Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Questionnaire Investigation
2.3.1. Demographic Information
2.3.2. Parent’s Knowledge of Free Sugar
2.3.3. Parent’s Attitude to Free Sugar
2.3.4. Parental Practice of Free Sugar
2.3.5. Classification of Knowledge, Attitude and Practice
2.4. Data Processing and Statistical Analysis
3. Results
3.1. Sociodemographic Data
3.2. Knowledge, Attitude and Practice (KAP) Related to Free Sugar
3.2.1. Free Sugar-Related Knowledge
3.2.2. Free Sugar-Related Attitude
3.2.3. Free Sugar-Related Practice
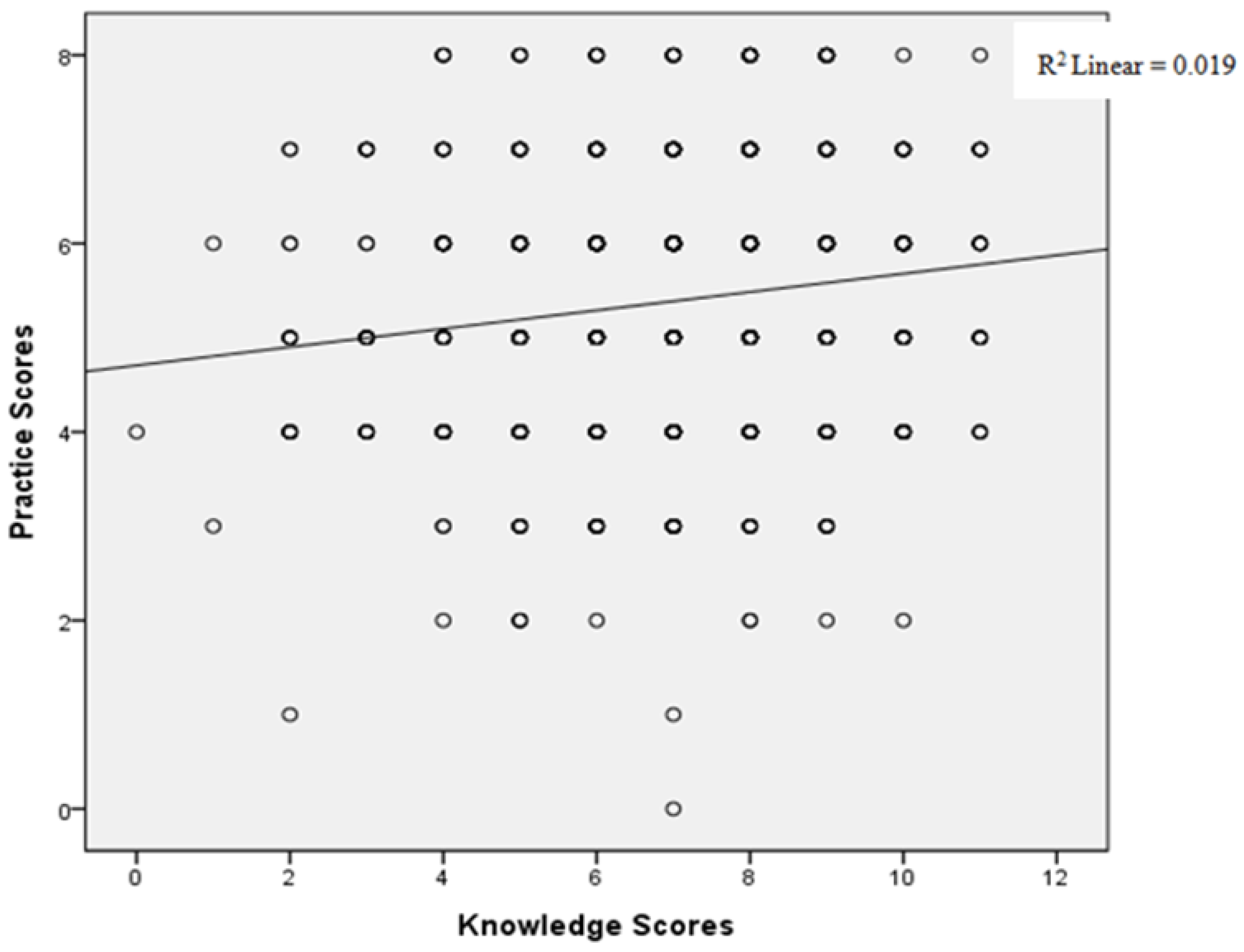
3.2.4. Correlation between Knowledge Scores and Practice Scores
3.3. Relevant Factors Affecting the Knowledge of Adolescent Parents
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mela, D.J.; Woolner, E.M. Perspective: Total, Added, or Free? What Kind of Sugars Should We Be Talking About? Adv. Nutr. 2018, 9, 63–69. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines Approved by the Guidelines Review Committee. In Guideline: Sugars Intake for Adults and Children; World Health Organization Copyright (c) World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Ferretti, F.; Mariani, M. Simple vs. Complex Carbohydrate Dietary Patterns and the Global Overweight and Obesity Pandemic. Int. J. Environ. Res. Public Health 2017, 14, 1174. [Google Scholar] [CrossRef] [PubMed]
- Kosova, E.C.; Auinger, P.; Bremer, A.A. The relationships between sugar-sweetened beverage intake and cardiometabolic markers in young children. J. Acad. Nutr. Diet. 2013, 113, 219–227. [Google Scholar] [CrossRef]
- Hoare, E.; Varsamis, P.; Owen, N.; Dunstan, D.W.; Jennings, G.L. Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk. Nutrients 2017, 9, 1075. [Google Scholar] [CrossRef]
- Johnson, R.J.; Sanchez-Lozada, L.G.; Andrews, P.; Lanaspa, M.A. Perspective: A Historical and Scientific Perspective of Sugar and Its Relation with Obesity and Diabetes. Adv. Nutr. 2017, 8, 412–422. [Google Scholar] [CrossRef]
- Fisberg, M.; Kovalskys, I.; Gomez, G.; Rigotti, A.; Sanabria, L.Y.C.; Garcia, M.C.Y.; Torres, R.G.P.; Herrera-Cuenca, M.; Zimberg, I.Z.; Koletzko, B.; et al. Total and Added Sugar Intake: Assessment in Eight Latin American Countries. Nutrients 2018, 10, 389. [Google Scholar] [CrossRef]
- Kibblewhite, R.; Nettleton, A.; McLean, R. Erratum: Estimating Free and Added Sugar Intakes in New Zealand; Nutrients 2017, 9, 1292. Nutrients 2018, 10, 638. [Google Scholar] [CrossRef]
- Ruiz, E.; Rodriguez, P.; Valero, T.; Avila, J.M.; Aranceta-Bartrina, J.; Gil, A.; Gonzalez-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Dietary Intake of Individual (Free and Intrinsic) Sugars and Food Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2017, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- Braz, M.; Assumpcao, D. Added sugar intake by adolescents: A population-based study. Cienc. Saude Colet. 2018, 24, 3237–3246. [Google Scholar] [CrossRef] [PubMed]
