The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review




Abstract
1. Introduction
2. Method
2.1. Information Sources and Search Strategies
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Risk of Bias in Individual Studies
3. Results
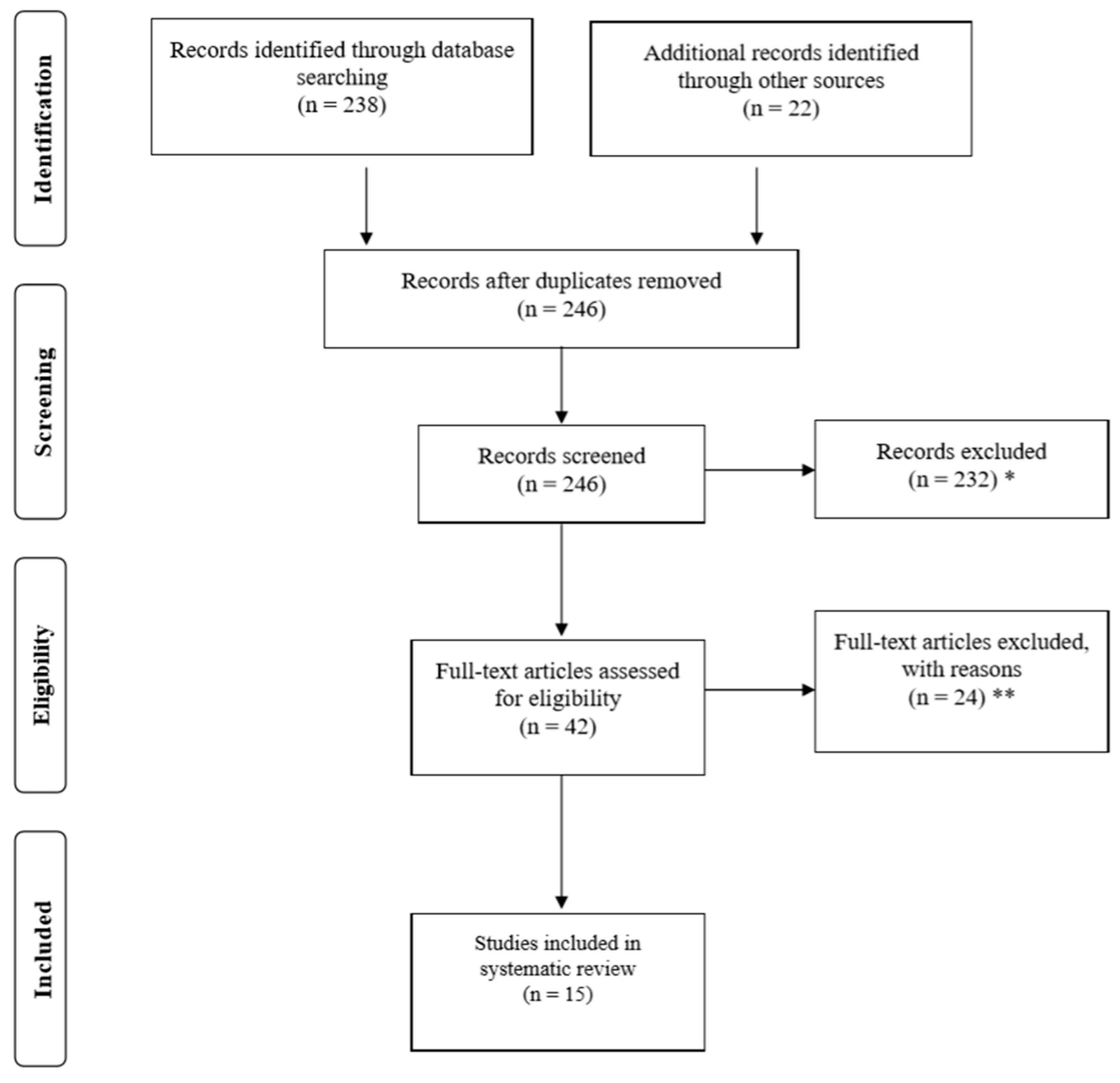
3.1. Study Selection
3.2. Quality and Risk of Bias Assessment
3.3. Data Items
3.4. Measurement Protocol
3.5. The Effectiveness of VR on Physiological Outcomes
3.6. The Effectiveness of VR on Psychological Outcomes
3.7. The Effectiveness of VR on Rehabilitative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chou, C.-H.; Hwang, C.-L.; Wu, Y.-T. Effect of Exercise on Physical Function, Daily Living Activities, and Quality of Life in the Frail Older Adults: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A.; Byrne, D. The effect of exercise on depression, anxiety and other mood states: A review. J. Psychosom. Res. 1993, 37, 565–574. [Google Scholar] [CrossRef]
- Zhu, W. If you are physically fit, you will live a longer and healthier life: An interview with Dr. Steven N. Blair. J. Sport Health Sci. 2019, 8, 524–526. [Google Scholar] [CrossRef] [PubMed]
- WHO. Fact Sheet on Physical Activity. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 23 February 2018).
- Ahn, S.J.; Fox, J. Immersive Virtual Environments, Avatars, and Agents for Health. Oxf. Res. Encycl. Commun. 2017. [Google Scholar] [CrossRef]
- Mestre, D.; Dagonneau, V.; Mercier, C.-S. Does Virtual Reality Enhance Exercise Performance, Enjoyment, and Dissociation? An Exploratory Study on a Stationary Bike Apparatus. Presence Teleoper. Virtual Environ. 2011, 20, 1–14. [Google Scholar] [CrossRef]
- Plante, T.G.; Aldridge, A.; Bogden, R.; Hanelin, C. Might virtual reality promote the mood benefits of exercise? Comput. Hum. Behav. 2003, 19, 495–509. [Google Scholar] [CrossRef]
- Pasco, D. The Potential of Using Virtual Reality Technology in Physical Activity Settings. Quest 2013, 65, 429–441. [Google Scholar] [CrossRef]
- Zeng, N.; Pope, Z.C.; Lee, J.E.; Gao, Z. Virtual Reality Exercise for Anxiety and Depression: A Preliminary Review of Current Research in an Emerging Field. J. Clin. Med. 2018, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Zeng, N.; Pope, Z.C.; Wang, R.; Yu, F. Effects of exergaming on motor skill competence, perceived competence, and physical activity in preschool children. J. Sport Health Sci. 2019, 8, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Vieira, G.D.P.; De Araujo, D.F.G.H.; Leite, M.A.A.; Orsini, M.; Correa, C.L. Realidade virtual na reabilitação física de pacientes com doença de Parkinson. J. Hum. Growth Dev. 2014, 24, 31. [Google Scholar] [CrossRef]
- Imam, B.; Jarus, T. Virtual Reality Rehabilitation from Social Cognitive and Motor Learning Theoretical Perspectives in Stroke Population. Rehabil. Res. Pr. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Juras, G.; Brachman, A.; Michalska, J.; Kamieniarz, A.; Pawłowski, M.; Hadamus, A.; Białoszewski, D.; Błaszczyk, J.; Słomka, K.J. Standards of Virtual Reality Application in Balance Training Programs in Clinical Practice: A Systematic Review. Games Health J. 2019, 8, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Valmaggia, L.; Latif, L.; Kempton, M.J.; Rus-Calafell, M.; Kemptom, M.J.; Maria, R.