The Benefits of Physical Exercise on Mental Disorders and Quality of Life in Substance Use Disorders Patients. Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Method
2.1. Research Strategies
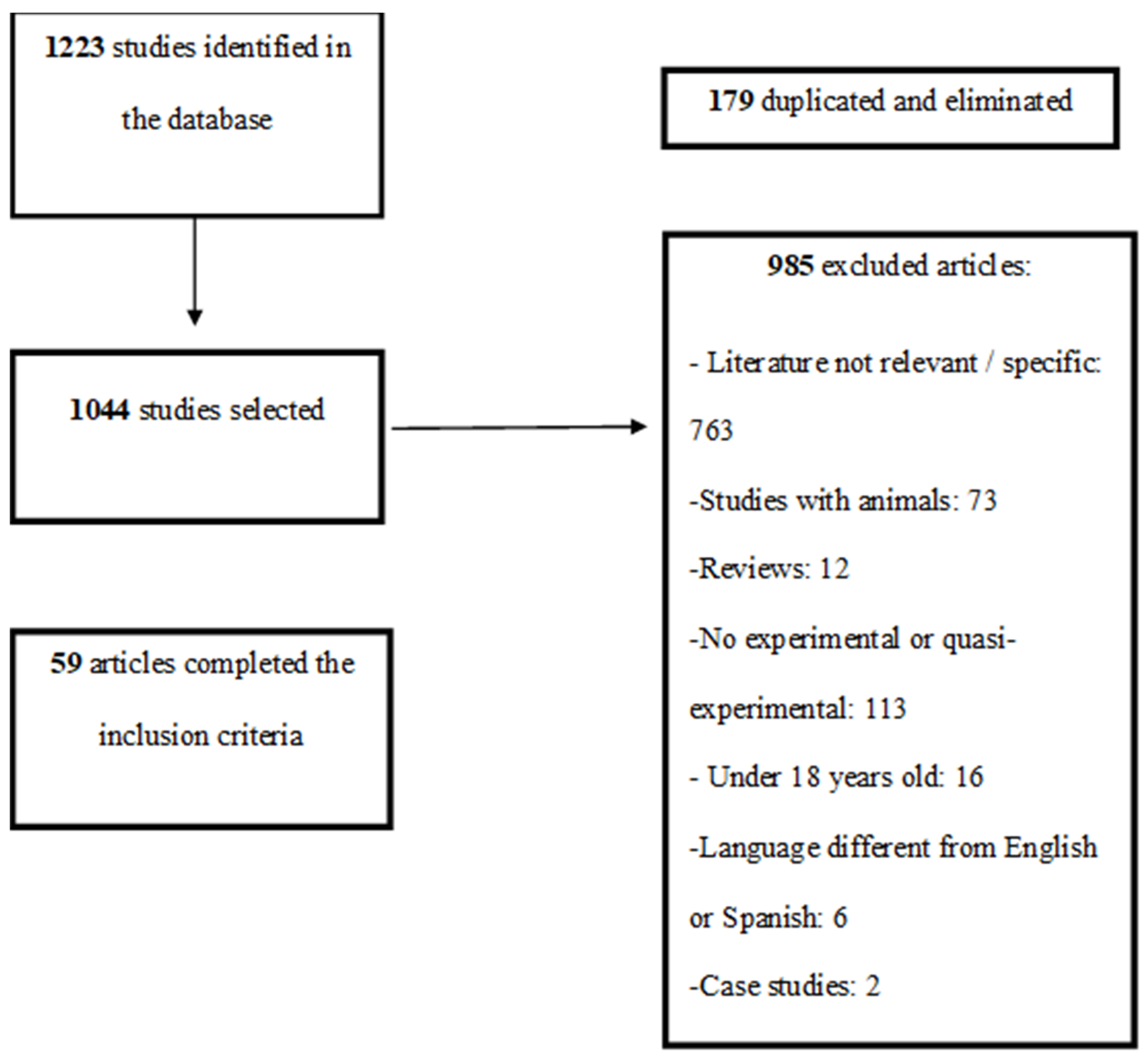
2.2. Selection of Studies
2.3. Data Extraction
2.4. Quality Analysis of the Studies
2.5. Meta-Analysis
3. Results
3.1. Descriptive Characteristics of the Selected Studies
3.2. Methodological Quality of the Selected Studies
3.3. Acute Effect of the Exercise
3.4. Long-Term Effect of Exercise
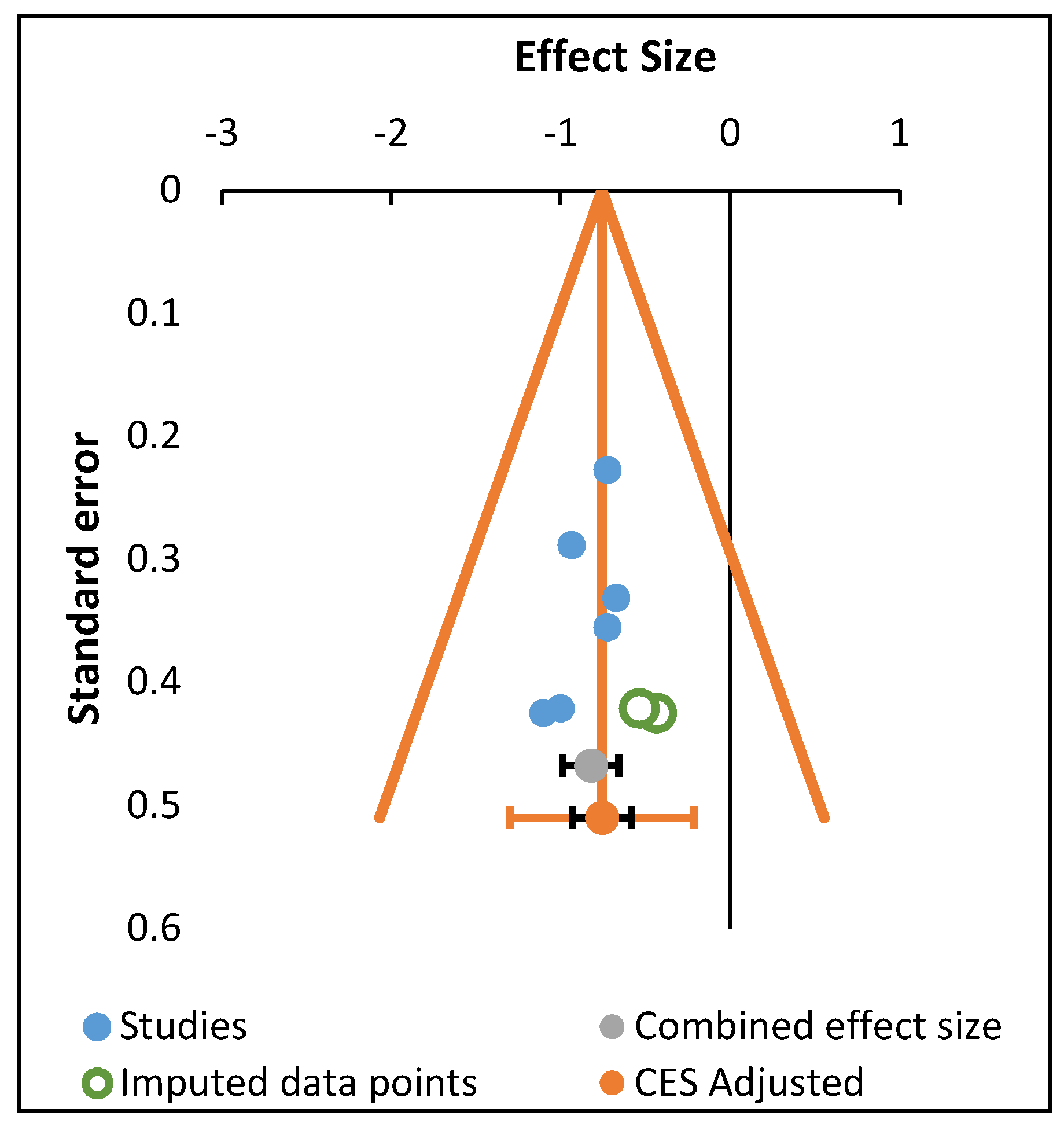
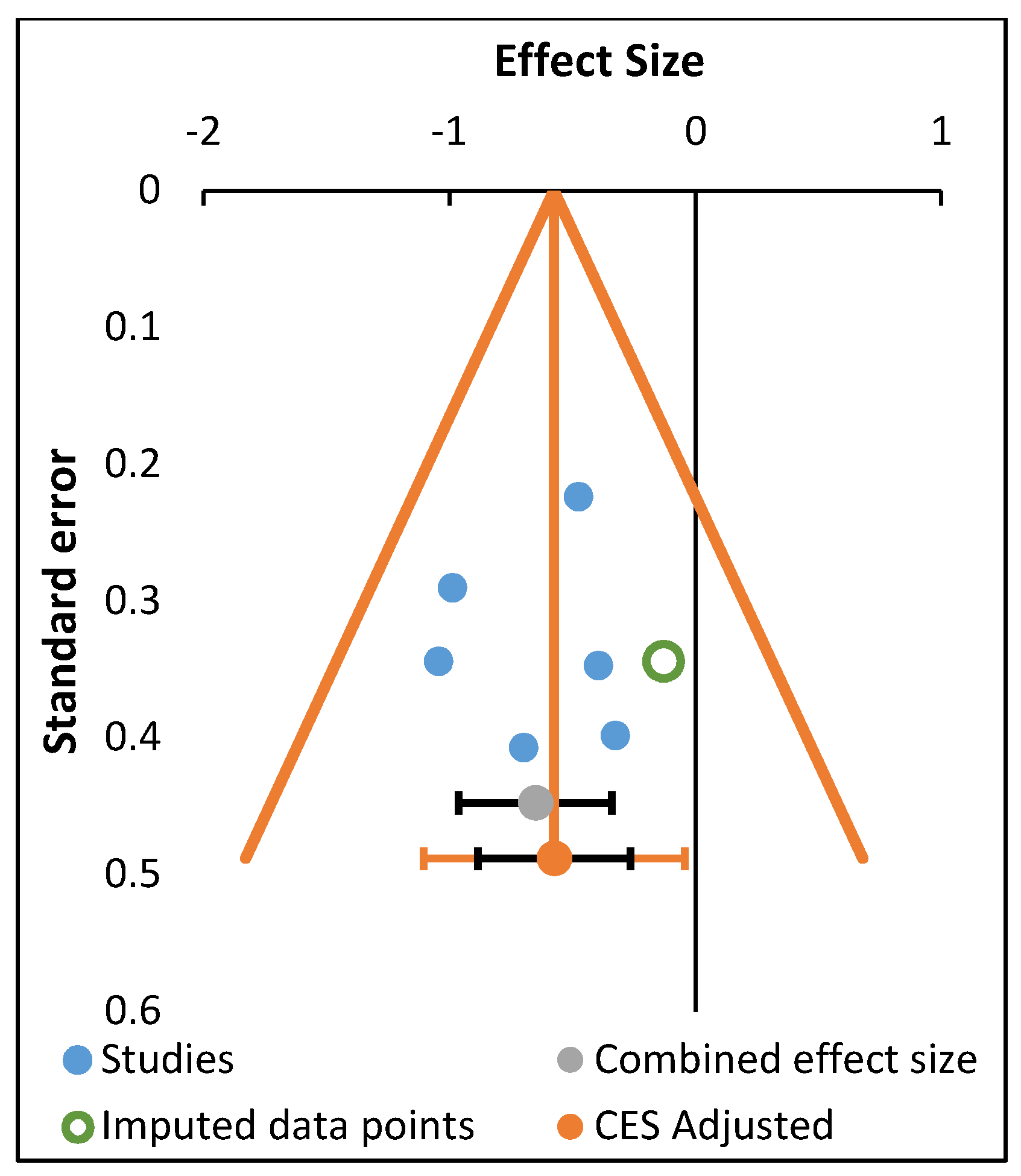
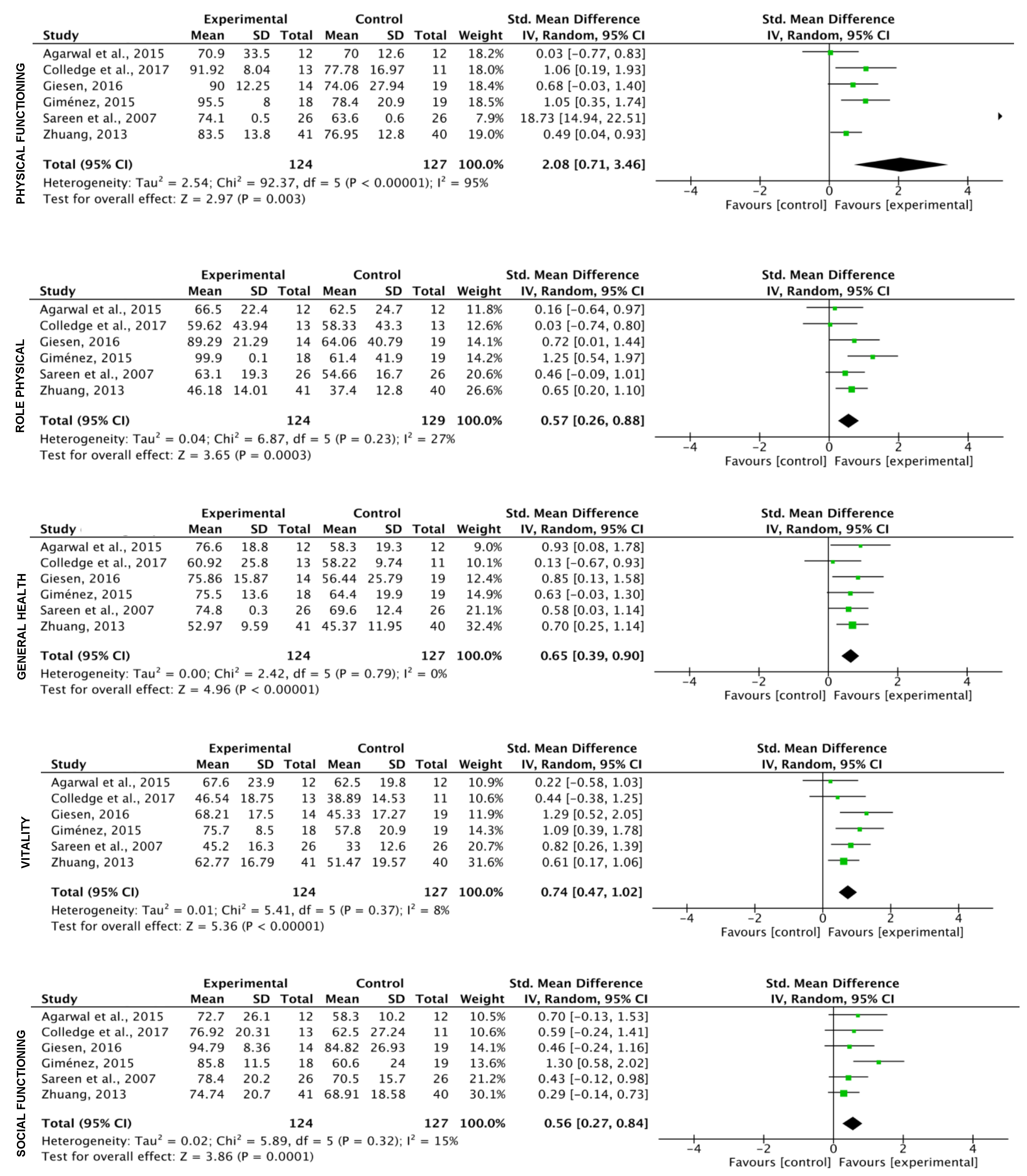
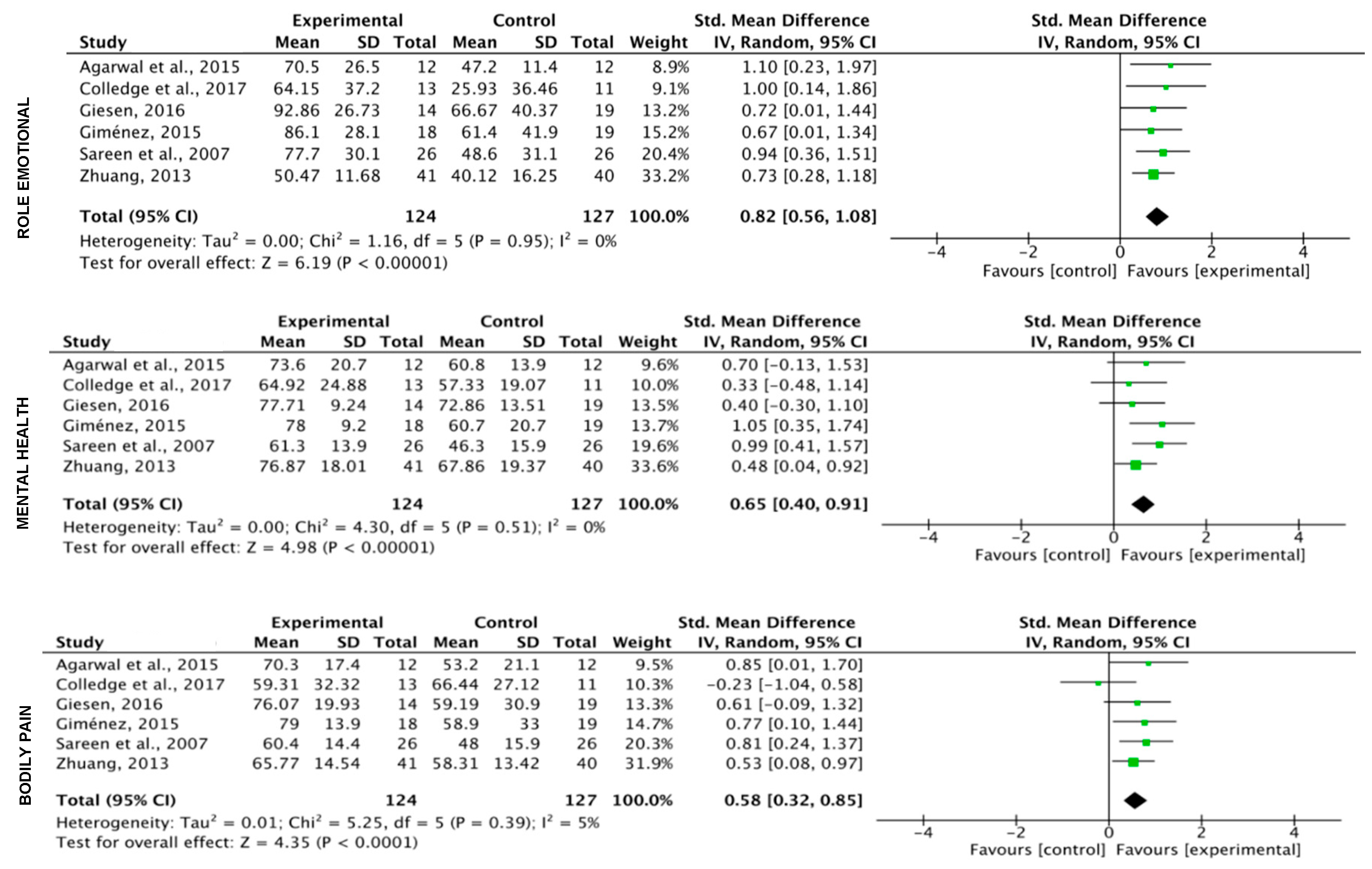
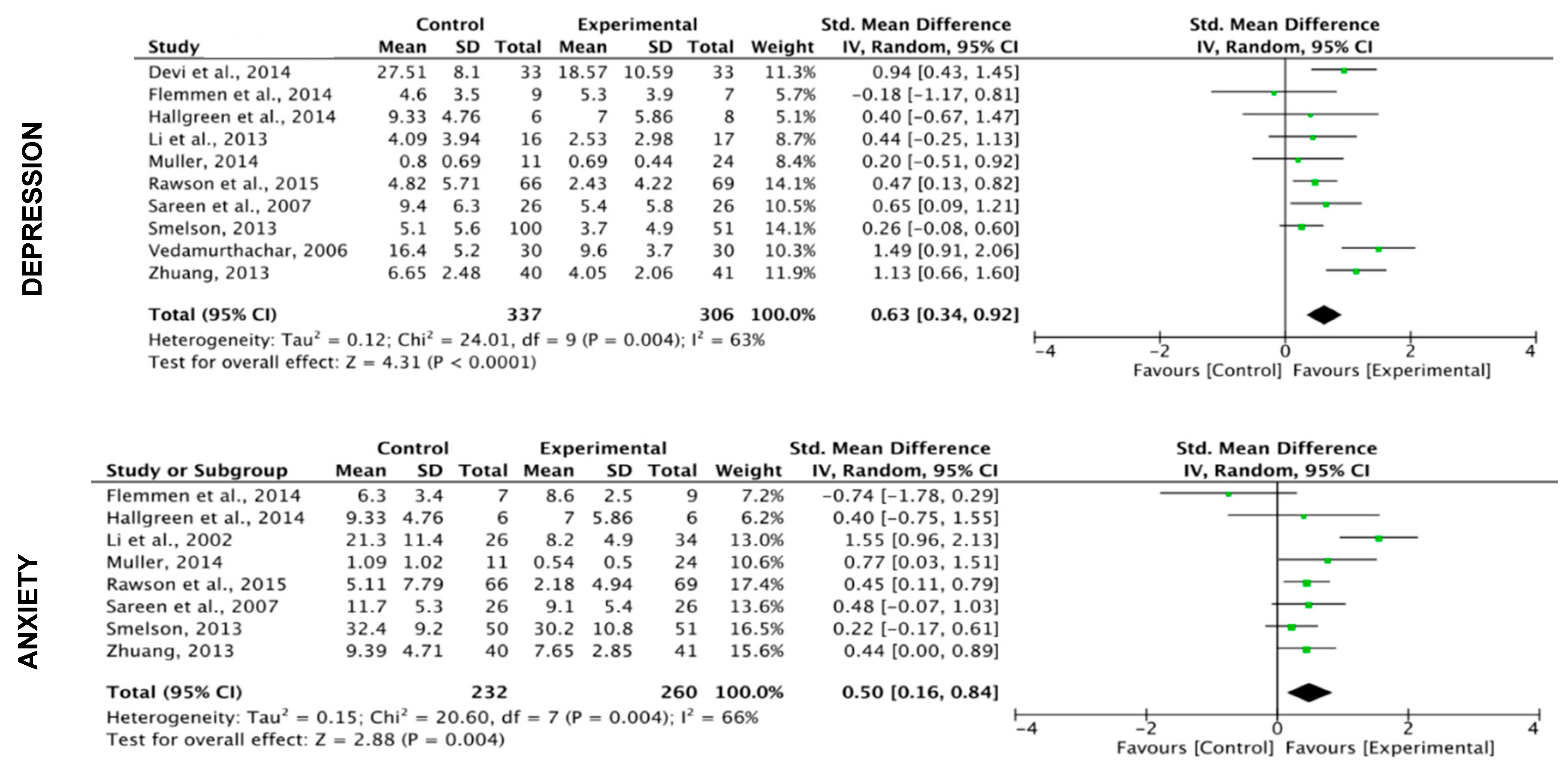
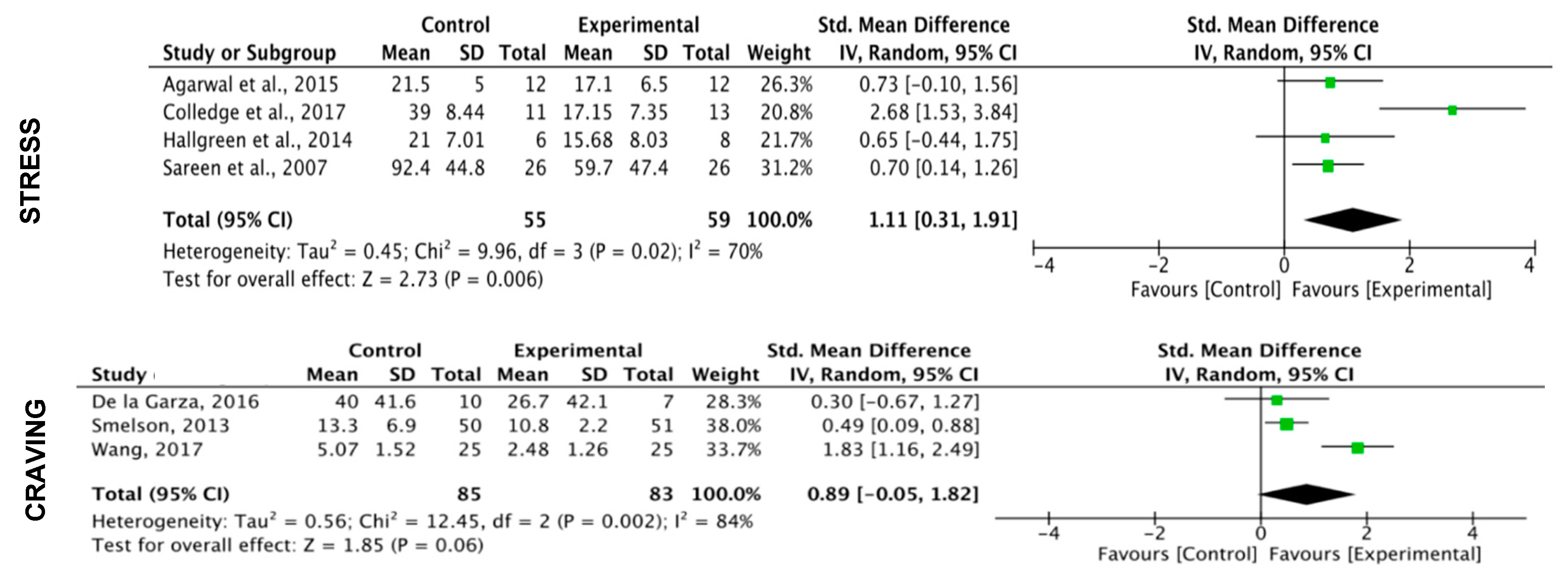
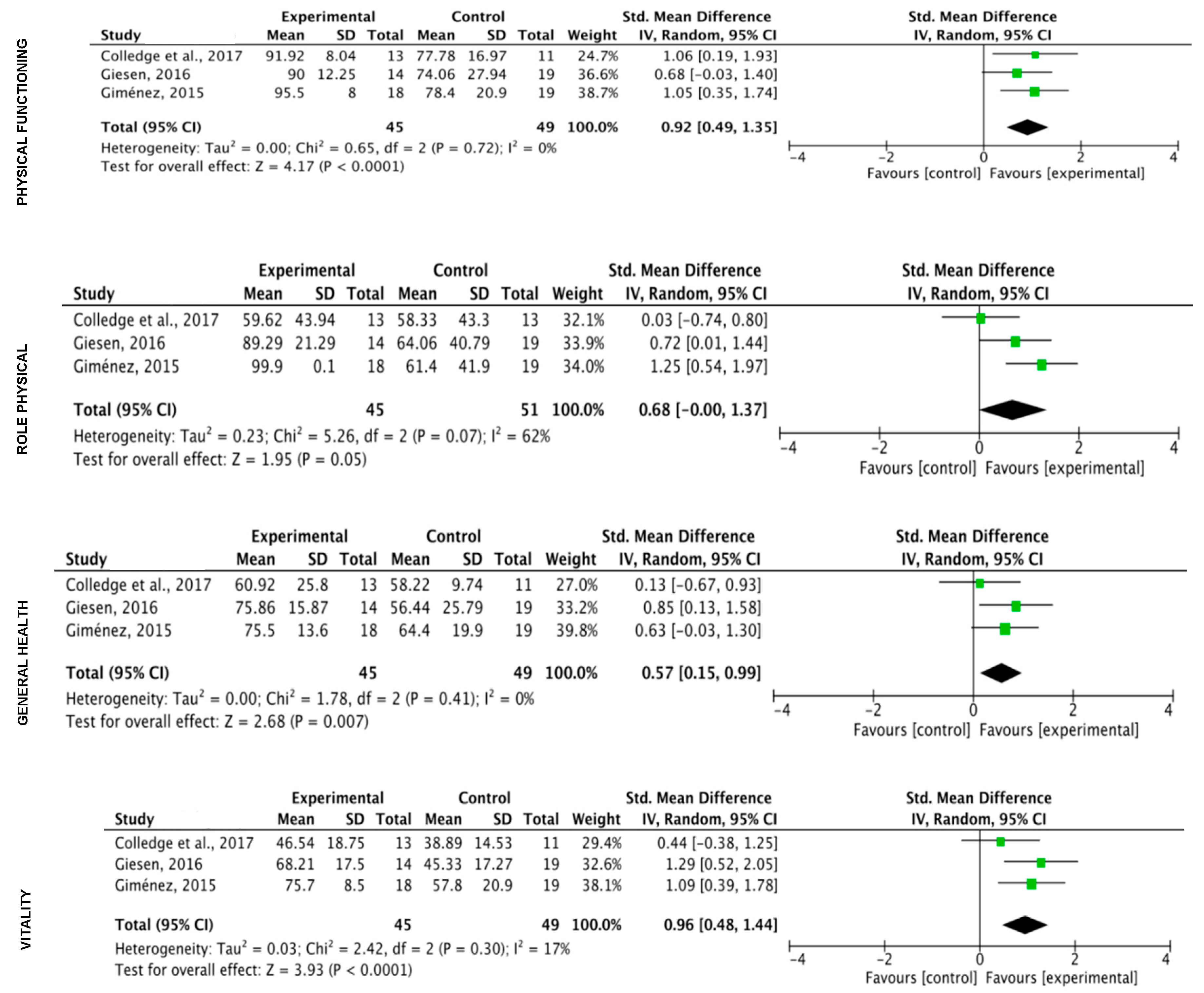
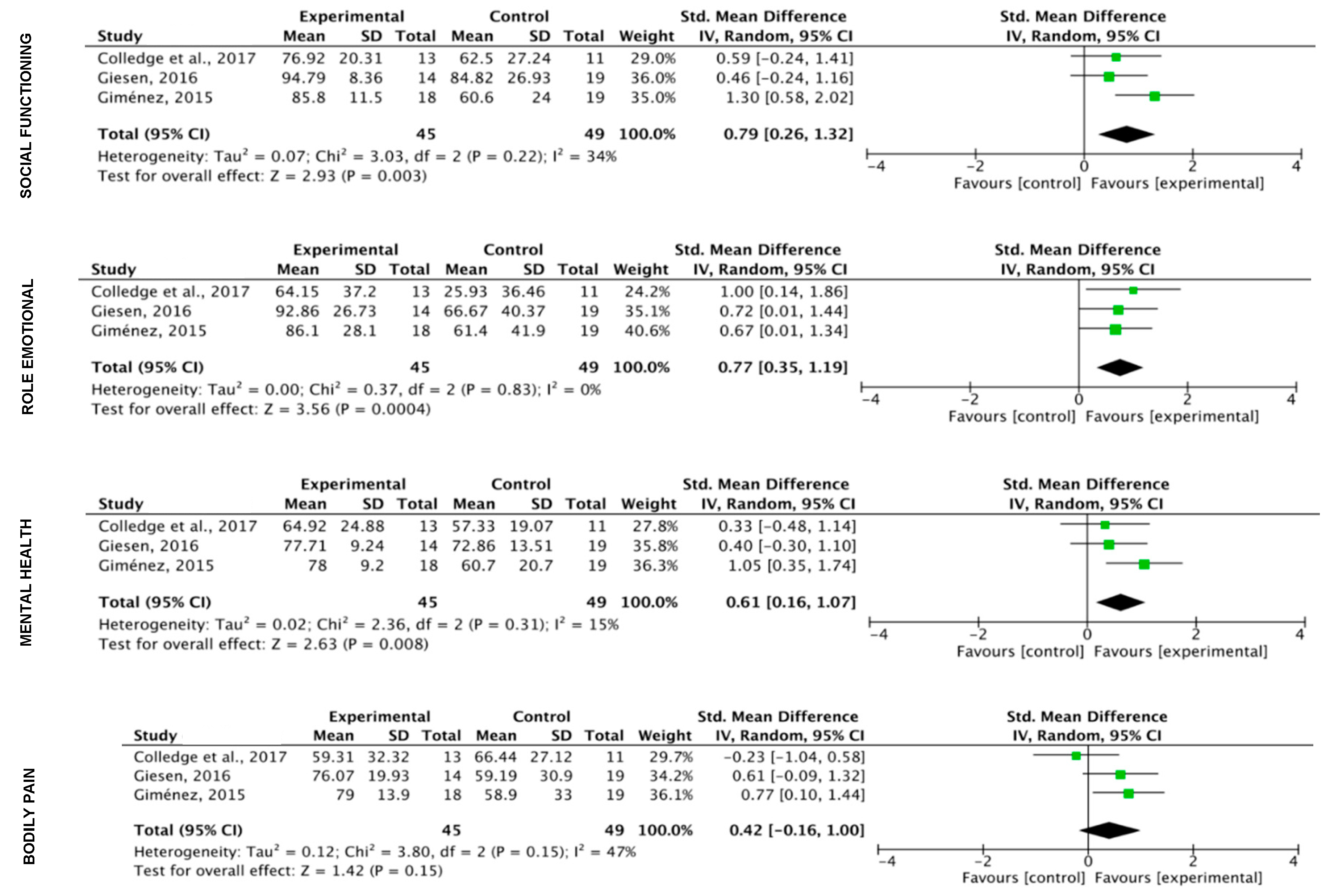
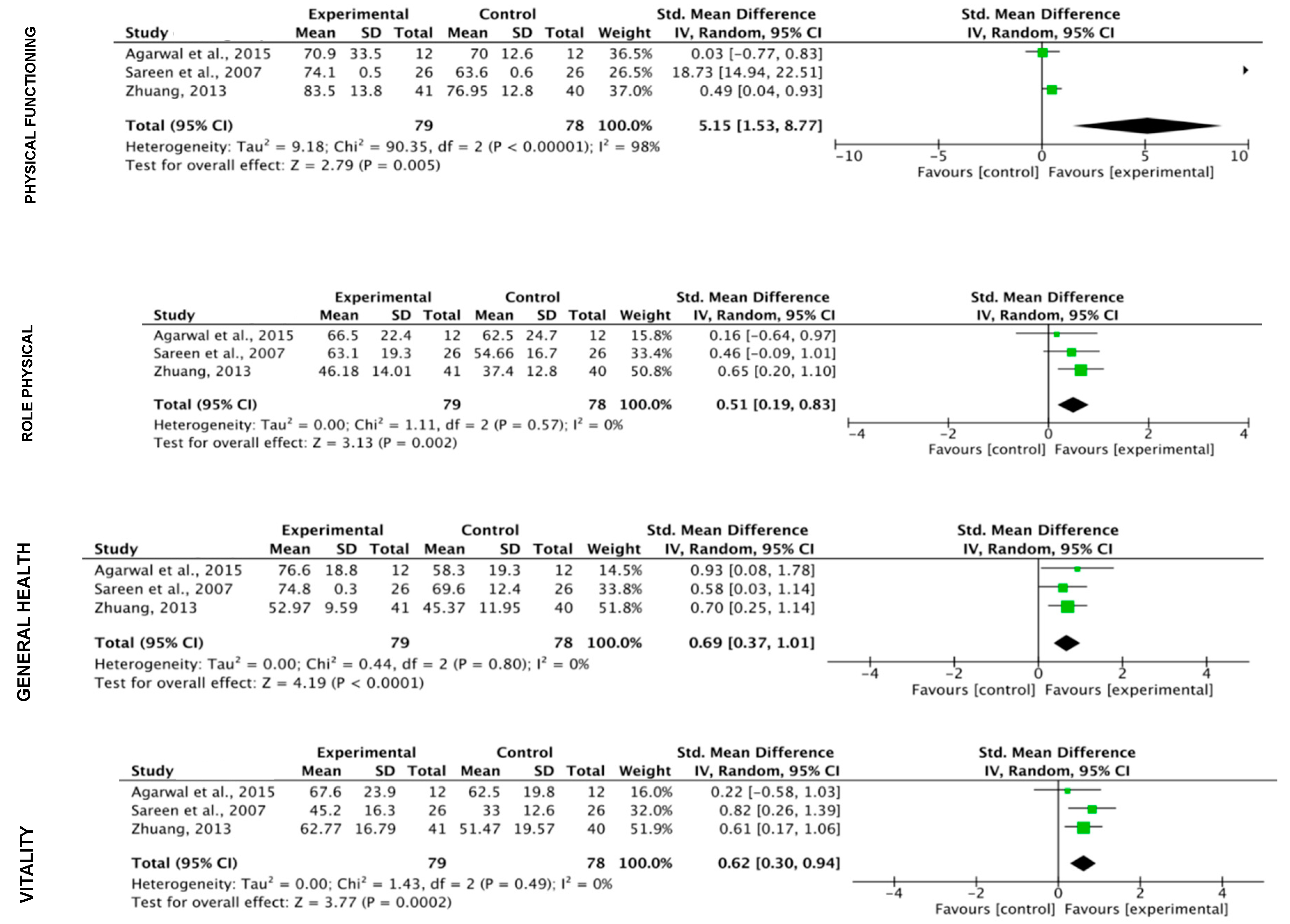
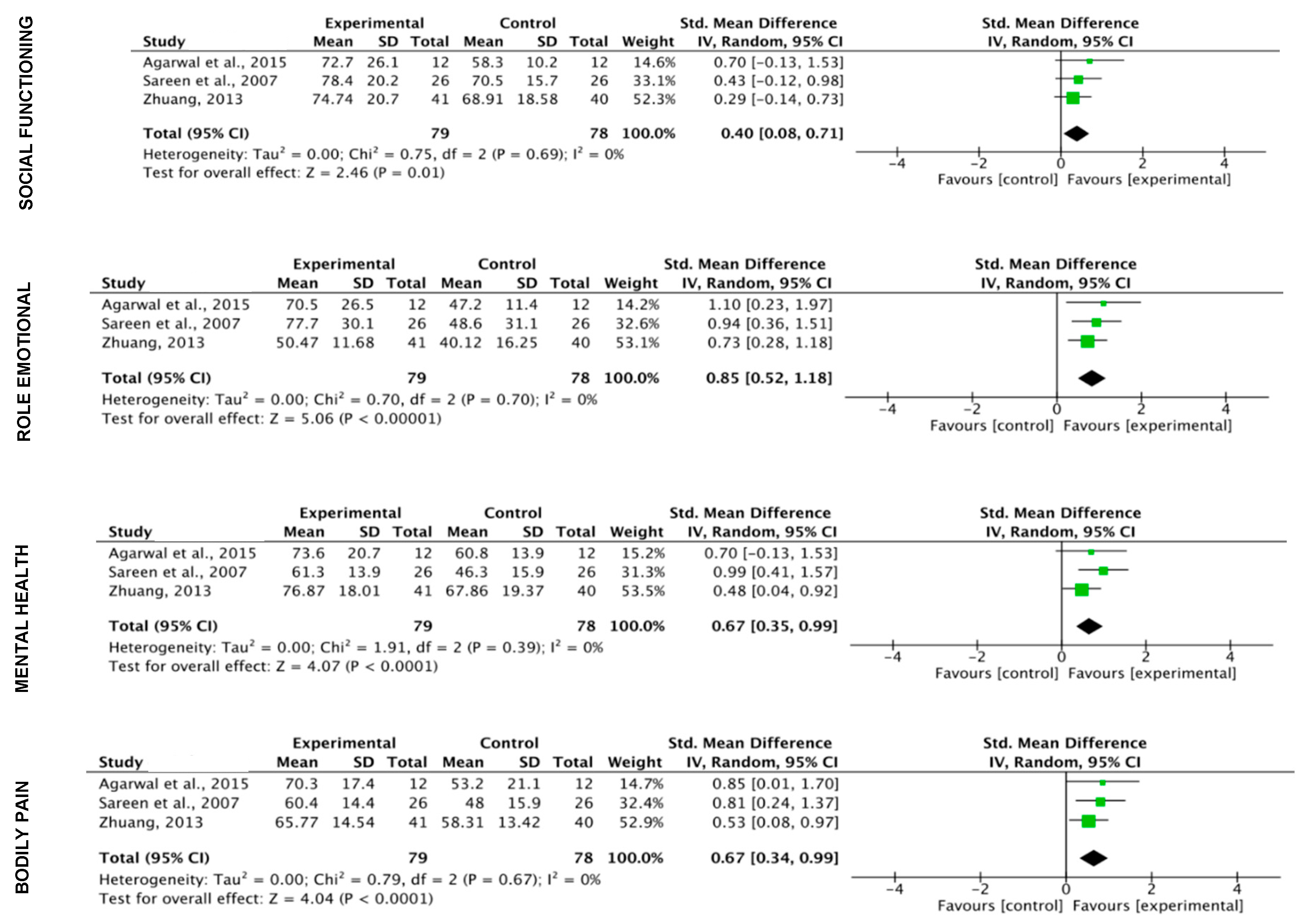
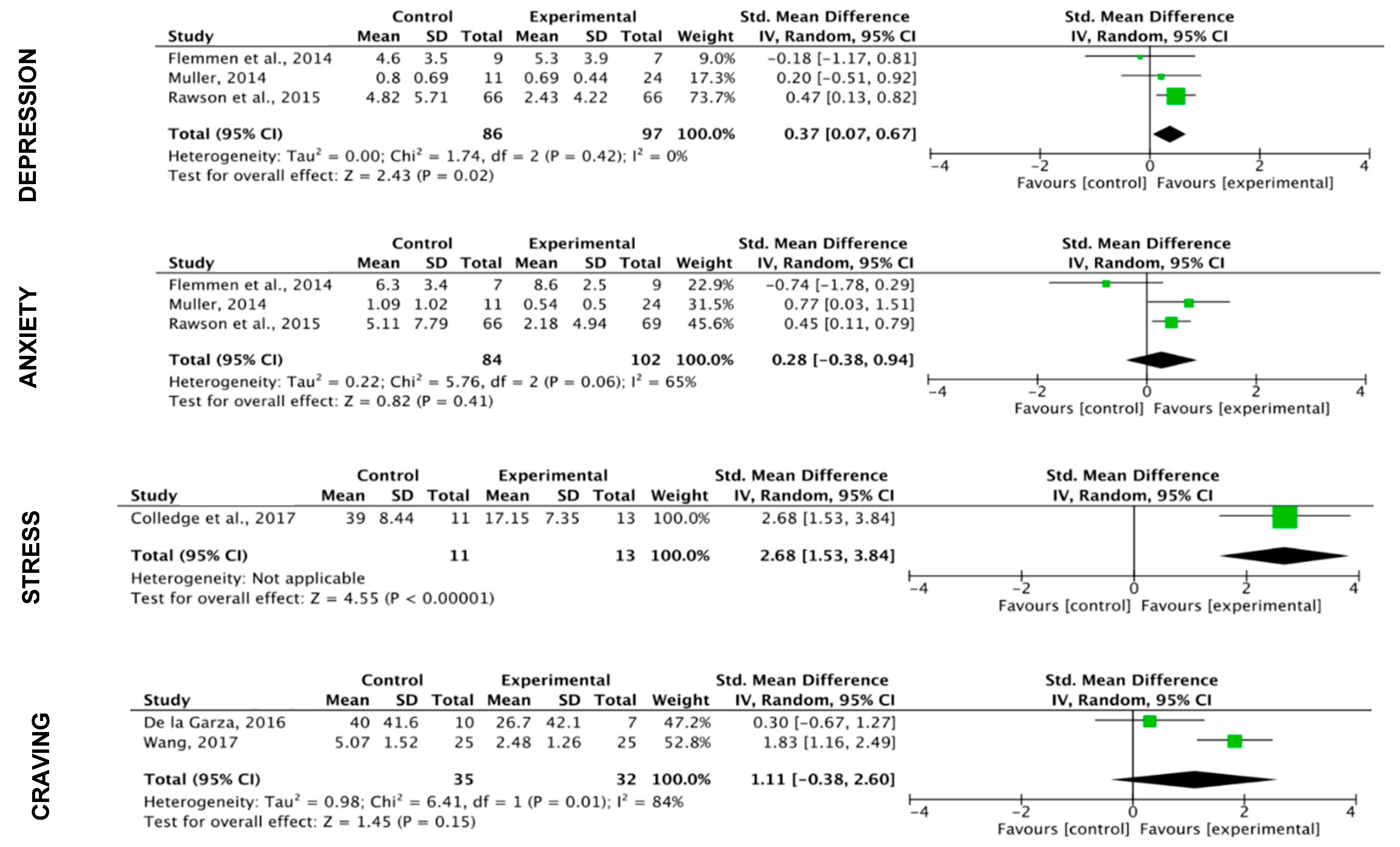
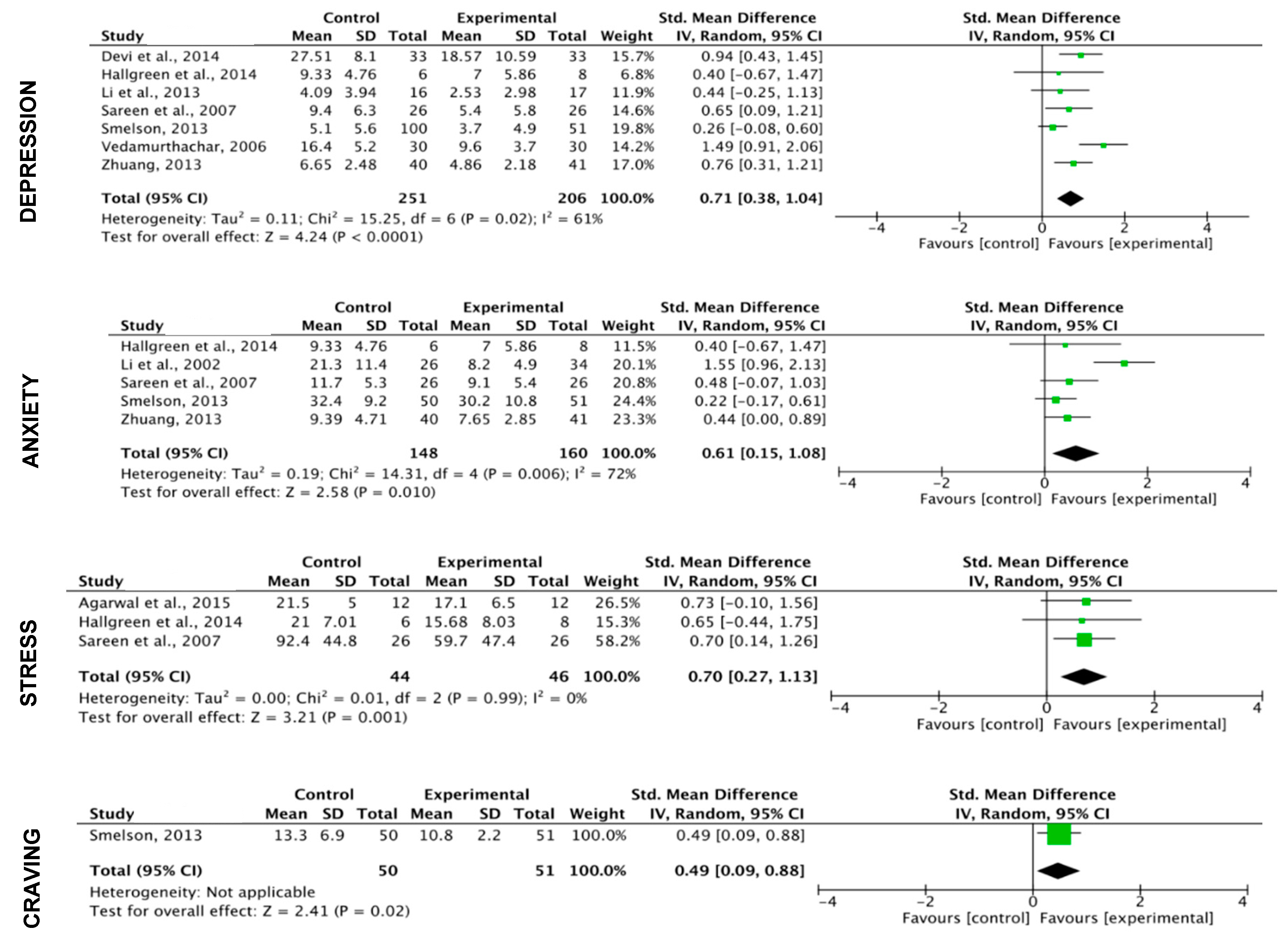
3.5. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- United Nations Office on Drugs and Crime. World Drug Report 2016; Sales No. E.16.XI.7; United Nations publication: New York, NY, USA, 2013. [Google Scholar]
- Laudet, A.B. What does recovery mean to you? Lessons from the recovery experience for research and practice. J. Subst Abuse Treat. 2007, 33, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Lisha, N.E.; Sussman, S. Relationship of high school and college sports participation with alcohol, tobacco, and illicit drug use: A review. Addict Behav. 2010, 35, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.A.; Abrantes, A.M.; Minami, H.; Read, J.P.; Marcus, B.H.; Jakicic, J.M.; Strong, D.R.; Dubreuil, M.E.; Gordon, A.A.; Ramsey, S.E.; et al. A preliminary, randomized trial of aerobic exercise for alcohol dependence. J. Subst. Abuse Treat. 2014, 47, 1–9. [Google Scholar] [CrossRef]
- Brown, R.A.; Prince, M.A.; Minami, H.; Abrantes, A.M. An exploratory analysis of changes in mood, anxiety and craving from pre- to post-single sessions of exercise, over 12 weeks, among patients with alcohol dependence. Ment. Health Phys. Act. 2016, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Giesen, E.S.; Zimmer, P.; Bloch, W. Effects of an Exercise Program on Physical Activity Level and Quality of Life in Patients with Severe Alcohol Dependence. Alcohol Treat Q. 2016, 34, 63–78. [Google Scholar] [CrossRef]
- Buchowski, M.S.; Meade, N.N.; Charboneau, E.; Park, S.; Dietrich, M.S.; Cowan, R.L.; Martin, P.R. Aerobic exercise training reduces cannabis craving and use in non-treatment seeking cannabis-dependent adults. PLoS ONE 2011, 6, e17465. [Google Scholar] [CrossRef]
- De La Garza, R.; Yoon, J.H.; Thompson-Lake, D.G.; Haile, C.N.; Eisenhofer, J.D.; Newton, T.F.; Mahoney, J.J. Treadmill exercise improves fitness and reduces craving and use of cocaine in individuals with concurrent cocaine and tobacco-use disorder. Psychiatry Res. 2016, 245, 133–140. [Google Scholar] [CrossRef]
- Smelson, D.; Chen, K.W.; Ziedonis, D.; Andes, K.; Lennox, A.; Callahan, L.; Rodrigues, S.; Eisenberg, D. A pilot study of qigong for reducing cocaine craving early in recovery. J. Altern. Complement. Med. 2013, 19, 97–101. [Google Scholar] [CrossRef]
- Wang, D.; Zhou, C.; Chang, Y.K. Acute exercise ameliorates craving and inhibitory deficits in methamphetamine: An ERP study. Physiol. Behav. 2015, 147, 38–46. [Google Scholar] [CrossRef]
- Wang, D.; Zhou, C.; Zhao, M.; Wu, X.; Chang, Y.K. Dose-response relationships between exercise intensity, cravings, and inhibitory control in methamphetamine dependence: An ERPs study. Drug Alcohol Depend. 2016, 61, 331–339. [Google Scholar] [CrossRef]
- Wang, D.; Zhu, T.; Zhou, C.; Chang, Y.K. Aerobic exercise training ameliorates craving and inhibitory control in methamphetamine dependencies: A randomized controlled trial and event-related potential study. Psychol. Sport Exerc. 2017, 30, 82–90. [Google Scholar] [CrossRef]
- Brown, R.A.; Abrantes, A.M.; Read, J.P.; Marcus, B.H.; Jakicic, J.; Strong, D.R.; Oakley, J.R.; Ramsey, S.E.; Kahler, C.W.; Stuart, G.L.; et al. A pilot study of aerobic exercise as an adjunctive treatment for drug dependence. Ment. Health Phys. Act. 2010, 3, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, J.; Barry, D.; Petry, N.M. Exercise-related activities are associated with positive outcome in contingency management treatment for substance use disorders. Addict Behav. 2008, 33, 1072–1075. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.P.; Kumar, A.; Lewis, J.E. A pilot feasibility and acceptability study of yoga/meditation on the quality of life and markers of stress in persons living with HIV who also use crack cocaine. J. Altern. Complement Med. 2015, 21, 152–158. [Google Scholar] [CrossRef]
- Mamen, A.; Pallesen, S.; Martinsen, E.W. Changes in mental distress following individualized physical training in patients suffering from chemical dependence. Eur. J. Sport Sci. 2011, 11, 269–276. [Google Scholar] [CrossRef]
- Rawson, R.A.; Chudzynski, J.; Gonzales, R.; Mooney, L.; Dickerson, D.; Ang, A.; Dolezal, B.; Cooper, C.B. The impact of exercise on depression and anxiety symptoms among abstinent methamphetamine-dependent individuals in a residential treatment setting. J. Subst. Abuse Treat. 2015, 57, 36–40. [Google Scholar] [CrossRef]
- Flemmen, G.; Unhjem, R.; Wang, E. High-intensity interval training in patients with substance use disorder. Biomed. Res. Int. 2014, 1, 1–8. [Google Scholar] [CrossRef]
- American Psychiatric Association. Use of the Manual. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013; ISBN 978-0-89042-559-6. [Google Scholar]
- Muller, A.E.; Clausen, T. Group exercise to improve quality of life among substance use disorder patients. Scand. J. Public Health 2014, 43, 146–152. [Google Scholar] [CrossRef]
- Zhuang, S.; An, S.; Zhao, Y. Yoga effects on mood and quality of life in Chinese women undergoing heroin detoxification: A randomized controlled trial. Nurs Res. 2013, 62, 260–268. [Google Scholar] [CrossRef]
- Grandjean Da Costa, K.; Barbieri, J.; Hohl, R.; Costa, E.; Fontes, E. Exercise training improves cardiorespiratory fitness and cognitive function in individuals with substance use disorders: A pilot study. Sport Sci. Health 2016, 13, 437–441. [Google Scholar] [CrossRef]