- Mesana, M.I.; Hilbig, A.; Androutsos, O.; Cuenca-Garcia, M.; Dallongeville, J.; Huybrechts, I.; De Henauw, S.; Widhalm, K.; Kafatos, A.; Nova, E.; et al. Dietary sources of sugars in adolescents’ diet: The HELENA study. Eur. J. Nutr. 2018, 57, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Braunack-Mayer, A. “When we were young, it really was a treat; now sugar is just the norm every day”-A qualitative study of parents’ and young adults’ perceptions and consumption of sugary drinks. Health Promot. J. Aust. 2019. [Google Scholar] [CrossRef] [PubMed]
- Su, L. Chinese Residents’ Consumption, Changes of Sugary Foods, and the Relationship with Overweight and Obesity from 2002 to 2012; Chinese Center for Disease Control and Prevention: Beijing, China, 2016. [Google Scholar]
- Jiguo, Z.; Huijun, W.; Zhu, W.; Bing, Z. Study on sugar intake of children and adolescents in 15 provinces of China in 2015. In Proceedings of the Nutrition Research and Clinical Practice—The 14th China Nutrition Science Congress and the 11th Asia Pacific Confrence on Clinical Nutrition, Nanjing, China, 19–22 September 2019. [Google Scholar]
- Azais-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Fulgoni, V.L., 3rd; Gaine, P.C.; Scott, M.O.; Ricciuto, L.; DiFrancesco, L. Association of Added Sugars Intake with Micronutrient Adequacy in US Children and Adolescents: NHANES 2009–2014. Curr. Dev. Nutr. 2019, 3, nzz126. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, G.L.M.; Kovalskys, I.; Fisberg, M.; Gomez, G.; Rigotti, A.; Sanabria, L.Y.C.; Garcia, M.C.Y.; Torres, R.G.P.; Herrera-Cuenca, M.; Zimberg, I.Z.; et al. Anthropometry, dietary intake, physical activity and sitting time patterns in adolescents aged 15–17 years: An international comparison in eight Latin American countries. BMC Pediatr. 2020, 20, 24. [Google Scholar] [CrossRef]
- Wanselius, J.; Axelsson, C.; Moraeus, L.; Berg, C.; Mattisson, I.; Larsson, C. Procedure to Estimate Added and Free Sugars in Food Items from the Swedish Food Composition Database Used in the National Dietary Survey Riksmaten Adolescents 2016–17. Nutrients 2019, 11, 1342. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; Lucan, S.C.; O’Keefe, J.H. The Evidence for Saturated Fat and for Sugar Related to Coronary Heart Disease. Prog. Cardiovasc. Dis. 2016, 58, 464–472. [Google Scholar] [CrossRef]
- Rippe, J.M.; Sievenpiper, J.L.; Le, K.A.; White, J.S.; Clemens, R.; Angelopoulos, T.J. What is the appropriate upper limit for added sugars consumption? Nutr. Rev. 2017, 75, 18–36. [Google Scholar] [CrossRef]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef]
- McGuire, S.; Ervin, R.B.; Kit, B.K.; Carroll, M.D.; Ogden, C.L. Consumption of added sugar among U.S. children and adolescents, 2005–2008. NCHS data brief no 87. Hyattsville, MD: National Center for Health Statistics. Adv. Nutr. 2012, 3, 534. [Google Scholar] [CrossRef]
- Watts, A.W.; Masse, L.C.; Barr, S.I.; Lovato, C.Y.; Hanning, R.M. Parent-child associations in selected food group and nutrient intakes among overweight and obese adolescents. J. Acad. Nutr. Diet. 2014, 114, 1580–1586. [Google Scholar] [CrossRef]
