |||||
| Mean daily sedentary behavior (min) at baseline | 0.33 | 0.23 | 0.43 | <0.01 | |
| Gender | Female | 44.89 | −48.38 | 138.17 | 0.34 |
| Male | |||||
| Age | −3.46 | −5.58 | −1.34 | <0.01 | |
| Weeks Pregnant | 0.39 | −2.46 | 3.24 | 0.79 | |
| Weeks Since Giving Birth | 0.17 | −2.82 | 3.16 | 0.91 | |
| Average total wear time in minutes/day at 12-month follow-up | 0.51 | 0.43 | 0.58 | <0.01 | |
| Study Site | Recreation Site 1 | −2.57 | −41.82 | 36.68 | 0.9 |
| Recreation Site 2 | |||||
| Group Size | 3.03 | −3.17 | 9.22 | 0.34 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gesell, S.B.; de la Haye, K.; Sommer, E.C.; Saldana, S.J.; Barkin, S.L.; Ip, E.H. Identifying Social Network Conditions that Facilitate Sedentary Behavior Change: The Benefit of Being a “Bridge” in a Group-based Intervention. Int. J. Environ. Res. Public Health 2020, 17, 4197. https://doi.org/10.3390/ijerph17124197
Gesell SB, de la Haye K, Sommer EC, Saldana SJ, Barkin SL, Ip EH. Identifying Social Network Conditions that Facilitate Sedentary Behavior Change: The Benefit of Being a “Bridge” in a Group-based Intervention. International Journal of Environmental Research and Public Health. 2020; 17(12):4197. https://doi.org/10.3390/ijerph17124197
Chicago/Turabian StyleGesell, Sabina B., Kayla de la Haye, Evan C. Sommer, Santiago J. Saldana, Shari L. Barkin, and Edward H. Ip. 2020. "Identifying Social Network Conditions that Facilitate Sedentary Behavior Change: The Benefit of Being a “Bridge” in a Group-based Intervention" International Journal of Environmental Research and Public Health 17, no. 12: 4197. https://doi.org/10.3390/ijerph17124197
APA StyleGesell, S. B., de la Haye, K., Sommer, E. C., Saldana, S. J., Barkin, S. L., & Ip, E. H. (2020). Identifying Social Network Conditions that Facilitate Sedentary Behavior Change: The Benefit of Being a “Bridge” in a Group-based Intervention. International Journal of Environmental Research and Public Health, 17(12), 4197. https://doi.org/10.3390/ijerph17124197