Association between Ambient Air Pollution and Hospital Length of Stay among Children with Asthma in South Texas

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Data Sources
2.2. Measurement
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Limitations
4.2. Public Health and Policy Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Lag Days Pre-Admission | Coefficient (r) |
|---|---|
| Lag0 | 0.092 * |
| Lag0–1 | 0.105 ** |
| Lag0–2 | 0.115 ** |
| Lag0–3 | 0.102 ** |
| Lag0–4 | 0.100 ** |
| Lag0–5 | 0.103 ** |
| Lag0–6 | 0.114 ** |
| Lag0–7 | 0.123 ** |
References
- Van Tien, T.; Phuong, H.T.; Mathauer, I.; Phuong, N.T.K. A health financing review of Vietnam; World Health Organization: Geneva, Switzerland, 2011; pp. 1–46. Available online: https://www.who.int/health_financing/documents/oasis_f_11-vietnam.pdf (accessed on 1 December 2019).
- Macy, M.L.; Stanley, R.M.; Lozon, M.M.; Sasson, C.; Gebremariam, A.; Davis, M.M. Trends in high-turnover stays among children hospitalized in the United States, 1993-2003. Pediatrics 2009, 123, 996–1002. [Google Scholar] [CrossRef]
- Fassl, B.A.; Nkoy, F.L.; Stone, B.L.; Srivastava, R.; Simon, T.D.; Uchida, D.A.; Koopmeiners, K.; Greene, T.; Cook, L.J.; Maloney, C.G. The Joint Commission Children’s Asthma Care Quality Measures and Asthma Readmissions. Pediatrics 2012, 130, 482–491. [Google Scholar] [CrossRef]
- Luo, L.; Ren, J.; Zhang, F.; Zhang, W.; Li, C.; Qiu, Z.; Huang, D. The effects of air pollution on length of hospital stay for adult patients with asthma. Int. J. Health Plan. Manag. 2018, 33, e751–e767. [Google Scholar] [CrossRef]
- Soyiri, I.; Reidpath, D.D.; Sarran, C. Asthma Length of Stay in Hospitals in London 2001–2006: Demographic, Diagnostic and Temporal Factors. PLoS ONE 2011, 6, e27184. [Google Scholar] [CrossRef]
- González-Barcala, F.-J.; Calvo-Alvarez, U.; Salgado-Castro, F.-J.; Facal, D.; Garcia-Sanz, M.-T.; Muñoz, X.; García-Couceiro, N.; Paz-Neira, O.; San-Jose, E.; Valdes-Cuadrado, L.; et al. Asthma exacerbations: Factors related to longer hospital stay. Acta Clin. Belg. 2017, 72, 379–384. [Google Scholar] [CrossRef]
- Shanley, L.; Lin, H.; Flores, G. Factors associated with length of stay for pediatric asthma hospitalizations. J. Asthma 2014, 52, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Calhoun, W.J.; Pei, Y.V.; Chasm, R.M.; Youngquist, S.T.; Bittner, J.C.; Camargo, C.A. Sex differences in hospital length of stay in children and adults hospitalized for asthma exacerbation. Ann. Allergy Asthma Immunol. 2015, 115, 533–535.e1. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Nochioka, K.; Hataya, H.; Sakakibara, H.; Terakawa, T.; Testa, M. Burden of Obesity on Pediatric Inpatients with Acute Asthma Exacerbation in the United States. J. Allergy Clin. Immunol. Pr. 2016, 4, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.-Y.; Ding, H.; Jiang, L.-N.; Chen, S.-W.; Zheng, J.-P.; Qiu, M.; Zhou, Y.-X.; Chen, Q.; Guan, W.-J. Association between Air Pollutants and Asthma Emergency Room Visits and Hospital Admissions in Time Series Studies: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef]
- Grineski, S.E.; Staniswalis, J.G.; Bulathsinhala, P.; Peng, Y.; Gill, T.E. Hospital admissions for asthma and acute bronchitis in El Paso, Texas: Do age, sex, and insurance status modify the effects of dust and low wind events? Environ. Res. 2011, 111, 1148–1155. [Google Scholar] [CrossRef]
- Esposito, S.; Tenconi, R.; Lelii, M.; Preti, V.; Nazzari, E.; Consolo, S.; Patria, M.F. Possible molecular mechanisms linking air pollution and asthma in children. BMC Pulm. Med. 2014, 14, 31. [Google Scholar] [CrossRef] [PubMed]
- Dietert, R.R.; Etzel, R.A.; Chen, D.; Halonen, M.; Holladay, S.D.; Jarabek, A.M.; Landreth, K.; Peden, D.B.; Pinkerton, K.; Smialowicz, R.J.; et al. Workshop to identify critical windows of exposure for children’s health: Immune and respiratory systems work group summary. Environ. Health Perspect 2000, 108, 483–490. [Google Scholar] [PubMed]
- Bateson, T.F.; Schwartz, J. Children’s Response to Air Pollutants. J. Toxicol. Environ. Health Part A 2007, 71, 238–243. [Google Scholar] [CrossRef]