- Ha, D.H.; Do, L.G.; Spencer, A.J.; Thomson, W.M. Factors Influencing Early Feeding of Foods and Drinks Containing Free Sugars-A Birth Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1270. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, M.; Lien, N.; Grydeland, M.; Bergh, I.H.; Anderssen, S.A.; Ommundsen, Y.; Klepp, K.I.; Andersen, L.F. Intakes and perceived home availability of sugar-sweetened beverages, fruit and vegetables as reported by mothers, fathers and adolescents in the HEIA (HEalth In Adolescents) study. Public Health Nutr. 2011, 14, 2156–2165. [Google Scholar] [CrossRef] [PubMed]
- Gui, Z.H.; Zhu, Y.N.; Cai, L.; Sun, F.H. Sugar-Sweetened Beverage Consumption and Risks of Obesity and Hypertension in Chinese Children and Adolescents: A National Cross-Sectional Analysis. Nutrients 2017, 9, 1302. [Google Scholar] [CrossRef] [PubMed]
- Tierney, M.; Gallagher, A.M.; Giotis, E.S.; Pentieva, K. An Online Survey on Consumer Knowledge and Understanding of Added Sugars. Nutrients 2017, 9. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Diangelo, C.L.; Marsden, S.L.; Pasut, L.; Kitts, D.; Bellissimo, N. Knowledge of Sugars Consumption and the WHO Sugars Guideline among Canadian Dietitians and Other Health Professionals. Can. J. Diet. Pract. Res. 2020, 1–4. [Google Scholar] [CrossRef]
- Dallacker, M.; Hertwig, R.; Mata, J. Parents’ considerable underestimation of sugar and their child’s risk of overweight. Int. J. Obes. 2018, 42, 1097–1100. [Google Scholar] [CrossRef]
- Rampersaud, G.C.; Kim, H.; Gao, Z.; House, L.A. Knowledge, perceptions, and behaviors of adults concerning nonalcoholic beverages suggest some lack of comprehension related to sugars. Nutr. Res. 2014, 34, 134–142. [Google Scholar] [CrossRef]
- Bellisle, F.; Hebel, P.; Fourniret, A.; Sauvage, E. Consumption of 100% Pure Fruit Juice and Dietary Quality in French Adults: Analysis of a Nationally Representative Survey in the Context of the WHO Recommended Limitation of Free Sugars. Nutrients 2018, 10, 459. [Google Scholar] [CrossRef]
- Faith, M.S.; Dennison, B.A.; Edmunds, L.S.; Stratton, H.H. Fruit juice intake predicts increased adiposity gain in children from low-income families: Weight status-by-environment interaction. Pediatrics 2006, 118, 2066–2075. [Google Scholar] [CrossRef]
- Boles, M.; Adams, A.; Gredler, A.; Manhas, S. Ability of a mass media campaign to influence knowledge, attitudes, and behaviors about sugary drinks and obesity. Prev. Med. 2014, 67 (Suppl. 1), S40–S45. [Google Scholar] [CrossRef]
- Palmedo, P.C.; Gordon, L.M. How to be SSB-free: Assessing the attitudes and readiness for a sugar sweetened beverage-free healthcare center in the Bronx, NY. PLoS ONE 2019, 14, e0215127. [Google Scholar] [CrossRef] [PubMed]
- Evans, E.W.; Hayes, C.; Palmer, C.A.; Bermudez, O.I.; Cohen, S.A.; Must, A. Dietary intake and severe early childhood caries in low-income, young children. J. Acad. Nutr. Diet. 2013, 113, 1057–1061. [Google Scholar] [CrossRef]
- Emmett, P.M.; Jones, L.R. Diet, growth, and obesity development throughout childhood in the Avon Longitudinal Study of Parents and Children. Nutr. Rev. 2015, 73 (Suppl. 3), 175–206. [Google Scholar] [CrossRef] [PubMed]
- Fisk, C.M.; Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Robinson, S.M. Influences on the quality of young children’s diets: The importance of maternal food choices. Br. J. Nutr. 2011, 105, 287–296. [Google Scholar] [CrossRef]