- Nani, S.; Matsouka, O.; Tsitskari, E.; Avgerinos, A. The role of physical activity in life happiness of Greek drug abusers participating in a treatment program. Sport Sci. Health 2017, 13, 25–32. [Google Scholar] [CrossRef]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Colledge, F.; Vogel, M.; Dürsteler-Macfarland, K.; Strom, J.; Schoen, S.; Pühse, U.; Gerber, M. A pilot randomized trial of exercise as adjunct therapy in a heroin-assisted treatment setting. J. Subst. Abuse Treat. 2017, 76, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Mamen, A.; Martinsen, E.W. Development of aerobic fitness of individuals with substance abuse/dependence following long-term individual physical activity. Eur. J. Sport Sci. 2010, 10, 255–262. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Chudzynski, J.; Dickerson, D.; Mooney, L.; Rawson, R.A.; Garfinkel, A.; Cooper, C.B. Exercise training improves heart rate variability after methamphetamine dependency. Med. Sci. Sports Exerc. 2014, 46, 1057–1066. [Google Scholar] [CrossRef]
- Chen, K.W.; Comerford, A.; Shinnick, P.; Ziedonis, D.M. Introducing qigong meditation into residential addiction treatment: A Pilot Study Where Gender Makes a Difference. J. Altern. Complement Med. 2010, 16, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Hallgren, M.; Romberg, K.; Bakshi, A.S.; Andréasson, S. Yoga as an adjunct treatment for alcohol dependence: A pilot study. Complement. Ther. Med. 2014, 22, 441–445. [Google Scholar] [CrossRef]
- Li, D.X.; Zhuang, X.Y.; Zhang, Y.P.; Guo, H.; Wang, Z.; Zhang, Q.; Feng, Y.M.; Yao, Y.G. Effects of tai chi on the Protracted Abstinence Syndrome: A Time Trial Analysis. Am. J. Chin. Med. 2013, 41, 43–57. [Google Scholar] [CrossRef]
- Reddy, S.; Dick, A.M.; Gerber, M.R.; Mitchell, K. The Effect of a yoga intervention on alcohol and drug abuse risk in veteran and civilian women with posttraumatic stress disorder. J. Altern. Complement. Med. 2014, 20, 750–756. [Google Scholar] [CrossRef]
- Morris, L.; Stander, J.; Ebrahim, W.; Eksteen, S.; Meaden, O.A.; Ras, A.; Wessels, A. Effect of exercise versus cognitive behavioural therapy or no intervention on anxiety, depression, fitness and quality of life in adults with previous methamphetamine dependency: A systematic review. Addict. Sci. Clin. Pract. 2018, 13, 1–12. [Google Scholar] [CrossRef]
- Kuppili, P.; Parmar, A.; Gupta, A.; Balhara, Y. Role of yoga in management of substance use disorders: A narrative review. J. Neurosci. Rural Pract. 2018, 9, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Hallgren, M.; Vancampfort, D.; Giesen, E.S.; Lundin, A.; Stubbs, B. Exercise as treatment for alcohol use disorders: Systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Manthou, E.; Georgakouli, K.; Fatouros, I.; Gianoulakis, C.; Theodorakis, Y.; Jamurtas, A. Role of exercise in the treatment of alcohol use disorders (Review). Biomed. Rep. 2016, 4, 535–545. [Google Scholar] [CrossRef]
- Bardo, M.T.; Compton, W.M. Does physical activity protect against drug abuse vulnerability? Drug Alcohol Depend. 2015, 153, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Siñol, N.; Martínez-Sánchez, E.; Guillamó, E.; Campins, M.; Larger, F.; Trujols, J. Effectiveness of exercise as a complementary intervention in addictions: A review. Adicciones 2013, 25, 71–85. [Google Scholar] [CrossRef] [PubMed]
- Zschucke, E.; Heinz, A.; Ströhle, A. Exercise and physical activity in the therapy of substance use disorders. Sci. World J. 2012, 46, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Wang, Y.; Wang, Y.; Li, R.; Zhou, C. Impact of physical exercise on substance use disorders: A meta-analysis. PLoS ONE 2014, 9, e110728. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- PEDro: Physiotherapy Evidence Database. Available online: https://www.pedro.org.au (accessed on 20 February 2018).
- De Morton, N. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.; De Vet, H.; De Bie, R.; Kessels, A.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]
- Gary, V.; Guthrie, D. The effect of jogging on physical fitness and self-concept in hospitalized alcoholics. Q. J. Stud. Alcohol 1972, 33, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Frankel, A.; Murphy, J. Physical fitness and personality in alcoholism. Canonical analysis of measures before and after treatment. Q. J. Stud. Alcohol 1974, 35, 1272–1278. [Google Scholar] [CrossRef]
- Piorkowski, M.; Axtell, L. Effect of circuit exercise training on physical fitness of alcoholic patients. Phys. Ther. 1976, 56, 403–406. [Google Scholar] [CrossRef]
- McKelvy, P.L.; Stein, C.A.; Bertini, A.B. Heart-rate response to a conditioning program for young, alcoholic men. Phys. Ther. 1980, 184–187. [Google Scholar] [CrossRef]
- Sinyor, D.; Brown, T.; Rostant, L.; Seraganian, P. The role of a physical fitness program in the treatment of alcoholism. J. Stud. Alcohol. 1982, 43, 380–386. [Google Scholar] [CrossRef]
- Palmer, J.; Vacc, N.; Epstein, J. Adult inpatient alcoholics: Physical exercise as a treatment intervention. J. Stud. Alcohol. 1988, 49, 418–421. [Google Scholar] [CrossRef]
- Donaghy, M. The investigation of exercise as an adjunct to the treatment and rehabilitation of the problem drinker. Ph.D. Thesis, University of Glasgow, Glasgow, Scotland, 1997. [Google Scholar]
- Ermalinski, R.; Hanson, P.G.; Lubin, B.; Thornby, J.; Nahormek, P.A. Impact of a Body-Mind Treatment Component on Alcoholic Inpatients. J. Psychosoc. Nurs. Ment. Health Serv. 1997, 35, 39–45. [Google Scholar]
- Vedamurthachar, A.; Janakiramaiah, N.; Hegde, J.M.; Shetty, T.K.; Subbakrishna, D.K.; Sureshbabu, S.V.; Gangadhar, B.N. Antidepressant efficacy and hormonal effects of Sudarshana Kriya Yoga (SKY) in alcohol dependent individuals. J. Affect. Disord. 2006, 94, 249–253. [Google Scholar] [CrossRef]
- Sareen, S.; Kumari, V.; Gajebasia, K.; Gajebasia, N.K. Yoga: A tool for improving the quality of life in chronic pancreatitis. World J. Gastroenterol. 2007, 21, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.A.; Abrantes, A.M.; Read, J.P.; Marcus, B.H.; Jakicic, J.; Strong, D.R.; Oakley, J.R.; Ramsey, S.E.; Kahler, C.V.; Stuart, G.; et al. Aerobic exercise for alcohol recovery: Rationale, program description, and preliminary findings. Behav. Modif. 2009, 33, 220–249. [Google Scholar] [CrossRef] [PubMed]
- Roessler, K.K.; Bilberg, R.; Jensen, K.; Kjaergaard, A.S.; Dervisevic, A.; Nielsen, B. Exercise as treatment for alcohol dependence. SSR 2013, 23, 205–216. [Google Scholar] [CrossRef]