- Makri, A.; Stilianakis, N.I. Vulnerability to air pollution health effects. Int. J. Hyg. Environ. Health 2008, 211, 326–336. [Google Scholar] [CrossRef]
- Ross, K.R.; Chmiel, J.F.; Ferkol, T. The impact of the Clean Air Act. J. Pediatr. 2012, 161, 781–786. [Google Scholar] [CrossRef]
- Gilliland, P.F. Outdoor air pollution, genetic susceptibility, and asthma management: Opportunities for intervention to reduce the burden of asthma. Pediatrics 2009, 123, S168–S173. [Google Scholar] [CrossRef]
- Nhung, N.T.T.; Schindler, C.; Dien, T.M.; Probst-Hensch, N.; Perez, L.; Künzli, N. Acute effects of ambient air pollution on lower respiratory infections in Hanoi children: An eight-year time series study. Environ. Int. 2018, 110, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.-Y.; Chan, C.-K.; Wu, C.-Y.; Phan, D.-V.; Chan, C.-L. The Short-Term Effects of Ambient Air Pollutants on Childhood Asthma Hospitalization in Taiwan: A National Study. Int. J. Environ. Res. Public Health 2019, 16, 203. [Google Scholar] [CrossRef]
- Roy, A.; Sheffield, P.; Wong, K.; Trasande, L. The Effects of Outdoor Air Pollutants on the Costs of Pediatric Asthma Hospitalizations in the United States, 1999 to 2007. Med. Care 2011, 49, 810–817. [Google Scholar] [CrossRef]
- Nhung, N.T.T.; Schindler, C.; Dien, T.M.; Probst-Hensch, N.; Künzli, N. Association of ambient air pollution with lengths of hospital stay for hanoi children with acute lower-respiratory infection, 2007–2016. Environ. Pollut. 2019, 247, 752–762. [Google Scholar] [CrossRef]
- Ramirez, A.G.; Thompson, I.M.; Vela, L. The South Texas Health Status Review: A Health Disparities Roadmap; Springer: Berlin/Heidelberg, Germany, 2013; pp. 1–155. [Google Scholar]
- Driscoll Children’s Hospital; About Us. 2019. Available online: https://www.driscollchildrens.org/about-us (accessed on 1 August 2019).
- Federal Communications Commission; Census Tracts and Tract Codes. 2015. Available online: https://transition.fcc.gov/form477/Geo/more_about_census_tracts.pdf (accessed on 2 April 2020).
- Michigan State University; Finding Census Tract Data: About Census Tracts. Available online: https://libguides.lib.msu.edu/c.php?g=96120&p=625755 (accessed on 2 April 2020).
- Centers for Disease Control and Prevention. National Environmental Public Health Tracking Network. 2018. Available online: www.cdc.gov/ephtracking (accessed on 10 July 2019).
- Centers for Disease Control and Prevention. Outdoor Air: Monitor + Model Air Data. Available online: https://ephtracking.cdc.gov/showAirMonModData (accessed on 1 August 2019).
- Nkoy, F.L.; Stone, B.; Knighton, A.J.; Fassl, B.A.; Johnson, J.M.; Maloney, C.G.; Savitz, L.A. Neighborhood Deprivation and Childhood Asthma Outcomes, Accounting for Insurance Coverage. Hosp. Pediatr. 2018, 8, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Bloomberg, G.R.; Banister, C.; Sterkel, R.; Epstein, J.; Bruns, J.; Swerczek, L.; Wells, S.; Yan, Y.; Garbutt, J.M. Socioeconomic, family, and pediatric practice factors that affect level of asthma control. Pediatrics 2009, 123, 829–835. [Google Scholar] [CrossRef]
- Anis, A.H.; Lynd, L.D.; Wang, X.-H.; King, G.; Spinelli, J.J.; Fitzgerald, M.; Bai, T.; Paré, P. Double trouble: Impact of inappropriate use of asthma medication on the use of health care resources. Can. Med. Assoc. J. 2001, 164, 625–631. [Google Scholar]
- Baek, J.; Huang, K.; Conner, L.; Tapangan, N.; Xu, X.; Carrillo, G. Effects of the home-based educational intervention on health outcomes among primarily Hispanic children with asthma: A quasi-experimental study. BMC Public Health 2019, 19, 912. [Google Scholar] [CrossRef]
- Bodaghkhani, E.; Mahdavian, M.; MacLellan, C.; Farrell, A.; Asghari, S. Effects of Meteorological Factors on Hospitalizations in Adult Patients with Asthma: A Systematic Review. Can. Respir. J. 2019, 2019, 3435103–3435111. [Google Scholar] [CrossRef]
- Environmental Protection Agency. Ground-level Ozone Pollution: Ground-level Ozone Basics. 2018. Available online: http://www.epa.gov/ground-level-ozone-pollution/ground-level-ozone-basics#effects (accessed on 19 May 2020).