-C. Virtual reality in the psychological treatment for mental health problems: An systematic review of recent evidence. Psychiatry Res. Neuroimaging 2016, 236, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Pope, Z.; Lee, J.E.; Gao, Z. A systematic review of active video games on rehabilitative outcomes among older patients. J. Sport Health Sci. 2017, 6, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Han, X.-G.; Sheng, J.; Ma, S.-J. Virtual reality for improving balance in patients after stroke: A systematic review and meta-analysis. Clin. Rehabil. 2015, 30, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.G.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Pope, Z.; Gao, Z. Acute Effect of Virtual Reality Exercise Bike Games on College Students’ Physiological and Psychological Outcomes. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Podlog, L. Urban Latino Children’s Physical Activity Levels and Performance in Interactive Dance Video Games. Arch. Pediatr. Adolesc. Med. 2012, 166, 933. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gao, Z. Motivated but Not Active: The Dilemmas of Incorporating Interactive Dance into Gym Class. J. Phys. Act. Health 2012, 9, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, J.-Y.; Kim, M.-Y.; Jeon, Y.-J.; Kim, S.; Shin, J.-H. Virtual Reality Rehabilitation With Functional Electrical Stimulation Improves Upper Extremity Function in Patients With Chronic Stroke: A Pilot Randomized Controlled Study. Arch. Phys. Med. Rehabil. 2018, 99, 1447–1453. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, S.O.; De Sousa, V.P.S.; Viana, E.D.S.R. Influence of a virtual reality-based exercise protocol on the sit-to-stand activity kinematic variables in pregnant women: A randomized controlled trial. Mot. Rev. Educ. Física 2017, 23, 1–8. [Google Scholar] [CrossRef]
- Chen, C.-H.; Jeng, M.-C.; Fung, C.-P.; Doong, J.-L.; Chuang, T.-Y. Psychological benefits of virtual reality for patients in rehabilitation therapy. J. Sport Rehabil. 2009, 18, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Sohng, K.-Y. The Effect of a Virtual Reality Exercise Program on Physical Fitness, Body Composition, and Fatigue in Hemodialysis Patients. J. Phys. Sci. 2014, 26, 1661–1665. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Choi, W.; Lee, K.; Song, C.; Lee, S. Virtual Reality Training With Three-Dimensional Video Games Improves Postural Balance and Lower Extremity Strength in Community-Dwelling Older Adults. J. Aging Phys. Act. 2017, 25, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Lotan, M.; Yalon-Chamovitz, S.; Weiss, P.L. (Tamar) Virtual reality as means to improve physical fitness of individuals at a severe level of intellectual and developmental disability. Res. Dev. Disabil. 2010, 31, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Cho, G.H.; Hwangbo, G.; Shin, H.S. The Effects of Virtual Reality-based Balance Training on Balance of the Elderly. J. Phys. Sci. 2014, 26, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.; Levac, D.; Sveistrup, H. The Effects of a 5-Day Virtual-Reality Based Exercise Program on Kinematics and Postural Muscle Activity in Youth with Cerebral Palsy. Phys. Occup. Pediatr. 2018, 39, 388–403. [Google Scholar] [CrossRef] [PubMed]