- Georgakouli, K.; Manthou, E.; Georgoulias, P.; Ziaka, A.; Fatouros, I.G.; Mastorakos, G.; Koutedakis, Y.; Theodorakis, Y.; Jamurta, A.Z. Exercise training reduces alcohol consumption but does not affect HPA-axis activity in heavy drinkers. Physiol. Behav. 2017, 179, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Roessler, K.K.; Bilberg, R.; Nielsen, A.S.; Jensen, M.B.; Ekstrøm, C.T.; Sari, S. Exercise as adjunctive treatment for alcohol use disorder: A randomized controlled trial. PLoS ONE 2017, 12, e0186076. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.B.; Nielsen, C.; Ekstrøm, C.T.; Roessler, K.K. Physical exercise in the treatment of alcohol use disorder (AUD) patients affects their drinking habits: A randomized controlled trial. Scand. J. Public Health 2018, 47, 462–468. [Google Scholar] [CrossRef]
- Roessler, K.K.; Mau, M.; Ekstrøm, C.T. Interpersonal problems of alcohol use disorder patients undergoing a physical exercise intervention—A randomised controlled trial. Nord. Psychol. 2018, 70, 1–11. [Google Scholar] [CrossRef]
- Burling, T.A.; Seidner, A.L.; Robbins-Sisco, D.; Krinsky, A.; Hanser, S.B. Batter up! Relapse prevention for homeless veteran substance abusers via softball team participation. J. Subst. Abus. 1992, 4, 407–413. [Google Scholar] [CrossRef]
- Palmer, J.A.; Palmer, L.K.; Michiels, K.; Thigpen, B. Effects of Type of Exercise on Depression in Recovering Substance Abusers. Percept. Mot. Ski. 1995, 80, 523–530. [Google Scholar] [CrossRef]
- Shaffer, H.J.; A LaSalvia, T.; Stein, J.P. Comparing Hatha yoga with dynamic group psychotherapy for enhancing methadone maintenance treatment: A randomized clinical trial. Altern. Ther. Health Med. 1997, 3, 57–66. [Google Scholar]
- Li, M.; Chen, K.; Mo, Z. Use of qigong therapy in the detoxification of heroin addicts. Altern. Ther. Health Med. 2002, 8, 50–59. [Google Scholar] [PubMed]
- Khalsa, S.B.S.; Khalsa, G.S.; Khalsa, H.K.; Khalsa, M.K. Evaluation of a Residential Kundalini Yoga Lifestyle Pilot Program for Addiction in India. J. Ethn. Subst. Abus. 2008, 7, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Roessler, K.K. Exercise treatment for drug abuse—A Danish pilot study. Scand. J. Public Health 2010, 38, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Dolezal, B.A.; Chudzynski, J.; Storer, T.W.; Abrazado, M.; Penate, J.; Mooney, L.; Dickerson, D.; Rawson, R.A.; Cooper, C.B. Eight Weeks of Exercise Training Improves Fitness Measures in Methamphetamine-Dependent Individuals in Residential Treatment. J. Addict. Med. 2013, 7, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Cutter, C.J.; Schottenfeld, R.S.; Moore, B.A.; Ball, S.A.; Beitel, M.; Savant, J.D.; Stults-Kolehmainen, M.A.; Doucette, C.; Barry, D.T. A pilot trial of a videogame-based exercise program for methadone maintained patients. J. Subst. Abus. Treat. 2014, 47, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Devi, N.; Benji, T. Efect of yoga on depression and quality of life in drug abusers. Int. J. Ayurveda Pharma Res. 2014, 2, 61–65. [Google Scholar]
- Dhawan, A.; Chopra, A.; Jain, R.; Yadav, D. Effectiveness of yogic breathing intervention on quality of life of opioid dependent users. Int. J. Yoga 2015, 8, 144–147. [Google Scholar] [CrossRef]
- Giménez-Meseguer, J.; Tortosa-Martinez, J.; Fernández-Valenciano, M.D.L.R. Benefits of Exercise for the Quality of Life of Drug-Dependent Patients. J. Psychoact. Drugs 2015, 47, 1–8. [Google Scholar] [CrossRef]
- Zhu, N.; Xu, D.; Dai, G.; Wang, F.; Xu, X.; Zhou, D. Beneficial effects of Tai Chi for amphetamine-type stimulant dependence: A pilot study. Am. J. Drug Alcohol Abus. 2016, 42, 1–10. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Greer, T.L.; Rethorst, C.D.; Carmody, T.; Grannemann, B.D.; Walker, R.; Warden, D.; Shores-Wilson, K.; Stoutenberg, M.; Oden, N.; et al. Randomized Controlled Trial Comparing Exercise to Health Education for Stimulant Use Disorder: Results From the CTN-0037 STimulant Reduction Intervention Using Dosed Exercise (STRIDE) Study. J. Clin. Psychiatry 2017, 78, 1075–1082. [Google Scholar] [CrossRef]
- Carmody, T.; Greer, T.L.; Walker, R.; Rethorst, C.D.; Trivedi, M.H. A complier average causal effect analysis of the Stimulant Reduction Intervention using dosed exercise study. Contemp. Clin. Trials Commun. 2018, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, Q.; Jiang, H.; Du, J.; Zhou, C.; Yu, S.; Hashimoto, K.; Zhao, M. Impact of aerobic exercise on cognitive impairment and oxidative stress markers in methamphetamine-dependent patients. Psychiatry Res. Neuroimaging 2018, 266, 328–333. [Google Scholar] [CrossRef]
- Ussher, M.; Sampuran, A.K.; Doshi, R.; West, R.; Drummond, C. Acute effect of a brief bout of exercise on alcohol urges. Addiction 2004, 99, 1542–1547. [Google Scholar] [CrossRef] [PubMed]
- Jamurtas, A.Z.; Zourbanos, N.; Georgakouli, K.; Georgoulias, P.; Manthou, E.; Fatouros, I.G.; Goudas, M.; Koutedakis, Y.; Theodorakis, Y. Beta Endorphin and Alcohol Urge Responses in Alcoholic Patients Following an Acute Bout of Exercise. J. Addict. Res. Ther. 2014, 5, 1–6. [Google Scholar] [CrossRef]
- Georgakouli, K.; Manthou, E.; Fatouros, I.G.; Deli, C.K.; Spandidos, D.; Tsatsakis, A.M.; Kouretas, D.; Koutedakis, Y.; Theodorakis, Y.; Jamurtas, A.Z. Effects of acute exercise on liver function and blood redox status in heavy drinkers. Exp. Ther. Med. 2015, 10, 2015–2022. [Google Scholar] [CrossRef] [PubMed]
- Ciccolo, J.T.; Whitworth, J.; Dunsiger, S.I.; Santabarbara, N.J.; Nosrat, S.; LaBrec, J.E. Acute effects of resistance exercise on affect, arousal, and urge to drink in temporarily abstinent young adult hazardous drinkers. Am. J. Addict. 2016, 25, 623–627. [Google Scholar] [CrossRef]
- Giesen, E.S.; Deimel, H.; Bloch, W. Clinical Exercise Interventions in Alcohol Use Disorders: A Systematic Review. J. Subst. Abus. Treat. 2015, 52, 1–9. [Google Scholar] [CrossRef]
- Vancampfort, D.; Rosenbaum, S.; Schuch, F.B.; Ward, P.B.; Probst, M.; Stubbs, B.; Information, P.E.K.F.C. Prevalence and predictors of treatment dropout from physical activity interventions in schizophrenia: A meta-analysis. Gen. Hosp. Psychiatry 2016, 39, 15–23. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Horikawa, C.; Saito, A.; Heianza, Y.; Anasako, Y.; Nishigaki, Y.; Yachi, Y.; Iida, K.T.; et al. Alcohol Consumption and Risk of Atrial Fibrillation. J. Am. Coll. Cardiol. 2011, 57, 427–436. [Google Scholar] [CrossRef]
- Moreira, T.D.C.; Figueiró, L.R.; Fernandes, S.; Justo, F.M.; Dias, I.R.; Barros, H.M.T.; Ferigolo, M. Quality of life of users of psychoactive substances, relatives, and non-users assessed using the WHOQOL-BREF. Ciência Saúde Coletiva 2013, 18, 1953–1962. [Google Scholar] [CrossRef]