- Glick, A.F.; Tomopoulos, S.; Fierman, A.H.; Elixhauser, A.; Trasande, L. Association Between Outdoor Air Pollution Levels and Inpatient Outcomes in Pediatric Pneumonia Hospitalizations, 2007 to 2008. Acad. Pediatr. 2019, 19, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Chen, Q.; Zheng, X.; Li, Y.; Han, M.; Liu, T.; Xiao, J.; Guo, L.; Zeng, W.; Zhang, J.; et al. Effects of ambient ozone concentrations with different averaging times on asthma exacerbations: A meta-analysis. Sci. Total. Environ. 2019, 691, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Jalaludin, B.; Khalaj, B.; Sheppeard, V.; Morgan, G. Air pollution and ED visits for asthma in Australian children: A case-crossover analysis. Int. Arch. Occup. Environ. Health 2007, 81, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Strickland, M.J.; Darrow, L.A.; Klein, M.; Flanders, W.D.; Sarnat, J.A.; Waller, L.A.; Sarnat, S.E.; Mulholland, J.A.; Tolbert, P.E. Short-term Associations between Ambient Air Pollutants and Pediatric Asthma Emergency Department Visits. Am. J. Respir. Crit. Care Med. 2010, 182, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Gleason, J.A.; Bielory, L.; Fagliano, J.A. Associations between ozone, PM2.5, and four pollen types on emergency department pediatric asthma events during the warm season in New Jersey: A case-crossover study. Environ. Res. 2014, 132, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.; Campbell, M.J.; Bianchi, S.; Murray-Thomas, T. Seasonality of medical contacts in school-aged children with asthma: Association with school holidays. Public Health 2011, 125, 769–776. [Google Scholar] [CrossRef]
- Scheuerman, O.; Meyerovitch, J.; Marcus, N.; Hoffer, V.; Batt, E.; Garty, B.Z. The September epidemic or asthma in Israel. J. Asthma 2009, 46, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Julious, S.; Osman, L.; Jiwa, M. Increases in asthma hospital admissions associated with the end of the summer vacation for school-age children with asthma in two cities from England and Scotland. Public Health 2007, 121, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Hua, J.; Yin, Y.; Peng, L.; Du, L.; Geng, F.; Zhu, L. Acute effects of black carbon and PM2.5 on children asthma admissions: A time-series study in a Chinese city. Sci. Total. Environ. 2014, 481, 433–438. [Google Scholar] [CrossRef]
- Ding, L.; Zhu, D.; Peng, D.; Zhao, Y. Air pollution and asthma attacks in children: A case–crossover analysis in the city of Chongqing, China. Environ. Pollut. 2017, 220, 348–353. [Google Scholar] [CrossRef]
- Berrocal, V.J.; Gelfand, A.E.; Holland, D.M. A Spatio-Temporal Downscaler for Output from Numerical Models. J. Agric. Boil. Environ. Stat. 2010, 15, 176–197. [Google Scholar] [CrossRef]