- Neumann, M.M.; Moffitt, R.L. Affective and Attentional States When Running in a Virtual Reality Environment. Sports 2018, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Cohen, L.G.; Mamdani, M.; Pooyania, S.; Ploughman, M.; Cheung, D.; Shaw, J.; Hall, J.; Nord, P.; Dukelow, S.; et al. Efficacy and safety of non-immersive virtual reality exercising in stroke rehabilitation (EVREST): A randomised, multicentre, single-blind, controlled trial. Lancet Neurol. 2016, 15, 1019–1027. [Google Scholar] [CrossRef]
- Meyns, P.; Pans, L.; Plasmans, K.; Heyrman, L.; Desloovere, K.; Molenaers, G. The Effect of Additional Virtual Reality Training on Balance in Children with Cerebral Palsy after Lower Limb Surgery: A Feasibility Study. Games Health J. 2017, 6, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.-H. Effects of Virtual Reality Exercise Program on Balance in Multiple Sclerosis Patients. J. Korean Phys. 2015, 27, 61–67. [Google Scholar] [CrossRef]
- Park, J.; Lee, D.; Lee, S. Effect of Virtual Reality Exercise Using the Nintendo Wii Fit on Muscle Activities of the Trunk and Lower Extremities of Normal Adults. J. Phys. Sci. 2014, 26, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Segura-Ortí, E.; García-Testal, A. Intradialytic virtual reality exercise: Increasing physical activity through technology. Semin. Dial. 2019, 32, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Luan, X.; Tian, X.; Zhang, H.; Huang, R.; Li, N.; Chen, P.; Wang, R. Exercise as a prescription for patients with various diseases. J. Sport Health Sci. 2019, 8, 422–441. [Google Scholar] [CrossRef] [PubMed]
- Schultz, A.B.; Alexander, N.B.; Ashton-Miller, J.A. Biomechanical analyses of rising from a chair. J. Biomech. 1992, 25, 1383–1391. [Google Scholar] [CrossRef]
- Gazaneo, M.M.; de Oliveira, L.F. Alterações posturais Durante a Gestação. Rev. Bras. Ativ. Fís. Saúde 1998, 3, 13–21. [Google Scholar]
- Ribas, E.; Guirro, S. Analysis of plantar pressure and postural balance during different phases of pregnancy. Rev. Bras. Fisioter. 2007, 35, 3–8. [Google Scholar]
- Ramsey, V.K.; A Miszko, T.; Horvat, M. Muscle activation and force production in Parkinson’s patients during sit to stand transfers. Clin. Biomech. 2004, 19, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Mathiyakom, W.; McNitt-Gray, J.; Requejo, P.; Costa, K. Modifying center of mass trajectory during sit-to-stand tasks redistributes the mechanical demand across the lower extremity joints. Clin. Biomech. 2005, 20, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.E.; Lang, E.B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [PubMed]
- Holden, M.K.; Dyar, T. Virtual Environment Training: A new tool for neurorehabilitation. Neurol. Rep. 2002, 26, 62–71. [Google Scholar] [CrossRef]
- Cowan, R.L.; Frederick, B.D.; Rainey, M.; Levin, J.M.; Maas, L.C.; Bang, J.; Hennen, J.; E Lukas, S.; Renshaw, P.F. Sex differences in response to red and blue light in human primary visual cortex: A bold fMRI study. Psychiatry Res. Neuroimaging 2000, 100, 129–138. [Google Scholar] [CrossRef]