- National Institute on Drug Abuse. Drugs, Brains and Behaviour: The Science of Addiction. Available online: https://d14rmgtrwzf5a.cloudfront.net/sites/default/files/soa.pdf (accessed on 16 February 2018).
- Brownell, K.D.; Marlatt, G.A.; Lichtenstein, E.; Wilson, G.T. Understanding and preventing relapse. Am. Psychol. 1986, 41, 765–782. [Google Scholar] [CrossRef] [PubMed]
- Witkiewitz, K.; Bowen, S.; Donovan, D. Moderating effects of a craving intervention on the relation between negative mood and heavy drinking following treatment for alcohol dependence. J. Consult. Clin. Psychol. 2011, 79, 54–63. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | 1. Election Criteria | 2. RTC | 3. Blind Assignm. | 4. Baseline Similar. | 7. Blind Eval. | 8. Measur. of >85% | 9. Intent to Treat | 10. Between Groups | 11. Variab. Measures | Total |
|---|---|---|---|---|---|---|---|---|---|---|
| Gary et al. [46] | No | Yes | No | Yes | No | Yes | No | No | Yes | 4/9 |
| Frankel et al. [47] | No | No | No | No | No | No | No | No | Yes | 1/9 |
| Piorkowski et al. [48] | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | 8/9 |
| McKelvy et al. [49] | Yes | Yes | Yes | Yes | No | Yes | No | No | Yes | 6/9 |
| Sinyor et al. [50] | No | No | No | No | No | No | No | No | Yes | 1/9 |
| Palmer et al. [51] | Yes | No | No | Yes | No | No | No | Yes | No | 3/9 |
| Burling et al. [62] | Yes | No | No | Yes | No | No | No | Yes | No | 3/9 |
| Palmer et al. [63] | Yes | Yes | Yes | Yes | No | No | No | No | Yes | 5/9 |
| Donaghy et al. [52] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Ermalinski et al. [53] | No | No | No | No | No | No | No | Yes | No | 1/9 |
| Shaffer et al. [64] | Yes | Yes | Yes | Yes | No | No | No | Yes | No | 5/9 |
| Li et al. [65] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Ussher et al. [77] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 7/9 |
| Vedamurthachar et al. [54] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | No | 7/9 |
| Sareen et al. [55] | Yes | Yes | Yes | Yes | No | Yes | Yes | No | No | 6/9 |
| Khalsa et al. [66] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Weinstock et al. [14] | Yes | No | No | No | No | Yes | No | Yes | Yes | 4/9 |
| Brown et al. [56] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Brown et al. [13] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Chen et al. [28] | No | No | No | Yes | No | No | No | Yes | No | 2/9 |
| Mamen et al. [26] | No | No | No | No | No | No | No | Yes | Yes | 2/9 |
| Roessler et al. [69] | Yes | No | No | No | No | No | No | No | No | 1/9 |
| Buchowski et al. [7] | Yes | No | No | No | No | Yes | No | No | Yes | 3/9 |
| Mamen et al. [16] | No | No | No | No | No | No | No | Yes | Yes | 2/9 |
| Dolezal et al. [68] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Li et al. [30] | Yes | Yes | Yes | No | No | No | No | Yes | Yes | 5/9 |
| Roessler et al. [57] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Smelson et al. [9] | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes | 6/9 |
| Zhuang et al. [21] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | 7/9 |
| Brown et al. [4] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Cutter et al. [69] | Yes | Yes | Yes | No | No | Yes | No | Yes | Yes | 6/9 |
| Devi et al. [70] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Dolezal et al. [27] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Flemmen et al. [18] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 7/9 |
| Hallgren et al. [29] | Yes | Yes | Yes | No | No | No | No | Yes | Yes | 5/9 |
| Jamurtas et al. [78] | No | No | No | No | No | Yes | Yes | Yes | Yes | 4/9 |
| Muller et al. [20] | Yes | No | No | No | No | No | No | Yes | No | 2/9 |
| Agarwal et al. [15] | Yes | Yes | Yes | Yes | No | No | No | No | Yes | 5/9 |
| Dhawan et al. [71] | Yes | Yes | No | Yes | No | No | No | Yes | Yes | 5/9 |
| Georgakouli et al. [79] | Yes | No | No | Yes | No | Yes | Yes | Yes | Yes | 6/9 |
| Giménez et al. [72] | Yes | No | No | Yes | No | No | No | Yes | Yes | 4/9 |
| Rawson et al. [17] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | 7/9 |
| Wang et al. [10] | Yes | No | No | No | No | Yes | Yes | No | Yes | 4/9 |
| Brown et al. [5] | Yes | Yes | Yes | No | No | No | No | No | Yes | 4/9 |
| Ciccolo et al. [80] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Grandjean da Costa et al. [22] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| De la Garza et al. [8] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Giesen et al. [6] | Yes | No | No | Yes | No | No | No | Yes | Yes | 4/9 |
| Wang et al. [11] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 7/9 |
| Zhu et al. [73] | Yes | No | No | No | No | Yes | No | Yes | Yes | 4/9 |
| Colledge et al. [25] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Georgakouli et al. [58] | Yes | No | No | No | No | No | No | No | Yes | 2/9 |
| Roessler et al. [59] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Trivedi et al. [74] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 8/9 |
| Wang et al. [12] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Carmody et al. [75] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | 7/9 |
| Jensen et al. [60] | Yes | Yes | Yes | Yes | No | No | No | Yes | Yes | 6/9 |
| Roessler et al. [61] | Yes | Yes | Yes | Yes | No | Yes | No | Yes | No | 6/9 |
| Zhang et al. [76] | Yes | Yes | No | Yes | No | Yes | No | Yes | Yes | 6/9 |
| Article | Subst. | N (Exp + Control) | Program | Adherence (% Attendance) | Measuring Instruments | Main Results |
|---|---|---|---|---|---|---|
| Ussher et al. [77] | Alcohol | 20 (All went through the exp/control conditions) | 10 min of static bicycle. Experimental session: Moderate intensity (40–60% FC reserve) Control session: Very slight intensity (5–20% FC reserve) | - | Alcohol Urge Questionnaire Six-item measure of mood disturbance | Decrease in the impulse to consume alcohol during exercise in an experimental group compared to the control group. There were no significant differences at the end of the exercise. |
| Jamurtas et al. [78] | Alcohol | 17 (9 + 8) | A mild intensity cycle ergometer session (55–60% FCM) | - | Alcohol Urge Questionnaire B-E Analysis Blood Measurements | Increase in B-endorphin levels There were no significant improvements Craving. |
| Georgakouli et al. [79] | Alcohol | 34 (17 + 17) | A 30 min session of moderate intensity aerobic exercise (cycle ergometer) | - | Metabolic measurements | The response of liver enzymes was improved. |