- Carroll, C.L.; Uygungil, B.; Zucker, A.R.; Schramm, C. Identifying an At-Risk Population of Children with Recurrent Near-Fatal Asthma Exacerbations. J. Asthma 2010, 47, 460–464. [Google Scholar] [CrossRef]
- Schoetz, D.J.; Bockler, M.; Rosenblatt, M.S.; Malhotra, S.; Roberts, P.L.; Murray, J.J.; Coller, J.A.; Rusin, L.C. "Ideal" length of stay after colectomy: Whose ideal? Dis. Colon. Rectum 1997, 40, 806–810. [Google Scholar] [CrossRef]
- O’Keefe, G.E.; Jurkovich, G.J.; Maier, R.V. Defining Excess Resource Utilization and Identifying Associated Factors for Trauma Victims. J. Trauma: Inj. Infect. Crit. Care 1999, 46, 473–478. [Google Scholar] [CrossRef]
- Holloway, S.; Sarosi, G.; Kim, L.; Nwariaku, F.; O’Keefe, G.; Hynan, L.; Jones, C.; Anthony, T. Health-related quality of life and postoperative length of stay for patients with colorectal cancer. J. Surg. Res. 2002, 108, 273–278. [Google Scholar] [CrossRef]
- Brasel, K.J.; Lim, H.J.; Nirula, R.; Weigelt, J.A. Length of stay: An appropriate quality measure? Arch. Surg. 2007, 142, 461–465. [Google Scholar] [CrossRef]
- Carrillo, G.; Spence-Almaguer, E.; Lucio, R.; Chong-Menard, B.; Smith, K. Improving Asthma in Hispanic Families Through a Home-Based Educational Intervention. Pediatr. Allergy Immunol. Pulmonol. 2015, 28, 165–171. [Google Scholar] [CrossRef]
- Campbell, J.D.; Brooks, M.; Hosokawa, P.; Robinson, J.; Song, L.; Krieger, J. Community Health Worker Home Visits for Medicaid-Enrolled Children With Asthma: Effects on Asthma Outcomes and Costs. Am. J. Public Health 2015, 105, 2366–2372. [Google Scholar] [CrossRef]

| Variables | Total † | High (LOS > 2) † | Low (LOS ≤ 2) † | p-Value |
|---|---|---|---|---|
| Total | 711 (100.0) | 160 (100.0) | 551 (100.0) | |
| Age (continuous) | 9.2 ± 3.5 (5, 18) | 9.5 ± 3.6 (5, 18) | 9.1 ± 3.5 (5, 18) | 0.152 |
| Age | 0.451 | |||
| 5–11 years old | 536 (75.4) | 117 (73.1) | 419 (76.0) | |
| 12–18 years old | 175 (24.6) | 43 (26.9) | 132 (24.0) | |
| Gender | 0.925 | |||
| Female | 291 (40.9) | 66 (41.3) | 225 (40.8) | |
| Male | 420 (59.1) | 94 (58.7) | 326 (59.2) | |
| Ethnicity | 0.305 | |||
| Hispanic | 527 (74.2) | 123 (77.4) | 404 (73.3) | |
| Non-Hispanic | 183 (25.8) | 36 (22.6) | 147 (26.7) | |
| Insurance | 0.733 | |||
| Public (Medicaid) | 488 (68.7) | 108 (67.5) | 380 (69.0) | |
| Private | 205 (28.8) | 49 (30.6) | 156 (28.3) | |
| Self-pay | 18 (2.5) | 3 (1.9) | 15 (2.7) | |
| Use of Medication | 0.206 | |||
| Yes | 654 (92.0) | 151 (94.4) | 503 (91.3) | |
| No | 57 (8.0) | 9 (5.6) | 48 (8.7) | |
| Family History of Asthma or Respiratory Diseases | 0.053 | |||
| Yes | 352 (49.5) | 90 (56.2) | 262 (47.6) | |
| No | 359 (50.5) | 70 (43.8) | 289 (52.4) | |
| Recipient of Asthma Education | 0.265 | |||
| Yes | 677 (95.2) | 155 (96.9) | 522 (94.7) | |
| No | 34 (4.8) | 5 (3.1) | 29 (5.3) | |
| Admission Day | 0.199 | |||
| Weekday (Mon –Thu) | 431 (60.6) | 90 (56.2) | 341 (61.9) | |