- Mackey, C.; Plegue, M.A.; Deames, M.; Kittle, M.; Sonneville, K.R.; Chang, T. Family physicians’ knowledge, attitudes, and behaviors regarding the weight effects of added sugar. SAGE Open Med. 2018, 6, 2050312118801245. [Google Scholar] [CrossRef] [PubMed]
- Eck, K.M.; Dinesen, A.; Garcia, E.; Delaney, C.L. “Your Body Feels Better When You Drink Water”: Parent and School-Age Children’s Sugar-Sweetened Beverage Cognitions. Nutrients 2018, 10, 1232. [Google Scholar] [CrossRef]
- Harington, K.; Smeele, R.; Van Loon, F.; Yuan, J.; Haszard, J.J.; Drewer, A.; Venn, B.J. Desire for Sweet Taste Unchanged After Eating: Evidence of a Dessert Mentality? J. Am. Coll. Nutr. 2016, 35, 581–586. [Google Scholar] [CrossRef]
- Ares, G.; Besio, M.; Gimenez, A.; Deliza, R. Relationship between involvement and functional milk desserts intention to purchase. Influence on attitude towards packaging characteristics. Appetite 2010, 55, 298–304. [Google Scholar] [CrossRef]
- Vereecken, C.A.; Keukelier, E.; Maes, L. Influence of mother’s educational level on food parenting practices and food habits of young children. Appetite 2004, 43, 93–103. [Google Scholar] [CrossRef]
- Wijtzes, A.I.; Jansen, W.; Jansen, P.W.; Jaddoe, V.W.; Hofman, A.; Raat, H. Maternal educational level and preschool children’s consumption of high-calorie snacks and sugar-containing beverages: Mediation by the family food environment. Prev. Med. 2013, 57, 607–612. [Google Scholar] [CrossRef]
- Ahmadi, N.; Black, J.L.; Velazquez, C.E.; Chapman, G.E.; Veenstra, G. Associations between socio-economic status and school-day dietary intake in a sample of grade 5–8 students in Vancouver, Canada. Public Health Nutr. 2015, 18, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ji, M.; Zou, J.; Yuan, T.; Deng, J.; Yang, L.; Li, M.; Qin, H.; Chen, J.; Lin, Q. Effect of a Conditional Cash Transfer Program on Nutritional Knowledge and Food Practices among Caregivers of 3–5-Year-Old Left-Behind Children in the Rural Hunan Province. Int. J. Environ. Res. Public Health 2018, 15, 525. [Google Scholar] [CrossRef]
- Konig, L.M.; Ziesemer, K.; Renner, B. Quantifying Actual and Perceived Inaccuracy When Estimating the Sugar, Energy Content and Portion Size of Foods. Nutrients 2019, 11, 2425. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, M.; Hausken, S.E.; Bergh, I.H.; Grydeland, M.; Klepp, K.I.; Andersen, L.F.; Totland, T.H.; Lien, N. Changes in adolescents’ and parents’ intakes of sugar-sweetened beverages, fruit and vegetables after 20 months: Results from the HEIA study—A comprehensive, multi-component school-based randomized trial. Food Nutr. Res. 2015, 59, 25932. [Google Scholar] [CrossRef]
- Di Giacomo, D.; De Liso, G.; Ranieri, J. Self body-management and thinness in youth: Survey study on Italian girls. Health Qual. Life Outcomes 2018, 16, 120. [Google Scholar] [CrossRef] [PubMed]