| Wang et al. [10] | Methamphetamine | 24 (All went through the exp/control conditions) | Experimental session: 30 min of static bicycle moderate intensity (65–75% FC max) Control session: 30 min of reading. | - | Visual Analog Scale for craving measurement Standard and MA-related Go/Nogo tasks Electroencephalogram | Improvements in craving during, immediately after and 50 min after exercise, with respect to the control group. Improvements at the cognitive level (concentration). |
| Brown et al. [5] | Alcohol | 26 | 12 weeks aerobic exercise moderate intensity | 70% | Likert scale (not validated) to measure mood and anxiety and craving. | Acute improvements after each exercise session in mood and anxiety. |
| Ciccolo et al. [80] | Alcohol | 14 (All went through the exp/control conditions) | A session (20 min) of strength and a passive display (20 min) of video. | 70% | Alcohol Use Disorders Identification Test (AUDIT) The Alcohol Urge Questionnaire Borg Rating of Perceived Exertion The Feeling Scale | Improvements in affection and arousal acutely. No significant improvements were found for craving. |
| Article | Substance | N (Exp + Control) | Program | Adherence (% Attendanc.) | Measuring Instruments | Main Results |
|---|---|---|---|---|---|---|
| Gary et al. [46] | Alcohol | 20 (10 + 10) | Experimental: 4 weeks, 5 sessions (run 1 mile per day) per week Control: Conventional treatment, group therapy. | - | Gough Adjective Check List Jourard Body-Cathexis Scale Self-Cathexis Scale Schneider Physical Test Control of alcohol consumption Control of sleep problems | Significant improvements at the cardiovascular level Lower level of sleep problems. |
| Frankel et al. [47] | Alcohol | 214 | Experimental: 12 weeks of aerobic exercise y strength, 5 sessions (60 min) per week. | - | Cardiovascular and anthropometric measures Illinois Standard Test of Physical Fitness Minnesota Multiphasic Personality Inventory | Significant improvements in physical conditions Significant improvements in some variables of the personality test. |
| Piorkowski et al. [48] | Alcohol | 26 (14 + 12) | Experimental: 4 weeks of circuit training, 5 sessions (55 min) per week Control: table games, 5 sessions per week | - | Stair climb Cardiac frequency | Improvements in physical conditions. |
| McKelvy et al. [49] | Alcohol | 48 (31 + 17) | Experimental: 4 weeks, 5 sessions (1,2 miles of running) per week at 85% FC max Control: Sedentary activities | - | One-Minute Step Test Three-Minute Step Test Manual capture of FC (carotid palpation) | Significant improvements in FC of rest and FC during effort. |
| Sinyor et al. [50] | Alcohol | 79 (58 + 12 + 9) | Experimental: 6 weeks of aerobic exercise and stretching, 5 sessions (40–50 min) per week Control: Conventional treatment. | - | Cardio-physiological and anthropometric measurements | Greater abstinence from experimental group at the end of treatment and at 3 and 18 months of follow-up Fitness improvements |
| Palmer et al. [51] | Alcohol | 53 (27 + 26) | Experimental: 4 weeks of aerobic exercise, 3 sessions (40–50 min) per week. Control: Conventional treatment | - | Zung Self-Rating Depression Scale Spielberger State-Trait Anxiety Inventory Tennessee Self-Concept Scale Astrand-Rhyming bicycle ergometer test | Improvements in anxiety and depression There were no improvements in physical conditions in experimental group. |
| Donaghy et al. [52] | Alcohol | 158 (80 + 78) | Experimental: Aerobic and strength exercises. 15 weeks, 3 sessions (30 min) per week Control: Stretching and breathing exercises | - | Test of physical conditions (Sit and reach, sit up, VO2) Weight control Resting heart rate Physical Self-Perception Profile Beck depression inventory Zung Self-Rating Anxiety Scale | There were no differences in abstinence Improvements in physical conditions Improvements in anxiety and depression in both groups, without differences between groups. |
| Ermalinski et al. [53] | Alcohol | 90 (48 + 42) | Experimental: 6 weeks of “body–mind-component” (yoga, jogging, motivational training) 5 sessions (90 min) per week. Control: Conventional treatment. | - | Multidimensional Health Locus of Control Scales Body cathexis scale Self-Cathexis scale Depression adjective check lists | Improvements in systolic blood pressure and aerobic capacity significantly Significant improvements in “craving” in experimental group Significant improvements in locus of control and responsibility in health care There were no improvements in depression or in “body satisfaction”. |
| Vedamurthachar et al. [54] | Alcohol | 60 (30 + 30) | Experimental: 2 weeks of Sudarshana Kriya Yoga, 60 min of daily yoga Control: Conventional treatment | - | Beck Depression Inventory Analysis of cortisol and ACTH levels | Improvements in depression in both groups, but significantly more in the experimental group Decrease of ACTH and cortisol, but significantly more in experimental group. |
| Sareen et al. [55] | Alcohol | 52 (26 + 26) | 12 weeks of yoga, 3 sessions (60 min) per week Control: Conventional treatment | - | Short Form Health Survey (SF-36) The Profile of Mood States (POMS) The Symptoms of Stress Inventory (SOSI) | Significant improvements in quality of life, stress, mood, alcohol dependence and appetite. |
| Brown et al. [56] | Alcohol | 19 | 12 weeks of aerobic exercise moderate intensity (1 day per week supervised, the rest autonomous) and 1 day weekly of teaching proper physical-sports habits. | 68% (to supervised sessions) Economic incentives to favor adherence | Structured Clinical Interview for DSM-IV Timeline Follow Back Expired air analysis Submaximal effort test Cutaneous folds and scale meter | Abstinence improvements Improvements in cardiorespiratory fitness Decrease in BMI. |
| Roessler et al. [57] | Alcohol | 7 | 6 weeks of aerobic work, moderate intensity, 2 sessions per week | 59% | Bruce treadmill protocol Screening Questionnaire of Common Mental Disorders Becks Depression Inventory | There were no significant improvements in physical conditions. A tendency was observed in the improvement of anxiety, depression and emotional disorders, but without significant results. |
| Brown et al. [4] | Alcohol | 49 (26 + 23) | 12 weeks of moderate intensity aerobic exercise (1 day per week supervised, the rest autonomous) and 1 day weekly of teaching proper physical-sports habits. | 70% (to supervised sessions) Economic incentives to favor adherence | Timeline Follow Back Analysis of expired air Center for Epidemiological Studies-Depression scale The Spielberger State-Trait Anxiety Inventory Situational Confidence Questionnaire Submaximal effort test | Significant improvements in abstinence/alcohol consumption Better results in abstinence/consumption in participants who attended more than 66% of the sessions There were no significant differences in VO2, anxiety, depression and self-efficacy. |