- Ruuskanen, J.M.; Parkatti, T. Physical Activity and Related Factors Among Nursing Home Residents. J. Am. Geriatr. Soc. 1994, 42, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Temple, V.A. Barriers, enjoyment, and preference for physical activity among adults with intellectual disability. Int. J. Rehabil. Res. 2007, 30, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Ijntema, H.; Meyerbröker, K.; Emmelkamp, P.M. Can virtual reality exposure therapy gains be generalized to real-life? A meta-analysis of studies applying behavioral assessments. Behav. Res. 2015, 74, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Farren, G.L.; Zhang, T.; Gu, X.; Thomas, K.T. Sedentary behavior and physical activity predicting depressive symptoms in adolescents beyond attributes of health-related physical fitness. J. Sport Health Sci. 2018, 7, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zeng, N.; Pope, Z.C.; McDonough, D.J.; Gao, Z. Acute Effects of Immersive Virtual Reality Exercise on Young Adults’ Situational Motivation. J. Clin. Med. 2019, 8, 1947. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Articles | Randomization | Control | Pre–Post | Retention | Mission Data | Power Analysis | Validity Measure | Follow-Up | Score | Effectiveness |
|---|---|---|---|---|---|---|---|---|---|---|
| Lee et al. [21] | + | + | + | + | + | − | + | − | 6 | YES |
| Ribeiro et al. [22] | + | + | + | + | − | − | + | − | 5 | NA |
| Chen et al. [23] | + | + | + | − | − | − | + | − | 4 | YES |
| Cho et al. [24] | + | + | + | + | + | + | + | − | 7 | YES |
| Lee et al. [25] | + | + | + | + | + | + | + | − | 7 | YES |
| Lotan et al. [26] | + | + | + | − | − | − | + | − | 4 | NA |
| Cho et al. [27] | + | + | + | − | − | − | − | − | 3 | YES |
| Mills et al. [28] | − | + | + | − | + | − | + | − | 4 | NA |
| Neumann et al. [29] | − | + | − | + | − | + | + | − | 4 | NA |
| Saposnik et al. [30] | + | + | + | + | − | + | + | − | 6 | NA |
| Plante et al. [7] | + | + | + | − | − | − | + | − | 4 | YES |
| Meyns et al. [31] | − | + | + | + | + | + | + | − | 6 | YES |
| Lee [32] | + | + | + | + | − | − | + | − | 5 | YES |
| Park et al. [33] | − | + | + | − | − | − | + | − | 3 | YES |
| Segura-Ortí1 et al. [34] | + | + | + | − | − | + | + | − | 5 | YES |
| Reference | Sample | Testing/Setting | Outcomes/Instrument | Exposure | Dose | Finding |
|---|---|---|---|---|---|---|
| Lee et al. [21] 2018, Korea | RCT; N = 48 (chronic stroke); Intervention (VR + FES) = 20 (49.5 ± 13.7 years); Control (FES) = 21 (46.1 ± 13.0 years). | Baseline, week 2, 4, 8; Stroke rehabilitation. | Upper limb: the Fugl-Meyer Assessment-Upper Extremity (FMA-UE) and Wolf Motor Function Test (WMFT). | The intervention group used a VR-based wearable rehabilitation device and Functional Electrical Stimulation (FES), while the control group used FES only. | Both groups received 20 intervention sessions of 30 min on weekdays (5 times/week) over 4 weeks. | FES with VR-based rehabilitation may be more effective than cyclic FES in improving distal upper extremity gross motor performance poststroke. |