- Handford, C.M.; Rapee, R.M.; Fardouly, J. The influence of maternal modeling on body image concerns and eating disturbances in preadolescent girls. Behav. Res. Ther. 2018, 100, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, P.; Adhikari, V.; Harrington, R.A.; Elhussein, A.; Briggs, A.; Rayner, M. Impact of the announcement and implementation of the UK Soft Drinks Industry Levy on sugar content, price, product size and number of available soft drinks in the UK, 2015–19: A controlled interrupted time series analysis. PLoS Med. 2020, 17, e1003025. [Google Scholar] [CrossRef]
- Lee, M.M.; Falbe, J.; Schillinger, D.; Basu, S.; McCulloch, C.E.; Madsen, K.A. Sugar-Sweetened Beverage Consumption 3 Years After the Berkeley, California, Sugar-Sweetened Beverage Tax. Am. J. Public Health 2019, 109, 637–639. [Google Scholar] [CrossRef]
- Colchero, M.A.; Rivera-Dommarco, J.; Popkin, B.M.; Ng, S.W. In Mexico, Evidence Of Sustained Consumer Response Two Years After Implementing A Sugar-Sweetened Beverage Tax. Health Aff. 2017, 36, 564–571. [Google Scholar] [CrossRef]
- Acton, R.B.; Jones, A.C.; Kirkpatrick, S.I.; Roberto, C.A.; Hammond, D. Taxes and front-of-package labels improve the healthiness of beverage and snack purchases: A randomized experimental marketplace. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 46. [Google Scholar] [CrossRef]
- Von Philipsborn, P.; Stratil, J.M.; Burns, J.; Busert, L.K.; Pfadenhauer, L.M.; Polus, S.; Holzapfel, C.; Hauner, H.; Rehfuess, E. Environmental interventions to reduce the consumption of sugar-sweetened beverages and their effects on health. Cochrane Database Syst. Rev. 2019, 6, Cd012292. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Frequency | Percentage | Mean | SD |
|---|---|---|---|---|
| Parents | ||||
| Gender | ||||
| Male | 336 | 29.6 | ||
| Female | 800 | 70.4 | ||
| Age | 41.76 | 5.27 | ||
| Ethnicity | ||||
| Han nationality | 1095 | 96.4 | ||
| Minority | 41 | 3.6 | ||
| Education level | ||||
| Primary school | 26 | 2.3 | ||
| Junior high school | 280 | 24.6 | ||
| High school/vocational school | 484 | 42.6 | ||
| University and above | 346 | 30.5 | ||
| Monthly household income per capita | ||||
| ≤1000 yuan | 23 | 2.0 | ||
| 1001–3000 yuan | 203 | 17.9 | ||
| 3001–5000 yuan | 310 | 27.3 | ||
| 5001–7000 yuan | 231 | 20.3 | ||
| ≥7001 yuan | 369 | 32.5 | ||
| BMI | ||||
| Wasting | 67 | 5.9 | ||
| Normal | 768 | 67.6 | ||
| Overweight | 256 | 22.5 | ||
| Obese | 45 | 4.0 | ||
| Adolescent | ||||
| Gender | ||||
| Male | 597 | 52.6 | ||
| Female | 539 | 47.4 | ||
| Age | 13.57 | 0.69 | ||
| Only child | 653 | 57.5 | ||
| BMI | ||||
| Wasting | 45 | 4.0 | ||
| Normal | 786 | 69.2 | ||
| Overweight | 169 | 14.6 | ||
| Obese | 136 | 12.0 | ||
| Total | 1136 | 100 |
| Items | Mean (P25, P75) | >P75 (n %) |
|---|---|---|
| Knowledge | 7.04 (6, 8) | 241 (21.2%) |
| Attitude | 5.17 (5, 6) | 580 (51.1%) |
| Practice | 5.39 (4, 6) | 218 (19.2%) |
| Questions | Correct Responses | |
|---|---|---|
| Frequency | Percentage | |
| Know the definition of free sugar. | 84 | 7.4 |
| Know the recommended daily sugar intake in The Chinese Dietary Guidelines. | 386 | 34.0 |
| Know recommended ratio of free sugar to total daily energy. (≤10%) | 346 | 30.5 |
| Knowledge of free sugar content in food. | ||
| Biscuits, cakes | 892 | 78.5 |
| Vegetable, fruit | 967 | 85.1 |
| Sugar-sweetened beverages | 944 | 83.1 |