| Hallgren et al. [29] | Alcohol | 14 (6 + 8) | Experimental: 10 weeks of yoga, 1 session (90 min) weekly group. Patients were encouraged to perform yoga exercises autonomously. Control group: Conventional treatment. | - | Timeline Follow-back Method DSM-IV criteria for alcohol dependence Short Alcohol Dependence Data Questionnaire Hospital Anxiety and Depression Scale Sheehan Disability Scale Perceived Stress Scale | Quantitative: There were no significant differences in any variable Qualitative: Improvements in perception, stress and anxiety, increase in well-being, improvement of sleep quality, improvements in craving. |
| Brown et al. [5] | Alcohol | 26 | 12 weeks of moderate intensity aerobic exercise | 70% | Likert scale (not validated) to measure mood and anxiety and craving. | Acute improvements in mood and anxiety. |
| Giesen et al. [6] | Alcohol | 33 (14 + 19) | Experimental: 12 months, 2 sessions (60 min) per week. Example: Aerobic, strength, coordination and flexibility. Control: Conventional treatment | - | Daily monitoring of physical activity levels Short Form Health Survey (SF-36) Toxicological test | Significant improvements in quality of life (variables physical function, vitality, emotional role and mental health). |
| Georgakouli et al. [58] | Alcohol | 20 (9 + 11) | 8 weeks of supervised exercise | - | Anthropometric and physiological measurements International Physical Activity Questionnaire Alcohol Use Disorders Identification Test (AUDIT) | Improvements in alcohol consumption and physical conditions. |
| Roessler et al. [59] | Alcohol | 172 (61 + 59 + 52) | 6 months of aerobic exercise, mild-moderate intensity, 2 sessions (30-60 min) per week Exp. group 1: in groups Exp. group 2: Individual Control: Conventional treatment | - | The Addiction Severity Index The Timeline Follow-Back questionnaire International Physical Activity Questionnaire | There was no effect of the exercise program on alcohol consumption A greater protective effect of excessive alcohol consumption was observed in patients with a higher level of physical activity. |
| Jensen et al. [60] | Alcohol | 105 (38 + 35 + 32) | 24 weeks of aerobic exercise, 2 sessions (30-60 min) per week Exp. group 1: in groups Exp. group 2: Individual Control: Conventional treatment | - | The Bruce treadmill protocol Timeline Follow Back Measures of VO2 and FC | Only the group that worked individually improved their VO2, but without significant differences between groups. There were no significant differences in alcohol consumption between groups. |
| Roessler et al. [61] | Alcohol | 116 (81 + 35) | 6 months of aerobic exercise, mild-moderate intensity, 2 sessions (30–60 min) per week. Exp. group 1: in groups Exp. group 2: Individual Control: Conventional treatment | - | The Inventory of Interpersonal Problems | There were no significant changes between the control and experimental groups in any of the 4 measured subscales. |
| Article | Population/Substance | N (Exp + Control) | Program | Adherence (%Attendance) | Measuring Instruments | Main Results |
|---|---|---|---|---|---|---|
| Burling et al. [62] | SUD (varied substances) | 95 (34 + 61) | Exp group: 4 weeks of softball, 1 session per week Control group: Conventional treatment | - | Abstinence Sociodemographic data | Improvement in abstinence. |
| Palmer et al. [63] | SUD (varied substances) | 45 | 4 weeks of supervised exercise, 3 sessions (30–40 min): G. 1: Aerobic 60% FC max G. 2: Body-building G. 3: Circuit training | - | Health Status Questionnaire Center of Epidemiological Studies-Depression Kasch Step Test Anthropometric and cardio-physiological measurements | Physical condition did not improve in any group Significant improvements in depression in group 2 (body building). |
| Shaffer et al. [64] | SUD in maintenance with methadone | 59 (30 + 29) | Exp. group: 22 weeks of yoga, 75min per session Control group: Psychotherapy | - | Symptom check list Addiction severity index | There were not significant differences in any variable between the two groups. |
| Li et al. [65] | Heroin | 86 (34 + 26 + 26) | Exp. group: 10 days of qigong, 25–30 min per session, without pharmacological treatment Control group 1 and 2: different pharmacological treatments, without physical exercise. | 100% | Urine analysis Electrocardiogram Hamilton Anxiety Scale Withdrawal-symptom evaluation scale | Significant improvement with respect to the control groups in symptoms of withdrawal syndrome, anxiety, and consumption. |
| Khalsa et al. [66] | SUD (varied substances) | 8 | 90 days of yoga | - | The Perceived Stress Scale (PSS) The 32-item Behavior and Symptom Identification Scale (BASIS-32) Quality of Recovery Index (QRI) | Improvement in the BASIS-32 and QRI test. There was a decrease in perceived stress (PSS), but it was not significant. |
| Weinstock et al. [14] | SUD (varied substances) | 187 (45 + 142) | G. exp: Chose at least one sport activity offered. Control group: Did not do any sports activity. | - | Addiction Severity Index Urine and air test | Improvements in abstinence in participants who did physical-sports activities. |
| Brown et al. [13] | SUD (varied substances) | 16 | 12 weeks of moderate intensity aerobic exercise (1 day weekly supervised, the rest autonomous work) and 1 day weekly of teaching proper physical-sporting habits. | 71% (supervised sessions) Economic incentives to favor adherence | Structured Clinical Interview for DSM-IV Timeline Follow Back Expired air analysis Submaximal effort test Folds meter | Abstinence improvements Improvements in cardiorespiratory fitness There were no differences in body composition. |
| Chen et al. [28] | SUD (varied substances) | 207 (126 + 81) | G. exp: qigong G. control: Standard relaxation techniques (SMART) One session daily of qigong (1st phase) or two sessions daily (2nd phase) of qigong or SMART during 4 weeks. | Experimental group: 92% Control group: 78% | Adjectuve Rating Scale for Withdrawal Voris craving/negative-mood scale CES Depression Scale Spielberger State–Trait Anxiety Inventory–State only Substance-specific craving scale | Both groups improved in craving, sleep, anxiety, depression and symptoms of withdrawal syndrome, without significant differences between groups, except in craving, where qigong Group improved more than SMART group. Qigong Group achieved greater adherence to the program. |