| Ribeiro et al. [22] 2017, Brazil | RCT; N = 44 (pregnant women); Control Group-2nd Trimester (CG2T) = 10; Experimental Group-2nd Trimester (EG2T) = 8; (2nd Trimester = 28.55 ± 3.83 years); Control Group-3rd Trimester (CG3T) = 10; Experimental Group-3rd Trimester (EG3T) = 16; (3rd Trimester = 29.42 ± 3.23 years). | Pre–post: laboratory. | The sit-to-stand activity kinematic variables: Qualisys Track Manager (QTM). | The intervention group used a Wii balance board (WBB) to exercise additionally, while the control group did not. | An intervention with game therapy was performed in 12 sessions of 30 min each, three times a week in 4 weeks. | The use of the Nintendo Wii Fit Plus was not able to influence sit-to-stand kinematic variables in the pregnant women. |
| Chen et al. [23] 2009, Taiwan | RCT; N = 30 (incomplete low spinal-cord injuries) (16 women and 14 men, 48.2 ± 18.07 years); Intervention = 15 (51.3 ± 15.83 years); Control = 15 (45.36 ± 14.24 years). | Pre–post; hospital laboratory. | Mood states: the Activation-Deactivation Adjective Check List (AD-ACL). | An experimental group underwent therapy with a VR-based exercise bike, and a control group underwent the therapy without VR equipment. | Acute. | A VR-based rehabilitation program can ease patients’ tension and induce calm. |
| Cho et al. [24] 2014, Korea | RCT; N = 46 (hemodialysis patients); Exercise = 23 (60.8 ± 6.9 years); Control = 23 (57.7 ± 9.5 years). | Pre–post. | Fitness (strength, flexibility, balance), body composition and fatigue. | While waiting for their dialyses, the exercise group followed a Virtual Reality Exercise Program (VREP), and the control group received only their usual care. | The VREP was accomplished using Nintendo’s Wii Fit Plus for 40 min, 3 times a week for 8 weeks. | The VR Exercise Program improves physical fitness, body composition, and fatigue in hemodialysis patients. |
| Lee et al. [25] 2017, Korea | RCT; N = 44 (community dwelling older adults); Experimental group = 21 (76.15 ± 4.55 years); Control group = 19 (75.71 ± 4.91 years). | Pre–post. | Static Balance: The Good Balance System and the one leg stance test; dynamic balance: the Berg Balance Scale (BBS); extremity strength: the sit-to-stand test. | The intervention group attended a 60-min VR training session, while the control group did not. | The virtual reality training was conducted for 60 min, twice a week for 6 weeks. | Three-dimensional video gaming technology might be beneficial for improving postural balance and lower-extremity strength in community-dwelling older adults. |
| Lotan et al. [26] 2010, Israel | RCT; N = 44 (IDD sever level); Experimental group = 20 (47.9 ± 8.6 years); Comparison groups = 24 (46.2 ± 9.3 years). | Pre–post. | Fitness: heart rate (HR). | The intervention groups did game-like exercises provided by a video capture VR system, while the control group did not. | An 8-week fitness program consisting of 2–3 30-min sessions per week. | It is not strong enough functionally to claim that this program improved physical fitness of individuals with severe intellectual disability. |