| 100% fruit juice | 312 | 27.5 |
| Honey | 692 | 60.9 |
| Do you think that excessive intake of sugary drinks will affect the growth and development of adolescents? (YES) | 1024 | 90.1 |
| What diseases do you think excessive sugar intake may be related to? | ||
| Dental caries | 856 | 75.4 |
| Overweight or obese | 1021 | 89.9 |
| Chronic diseases in adulthood | 474 | 41.7 |
| Items | Agree | Neutral | Disagree |
|---|---|---|---|
| Eating too much sugary food is not good. | 717 (63.1) | 373 (32.8) | 46 (4.0) |
| Drinking too much sugar-sweetened beverages is addictive. | 910 (80.1) | 40 (3.5) | 186 (16.4) |
| Teenagers should reduce the consumption of sugary foods. | 1028 (90.5) | 57 (5.0) | 51 (4.5) |
| Drinks and desserts should limit the amount of sugar added. | 1061 (93.4) | 39 (3.4) | 36 (3.2) |
| Limiting sugary foods is good for your child’s health. | 1068 (94.0) | 39 (3.4) | 29 (2.6) |
| Parents should consciously control children’s intake of sugary foods. | 1094 (96.3) | 36 (3.2) | 6 (0.6) |
| Questions | Good behavior | |
|---|---|---|
| Frequency | Percentage | |
| You had bought three or more drinks for your child in the past month. | 67 | 5.9 |
| You had stored drinks at home in the past month. | 417 | 36.7 |
| You had bought three or more desserts for your child in the past month. | 97 | 8.5 |
| You had stored desserts at home in the past month. | 688 | 60.6 |
| You did not use drinks as a reward when your child is doing well. | 1072 | 94.4 |
| You did not use dessert as a reward when your child is doing well. | 1025 | 90.2 |
| You were conscious of avoiding buying sugar-sweetened beverages in front of your child. | 394 | 34.7 |
| You were conscious to avoid drinking sugar-sweetened beverages in front of your child. | 422 | 37.1 |
| Factors | b | Waldχ2 | p | OR (95%CI) |
|---|---|---|---|---|
| Parents gender | 0.563 | 10.383 | 0.001 ∗∗∗ | 1.756 (1.247, 2.473) |
| Education level of parents | 0.350 | 13.462 | 0.000 ∗∗∗ | 1.419 (1.177, 1.710) |
| Students gender(girl) | 0.290 | 3.864 | 0.049 ∗ | 1.336 (1.001, 1.783) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Q.; Lin, Q.; Yang, Q.; Sun, M.; Liu, H.; Yang, L. Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition. Int. J. Environ. Res. Public Health 2020, 17, 4003. https://doi.org/10.3390/ijerph17114003
Tang Q, Lin Q, Yang Q, Sun M, Liu H, Yang L. Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition. International Journal of Environmental Research and Public Health. 2020; 17(11):4003. https://doi.org/10.3390/ijerph17114003
Chicago/Turabian StyleTang, Qiong, Qian Lin, Qiping Yang, Minghui Sun, Hanmei Liu, and Lina Yang. 2020. "Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition" International Journal of Environmental Research and Public Health 17, no. 11: 4003. https://doi.org/10.3390/ijerph17114003
APA StyleTang, Q., Lin, Q., Yang, Q., Sun, M., Liu, H., & Yang, L. (2020). Knowledge, Attitude, and Practice of Adolescent Parents on Free Sugar and Influencing Factors about Recognition. International Journal of Environmental Research and Public Health, 17(11), 4003. https://doi.org/10.3390/ijerph17114003