| Mamen et al. [26] | SUD (varied substances) | 33 | 7.5 months (300 h) of aerobic exercise (light intensity) individualized, with “trainer partners” | - | Lactate measurements Heart rate 15-point rating of perceived exertion Maximum VO2 test | Significant improvements in aerobic power and production/elimination of lactate. |
| Roessler et al. [67] | SUD (varied substances) | 20 | 2–6 months of aerobic exercise, 3 sessions (120 min) per week. | 52% | Indirect VO2 maximum test (www.steptest.dk) European Addiction Severity Index 19 Semi-structured interviews | Quantitative: Significant improvements in VO2 maximum Qualitative: Improvements in perception of quality of life, energy level, body image and decrease in consumption. |
| Buchowski et al. [7] | Cannabis (active consumers) | 12 | 10 sessions (30 min) of moderate intensity supervised aerobic exercise. | 100% | Marijuana Craving Questionnaire Timeline Follow-back Method | Less cannabis use during the program Craving improvements. |
| Mamen et al. [16] | SUD (varied substances) | 33 | Between 2–15 months (average duration: 7.5 months, 301 h) of aerobic exercise (mild intensity) individualized | - | Lactate measurements VO2 max test The Beck Depression Inventory The Beck Anxiety Inventory The Brief Social Phobia Scale The Symptom Checklist-90 The Short Michigan Alcoholism Screening Test The Drug Abuse Screening Test-20 | Significant improvements in aerobic power and production/elimination of lactate. Decreased levels of anxiety, depression, social phobia and mental anguish. No significant improvements in alcoholism and drug abuse tests. |
| Dolezal et al. [68] | Methamphetamine | 29 (15 + 14) | 8 weeks, 3 days (60 min) per week. Experimental group: aerobic endurance and muscular strength Control group: Educational intervention, without exercise. | Experimental group: 92% Control group: 96% Economic incentives | Scale, stadiometer and bending meter for anthropometric measurements Stress test to measure VO2 and cardiac function Electrocardiogram 1RM maximum leg press and pectoral press | Significant improvements in VO2 and strength of legs and chest. Significant decrease in body fat and total weight Non-significant increase in fat-free weight. |
| Li et al. [30] | Heroine (women) | 33 (17 + 16) | Experimental group: 6 months of tai chi, 2–3 sessions (60 min) per week. Control group: Conventional treatment | - | Blood test Hamilton Rating Scale for Depression Rating scale of heroin withdrawal symptoms | At the end of the program, there were no statistically significant differences between the two groups in any of the variables measured. |
| Smelson et al. [9] | Cocaine | 86 (45 + 41) | 2 weeks of qigong, between 4–6 sessions. Experimental group: real qigong Control group: simulated qigong. | Experimental group: 90% Control group: 74% | Cocaine Craving Questionnaire Brief Voris Cocaine Craving Scale Spielberger State-Trait Anxiety Inventory– State only Beck Depression Inventory Credibility/ Expectancy Questionnaire Addiction Severity Index | Improvements in craving and depression. |
| Zhuang et al. [21] | Heroine (women) | 75 (37 + 38) | Experimental group: 6 months of yoga, 5 sessions (50 min) per week. Control group: Conventional treatment | 100% | The Profile of Mood States (POMS) Short Form Health Survey (SF-36) | Improvements in quality of life (variables with physical role, pain, general health, vitality, emotional role and mental health). Improvements in mood in the variables tension and anxiety, depression, fatigue and confusion. |
| Cutter et al. [69] | Cocaine and/or opiates in maintenance with methadone | 27 (14 + 13?) | 8 weeks, 5 sessions (20–25 min) per week. Experimental group: Physical exercise (aerobic, strength, balance and yoga) through video game (Wii Fit Plus) Control Group: Sedentary video game (Wii). | Experimental group: 63% Control group: 68% | International Physical Activity Questionnaire-Long Version (IPAQ) Toxicological analysis of urine Timeline Follow Back. Perceived Stress Scale Life Orientation Test-Revised Brief Symptom Inventory-18 Brief Life Satisfaction Scale | The experimental group showed higher levels of physical activity in their day to day (IPAQ) The two groups improved in drug use, optimism and perceived stress, without differences between groups. There were no significant differences in global psychiatric symptoms or in life satisfaction. |
| Devi et al. [70] | SUD (various substances) | 66 (33 + 33) | Experimental group: 4 weeks of yoga, 70 min daily Control group: Conventional treatment | - | Beck Depression Inventory WHO Quality of Life –BREF | Significant improvements in depression and quality of life (domains physical health, psychological health and social relationships). |
| Dolezal et al. [27] | Methamphetamine | 28 (14 + 14) | 8 weeks, 3 days (60 min) per week. Experimental group: aerobic endurance and muscular strength Control group: Educational intervention, without exercise. | Experimental group: 92% Control group: 96% Economic incentives to favor adherence. | Scale, stadiometer and bending meter for anthropometric measurements Stress test to measure VO2 and cardiac function Electrocardiogram 1RM maximum leg press and chest press | Significant improvements in VO2 and strength of legs and chest Improvements in body composition Significant improvements in heart rate variability rates. |
| Flemmen et al. [18] | SUD (various substances) | 16 (9 + 7) | Experimental group: 8 weeks, 3 days per week of high intensity interval training (4 × 4 ‘90–95% HRmax) Control group: Conventional rehabilitation treatment. | 92% | Stress test (Cortex Metamax II portable metabolic test system) to assess VO2 and effort economy. Addiction Severity Index Insomnia Severity Index Hospital Anxiety and Depression Scale | Significant improvement in VO2 Significant improvement (intragroup, but not between groups) in depression There were no significant differences in effort economy, insomnia and anxiety. |
| Muller et al. [20] | SUD (various substances) | 35 (24 + 11) | Experimental group: 10 weeks of aerobic exercise and light strength, 3 sessions (30 min) per week. Control group: Conventional treatment | 69% | The World Health Organization Quality of Life Brief The Hopkins Symptoms Checklist European Addiction Severity Index | Significant improvements in the domains “Physical Health” and “Psychological Health” of Quality of Life. Improvements in anxiety and depression, but not significant. |