| Cho et al. [27] 2014, Korea | RCT; N = 32 (healthy elderly people) VR training group = 17 (73.1 ± 1.1 years); Control group = 15 (71.7 ± 1.2 years). | Pre–post. | Balance: the Romberg test. | The VR training group engaged in an exercise session using Wii Fit, while the control group received no intervention. | A 30-min exercise session using Wii Fit 3 times a week for 8 weeks. | Virtual reality training is effective at improving the balance of the healthy elderly. |
| Mills et al. [28] 2019, Canada | Control trial; N = 11 (7–17 years) (6 males and 5 females with GMFCS levels I and II); Interactive Rehabilitation Exercise System (IREX) group = 5; Control group = 6. | Pre–post; treatment center. | Balance: the balance testing paradigm. | Participants in the intervention group received 1 h one-on-one physiotherapist-supervised VR balance games for 5 consecutive days between assessments, while the control group received no intervention. | 60 min/day in 5 consecutive days. | There was no effect of a 5-day VR-based intervention on postural control mechanisms used in response to oscillating platform perturbations. |
| Neumann et al. [29] 2018, Australia | Causal-comparative design; N = 40; Virtual Reality group = 24 (Male = 11 Female = 13 M = 24.58 years); Neutral Images group = 16 (Male = 8 Female = 8 M = 24.37 years). | Pre–post. | Affect state: the Physical Activity Affect Scale (PAAS); Attentional States: Measure of Attentional Focus (MAF). | The VR group ran in a computer-generated VR environment that included other virtual runners, while another group ran whilst viewing neutral images. | Depends on 70% VO2MAX. | VR may not always be better than distracting attention away from exercise-related cues. |
| Saposnik et al. [30] 2016, Canada | RCT; N = 141 (stroke); VR Wii group = 59 (62 ± 13 years); Recreational activity group = 62 (62 ± 12 years). | Pre–post; rehabilitation center. | Upper extremity motor performance: the Wolf Motor Function Test (WMFT). | The VR Wii group used the Nintendo Wii gaming system to add on conventional rehabilitation, while the control group used simple recreational activities (playing cards, bingo, Jenga, or a ball game). | Ten sessions of 60 min each, over a 2-week period. | Non-immersive virtual reality as an add-on therapy to conventional rehabilitation was not superior to a recreational activity intervention in improving motor function. |
| Plante et al. [7] 2003, USA | RCT; N = 88 (38.10 ± 12.31 years) Exercise group (E) = 28 VR group (V) = 28 Exercise + VR group (E + V) = 30. | Pre–post; laboratory | Momentary mood states: the Activation-Deactivation Adjective Check List (AD-ACL). | (1) E: bicycling at a moderate intensity (60–70% maximum heart rate) on a stationary bicycle; (2) V: playing a virtual reality computer bicycle game; (3) E + V: an interactive virtual reality bicycle experience on a computer while exercising on a stationary bike at moderate intensity (60–70% maximum heart rate). | 30 min. | The combination of virtual reality and exercise might improve some of the beneficial psychological effects of exercise compared with virtual reality or exercise alone. |