| Weekend (Fri–Sun) | 280 (39.4) | 70 (43.8) | 210 (38.1) | |
| Admission Season | 0.526 | |||
| Warm (May–October) | 273 (38.4) | 58 (36.3) | 215 (39.0) | |
| Cold (November–April) | 438 (61.6) | 102 (63.7) | 336 (61.0) | |
| Year | 0.081 | |||
| 2010 | 166 (23.3) | 48 (30.0) | 118 (21.4) | |
| 2011 | 133 (18.7) | 34 (21.1) | 99 (18.0) | |
| 2012 | 154 (21.7) | 26 (16.3) | 128 (23.2) | |
| 2013 | 125 (17.6) | 26 (16.3) | 99 (18.0) | |
| 2014 | 133 (18.7) | 26 (16.3) | 107 (19.4) |
| Lag Days Pre-Admission | PM2.5 (µg/m3) | Ozone (ppb) | Temperature (°C) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | Max | Mean | SD | Min | Max | Mean | SD | Min | Max | |
| Lag0 | 8.43 | 3.41 | 2.48 | 27.28 | 37.43 | 11.92 | 10.09 | 75.23 | 20.71 | 6.78 | 1.06 | 33.33 |
| Lag0–1 | 8.45 | 2.89 | 2.96 | 23.01 | 37.66 | 11.14 | 13.74 | 75.29 | 20.65 | 6.64 | 2.11 | 32.92 |
| Lag0–2 | 8.47 | 2.50 | 3.57 | 19.96 | 37.80 | 10.42 | 15.69 | 73.35 | 20.65 | 6.52 | 1.78 | 32.41 |
| Lag0–3 | 8.48 | 2.24 | 3.80 | 17.85 | 37.84 | 9.74 | 16.84 | 73.58 | 20.66 | 6.45 | 1.02 | 32.08 |
| Lag0–4 | 8.47 | 2.10 | 3.75 | 16.46 | 37.87 | 9.24 | 17.39 | 72.57 | 20.65 | 6.37 | 2.99 | 32.1 |
| Lag0–5 | 8.46 | 1.96 | 3.88 | 16.71 | 37.81 | 8.85 | 17.48 | 71.85 | 20.63 | 6.34 | 5.82 | 32.15 |
| Lag0–6 | 8.45 | 1.85 | 4.08 | 16.46 | 37.72 | 8.39 | 17.73 | 69.02 | 20.62 | 6.33 | 6.33 | 32.24 |
| Lag0–7 | 8.47 | 1.78 | 4.38 | 16.01 | 37.61 | 8.05 | 17.93 | 67.21 | 20.61 | 6.33 | 6.63 | 32.37 |
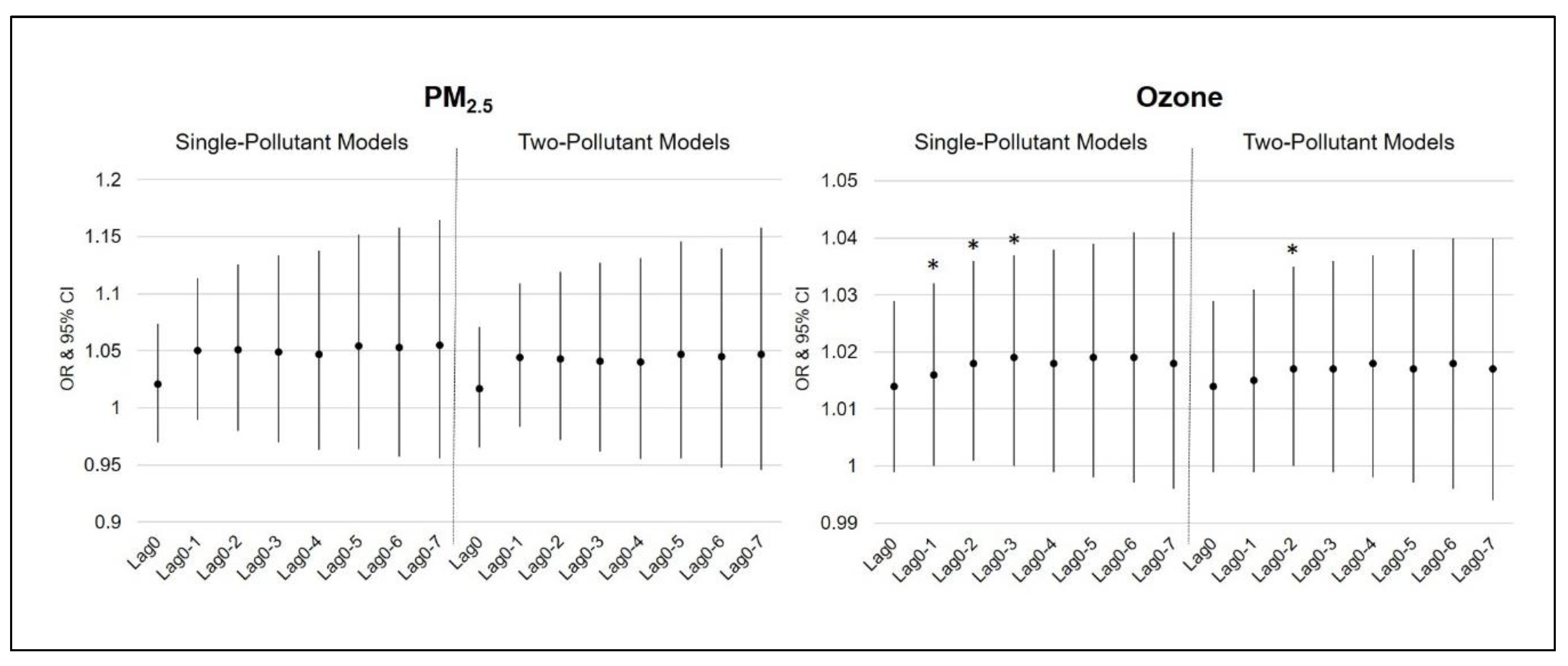
| Lag Days Pre-Admission. | Single-Pollutant Models | Two-Pollutant Models | ||||||
|---|---|---|---|---|---|---|---|---|
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.021 (0.970, 1.074) | 0.427 | 1.014 (0.999, 1.029) | 0.059 | 1.017 (0.965, 1.071) | 0.528 | 1.014 (0.999, 1.029) | 0.068 |
| Lag0–1 | 1.050 (0.989, 1.114) | 0.112 | 1.016 (1.000, 1.032) | 0.049 * | 1.044 (0.983, 1.109) | 0.162 | 1.015 (0.999, 1.031) | 0.069 |
| Lag0–2 | 1.051 (0.980, 1.126) | 0.162 | 1.018 (1.001, 1.036) | 0.033 * | 1.043 (0.972, 1.119) | 0.247 | 1.017 (1.000, 1.035) | 0.048 * |
| Lag0–3 | 1.049 (0.970, 1.134) | 0.231 | 1.019 (1.000, 1.037) | 0.048 * | 1.041 (0.962, 1.127) | 0.317 | 1.017 (0.999, 1.036) | 0.063 |
| Lag0–4 | 1.047 (0.963, 1.138) | 0.279 | 1.018 (0.999, 1.038) | 0.063 | 1.040 (0.955, 1.131) | 0.366 | 1.018 (0.998, 1.037) | 0.079 |
| Lag0–5 | 1.054 (0.964, 1.152) | 0.246 | 1.019 (0.998, 1.039) | 0.076 | 1.047 (0.956, 1.146) | 0.321 | 1.017 (0.997, 1.038) | 0.095 |
| Lag0–6 | 1.053 (0.957, 1.158) | 0.288 | 1.019 (0.997, 1.041) | 0.086 | 1.045 (0.948, 1.140) | 0.376 | 1.018 (0.996, 1.040) | 0.107 |
| Lag0–7 | 1.055 (0.956, 1.165) | 0.287 | 1.018 (0.996, 1.041) | 0.113 | 1.047 (0.946, 1.158) | 0.372 | 1.017 (0.994, 1.040) | 0.141 |
| Single-Pollutant Models | ||||||||