| Agarwal et al. [15] | Consumers of crack with HIV (cocaine) | 24 (12 + 12) | Experimental: 8 weeks of yoga/Meditation, 2 sessions (60 min) per week. Control: Conventional treatment | 88% | Short Form 36 Health Survey (SF-36) Perceived Stress Scale (PES) Impact of Events Scale(IES) Measurements of cortisol and DHEA-S in saliva | Significant improvements in perceived stress (PES and IES) No changes in Cortisol and DHEA-S in saliva. There were no significant improvements in quality of life. |
| Dhawan et al. [71] | Opiates (60% of heroin sample) | 84 (55 + 29) | G. exp: 3 sessions (60 min) of yoga. G. control: Not specified | - | World Health Organization quality of life brief scale Urine toxicology test | Improvements in quality of life in the domains of physical health, psychological health and the environment. |
| Giménez et al. [72] | SUD (various substances) | 37 (18 + 19) | Experimental group: 12 weeks, 3 sessions (60–90 min) per week of aerobic endurance, strength-endurance and aerobic games, moderate intensity, Control group: Conventional treatment. | 81% | Six-Minute Walk Test (6MWT) Timed Get Up and Go Test (TGUG) Chair Stand Test (CST) Short Form Health Survey (SF-36) 11 Semi-structured interviews | Quantitative: Significant improvements in physical conditions and quality of life. Qualitative: Decrease in the number of injuries when exercising, weight loss, improvements in stress and anxiety, improvements in craving. |
| Rawson et al. [17] | Methamphetamine | 135 (69 + 66) | Experimental group: 8 weeks of aerobic exercise (60–80% HRmax) and strength, 3 sessions (60 min) per week. Control group: Education for health | Experimental group: 72% Control group: 77% Economic incentives | The Beck Depression Inventory The Beck Anxiety Inventory | Significant improvements in anxiety and depression Positive relationship between adherence to the program and the benefits obtained in anxiety and depression. |
| Grandjean da Costa et al. [22] | Crack and cocaine | 9 | 12 weeks aerobic exercise (running), 3 sessions (60 min) per week | 62% | Cooper 12-min test PAR-Q (Physical Activity Readiness Questionnaire) Blood pressure measurements Heart rate | Significant improvements at the cardiovascular and cognitive levels. |
| De la Garza et al. [8] | Cocaine | 24 (10 + 7 + 7) | 4 weeks, 3 sessions (30 min)/week: G. exp. 1: 30 min of walking on belt (25% of Maximum Heart Rate) G. exp. 2: 30 min of running on belt (75% of Maximum Heart Rate) G. control: sedentary activity | - | Heart rate Urine tests to identify cocaine use Subjective measurement measures of “craving” | Significant differences between the “runners” and “sedentary” groups in FC rest. There were improvements in abstinence in the experimental groups, but not statistically significant. |
| Zhu et al. [73] | Methamphetamine | 59 (30 + 29) | G. exp: 12 weeks of Tai chi, 5 sessions per week G. control: Conventional treatment, recreational activities | - | Quality of life for drug addiction (QOL-DA) Anthropometric measures Sit and reach test | Improvements in quality of life in the Tai chi group compared to the control group. |
| Colledge et al. [25] | Heroine | 24 (11 + 13) | Experimental group: 12 weeks of varied exercise, two sessions per week Control group: Not specified | - | German version of the Centre for Epidemiologic Studies Depression Scale Self-report Insomnia Severity Index (ISI) Brief Self Control Scale (BSCS) Perceived Stress Scale (PSS) Short-form health survey questionnaire (SF-36) Timeline Follow-back (TLFB) Physical Activity Questionnaire Short Form | The exercise group increased its daily exercise levels significantly, but no significant improvement was observed in any of the other variables measured. |
| Trivedi et al. [74] | Stimulants | 302 (152+150) | Experimental group: 12 weeks of aerobic exercise, three sessions per week. Control group: Education for health | Experimental group: 64% Control group: 74.7% | Timeline Follow Back Urine analysis | No significant differences between groups, but when controlling adherence, a significant improvement in abstinence was detected |
| Wang et al. [12] | Methamphetamine | 50 (25 + 25) | G. exp: 12 weeks, 3 sessions (30 min) per week of moderate intensity aerobic exercise and behavioral treatment. G. control: Conventional treatment and behavioral treatment | - | Visual analogue scale for craving measurement Standard Go/Nogo and MA-related Go/Nogo tasks Electroencephalogram | Significant improvements in craving and self-control compared to control group. |
| Carmody et al. [75] | Stimulant drugs (cocaine, amphetamine, methamphetamine) | 218 (75 + 143) | Experimental group: 9 months of aerobic exercise, moderate-vigorous intensity, three sessions per week Control group: Health education | - | Timeline Follow Back Stimulant Selective Severity Assessment Concise Associated Symptoms Tracking- Self-Report Addiction Severity Index | The experimental group presented significantly lower probability of relapse and lower consumption in case of having a relapse than the control group. |
| Zhang et al. [76] | Methamphetamine | 66 (34 + 32) | G. exp: 12 weeks, 3 sessions (30 min) per week of ex. aerobic moderate intensity G. control: Conventional treatment | - | CogState battery assessment Blood samples | The experimental group improved the speed of information processing and fat oxidation. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giménez-Meseguer, J.; Tortosa-Martínez, J.; Cortell-Tormo, J.M. The Benefits of Physical Exercise on Mental Disorders and Quality of Life in Substance Use Disorders Patients. Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3680. https://doi.org/10.3390/ijerph17103680
Giménez-Meseguer J, Tortosa-Martínez J, Cortell-Tormo JM. The Benefits of Physical Exercise on Mental Disorders and Quality of Life in Substance Use Disorders Patients. Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(10):3680. https://doi.org/10.3390/ijerph17103680
Chicago/Turabian StyleGiménez-Meseguer, Jorge, Juan Tortosa-Martínez, and Juan M. Cortell-Tormo. 2020. "The Benefits of Physical Exercise on Mental Disorders and Quality of Life in Substance Use Disorders Patients. Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 10: 3680. https://doi.org/10.3390/ijerph17103680
APA StyleGiménez-Meseguer, J., Tortosa-Martínez, J., & Cortell-Tormo, J. M. (2020). The Benefits of Physical Exercise on Mental Disorders and Quality of Life in Substance Use Disorders Patients. Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(10), 3680. https://doi.org/10.3390/ijerph17103680