| Meyns et al. [31] 2017, Belgium | Controlled trial; N = 11 (4/7 males/females with spastic CPc following rehabilitation after lower limb orthopedic surgery) (5–18 years); Intervention = 4; Control = 7. | Pre–post; rehabilitation center. | Balance: the Trunk Control Measurement Scale (TCMS). | The control group received conventional physiotherapy, while the intervention group received additional VR training. | The additional VR training was given 3 times a week for 30 min until discharge from the hospital. | Including additional VR training to conventional physiotherapy was feasible and might be promising to train sitting balance in CPc after lower limb surgery. |
| Lee [32] 2016, Korea | RCT; N = 30 (12 female, 18 male with cognitive decline); Experimental = 15 (63.8 ± 10.2 years); Control groups = 15 (65.5 ± 8.1 years). | Pre–post. | Balance abilities: the Berg Balance Scale (BBS); life quality in patients: Geriatric Depression Scale-Korean (GDS-K) and the Korean version of quality of life Alzheimer’s disease (KQOL-AD) scale. | All subjects performed a traditional cognitive rehabilitation program and the experimental group performed additional VR based video game. | Three 40-min VR based video game (Wii) sessions per week for 12 weeks. | A virtual reality-training program could improve the outcomes in terms of balance, depression, and quality of life in patients with CD. |
| Park et al. [33] 2014, Korea | Controlled trial; N = 24 (15 males, 9 females); VR exercise group (VREG) = 12 (21.9 ± 1.4 years); Stable surface exercise group (SEG) = 12 (24.3 ± 3.9 years). | Pre–post. | Muscle activities: electromyography. | The VREG used the Nintendo Wii Fit, while the SEG used a stable surface. | Three times a week for six weeks. | Virtual reality exercise using the Nintendo Wii Fit was an effective intervention for the muscle activities of the TA and MG of normal adults. |
| Segura-Ortí1 et al. [34] 2019, Spain | RCT; N = 40 (hemodialysis patients); CG (control group) = 20; VRG (VR group) = 20. | Pre–post. | Physical activity: the physical function tests, physical activity questionnaire and health-related quality of life (HRQoL). | The VR program used the non-immersive gaming intervention for the VR group, comparing the results to a non-exercising control group. | 30 min for 12 weeks. | VR exercise during hemodialysis was safe and improved physical function and HRQoL and could be performed safely toward the end of the hemodialysis session. |
| Main Pathologies | Main Function | Main Effects | ||
|---|---|---|---|---|
| Health population | Older | Balance | Induce repetition; enhance motivation; enhance enjoyment. | |
| Youngers | Muscle activities | |||
| Patient | Physiology | Hemodialysis | Fitness | |
| Stroke patient | Limbs strength | |||
| Balance | ||||
| Psychology | CPc | Relief stress | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. https://doi.org/10.3390/ijerph17114133
Qian J, McDonough DJ, Gao Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(11):4133. https://doi.org/10.3390/ijerph17114133
Chicago/Turabian StyleQian, Jiali, Daniel J. McDonough, and Zan Gao. 2020. "The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 11: 4133. https://doi.org/10.3390/ijerph17114133
APA StyleQian, J., McDonough, D. J., & Gao, Z. (2020). The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health, 17(11), 4133. https://doi.org/10.3390/ijerph17114133