| Lag Days | 5–11 Years Old | 12–18 Years Old | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.052 (0.992, 1.116) | 0.092 | 1.015 (0.998, 1.033) | 0.091 | 0.926 (0.821, 1.046) | 0.262 | 1.012 (0.983, 1.042) | 0.422 |
| Lag0–1 | 1.086 (1.012, 1.165) | 0.022 * | 1.017 (0.998, 1.036) | 0.081 | 0.941 (0.822, 1.076) | 0.373 | 1.014 (0.982, 1.047) | 0.403 |
| Lag0–2 | 1.077 (0.993, 1.167) | 0.074 | 1.019 (0.999, 1.040) | 0.063 | 0.958 (0.821, 1.118) | 0.590 | 1.013 (0.979, 1.048) | 0.467 |
| Lag0–3 | 1.077 (0.984, 1.179) | 0.107 | 1.020 (0.998, 1.043) | 0.072 | 0.930 (0.780, 1.109) | 0.422 | 1.008 (0.972, 1.045) | 0.672 |
| Lag0–4 | 1.079 (0.979, 1.189) | 0.124 | 1.019 (0.996, 1.044) | 0.096 | 0.922 (0.769, 1.104) | 0.375 | 1.008 (0.970, 1.048) | 0.670 |
| Lag0–5 | 1.089 (0.982, 1.209) | 0.107 | 1.018 (0.994, 1.044) | 0.148 | 0.929 (0.771, 1.121) | 0.443 | 1.015 (0.975, 1.056) | 0.474 |
| Lag0–6 | 1.109 (0.975, 1.219) | 0.129 | 1.019 (0.993, 1.046) | 0.159 | 0.922 (0.756, 1.126) | 0.426 | 1.015 (0.973, 1.058) | 0.485 |
| Lag0–7 | 1.095 (0.974, 1.231) | 0.127 | 1.018 (0.991, 1.047) | 0.193 | 0.928 (0.757, 1.138) | 0.475 | 1.014 (0.971, 1.059) | 0.525 |
| Two-Pollutant Models | ||||||||
| Lag Days | 5–11 Years Old | 12–18 Years Old | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.047 (0.986, 1.112) | 0.134 | 1.014 (0.996, 1.032) | 0.131 | 0.922 (0.816, 1.042) | 0.194 | 1.014 (0.984, 1.045) | 0.363 |
| Lag0–1 | 1.080 (1.005, 1.160) | 0.035 * | 1.015 (0.996, 1.034) | 0.134 | 0.935 (0.816, 1.071) | 0.332 | 1.016 (0.983, 1.050) | 0.354 |
| Lag0–2 | 1.069 (0.984, 1.160) | 0.114 | 1.017 (0.997, 1.038) | 0.096 | 0.951 (0.814, 1.112) | 0.530 | 1.014 (0.979, 1.050) | 0.425 |
| Lag0–3 | 1.069 (0.975, 1.172) | 0.154 | 1.018 (0.996, 1.041) | 0.103 | 0.928 (0.778, 1.107) | 0.408 | 1.009 (0.972, 1.047) | 0.636 |
| Lag0–4 | 1.071 (0.971, 1.182) | 0.171 | 1.018 (0.995, 1.042) | 0.132 | 0.919 (0.768, 1.102) | 0.364 | 1.010 (0.970, 1.050) | 0.637 |
| Lag0–5 | 1.083 (0.974, 1.204) | 0.140 | 1.016 (0.992, 1.042) | 0.197 | 0.924 (0.765, 1.116) | 0.410 | 1.016 (0.976, 1.059) | 0.435 |
| Lag0–6 | 1.083 (0.967, 1.214) | 0.165 | 1.017 (0.991, 1.044) | 0.165 | 0.912 (0.745, 1.117) | 0.374 | 1.018 (0.975, 1.063) | 0.418 |
| Lag0–7 | 1.090 (0.968, 1.227) | 0.153 | 1.017 (0.989, 1.045) | 0.237 | 0.914 (0.741, 1.127) | 0.400 | 1.018 (0.973, 1.065) | 0.433 |
| Single-Pollutant Models | ||||||||
| Lag Days | Female | Male | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.023 (0.944, 1.108) | 0.579 | 1.015 (0.991, 1.038) | 0.221 | 1.021 (0.953, 1.093) | 0.557 | 1.011 (0.992, 1.032) | 0.231 |
| Lag0–1 | 1.076 (0.979, 1.183) | 0.130 | 1.016 (0.991, 1.042) | 0.218 | 1.044 (0.963, 1.132) | 0.298 | 1.015 (0.994, 1.036) | 0.168 |
| Lag0–2 | 1.096 (0.984, 1.221) | 0.096 | 1.020 (0.993, 1.047) | 0.141 | 1.031 (0.937, 1.135) | 0.534 | 1.017 (0.994, 1.041) | 0.142 |
| Lag0–3 | 1.085 (0.961, 1.223) | 0.187 | 1.023 (0.994, 1.052) | 0.118 | 1.034 (0.928, 1.151) | 0.546 | 1.015 (0.990, 1.041) | 0.241 |
| Lag0–4 | 1.093 (0.958, 1.247) | 0.184 | 1.027 (0.996, 1.058) | 0.085 | 1.022 (0.914, 1.143) | 0.701 | 1.012 (0.986, 1.039) | 0.367 |
| Lag0–5 | 1.131 (0.985, 1.299) | 0.080 | 1.030 (0.998, 1.064) | 0.067 | 1.006 (0.890, 1.136) | 0.928 | 1.010 (0.983, 1.038) | 0.474 |
| Lag0–6 | 1.135 (0.983, 1.309) | 0.083 | 1.033 (0.999, 1.069) | 0.060 | 0.995 (0.872, 1.135) | 0.940 | 1.009 (0.981, 1.038) | 0.533 |
| Lag0–7 | 1.106 (0.955, 1.282) | 0.180 | 1.030 (0.994, 1.067) | 0.097 | 1.017 (0.886, 1.167) | 0.813 | 1.010 (0.980, 1.041) | 0.517 |
| Two-Pollutant Models | ||||||||
| Lag Days | Female | Male | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.017 (0.938, 1.103) | 0.680 | 1.039 (0.991, 1.038) | 0.224 | 1.018 (0.949, 1.091) | 0.616 | 1.011 (0.992, 1.032) | 0.247 |
| Lag0–1 | 1.066 (0.968, 1.175) | 0.193 | 1.013 (0.987, 1.039) | 0.335 | 1.042 (0.960, 1.131) | 0.326 | 1.014 (0.993, 1.036) | 0.182 |
| Lag0–2 | 1.083 (0.969, 1.210) | 0.160 | 1.016 (0.989, 1.044) | 0.240 | 1.026 (0.932, 1.131) | 0.596 | 1.017 (0.994, 1.040) | 0.153 |
| Lag0–3 | 1.067 (0.942, 1.208) | 0.308 | 1.019 (0.991, 1.049) | 0.187 | 1.032 (0.926, 1.149) | 0.572 | 1.015 (0.989, 1.040) | 0.249 |
| Lag0–4 | 1.071 (0.933, 1.228) | 0.331 | 1.023 (0.992, 1.055) | 0.143 | 1.021 (0.912, 1.143) | 0.716 | 1.012 (0.986, 1.039) | 0.372 |
| Lag0–5 | 1.107 (0.958, 1.278) | 0.168 | 1.025 (0.992, 1.058) | 0.140 | 1.005 (0.889, 1.136) | 0.937 | 1.010 (0.983, 1.038) | 0.475 |
| Lag0–6 | 1.109 (0.955, 1.287) | 0.176 | 1.027 (0.993, 1.064) | 0.124 | 0.994 (0.870, 1.135) | 0.928 | 1.009 (0.981, 1.039) | 0.532 |
| Lag0–7 | 1.082 (0.927, 1.262) | 0.317 | 1.026 (0.989, 1.063) | 0.164 | 1.016 (0.884, 1.166) | 0.828 | 1.010 (0.980, 1.040) | 0.521 |
| Single-Pollutant Models | ||||||||
| Lag Days | Warm Season | Cold Season | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.025 (0.947, 1.109) | 0.544 | 1.014 (0.993, 1.036) | 0.198 | 1.022 (0.954, 1.095) | 0.538 | 1.027 (1.003, 1.053) | 0.028 * |
| Lag0–1 | 1.046 (0.961, 1.139) | 0.298 | 1.021 (0.999, 1.044) | 0.058 | 1.063 (0.973, 1.161) | 0.178 | 1.022 (0.995, 1.051) | 0.115 |
| Lag0–2 | 1.070 (0.972, 1.178) | 0.167 | 1.027 (1.004, 1.051) | 0.020 * | 1.035 (0.932, 1.150) | 0.520 | 1.021 (0.990, 1.053) | 0.180 |
| Lag0–3 | 1.094 (0.984, 1.216) | 0.097 | 1.032 (1.007, 1.057) | 0.012 * | 1.001 (0.887, 1.130) | 0.983 | 1.018 (0.984, 1.053) | 0.309 |
| Lag0–4 | 1.105 (0.987, 1.237) | 0.083 | 1.036 (1.009, 1.063) | 0.009 ** | 0.983 (0.863, 1.120) | 0.798 | 1.015 (0.979, 1.053) | 0.421 |
| Lag0–5 | 1.122 (0.996, 1.265) | 0.058 | 1.036 (1.008, 1.066) | 0.012 * | 0.977 (0.847, 1.127) | 0.750 | 1.017 (0.978, 1.058) | 0.397 |
| Lag0–6 | 1.121 (0.989, 1.269) | 0.073 | 1.037 (1.006, 1.069) | 0.018 * | 0.977 (0.835, 1.142) | 0.770 | 1.021 (0.979, 1.064) | 0.337 |
| Lag0–7 | 1.131 (0.995, 1.286) | 0.059 | 1.035 (1.003, 1.068) | 0.030 * | 0.959 (0.812, 1.132) | 0.621 | 1.025 (0.980, 1.072) | 0.283 |
| Two-Pollutant Models | ||||||||
| Lag Days | Warm Season | Cold Season | ||||||
| PM2.5 | Ozone | PM2.5 | Ozone | |||||
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Lag0 | 1.009 (0.927, 1.099) | 0.830 | 1.013 (0.991, 1.036) | 0.251 | 1.034 (0.964, 1.109) | 0.344 | 1.029 (1.004, 1.055) | 0.021 * |
| Lag0–1 | 1.023 (0.933, 1.121) | 0.633 | 1.019 (0.996, 1.043) | 0.100 | 1.076 (0.983, 1.178) | 0.111 | 1.026 (0.997, 1.055) | 0.075 |
| Lag0–2 | 1.038 (0.935, 1.152) | 0.484 | 1.024 (1.000, 1.049) | 0.047 * | 1.043 (0.938, 1.160) | 0.432 | 1.022 (0.991, 1.055) | 0.158 |
| Lag0–3 | 1.058 (0.942, 1.187) | 0.343 | 1.028 (1.002, 1.054) | 0.036 * | 1.009 (0.893, 1.141) | 0.877 | 1.018 (0.984, 1.054) | 0.304 |
| Lag0–4 | 1.066 (0.942, 1.205) | 0.310 | 1.031 (1.003, 1.059) | 0.028 * | 0.989 (0.868, 1.129) | 0.878 | 1.015 (0.978, 1.053) | 0.436 |
| Lag0–5 | 1.083 (0.951, 1.232) | 0.229 | 1.030 (1.001, 1.061) | 0.043 * | 0.985 (0.853, 1.139) | 0.843 | 1.016 (0.977, 1.057) | 0.419 |
| Lag0–6 | 1.081 (0.945, 1.238) | 0.253 | 1.031 (0.999, 1.063) | 0.057 | 0.987 (0.843, 1.157) | 0.876 | 1.020 (0.978, 1.064) | 0.354 |
| Lag0–7 | 1.096 (0.954, 1.257) | 0.194 | 1.028 (0.995, 1.062) | 0.096 | 0.973 (0.822, 1.152) | 0.751 | 1.023 (0.978, 1.071) | 0.316 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.; Kash, B.A.; Xu, X.; Benden, M.; Roberts, J.; Carrillo, G. Association between Ambient Air Pollution and Hospital Length of Stay among Children with Asthma in South Texas. Int. J. Environ. Res. Public Health 2020, 17, 3812. https://doi.org/10.3390/ijerph17113812
Baek J, Kash BA, Xu X, Benden M, Roberts J, Carrillo G. Association between Ambient Air Pollution and Hospital Length of Stay among Children with Asthma in South Texas. International Journal of Environmental Research and Public Health. 2020; 17(11):3812. https://doi.org/10.3390/ijerph17113812
Chicago/Turabian StyleBaek, Juha, Bita A. Kash, Xiaohui Xu, Mark Benden, Jon Roberts, and Genny Carrillo. 2020. "Association between Ambient Air Pollution and Hospital Length of Stay among Children with Asthma in South Texas" International Journal of Environmental Research and Public Health 17, no. 11: 3812. https://doi.org/10.3390/ijerph17113812
APA StyleBaek, J., Kash, B. A., Xu, X., Benden, M., Roberts, J., & Carrillo, G. (2020). Association between Ambient Air Pollution and Hospital Length of Stay among Children with Asthma in South Texas. International Journal of Environmental Research and Public Health, 17(11), 3812. https://doi.org/10.3390/ijerph17113812